Back to Journals » Clinical Ophthalmology » Volume 19
A Clinical Evaluation of Lifitegrast Ophthalmic Solution 5% in Symptomatic Contact Lens Wearers
Authors Schulze MM ![]() , Guthrie SE
, Guthrie SE ![]() , Ho B
, Ho B ![]() , Woods J
, Woods J ![]() , Jones L
, Jones L ![]()
Received 6 May 2025
Accepted for publication 21 August 2025
Published 29 August 2025 Volume 2025:19 Pages 3033—3049
DOI https://doi.org/10.2147/OPTH.S538184
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Marc-Matthias Schulze,1 Sarah E Guthrie,1 Brandon Ho,1,2 Jill Woods,1 Lyndon Jones1,2
1Centre for Ocular Research & Education (CORE), School of Optometry & Vision Science, University of Waterloo, Waterloo, ON, Canada; 2Centre for Eye and Vision Research (CEVR), The Hong Kong Polytechnic University, Pak Shek Kok, Shatin, Hong Kong
Correspondence: Marc-Matthias Schulze, Centre for Ocular Research & Education (CORE), School of Optometry & Vision Science, University of Waterloo, 200 University Avenue West, Waterloo, ON, N2L 3G1, Canada, Tel +1 519-888-4567 x45020, Email [email protected]
Purpose: To evaluate the effectiveness of lifitegrast ophthalmic solution 5% in alleviating end-of-day dryness and discomfort in symptomatic contact lens (CL) wearers.
Patients and Methods: This was an open-label study in symptomatic CL wearers with ratings of ≥ 40 for end-of-day dryness on a visual analog scale (VAS; 0– 100 scale; 100 worst). Participants wore their habitual CLs and instilled lifitegrast twice daily for 12 weeks with lenses removed. The performance of lifitegrast was assessed by comparing VAS 0– 100 ratings (100=worst) at 2, 6 and 12 weeks for end-of-day dryness and discomfort and Contact Lens Dry Eye Questionnaire-8 (CEQ-8) scores to baseline levels. Tear samples were collected at all visits to measure 10 different tear cytokines.
Results: Forty participants (33F, mean age 30.8± 12.1 years, 65% daily disposable CL users) completed the study. There were no serious adverse events. Median (range) visual analog scale ratings for end-of-day dryness (Baseline: 76 (19– 99); 2-weeks: 43 (0– 95); 6-weeks: 26 (0– 94); 12-weeks: 15 (0– 98)) and discomfort (Baseline: 70 (10– 97); 2-weeks: 45 (0– 95); 6-weeks: 25 (0– 84); 12-weeks 11 (0– 96)) both significantly improved over time (all p< 0.01). At baseline, 100% of participants rated dryness ≥ 40, which dropped to 17% at 12 weeks. Baseline CLDEQ-8 scores of 22 (12– 31) had significantly decreased to 11 (1– 26) at 12 weeks. Comfortable CL wear time increased significantly from 6± 2 hours at baseline to 9± 3 hours at 6 and 12 weeks (all p< 0.01). Cytokine levels did not change over time.
Conclusion: Lifitegrast significantly improved end-of-day dryness, end-of-day discomfort, CLDEQ-8 scores and comfortable CL wear time within 2 weeks of use.
Keywords: lifitegrast, contact lens, contact lens symptoms, contact lens discomfort, dry eye, tear cytokines
Introduction
The Tear Film and Ocular Surface Society’s (TFOS) workshop on contact lens discomfort (CLD) has defined CLD as a condition characterized by episodic or persistent adverse ocular sensations related to lens wear, either with or without visual disturbance, resulting from reduced compatibility between the contact lens and the ocular environment, which can lead to decreased wearing time and discontinuation of contact lens wear. 1
Contact lens discomfort is the leading cause for CL “dropout”, is prevalent in up to 50% of current wearers and is frequently associated with symptoms of ocular dryness.1–8 The severity of CL discomfort varies throughout the day but is typically found to be worst towards the end of the daily wearing time, a symptom typically referred to as end-of-day (EOD) discomfort.3,8,9 Contact lens discomfort can be caused by a variety of factors related to the contact lens (eg, material, fitting, design or surface characteristics) and/or to the patient (eg, demographics, tear film, ocular surface characteristics or the environment).1,2,5,10–12
Due to the multitude of these potential causes, there is no universal strategy in reducing symptoms of CL discomfort. Hence, CL wearers use various strategies, including discontinuation of CL wear,5,13–16 reducing wear time (days per week and/or hours per day),3,13–16 switching to a different contact lens type, material or wear modality6,16–18 or adopting the use of rewetting drops.7,16,19,20 The use of over-the-counter (OTC) rewetting drops, while providing temporary relief for some wearers, has been reported to be of moderate benefit, particularly later in the day.4,20
Prescription eye drops for dry eye disease (DED) may also have potential to reduce symptoms of discomfort in symptomatic CL wearers. One prescription medication that has been found to be safe and effective in treating signs and symptoms of patients with moderate-to-severe DED is lifitegrast ophthalmic solution 5%, sold under the brand name Xiidra (Bausch + Lomb, Bridgewater, New Jersey, USA).21–24 Lifitegrast is an immunomodulator that works by blocking the interaction between LFA-1 (lymphocyte function-associated antigen-1), an integrin found on lymphocytes, and ICAM-1 (intercellular adhesion molecule-1), which is present on the surface of immune cells, epithelial cells, endothelial cells, and keratinocytes.21–23,25,26 By preventing this binding, lifitegrast helps reduce inflammation and alleviate the signs and symptoms of dry eye disease.21–23,26 The immunomodulating mechanism of lifitegrast may also have the potential to reduce inflammatory processes caused by contact lens wear. The inflammatory nature of CL wear has been well documented and may present with both clinical (redness, swelling or EOD discomfort) and sub-clinical markers (cellular or biochemical reactions).2,10–12 However, the potential value of immunomodulators such as lifitegrast to alleviate discomfort in symptomatic contact lens wearers remains largely unexplored. A PubMed® search using the keywords “lifitegrast” and “contact lens” only resulted in a single publication on the use of lifitegrast in CL wearers.27 Gonzalez investigated the safety and efficacy of lifitegrast in contact lens discomfort in a group of habitual wearers of the same non-ionic, low modulus, silicone hydrogel monthly replacement lens material, samfilcon A (sold under the brand name Bausch + Lomb ULTRA®).27 After using lifitegrast over the course of eight weeks, participants were found to have significant reductions in the overall CLDEQ-8 score6 and for the CLDEQ-8 individual questions 1A (frequency of discomfort), 1B (severity of discomfort), 2A (frequency of eye dryness) and 2B (severity of eye dryness).27 While these findings are promising, they can only be representative for wearers of the study lens type, samfilcon A; no data on any other lens types in combination with the use of lifitegrast have yet been published. Gaining further knowledge on the use of lifitegrast in a larger population of symptomatic CL wearers with a multitude of different lens types may be of great interest for clinicians and patients.
The purpose of this study was to investigate whether comfort and dryness in symptomatic soft contact lens wearers improved after using lifitegrast ophthalmic solution 5% twice a day for 12 weeks while continuing to wear their habitual contact lenses.
Materials and Methods
Ethics
This clinical study was conducted in compliance with the ethical principles in the Declaration of Helsinki, the ICH guidelines for Good Clinical Practice (GCP), the University of Waterloo’s Guidelines for Research with Human Participants, and the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans, 2nd Edition. Ethics clearance was obtained through the Office of Research Ethics at the University of Waterloo before the commencement of the study. In addition, all participants had signed written informed consent prior to any study measurements being performed.
Study Design
This was an investigator-initiated, prospective, open-label, dispensing pilot study that was conducted at a single site in Waterloo, Ontario, Canada, and registered at https://www.clinicaltrials.gov with the trial number NCT04297618. The study included five study visits over the course of 12 weeks (Table 1).
 |
Table 1 Summary of Study Visits and Visit Windows |
Eligibility for the study was determined during a screening visit. The eligibility criteria for this study closely aligned with the criteria used in the original Phase III studies for the evaluation of lifitegrast in DED.21,22 To be eligible for the study, participants 18 years of age or older had to be symptomatic wearers of daily, soft, frequent replacement lenses (daily disposable, bi-weekly or monthly lenses for any kind of refractive error) that were available in Canada. In order to meet the criteria for symptomatic CL wear, participants had to (1) meet or exceed the minimum levels for symptomatic soft CL wear (frequency: sometimes; severity: ≥3 on the 0 = none to 5 = very intense scale) according to the categorization by Young et al28 and (2) rate the dryness at the end of their wear time (end-of-day; EOD) as ≥40 on a 0–100 visual analog scale (VAS, where 100 = maximum symptom severity); the VAS used in this study was a slightly modified version of the VAS used previously in DED patients,21,22 and asked participants to rate their CL wear-related eye dryness just before lens removal for a typical lens wear day. In addition, participants were required to wear their habitual soft CLs for a minimum of five days per week for six hours per day during the month prior to enrolment; had to be willing to maintain this CL wear routine for the 12-week duration of the study; had to achieve acceptable lens fit as well as visual acuity (VA) correctable to logMAR +0.20 or better in each eye with their habitual contact lens type; to have a history of artificial tear or rewetting drop use at least once in the 30 days prior to study enrolment; to be willing to use lifitegrast drops twice a day on a daily basis (irrespective of CL wear); and to stop use of any habitual rewetting drops and/or artificial tears over the course of the 12-week treatment phase.
Participants were excluded from the study if they were participating in any concurrent clinical or research study; were wearing soft CLs on an extended wear basis; had a known sensitivity to the investigational product or diagnostic substances (eg, fluorescein) to be used in the study; had any known ocular disease and/or infection; had a systemic condition (eg, active or uncontrolled systemic conditions such as allergies, autoimmune disease or immunodeficiency disease) or used any systemic or topical medications that may have affected a study outcome variable (eg, topical cyclosporine), any other topical ophthalmic medication, antihistamines, aspirin; were pregnant, lactating or planning a pregnancy at the time of enrolment (by self-report); had undergone refractive error surgery within the last six months or cataract surgery within the last 12 months.
Because of lifitegrast prescription requirements in Canada, a qualified investigator with a medical degree reviewed all screening documents after completion of the screening visit to confirm that the participant met all eligibility criteria and was suitable to be prescribed and to use lifitegrast during the 12-week study. Only after the qualified investigator had confirmed eligibility and approved of the drop use, eligible participants were invited to the baseline and dispense visit.
Assessment of Study Endpoints
To allow comparisons over time, all study assessments at the baseline and dispense visit and at the 2-week, 6-week and 12-week follow-up visits were identical. Participants attended each of these visits with a new pair of their habitual CLs that had been worn for at least six hours prior to visit start. Baseline assessments were conducted at the baseline and dispense visit prior to the first instillation of lifitegrast.
Study Endpoints
The primary endpoints for this study were subjective ratings of CL wear-related EOD discomfort and dryness (0–100 VAS scale, with 100 being worst) at 12 weeks compared to baseline.
Additional endpoints for this study included subjective ratings of CL wear-related EOD discomfort and dryness (0–100 VAS scale, with 100 being worst) at two and six weeks compared to baseline; CLDEQ-8 score at two, six and 12 weeks compared to baseline; comfortable and total wear time (hours); VAS ratings of CL wear-related burning/stinging, itching, foreign body sensation, photophobia and pain at two, six and 12 weeks compared to baseline; the quantity of tear film inflammatory markers after 6 hours of CL wear at two, six and 12 weeks compared to baseline; non-invasive tear break-up time (pre-lens; PLNITBUT) at two, six and 12 weeks compared to baseline; and ocular redness at two, six and 12 weeks compared to baseline.
Clinical Assessments
Study assessments at the baseline and dispense visit (V2) as well as all follow-up visits (V3 to V5) were conducted in the same order, from least to most invasive. First, participants assessed their own lens wear experience, which was followed by measurements of visual acuity (VA), pre-lens non-invasive tear film break-up time (NITBUT) and pre-lens ocular redness measurements. The participants were then asked to remove their CLs before tear samples were collected from their eyes. A full anterior segment biomicroscopy examination and a measurement of VA completed each study visit.
The participants assessed their subjective habitual lens wear experience by rating seven CL-wear related symptoms (EOD dryness, EOD discomfort, burning/stinging, itching, foreign body sensation, photophobia and pain) on a 0 to 100 VAS (100 = most severe symptom level) that was modified for CL wear from the VAS used by Tauber et al and Holland et al21,22 and by completing the CLDEQ-8 questionnaire.6 Participants were asked to rate the symptom severity for a typical day in the past week on a 100mm VAS that showed reference points at minimum (0%) and maximum severity (100%), with the scale mid-point being indicated as 50%; no other markings were visible on the scale. The distance in mm from the 0% mark to the participant’s severity marking was then measured by the study investigator and converted into a 0–100 symptom rating.
In addition, total and comfortable wear time on a typical day were recorded.
Pre-lens NITBUT was measured using a placido-disc based device (Atlas 991 corneal topographer; Zeiss Humphrey Systems, Dublin, California, USA) that projected concentric rings on the tear film; three measurements for each eye were taken and averaged, using the averaged NITBUT for analysis. Bulbar and limbal redness were assessed (with CLs on eye) subjectively at the slit-lamp biomicroscope and graded using the Efron 0–4 grading scale (with 0.1 increments) for each conjunctival quadrant followed by an automated redness measurement (temporal and nasal quadrant only; 0–4 scale in 0.1 increments) using the Keratograph 5M (Oculus, Wetzlar, Germany).
Safety measurements in this study were conducted at all study visits (V1 to V5) and included high illumination high contrast (HIHC) distance visual acuity (VA) measurements and a full anterior segment slit lamp biomicroscopy examination. Visual acuity was measured using computer-generated acuity charts (M&S Technologies, Niles, Illinois, USA) using the logarithm of the Minimum Angle of Resolution (logMAR) notation. Slit-lamp biomicroscopy assessments included the assessment of corneal integrity (such as infiltrates or opacities), the assessment and grading of corneal and conjunctival staining after application of sodium fluorescein using blue light and a Wratten 12 filter (Efron 0–4 scale using 0.1 increments) and the assessment and grading of redness and roughness of the palpebral conjunctiva (Efron scale using 0.25 increments).
Tear Collection and Inflammatory Marker Quantification
Samples of basal tears were collected at the baseline and dispense visit and at all follow-up visits to evaluate whether the use of lifitegrast resulted in changes in inflammatory tear film biomarkers over the course of the study. Basal tears were collected by holding a disposable, sterile glass tube near the participant’s lower lid without touching the surface of the eye. Tear collection started approximately three minutes after participants had removed their contact lenses, after all the CL-associated study measurements had been completed. During the procedure, participants were allowed to blink normally. Tears were collected from each eye until at least 5 µL of basal tears had been collected, or after a maximum of five minutes collection time, whichever occurred first. Tears collected from the right and left eye were pooled in a single vial. All tear samples were individually labeled with the participant ID number and visit code and frozen at −80°C until further processing.
Frozen tear samples went through a single freeze–thaw cycle prior to analysis and were thawed on ice. Approximately 3 µL of each tear sample was aliquoted into a microfuge tube prior to detection of tear film inflammatory markers. The tear samples were diluted to a total volume of 120 µL in Mesoscale Discovery assay diluent buffer provided by the manufacturer (Mesoscale Discovery K15049D, Rockville, Maryland, USA). Two technical replicates for each participant sample were added to the assay plate. The levels of ten pro-inflammatory cytokines (IFN-γ, IL-1β, IL-2, IL-4, IL-6, IL-8, IL-10, IL-12p70, IL-13, and TNF-α) were measured in each sample using the Mesoscale Discovery (MSD) V-PLEX Proinflammatory Panel 1 (Human) Immunoassay kit (MSD K15049D, Rockville, Maryland, USA). Each plate was quantified on the MESO QuickPlex SQ 120MM platform according to manufacturer instructions (MSD, Rockville, Maryland, USA).
Study Products and Treatments
Lifitegrast ophthalmic solution 5% is supplied in low-density polyethylene single-use containers, each containing 0.2 mL solution corresponding to 10 mg lifitegrast. Prior to the first application of lifitegrast during the baseline and dispense visit, the manufacturer’s instructions for use29 were provided to and reviewed with each participant to ensure appropriate use of the single-use containers and drops during the study. Participants were instructed to apply one drop of lifitegrast into the lower lid pouch of each eye twice a day, approximately 12 hours apart, using a new single-use container at each instillation time. The instructions also included that participants should not instill lifitegrast while wearing CLs and to wait at least 15 minutes after drop instillation before lens insertion. Lastly, the potential side effects for lifitegrast that may be experienced (eg, dysgeusia or instillation site discomfort) were reviewed.
To ensure that any potential study findings could be attributed to the newly introduced use of lifitegrast only, each participant continued to wear their habitual contact lens type and, if applicable, continued to use their habitual lens care products. In alignment with the eligibility criterion for minimum wear time, participants were instructed to continue wearing their CLs for a minimum of five days per week and six hours per day for the duration of the study. Participants were also instructed to wear a new pair of lenses to the baseline visit and the 2-week, 6-week and 12-week follow-up visits.
During the course of the study, participants were prohibited from using any habitual rewetting drops or artificial tears; hence, the use of lifitegrast instead of a participant’s habitual eye drops was the only change to the regular CL wear regimen of each participant.
Statistical Analysis
Data analysis of the clinical data was conducted using Statistica 13.5 and IBM SPSS Statistics 27.0; Python 3.7.1 was used for data plots and analysis of the inflammatory marker data.
Statistical analysis showed that data for the majority of clinical endpoints were not normally distributed (Kolmogorov–Smirnov test; p<0.05), so that all data were analyzed using non-parametric statistics for consistency. Friedman ANOVA was used to analyse variation over time, and Wilcoxon Matched Pairs testing was performed to identify differences between visits, with statistical significance set at 5%. Superiority testing for the primary outcome variable (ie, VAS ratings for CL-related eye dryness and discomfort at 12–weeks vs baseline) was performed using a superiority margin of 10 units on the 100-point scale. Since there was no difference between eyes for assessments conducted for each eye separately (redness, safety variables and NITBUT), the data for the right eye only are reported in this manuscript.
To analyze changes in cytokine level over time, the fold-change between each visit compared to the baseline was log2 transformed. This logarithmic normalization was performed to provide a symmetric scale for both upregulated and downregulated cytokine levels, compared to baseline.
Results
Forty-five participants were enrolled in the study (38 female, 7 male). Two participants did not pass the screening requirements and were ineligible to participate in the study, one due to an incompatible medical condition and one did not achieve the minimum visual acuity. A third participant was discontinued due to ocular findings (multiple corneal infiltrates in both eyes) that were identified during the biomicroscopy examination at the dispense visit; this participant was never exposed to the lifitegrast study drops. Two additional participants withdrew consent after exposure to lifitegrast, one due to inconvenience and one due to a lifitegrast side effect (increase in tears).
The remaining 40 participants (33 female, 7 male) completed the study and comprised the analysis population. All participants wore their habitual lenses between five and seven days per week. The mean age of the analysis population was 30.8 ± 12.1 years (median 26 years, range 18 to 66 years). The analysis population was composed of 26 daily disposable CL wearers (65%) and 14 reusable CL wearers (35%) who wore a total of 17 different lens types (11 daily disposable vs 6 reusable); differences in lens design were not accounted for in the number of lens types (eg, a spherical, toric or multifocal correction of lens type A were all recorded as lens type A, and not further sub-divided).
Study Endpoints
Primary Endpoints
Statistical analysis of the primary study endpoints showed that there was a significant variation in CL wear-related EOD dryness and discomfort over time (p<0.01).
Wilcoxon matched pairs testing was performed for pairwise comparisons between visits and detected a significant reduction in CL wear-related EOD dryness after two, six and 12 weeks of lifitegrast use compared to baseline values collected prior to the dispense of lifitegrast (Figure 1; all p<0.01).
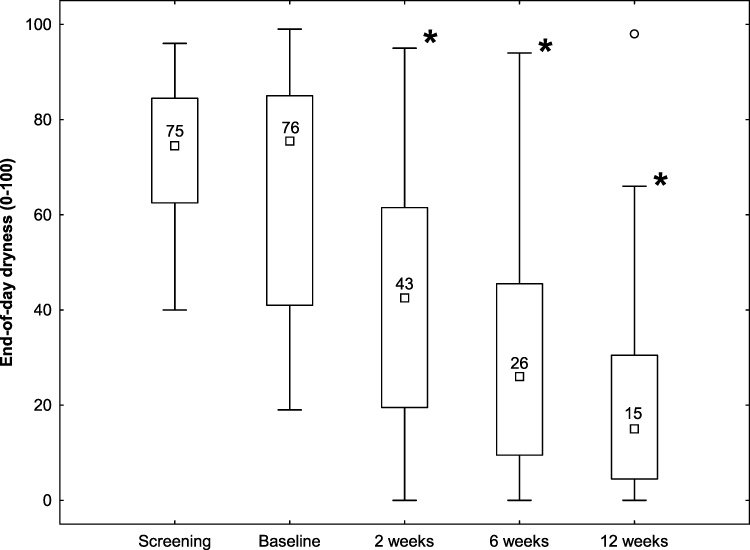 |
Figure 1 End-of-day dryness ratings over time; 0–100 integer scale where 0=no dryness. Box-Whisker plots show median (▫), 25–75% range (□), non-outlier range (Т), and outliers (◦). Statistical differences compared to baseline levels are indicated by *. |
Because CL wear-related EOD dryness was one of two inclusion criteria to determine symptomatic CL wear, it was of interest to evaluate whether the use of lifitegrast would have impacted participant eligibility for the study over time. To evaluate this during the statistical analysis of the study data, the relevant rating cut-off for EOD dryness of ≥40 that was used at the screening visit was also applied at all follow-up visits to identify the number of participants who fell below this threshold during the 12-week use of lifitegrast. At the screening visit, all participants had a CL wear-related dryness rating of at least 40, in alignment with the inclusion criterion. After two weeks, almost half of the participants (18 or 45%) would not have qualified for the study anymore, with the number of participants not qualifying for the study increasing to 30 (75%) after 6 weeks and 33 (83%) after 12 weeks of lifitegrast use.
Similar to EOD dryness, there was a significant reduction in CL wear-related EOD discomfort after two, six and 12 weeks compared to baseline values collected prior to the dispense of lifitegrast (Figure 2; all p<0.01).
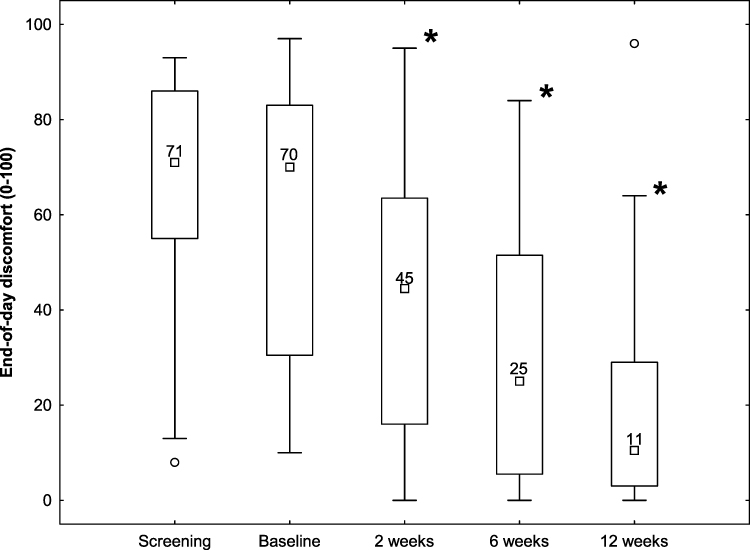 |
Figure 2 End-of-day discomfort ratings over time; 0–100 integer scale where 0=no discomfort. Box-Whisker plots show median (▫), 25–75% range (□), non-outlier range (Т), and outliers (◦). Statistical differences compared to baseline levels are indicated by *. |
Superiority testing was performed for both primary endpoints using a superiority margin of 10 units on the 100-point scale; this threshold was selected to exceed the previously reported just-noticeable difference in comfort for contact lens wear, which has been estimated at approximately 7 points.30,31 Participant ratings for CL wear-related EOD dryness and EOD discomfort after 12 weeks of using lifitegrast were statistically superior compared to ratings at baseline (p<0.01).
Other Endpoints
There was a significant variation in CLDEQ-8 scores over time (p<0.01). Lifitegrast use resulted in statistically significantly reduced CLDEQ-8 scores in comparison to baseline at the 2-week, 6-week and 12-week follow-up visit (Figure 3; all p<0.01).
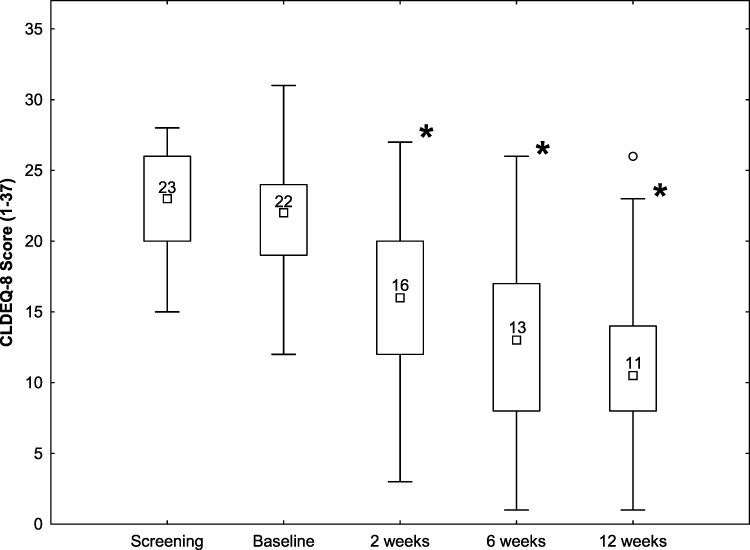 |
Figure 3 CLDEQ-8 scores over time. Box-Whisker plots show median (▫), 25–75% range (□), non-outlier range (Т), and outliers (◦). Statistical differences compared to baseline levels are indicated by *. |
Table 2 shows the number of participants, stratified by visit, who were diagnosed as highly symptomatic soft CL wearer (ie, CLDEQ-8 score of ≥12) according to the categorization by Chalmers et al32 and the number of participants who achieved a clinically significant improvement in CLDEQ-8 scores (ie, a change of 3 points or more)32 relative to baseline.
Similar to the VAS ratings for EOD dryness and discomfort, the primary outcome variables in this study, there was significant variation in symptom scores for the remaining five VAS symptoms of burning/stinging, itching, foreign body sensation, photophobia and pain over time. There was a significant improvement in ratings for each of these five symptoms after as early as two weeks of lifitegrast use (Figure 4).
 |
Table 2 Diagnostic Criteria Based on the CLDEQ-8 Score (Count (%)), According to Chalmers et al32 |
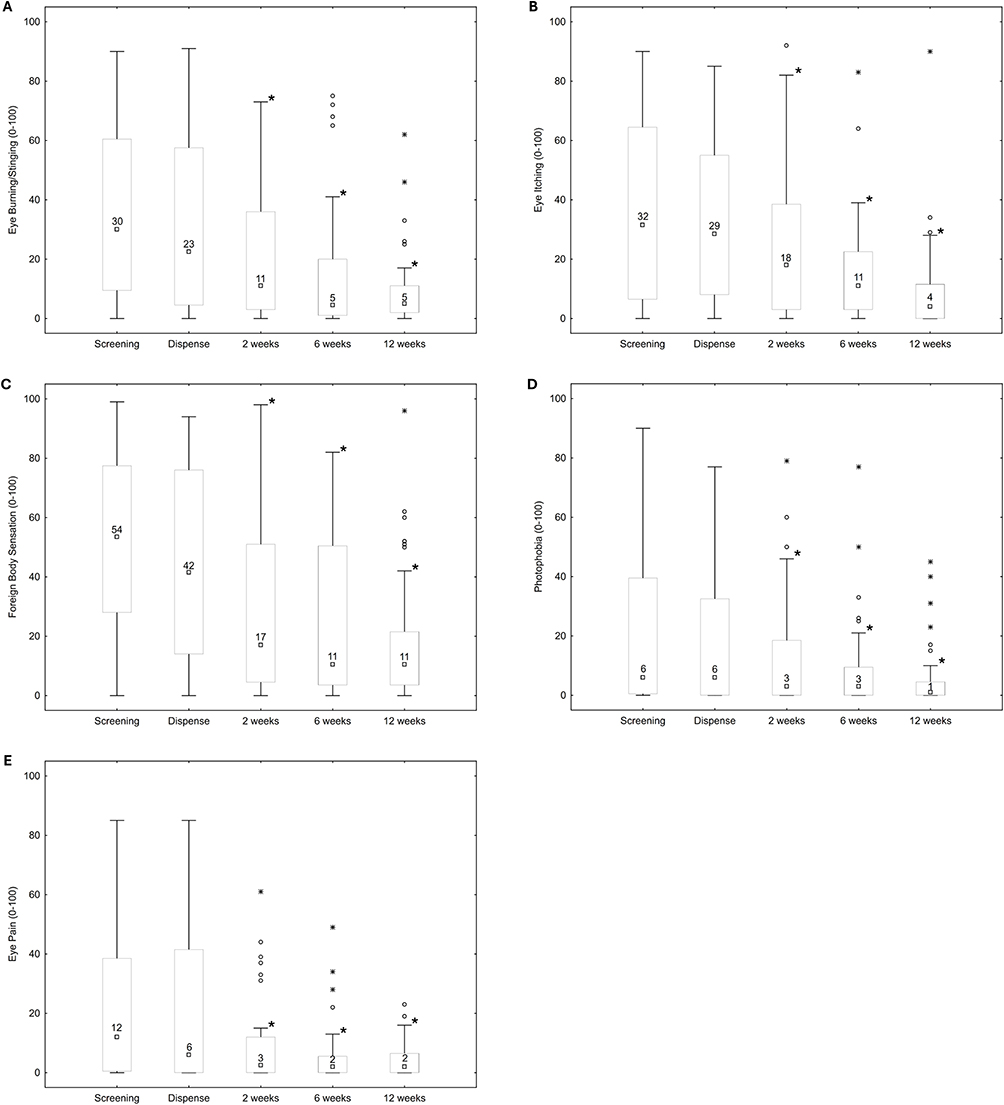 |
Figure 4 VAS symptom ratings over time for Burning/Stinging (A), Itching (B), Foreign Body Sensation (C), Photophobia (D) and Pain (E). Box-Whisker plots show median (▫), 25–75% range (□), non-outlier range (Т), outliers (◦) and extremes (□). Statistical differences are indicated by *. |
Figure 5 shows the self-reported total wear time (WT) and comfortable wear time (CWT) in hours at the baseline (BL) and the 2-week (2W), 6-week (6W) and 12-week (12W) study visits. While there were no changes in total wear time during the study, there was a significant improvement in comfortable wear time compared to baseline at all follow-up visits (Figure 5; all p<0.01).
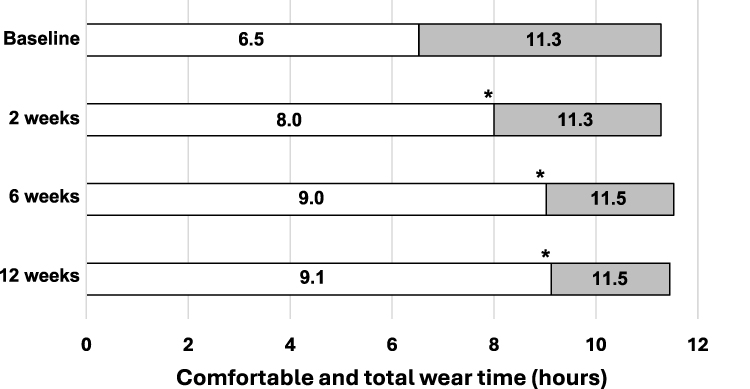 |
Figure 5 Comfortable wear time (white) and total wear time (grey) in hours. Significant differences in comfortable wear time compared to baseline are indicated by *. |
There was no significant difference in NITBUT (median [range]) after two weeks (5.3 [2.7 to 18.8]), six weeks (5.2 [2.7 to 12.5]) and 12 weeks (4.6 [2.3 to 10.9]) of lifitegrast use compared to baseline values (4.4 [1.9 to 11.4]) collected prior to the dispense of the lifitegrast drops (all p>0.05). Using lifitegrast eye drops did not result in any statistically or clinically significant changes in bulbar or limbal redness over the course of the study neither for the automated redness grades as determined by the K5M nor for subjective grades based on the Efron scale (Table 3; all p>0.05).
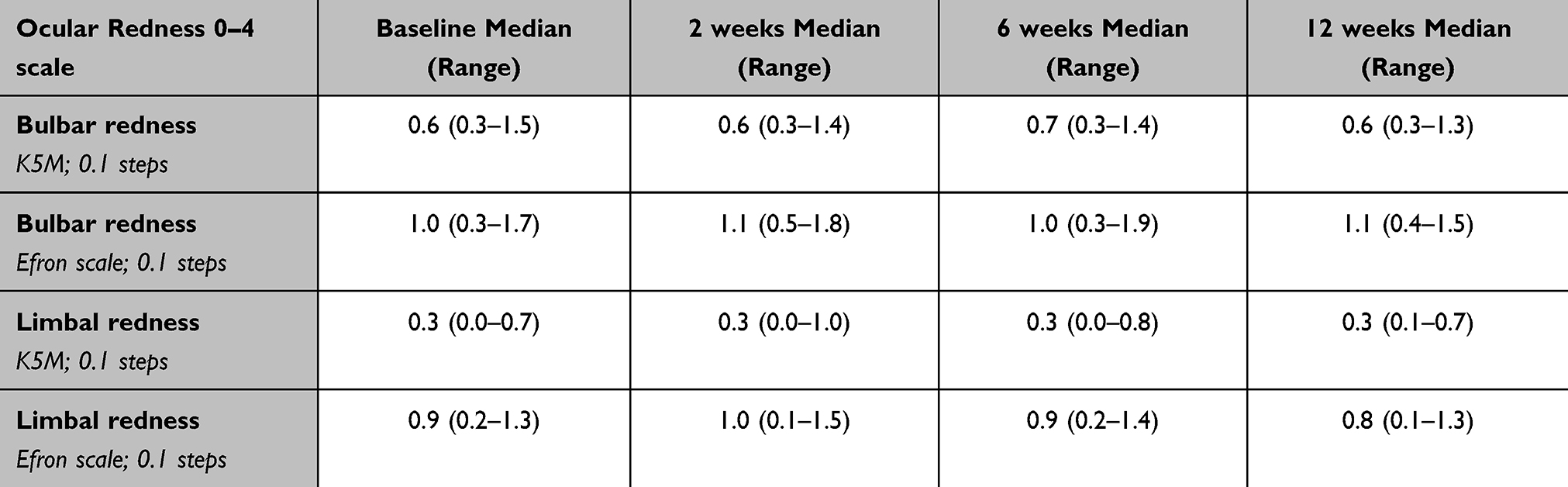 |
Table 3 Bulbar and Limbal Redness Over Time |
A collection of basal tears was attempted from the 40 participants who completed the baseline and all follow-up visits, corresponding to a theoretical total of 160 samples. In nine instances, insufficient tear volume (ie, <0.5µL) was acquired. This left a total of 151 samples for analysis of tear film inflammatory cytokines, which included 35 samples for which less than 3µL were available (Table 4). For the majority of participants, levels for six of the ten cytokines tested were below detection levels. Sample measurements were designated as reliable if they were within the limits of detection and within the curve fit for each cytokine standard curve as calculated by the software that was provided with the MSD Immunoassay kit. Cytokine data for the baseline and all follow-up visits was available for three of the ten tested cytokines (IL-1β, IL-6, and IL-8) only, with complete datasets from 18, 25 and 31 participants, respectively. One cytokine, IL-2, was reliably detected in only four participants for each visit. The remaining six cytokines were either not quantified or exhibited measurement values of low confidence (Figure 6 and Table 5).
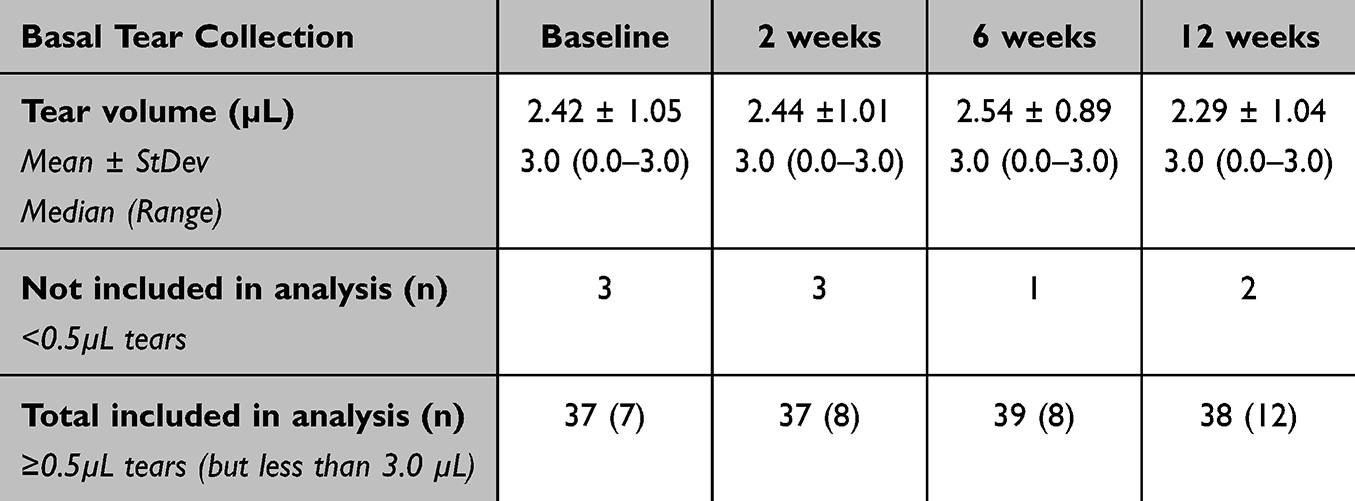 |
Table 4 Basal Tear Volumes Available for Cytokine Analysis by Study Visit. The Number of Participants That Had Insufficient Tears (ie, <0.5µL) and Whose Sample Could Not Be Included in the Analysis are Shown in the second Row. The Third Row Shows the Total Number of Samples That Were Included in the Analysis, with the Number in Brackets Corresponding to Samples with <3.0µL Which Were Still Included in the Cytokine Analysis |
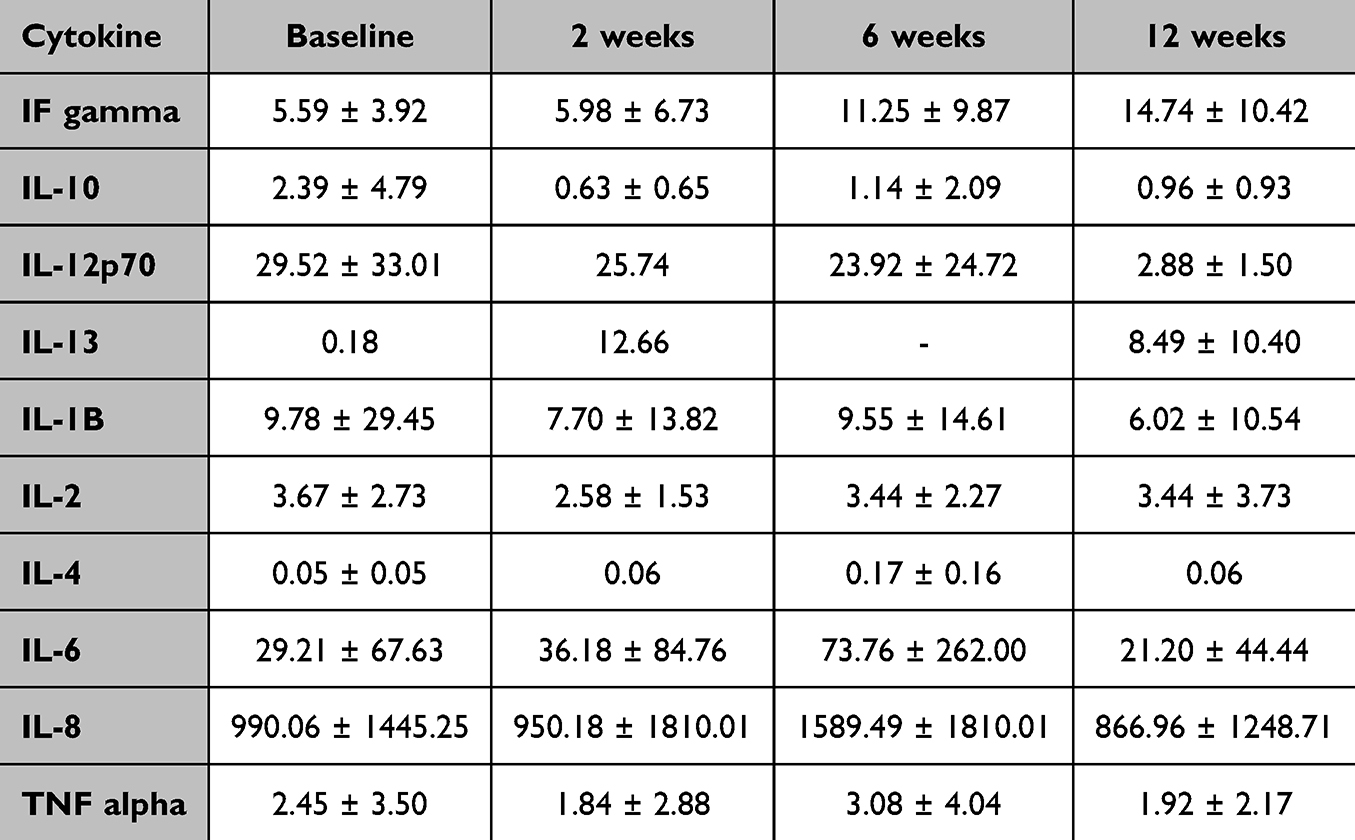 |
Table 5 Cytokines Detected in This Study, and the Average and Standard Deviation for Each Cytokine in pg/mL Across All Patients for Each Visit Is Indicated |
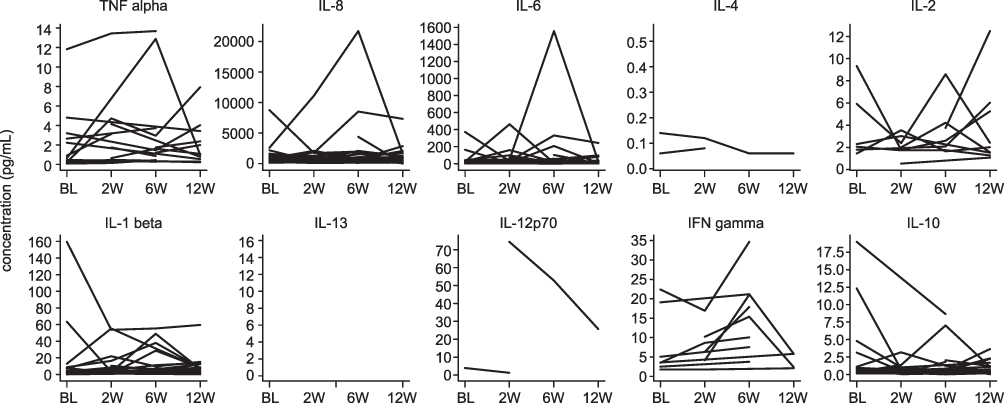 |
Figure 6 Changes in participant inflammatory cytokines over time. Concentration of 10 inflammatory cytokines (IFN gamma, IL-10, IL-12p70, IL-13, IL-1B, IL-2, IL-4, IL-6, IL-8, and TNF alpha) in pg/mL at each visit where tear samples were collected from participants. Each line represents the cytokine concentration for a single participant across all visits where a measurable quantity was obtained. Visit codes are shown as BL (Baseline), 2W (2 weeks), 6W (6 weeks) and 12W (12 weeks). |
Safety
To ensure the use of Lifitegrast did not result in any clinical complications, a full examination of the anterior eye as well as an assessment of distance vision were conducted at each study visit for safety purposes.
Biomicroscopy examinations found no changes over time for any of the ocular anterior segment parameters in this study (Table 6), with the exception of a temporary, statistically significant but not clinically meaningful difference to baseline grades for upper lid roughness at 6 weeks only (p=0.04).
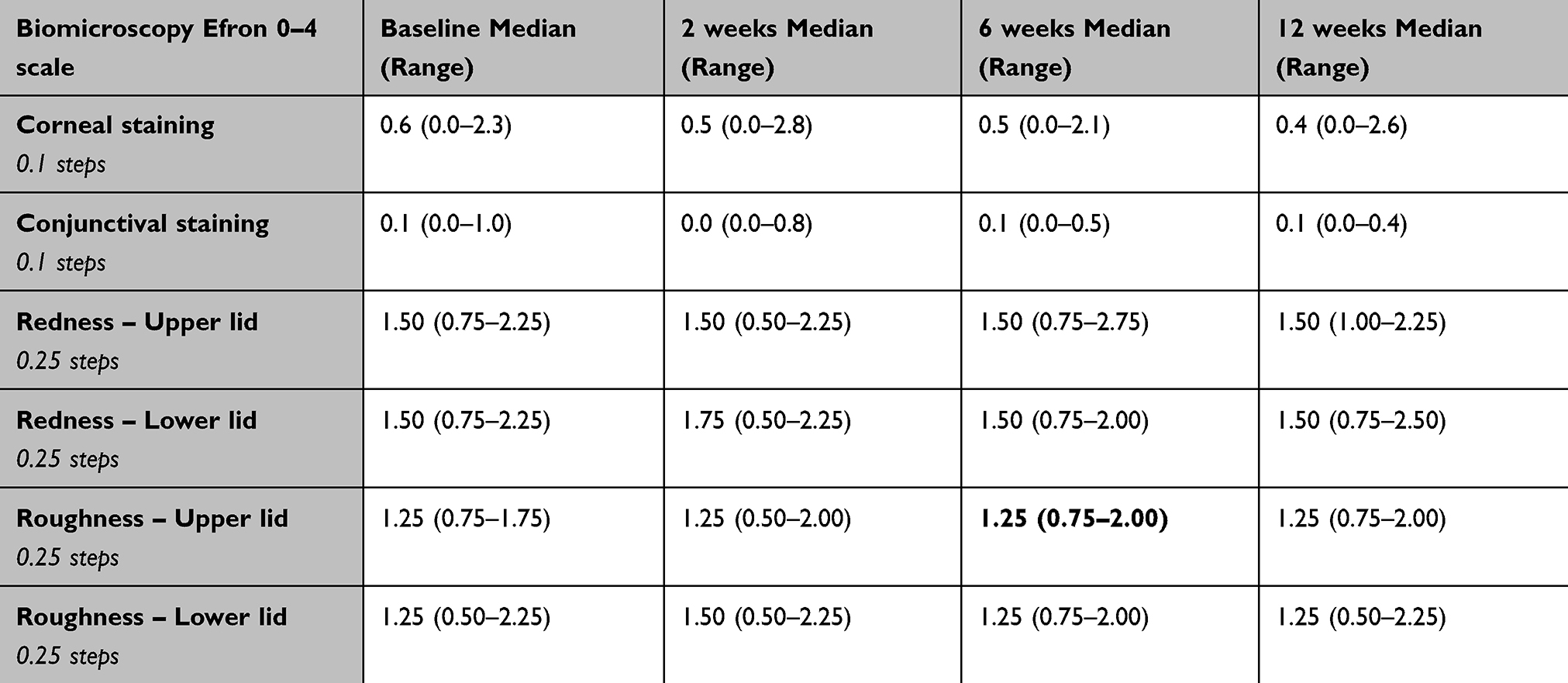 |
Table 6 Biomicroscopy Findings (Efron 0–4 Scale). Data are Shown for OD as Median (Range). Significant Differences Compared to Baseline are Shown in Bold |
Distance HIHC VA was found to be stable throughout the study, with a neither statistically nor clinically significant difference of ≤0.02 logMAR (corresponding to a single letter) at any follow-up visit in comparison to baseline VA levels (all p>0.05).
There were a total of 14 (eight ocular) adverse events in this study, with two of these adverse events (one ocular; one non-ocular) considered to be treatment related. The treatment-related ocular adverse event occurred in a participant who reported an increase in tears at the 6-week follow-up visit that resolved after cessation of lifitegrast use; this participant was discontinued from the study and their data were not part of the analysis population. The treatment-related non-ocular adverse event occurred in a participant who reported dryness around their periorbital eyelid skin, which may have been caused by spillage of lifitegrast eye drops out of the eyes during drop instillation. The adverse event fully resolved and the participant completed the study and their data were included in the analysis population.
The remaining adverse events were not or unlikely related to the use of lifitegrast. The ocular adverse events included four adverse events in the same discontinued participant (multiple bilateral sterile infiltrates diagnosed at the baseline and dispense visit, prior to exposure to the study drops, with the diagnosis later upgraded to infiltrative keratitis for both eyes); irritated red eye and purulent discharge due to a chemical and foreign body irritation (n=1); bacterial conjunctivitis caused by make-up accidentally applied to the eye (n=1); acute bacterial conjunctivitis of unknown cause (n=1). The non-ocular adverse events included COVID (n=2); ear infection (n=1); sinus infection (n=1); and a flare up in an existing medical condition (n=1).
Discussion
This study evaluated whether comfort and dryness in symptomatic contact lens (CL) wearers improved after using lifitegrast ophthalmic solution 5% twice a day for 12 weeks.
The primary outcome variables were VAS subjective ratings of CL wear-related EOD discomfort and dryness at 12 weeks compared to baseline. The improvements in median VAS scores of 61 and 59 points on a 100-point scale for EOD dryness and discomfort, respectively, after 12 weeks of lifitegrast use are a strong indication for the suitability of lifitegrast as potential treatment option for symptomatic CL wearers. While this finding on its own is promising for symptomatic soft CL wearers, the potential of prescribing lifitegrast as treatment for symptomatic CL wearers is further supported by statistically significant and clinically relevant improvements in EOD dryness and discomfort after as little as two weeks (Figures 1 and 2). In fact, the use of lifitegrast also significantly improved symptoms of burning/stinging, itching, foreign body sensation, photophobia and pain after two weeks, with symptoms continuing to improve throughout the study period (Figure 4). The finding that EOD dryness symptoms improved in about half of the 40 study participants (18/40 = 45%) to a degree that they would not have met the symptom-related eligibility criteria for this study after just two weeks of treatment further underscores the effectiveness of lifitegrast after even a short period of use. This fast treatment effect suggests that a similarly brief trial prescription of lifitegrast for symptomatic CL wearing patients may provide clinicians with the information they need for the future management of their symptomatic patients.
While quick improvements in symptoms are desirable, the ability to maintain or further improve symptoms is even more important when evaluating the effectiveness of a treatment. The continued reductions in median dryness and discomfort scores out to 12 weeks (both dropped a further 21 points from two to 12 weeks) are a clear indication of the continued treatment effect of lifitegrast in symptomatic soft CL wearers.
To date, the efficacy of lifitegrast in CL wearers has only been investigated in a single study that evaluated its use in a group of asymptomatic wearers of the same habitual lens type, samfilcon A, as defined by a history of at least 10 months of comfortable wear.27 In that study, a reduction of 1.68 points in CLDEQ-8 scores had been reported after eight weeks of lifitegrast use. In contrast, there was a 6-point reduction in CLDEQ-8 scores for the symptomatic wearers of 17 different contact lens types in this study after just two weeks, with CLDEQ-8 scores continuing to decrease over the 12-week study period (Figure 3). In order to facilitate interpretation of CLDEQ-8 scores, Chalmers et al reported a CLDEQ-8 cut-off value of ≥12 to identify highly symptomatic soft CL wearers and identified a clinically important difference of three points when comparing symptom scores over time.32 Using these criteria, all study participants met the diagnosis of highly symptomatic soft CL wearers at baseline (100%), while less than half (43%) of the study participants would still have been diagnosed as highly symptomatic at study exit (Table 2). Furthermore, after 12 weeks, 90% of participants had achieved a clinically meaningful improvement of at least three points in CLDEQ-8 scores compared to their baseline score. This suggests that almost all soft CL wearers in this study achieved a clinically relevant improvement in comfort after using lifitegrast for 12 weeks, further underscoring the potential of lifitegrast when used by symptomatic CL wearers.27 Comfortable and total CL wear time are a frequently reported concern of symptomatic CL wearers, which may eventually even lead to discontinuation of lens wear.1 It was interesting to note that while participants did not necessarily wear their habitual lenses for longer periods each day, they reported significantly longer comfortable wear times as the study progressed. Mean total and comfortable CL wear times were 11.3 and 6 hours at the baseline and dispense visit and 11.5 and 9 hours at the 12-week follow-up visit, respectively. These data indicate two things – for one, the consistent total wear time of roughly 11.5 hours suggests that CL wearers, despite being symptomatic, typically follow a CL wear routine that aligns with their personal requirements (eg, during the whole workday, including travel to and from work) rather than just for the time lenses remain comfortable. However, and this is perhaps the more crucial finding of the two, the increase in comfortable wear time to nine hours now spans beyond the duration of a typical workday,33 which could be of particular benefit to CL wearers working in office environments.
The use of rewetting drops or artificial tears is often the first step in the management of symptomatic contact lens wearers,4,17 and the efficacy of OTC products to alleviate EOD discomfort has been extensively studied.34–38 Using a similar 100mm visual analog comfort scale, Barabino et al reported an improvement of roughly 25 points on a 0–100 VAS after three weeks of using preservative-free artificial tears containing 0.9% sodium chloride four times a day.34 A study that evaluated EOD comfort changes after using a lubricating drop (Systane Ultra; Alcon, Fort Worth, USA) found an improvement of 0.6 points on a 1–5 Likert based scale after two weeks compared to baseline levels.35 Pucker et al evaluated EOD comfort ratings (0–100 VAS) in three groups of symptomatic daily disposable contact lens wearers that either used an artificial tear product (Systane Complete; Alcon, Fort Worth, USA), a rewetting drop (Sensitive Eyes; Bausch & Lomb, Rochester, USA) or received no treatment. After two weeks of use, there was a significant improvement in EOD comfort levels for the group using the rewetting drop (24 points on the 0–100 scale) but not for the groups using the artificial tear product or who did not receive treatment.36 In this study, the use of lifitegrast 5.0% resulted in a similar or greater improvement for EOD dryness and discomfort levels after the same two weeks of use. Because the majority of studies investigating artificial tear or rewetting drop use in contact lens wearers were conducted over two- or three-week periods only,34–38 a direct comparison to the 6- and 12-week data from this study is not possible. However, considering that the significant improvements in EOD comfort and dryness while using lifitegrast were achieved in CL wearers that already used OTC eyedrops, it may be reasonable to expect greater symptom relief in CL wearers with moderate-to-severe EOD dryness when introducing lifitegrast into the treatment plan.
An interesting observation from this study was that the mean age of the study population in this study (30.8 years of age) was significantly lower than the mean participant age in the Phase III studies (58.7 and 58.8 years of age, respectively).21,22 While a younger age in CL wearers is not surprising, the severity of CL-wear related symptoms in many of these relatively young study participants emphasizes the need for clinicians to continuously monitor and address patient-reported symptoms of discomfort and dryness, for example, by modifying the lens wear modality or lens care product or introducing over-the-counter or prescription eye drops.
While using lifitegrast resulted in significant improvements in EOD symptom levels, no changes were observed for any of the clinical signs evaluated in this study. Neither the tear film stability metric NITBUT nor any of the ocular health variables (ocular redness, staining or palpebral redness and roughness) showed any clinically relevant changes over time, remaining stable throughout the study. Because these variables by no means represent all of the potential dry eye variables that have previously been used for the diagnosis and assessment of dry eye signs, it is not possible to address whether the use of lifitegrast in symptomatic contact lens wearers improves clinical signs. However, they do demonstrate that the use of lifitegrast does not impact the ocular surface integrity during CL wear. Future studies could further evaluate whether other clinical signs, such as corneal staining or tear osmolarity, improve when CL wearers use lifitegrast over prolonged periods.
Similarly, no changes in tear film inflammatory markers could be detected in this study. Previous studies had found an association between tear film inflammatory markers and CL wear,2,39,40 with both CL wear in general (vs no CL wear)39 and a less frequent replacement modality (reusable vs daily disposable)40 being reported to result in significantly higher tear film cytokine levels. In this study, six of the ten cytokines were not reliably detected at each visit, and for the four that were detected at each visit (IL-1β, IL-2, IL-6, and L-8), no statistically significant change over time was detected (Figure 6). A meta-analysis of the available literature suggests that there is a high heterogeneity in the levels of tear inflammatory mediators within the population,41 which, when coupled with their low concentration in tears and the need for sample dilution for the assay, likely contributed to the inability to reach conclusions regarding changes to their levels within this study. This finding would not seem to be caused by the use of lifitegrast but rather to the generally low amounts of tear volumes that could be collected from some of the study participants (Table 4). To be eligible for this study, participants were required to wear their lenses for at least five days per week and six hours per day, be current users of lubricating eyedrops and to experience a typical level of eye dryness at the end of the wear of 40 on the 0–100 scale despite using these eyedrops. These criteria resulted in a (perhaps “drier” than typical) population of highly motivated contact lens wearers who were able to wear their lenses for most days of the week while using OTC eyedrops. The tear collection data in Table 4 support this assumption, with very similar tear volumes and number of available tear samples at baseline (prior to lifitegrast use) and throughout the 12-week study (during lifitegrast use).
In addition to being an effective treatment for symptomatic CL wearers, the findings of this study also indicated that lifitegrast could be safely used by the CL wearers in this study. There were no clinically relevant changes in visual acuity or for any of the anterior eye health variables that were assessed during the slit-lamp biomicroscopy examinations over the course of the study. There were only two adverse events that were attributed to the use of lifitegrast, with one leading to withdrawal of consent. None of the remaining 12 adverse events were related to the study drop use.
The experience from this study also showed that the thorough review of the instructions for use of lifitegrast29 was crucial to adequately set the participant’s expectations with regard to the expected benefits and side effects they may experience while using lifitegrast in this study. Prior to signing the informed consent, the volunteer participants were made aware of the potential side effects of using lifitegrast, such as the occurrence of dysgeusia, tearing and intermittent instillation site irritation, discomfort or blurred vision. These were again reviewed at the time of the dispense visit, where the patient medication information handout29 was reviewed with the participant to ensure proper use of the drops and to remind them of the most common side effects. It was interesting to observe that participants rarely reported on the experience of any of the known and documented side effects; exceptions to this were occasional mentions of temporary dysgeusia or instillation site irritation which were not classified as adverse events due to them being expected and short-term. It appears that taking the time to review the side effects with patients could be a very useful component in the clinician’s toolkit when prescribing lifitegrast to their patients.
The open-label study design, with no control treatment arm, leaves room for criticism due to the potential for placebo effects from the newly introduced treatment. All of the participants had to have used rewetting drops or similar eye drops at least once in the month prior to the screening visit; while this confirms familiarity with the use of eye drops, only 30% of all study participants used their habitual eye drops in the same daily frequency (twice per day) as required for the study, while the remaining 70% either had to increase (62%) or decrease (8%) their daily use frequency. It is possible that the more frequent use of the lifitegrast eye drops in this study for roughly 60% of the participants could have contributed to the reduction in symptoms that was found in this study.
With these limitations in mind, the overall study design was set out to keep changes to the habitual wear regimen of the study participants at a minimum. Hence, the only change to the participant’s CL wear routine in this study design was the use of lifitegrast drops twice a day throughout the study instead of any other OTC comfort enhancing drops, while habitual lens type and solution remained unchanged. With this study design, potentially confounding variables could be largely eliminated, and the study findings can be solely attributed to the introduction of lifitegrast eye drops into the wear routine. A second crucial component of the study design was that any kind of refractive error correction with soft CLs was permitted (eg, toric, spherical, monovision or multifocal). In contrast to the Gonzalez et al study,27 where only a single, reusable contact lens type was evaluated, the current study provides data for a wide variety of lens types (n=17) that included 26 daily disposable and 14 reusable CL wearers. Therefore, the findings from this study document the suitability of lifitegrast for the treatment of CL wear-related EOD dryness and discomfort in CL wearers for a large set of currently available CL hydrogel and silicone hydrogel lens types.
Conclusion
Using lifitegrast for as little as 2 weeks resulted in significant improvements in symptoms of EOD dryness and discomfort and a longer comfortable wear time, which further improved with continued use of lifitegrast during the 12-week study. Lifitegrast may be a suitable alternative for symptomatic CL wearers who cannot achieve satisfactory comfort and dryness with alternate CLs or over-the-counter comfort enhancing drops.
Abbreviations
2W, 2 weeks; 6W, 6 weeks; 12W, 12 weeks; BL, Baseline; CL, contact lens; CLD, contact lens discomfort; CLDEQ-8, Contact Lens Dry Eye Questionnaire – 8; DED, dry eye disease; EOD, end-of-day; ICAM-1, intercellular adhesion molecule-1; LFA-1, lymphocyte function-associated antigen-1; OTC, over-the-counter; TFOS, Tear Film and Ocular Surface Society; VA, visual acuity; VAS, visual analog scale.
Data Sharing Statement
The datasets generated and analysed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to thank Dr Robin Chalmers and Dr Carolyn Begley for their permission to use the CLDEQ-8 questionnaire in this study.
Funding
This was an investigator-initiated study. Funding was received from Novartis and Bausch+Lomb. With the investigator initiated study design, while Novartis and Bausch+Lomb provided funding, they had no influence in study design, manuscript preparation or analysis.
Disclosure
All authors are affiliated with CORE. Over the past three years, CORE has received research funding and/or honoraria from Alcon, Avizor, Azura Ophthalmics, Bausch + Lomb, CooperVision, Essilor, Euclid, Hoya, i-Med Pharma, Integral Biosystems, J&J Vision, Macumira, Menicon, Myoptechs, Novartis, Ophtecs, Pleryon, Scope Ophthalmics, SightGlass, Topcon and Visioneering Tech Inc. In addition, L Jones is a consultant and/or serves on an advisory board for Alcon, CooperVision and Ophtecs. The authors report no other conflicts of interest in this work.
References
1. Nichols KK, Redfern RL, Jacob JT, et al. The TFOS international workshop on contact lens discomfort: report of the definition and classification subcommittee. Investigat Opthalmol Vis Sci. 2013;54(11):TFOS14. doi:10.1167/iovs.13-13074
2. Stapleton F, Bakkar M, Carnt N, et al. BCLA CLEAR - contact lens complications. Contact Lens Anterior Eye. 2021;44(2):330–367. doi:10.1016/j.clae.2021.02.010
3. Dumbleton K, Caffery B, Dogru M, et al. The TFOS international workshop on contact lens discomfort: report of the subcommittee on epidemiology. Invest Ophthalmol Visual Sci. 2013;54(11):TFOS20–TFOS36. doi:10.1167/iovs.13-13125
4. Begley CG, Chalmers RL, Mitchell GL, et al. Characterization of ocular surface symptoms from optometric practices in North America. Cornea. 2001;20(6):610–618. doi:10.1097/00003226-200108000-00011
5. Pucker AD. A review of the compatibility of topical artificial tears and rewetting drops with contact lenses. Contact Lens Anterior Eye. 2020;43(5):426–432. doi:10.1016/j.clae.2020.04.013
6. Chalmers RL, Begley CG, Moody K, Hickson-Curran SB. Contact Lens Dry Eye Questionnaire-8 (CLDEQ-8) and opinion of contact lens performance. Optometry Vision Sci. 2012;89(10):1435–1442. doi:10.1097/OPX.0b013e318269c90d
7. Pucker AD, Tichenor AA. A review of contact lens dropout. Clin Optom. 2020;Volume 12:85–94. doi:10.2147/OPTO.S198637
8. Maldonado‐Codina C, Navascues‐Cornago M, Smith SL, Read ML, Lakkis C, Morgan PB. End‐of‐day assessment of asymptomatic versus highly symptomatic soft contact lens wearers. Ophthalmic Physiol Opt. 2024;44(4):704–717. doi:10.1111/opo.13305
9. McMonnies CW. An amplifying cascade of contact lens-related end-of-day hyperaemia and dryness symptoms. Current Eye Research. 2018;43(7):839–847. doi:10.1080/02713683.2018.1457163
10. Efron N. Contact lens wear is intrinsically inflammatory. Clin Exp Optom. 2017;100(1):3–19. doi:10.1111/cxo.12487
11. Willcox MD. Is there a role for inflammation in contact lens discomfort? Eye Contact Lens. 2017;43(1):5–16. doi:10.1097/icl.0000000000000343
12. Efron N. Is contact lens wear inflammatory? Br J Ophthalmol. 2012;96(12):1447–1448. doi:10.1136/bjophthalmol-2012-302075
13. Rueff EM. Visual discomfort and contact lens wear: a review. Contact Lens Anterior Eye. 2023;46(4):101872. doi:10.1016/j.clae.2023.101872
14. Dumbleton K, Woods CA, Jones LW, Fonn D. The impact of contemporary contact lenses on contact lens discontinuation. Eye Contact Lens. 2013;39(1):93–99. doi:10.1097/ICL.0b013e318271caf4
15. Richdale K, Sinnott LT, Skadahl E, Nichols JJ. Frequency of and factors associated with contact lens dissatisfaction and discontinuation. Cornea. 2007;26(2):168–174. doi:10.1097/01.ico.0000248382.32143.86
16. Jones L, Brennan NA, González-Méijome J, et al. The TFOS international workshop on contact lens discomfort: report of the contact lens materials, design, and care subcommittee. Investigat Opthalmol Vis Sci. 2013;54(11):TFOS37. doi:10.1167/iovs.13-13215
17. Chalmers R, Long B, Dillehay S, Begley C. Improving contact-lens related dryness symptoms with silicone hydrogel lenses. Article Optometry Vision Sci. 2008;85(8):778–784. doi:10.1097/OPX.0b013e318181a90d
18. Riley C, Young G, Chalmers R. Prevalence of ocular surface symptoms, signs, and uncomfortable hours of wear in contact lens wearers: the effect of refitting with daily-wear silicone hydrogel lenses (senofilcon a). Eye Contact Lens. 2006;32(6):281–286. doi:10.1097/01.icl.0000224522.04723.7a
19. Stahl U, Willcox M, Stapleton F. Role of hypo-osmotic saline drops in ocular comfort during contact lens wear. Contact Lens Anterior Eye. 2010;33(2):68–75. doi:10.1016/j.clae.2010.01.001
20. Caffery B, Pucker AD, Chidi-Egboka NC, et al. Lubricating drops for contact lens discomfort in adults. Cochrane Database Syst Rev. 2024;9(9):Cd015751. doi:10.1002/14651858.CD015751.pub2
21. Holland EJ, Luchs J, Karpecki PM, et al. Lifitegrast for the treatment of dry eye disease: results of a phase III, randomized, double-masked, placebo-controlled trial (OPUS-3). Ophthalmology. 2017;124(1):53–60. doi:10.1016/j.ophtha.2016.09.025
22. Tauber J, Karpecki P, Latkany R, et al. Lifitegrast ophthalmic solution 5.0% versus placebo for treatment of dry eye disease: results of the randomized phase III OPUS-2 study. Ophthalmology. 2015;122(12):2423–2431. doi:10.1016/j.ophtha.2015.08.001
23. Li JX, Tsai YY, Lai CT, Li YL, Wu YH, Chiang CC. Lifitegrast ophthalmic solution 5% is a safe and efficient eyedrop for dry eye disease: a systematic review and meta-analysis. J Clin Med. 2022;11(17). doi:10.3390/jcm11175014
24. Atallah RT, Castanos MV, Najac R, Donnenfeld E. Six months’ treatment with lifitegrast in patients with moderate-to-severe symptomatic dry eye: a retrospective chart review. Clin Ophthalmol. 2019;13:1033–1037. doi:10.2147/OPTH.S191635
25. Zhong M, Gadek TR, Bui M, et al. Discovery and development of potent LFA-1/ICAM-1 antagonist SAR 1118 as an ophthalmic solution for treating dry eye. ACS Med Chem Lett. 2012;3(3):203–206. doi:10.1021/ml2002482
26. Sun Y, Zhang R, Gadek TR, O’Neill CA, Pearlman E. Corneal inflammation is inhibited by the LFA-1 antagonist, lifitegrast (SAR 1118). J Ocul Pharmacol Ther. 2013;29(4):395–402. doi:10.1089/jop.2012.0102
27. Gonzalez A. Safety and efficacy of lifitegrast 5% ophthalmic solution in contact lens discomfort. Clin Ophthalmol. 2018;Volume 12:2079–2085. doi:10.2147/opth.s184776
28. Young G, Chalmers R, Napier L, Kern J, Hunt C, Dumbleton K. Soft contact lens-related dryness with and without clinical signs. Optometry Vision Sci. 2012;89(8):1125–1132. doi:10.1097/OPX.0b013e3182640af8
29. Novartis. Xiidra Lifitegrast Ophthalmic Solution - Product Monograph Including Patient Medication Information; 2019.
30. Papas EB, Keay L, Golebiowski B. Estimating a just-noticeable difference for ocular comfort in contact lens wearers. Invest Ophthalmol Visual Sci. 2011;52(7):4390–4394. doi:10.1167/iovs.10-7051
31. Navascues-Cornago M, Guthrie S, Morgan PB, Woods J. Determination of the Minimal Clinically Important Difference (MCID) for ocular subjective responses. Trans Vision Sci Technol. 2024;13(8):28. doi:10.1167/tvst.13.8.28
32. Chalmers RL, Keay L, Hickson-Curran SB, Gleason WJ. Cutoff score and responsiveness of the 8-item Contact Lens Dry Eye Questionnaire (CLDEQ-8) in a Large daily disposable contact lens registry. Contact Lens Anterior Eye. 2016;39(5):342–352. doi:10.1016/j.clae.2016.04.005
33. Bureau of Labor Statistics - US Department of Labor. American time use survey - 2023 results 04 March 2025. 2025. Available from: https://www.bls.gov/news.release/pdf/atus.pdf.
34. Barabino S, Rolando M, Camicione P, Chen W, Calabria G. Effects of a 0.9% sodium chloride ophthalmic solution on the ocular surface of symptomatic contact lens wearers. Can J Ophthalmol. 2005;40(1):45–50. doi:10.1016/S0008-4182(05)80116-4
35. McDonald M, Schachet JL, Lievens CW, Kern JR. Systane® ultra lubricant eye drops for treatment of contact lens–related dryness. Eye Contact Lens. 2014;40(2):106–110. doi:10.1097/ICL.0000000000000018
36. Pucker AD, McGwin G, Franklin QX, Dubey J, Nattis A, Lievens C. Application of systane complete for the treatment of contact lens discomfort. Contact Lens Anterior Eye. 2021;44(4):101399. doi:10.1016/j.clae.2020.12.004
37. Kading D. A two-week clinical evaluation of the safety of systane ultra in contact lens-wearing patients. Clin Ophthalmol. 2010;4:27–32. doi:10.2147/opth.s8079
38. Pucker AD, McGwin G, Franklin QX, Nattis A, Lievens C. Evaluation of systane complete for the treatment of contact lens discomfort. Contact Lens Anterior Eye. 2020;43(5):441–447. doi:10.1016/j.clae.2019.10.141
39. Schultz CL, Kunert KS. Interleukin-6 levels in tears of contact lens wearers. J Interferon Cytokine Res. 2000;20(3):309–310. doi:10.1089/107999000312441
40. Chao C, Stapleton F, Willcox MDP, Golebiowski B, Richdale K. Preinflammatory signs in established reusable and disposable contact lens wearers. Optometry Vision Sci. 2017;94(11):1003–1008. doi:10.1097/OPX.0000000000001129
41. Roda M, Corazza I, Bacchi Reggiani ML, et al. Dry eye disease and tear cytokine levels-a meta-analysis. Int J Mol Sci. 2020;21(9):3111. doi:10.3390/ijms21093111
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.