Back to Journals » International Medical Case Reports Journal » Volume 18
A Challenging Case of MOG-Associated Optic Neuritis: The Role of IL-6 Inhibition in Refractory Disease
Authors Alnajashi H ![]() , Alnahdi M
, Alnahdi M
Received 28 August 2025
Accepted for publication 2 December 2025
Published 6 December 2025 Volume 2025:18 Pages 1557—1560
DOI https://doi.org/10.2147/IMCRJ.S563753
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Hind Alnajashi,1,2 Mesedah Alnahdi2
1Neurology Department, King Abdulaziz University, Jeddah, Saudi Arabia; 2Neurology Department, King Abdulaziz University Hospital, Jeddah, Saudi Arabia
Correspondence: Hind Alnajashi, Neurology Department, King Abdulaziz University, Jeddah, Saudi Arabia, Tel +966 503369715, Email [email protected]
Abstract: We present a case of a 21-year-old woman diagnosed with myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD), characterized by recurrent optic neuritis and progressive vision loss. Despite multiple immunosuppressive therapies—including corticosteroids, intravenous immunoglobulin (IVIG), azathioprine, mycophenolate mofetil, and rituximab—the patient continued to experience disabling relapses, particularly during steroid tapering. Ongoing disease activity, combined with significant steroid-related side effects, prompted a trial of subcutaneous tocilizumab, an interleukin-6 (IL-6) receptor inhibitor. Following its introduction, the patient remained relapse-free, and her steroid dose was successfully reduced. This case highlights the complexity of managing refractory MOGAD and underscores the potential role of IL-6 inhibition in treatment-resistant cases. There are sparse reports about the use of subcutaneous tocilizumab (TCZ) in MOGAD, and this case contributes to the growing body of real-world evidence supporting its use. As no standardized treatment protocol currently exists, reporting such cases is vital for advancing future therapeutic strategies and guidelines.
Keywords: myelin oligodendrocyte glycoprotein antibody, tocilizumab, IL-6 inhibitor, demyelinating disease, optic neuritis
Introduction
Myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD) is a distinct form of central nervous system autoimmune disease, attributed to the presence of anti-MOG antibody. This condition presents with a spectrum of clinical manifestations, predominantly including optic neuritis and transverse myelitis, and acute disseminated encephalomyelitis (ADEM).
MOGAD is a rare demyelinating disease that can be observed in both adult and pediatric populations. It is more common in the pediatric population, making up to 30% of autoimmune central nervous system diseases, in contrast to only 5% in the adult population.1,2
The prevalence of the disease is not well described and varies worldwide; it ranges between 1.3 and 2.5 per 100,000.3
The disease course and prognosis are variable. Initially it was thought that it was a monophasic disease with a favorable prognosis; however, recent reports indicate that 35% of the cases are relapsing, with relapsing optic neuritis as the most common form. Permanent visual impairment and optic atrophy have been reported.1,4 Treatment for the acute phase depends mainly on steroid as the majority of the cases are steroid responsive. For severe cases and incomplete responses to steroid plasma exchange or intravenous immunoglobulin (IVIG), may be used.5 Long-term preventive therapy is still an area of exploration as there are no controlled clinical trials for approved treatment. In general, a long steroid taper is recommended in most cases to prevent early relapses.1,3 There is no clear guideline on who will need long-term preventive therapy and what is the best type of immunosuppressive therapy or steroid-sparing agent. The most commonly used first-choice treatment may be rituximab, azathioprine or mycophenolate mofetil, either by itself or in conjunction with a low-dose steroid. However, in the event of an inadequate response, there are no explicit guidelines for switching or escalating.6 Since there is no controlled trial, the treatment option is based on clinical experience and reported cases.
In this case we try to present a challenging case of refractory MOGAD that responded well to uncommonly used treatment IL-6 antagonist tocilizumab.
Case Presentation
The patient was a previously healthy 21-year-old female with no notable family history of autoimmune or hereditary conditions. In January 2017, she presented with a mild febrile illness, which rapidly progressed to altered consciousness. Initially, she was diagnosed with meningoencephalitis. However, her condition worsened despite therapy, prompting further investigation.
Upon further investigation, cerebrospinal fluid (CSF) analysis showed mild inflammation with negative bacterial and viral serologies and culture. Brain MRI revealed diffuse hyperintense lesions, suggesting a diagnosis of acute disseminated encephalomyelitis (ADEM). Figure 1. She was treated with intravenous immunoglobulin (IVIG) and pulse steroids, which led to improvement over a couple of weeks. After this, she was discharged on a tapering dose of oral steroids over 1 month.
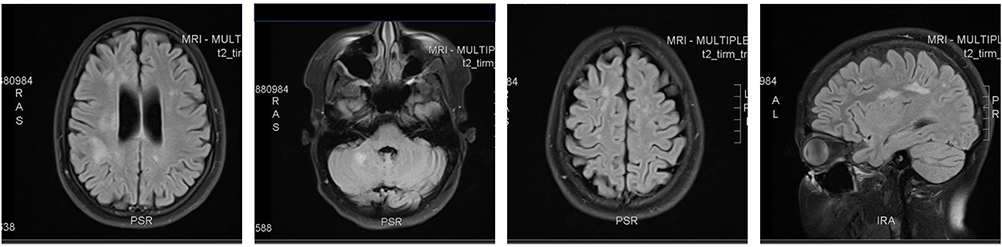 |
Figure 1 FLAIR image of brain MRI demonstrating hyperintense lesions involving bilateral subcortical white matter and infratentorial. Abbreviations: MRI, magnetic resonance imaging; FLAIR, fluid-attenuated inversion recovery. |
In the months following, the patient experienced several episodes of relapsing optic neuritis; all these episodes were steroid sensitive. First attack in April 2017 the patient developed right eye optic neuritis and responded to steroids. One month later, she had an episode of bilateral optic neuritis. The MRI at that time did not show new lesions with resolution of some old lesions. She received pulse steroids and high dose oral prednisone with partial improvement. August 2017—she was treated with plasma exchange and prednisone 1 milligram/kilogram (her weight 70 kilogram). Visual evoked potential showed no response in both eyes. Around this time the MOG antibodies came back positive on the live-based cell assay 1:100 and the patient was started on azathioprine titating to 2 mg/Kg and a slow taper of prednisone. In early 2018-reached 20 mg of prednisone but developed another optic neuritis relapse and had to increase the dose again and was on azathioprine 150 mg at that time. July 2018 she was on 10 mg of prednisone but had blurred vision and worsening right eye vision. The vision on the right eye at that time was 20/200 and on the left was 20/20. Plasma exchange was done for a total of 5 sessions, and the prednisone dose was increased. November 2018 had another relapse on the left eye after reducing the dose to 20 mg of prednisone. The exam showed worsening vision in the right eye was 20/70 and the left eye, 20/200 with optic atrophy in the left eye. At that time prednisone was increased to 60 mg daily and the patient was started on rituximab. However, at 4 months post-rituximab, vision deteriorated again in the left eye with only hand motion and count fingers in the right eye despite the B-cell response was good, with complete depletion of CD19-positive cells at 0%. This was considered as rituximab failure. She was treated with steroids and then IVIG 2 grams/kilogram initially and then 1 gram/kilogram every 3 weeks with a plan for mycophenolate mofetil MMF a 1000 mg twice daily and another trial of a slow prednisone taper. The patient continued on IVIG 1 gram/kilogram every 3–4 weeks in addition to mycophenolate and prednisone at fluctuating doses between 35 and 20 mg since May of 2019. The patient required increasing doses of prednisone when there would be decreased vision or pain in the eye. In early 2022, the patient reached 10 mg of prednisone, but there was a global shortage of IVIG, and she missed 4 doses between October 2021 and February 2022 and presented with right eye pain and decreased visual acuity. In the left eye, the acuity was 20/100 in 1 eye and count fingers in the other eye. Plasma exchange was offered, and the steroid was increased to 1 milligram/kilogram. After that, the patient was started on subcutaneous immunoglobulin. Every 2 weeks, but she developed optic neuritis in one eye, which was managed successfully with pulse steroids. However, she had a more severe episode of bilateral optic neuritis, requiring both pulse and oral steroids. No new lesions were seen on MRI, and some previous lesions had resolved.
Despite being on bimonthly subcutenous IVIG and MMF the patient had significant vision loss and recurrent relapse whenever steroid is tapered below 20 mg. As a complication of chronic steroid use, she developed osteoporosis, significant weight gain, and skin changes. Repeated anti-MOG testing showed persistent positive results at titre 1:100.
Treatment and Management
By March 2023, due to the ongoing relapses and side effects from long-term steroid use, we decided to start Tocilizumab (TCZ), an IL-6 receptor blocker. Doses were started as subcutaneous injections of 162 mg every other week for the first 2 months, then weekly with a slow steroid taper. Since then, the patient has remained stable, with no further relapses, and her steroid dose was reduced to 5 mg daily. The decision to start subcutenous TCZ rather than intervenous was to provide more convenient treatment for the patient. The patient still has residual visual impairment from previous attacks, but no acute worsening of vision or eye pain. Her last visual assessment showed acuity 20/100 in right eye and count fingers in the left eye. TCZ was well tolerated with transient elevation of lipid profile managed with lifestyle modification. Discussions around pregnancy and the effects of immunosuppressive therapies on pregnancy will also be an important part of her long-term care, as the patient is young and wishes to have kids after her disease stabilization.
Discussion
MOGAD is a rare but complex neuroimmunological disorder that can cause recurrent optic neuritis and other demyelinating events. Treatment of MOGAD is challenging, while some cases are monophasic and require no long term therapy others are left with significant residual disability or a relapsing course necessitating long-term treatment. To date, no randomized controlled trial for MOGAD treatment.7
Steroid use can cause multiple side effects, including osteoporosis, hypertension and weight gain. Azathioprine and Mycophenolate mofetil work occasionally. IV Ig showed promising results, especially in paediatric cases. While rituximab has good results in controlling disease activities in NMO and MS it has been less effective in MOGAD.8
Tocilizumab (TCZ), a humanized antibody directed against the IL-6 receptor that has been used widely in rheumatological disease, has emerged as a promising option in MOGAD. MOGAD pathophysiology involves microglial activation and inflammation triggered by Interleukin-6 (IL-6) release. Therefore, blocking IL-6 could control disease activity in MOGAD and stop demyelination.9 Few case reported the use of intravenous form of TCZ for MOGAD cases that were refractory to other treatment options.9,10 Our case presented the use of the subcutaneous (SC) form of TCZ, which can provide the advantage of convenient home administration in comparison with IV form. To our knowledge, reports focusing on the use of SC TCZ are lacking. In rheumatoid arthritis, SC and IV tocilizumab have comparable efficacy and safety profiles.11 Reporting the safety and effectiveness of TCZ various form IV and SC as off label treatment in MOGAD are really important to help accumulating evidence that can help in treatment guidelines and recommendations in the future.
This case also highlights the broader challenges in managing MOGAD Since, MOGAD is an evolving disease treatment selection, duration of treatment are still unanswered questions.
Conclusion
This case illustrates the challenges faced in managing MOG-associated disease, particularly when patients are dependent on steroids and relapses continue despite conventional treatments. The introduction of SC TCZ as a steroid-sparing agent has provided significant improvement in this patient’s disease course, highlighting its potential role in managing refractory MOGAD. While further research is needed to refine treatment protocols for MOGAD, this case offers hope for improved outcomes and quality of life for patients struggling with this complex disease. Since there is no clear guideline for the duration of treatment, young female patients who may encounter long-term considerations, such as fertility and the effects of immunosuppressive medications on pregnancy, provide extra hurdles. Consequently, considerations regarding the long-term implications of treatment are essential.
Consent
Written informed consent was obtained from the patient for publication of this case report. Institutional approval was not required for this single-patient case report.
Acknowledgments
The authors have nothing to report.
Disclosure
The authors declare no conflicts of interest. A preprint version of this article is available on Authorea (DOI: 10.22541/au.175325063.33744398/v1).
References
1. Gklinos P, Dobson R. Myelin oligodendrocyte glycoprotein-antibody associated disease: an updated review of the clinical spectrum, pathogenetic mechanisms and therapeutic management. Antibodies. 2024;13(2):43. doi:10.3390/antib13020043
2. Al-Ani A, Chen JJ, Costello F. Myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD): current understanding and challenges. J Neurol. 2023;270(8):4132–4150. doi:10.1007/s00415-023-11737-8
3. Hor JY, Fujihara K. Epidemiology of myelin oligodendrocyte glycoprotein antibody-associated disease: a review of prevalence and incidence worldwide. Front Neurol. 2023;14. doi:10.3389/fneur.2023.1260358
4. Hegen H, Reindl M. Recent developments in MOG-IgG associated neurological disorders. Ther Adv Neurol Disord. 2020;13:1756286420945135. doi:10.1177/1756286420945135
5. Ambrosius W, Michalak S, Kozubski W, Kalinowska A. Molecular sciences myelin oligodendrocyte glycoprotein antibody-associated disease: current insights into the disease pathophysiology, diagnosis and management. Int J Mol Sci. 2021;22:100. doi:10.3390/ijms22010100
6. Whittam DH, Karthikeayan V, Gibbons E, et al. Treatment of MOG antibody associated disorders: results of an international survey. J Neurol. 2020;267(12):3565. doi:10.1007/s00415-020-10026-y
7. Cobo-Calvo A, Ruiz A, Maillart E, et al. Clinical spectrum and prognostic value of CNS MOG autoimmunity in adults. Neurology. 2018;90(21):e1858–69. doi:10.1212/WNL.0000000000005560
8. Hamid S, Palace J, Messina S, et al. Clinical presentation and prognosis in MOG-antibody disease: a UK study. Brain. 2017;140(12):3128–3138. doi:10.1093/brain/awx276
9. Schirò G, Iacono S, Andolina M, Bianchi A, Ragonese P, Salemi G. Tocilizumab treatment in MOGAD: a case report and literature review. Neurological Sciences. 2023;45(4):1429. doi:10.1007/s10072-023-07189-7
10. Elsbernd PM, Hoffman WR, Carter JL, Wingerchuk DM. Interleukin-6 inhibition with tocilizumab for relapsing MOG-IgG associated disorder (MOGAD): a case-series and review. Mult Scler Relat Disord. 2021;48:102696. doi:10.1016/j.msard.2020.102696
11. Lauper K, Mongin D, Iannone F, et al. Comparative effectiveness of subcutaneous tocilizumab versus intravenous tocilizumab in a pan-European collaboration of registries. RMD Open. 2018;4(2):e000809. doi:10.1136/rmdopen-2018-000809
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.