Back to Journals » International Medical Case Reports Journal » Volume 18
A Challenging Approach: Iris Neovascularization and Vitreous Hemorrhage 40 Years after Treatment of Retinal Giant Tear Detachment
Authors Kreissig I, Mennel S
Received 3 July 2025
Accepted for publication 3 September 2025
Published 15 September 2025 Volume 2025:18 Pages 1211—1214
DOI https://doi.org/10.2147/IMCRJ.S548958
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ingrid Kreissig,1 Stefan Mennel2
1Department of Ophthalmology, Medical Faculty Mannheim of the Ruprecht-Karls-University Heidelberg, Mannheim, Germany; 2Department of Ophthalmology, Phillips-University Marburg, Marburg, Germany
Correspondence: Ingrid Kreissig, Universitäts-Augenklinik, Theodor-Kutzer-Ufer, Mannheim, 68167, Germany, Email [email protected]
Background: Iris neovascularization and vitreous hemorrhages are typical sequels of ischemic retinopathies. Here, we report about a patient who developed marked iris neovascularization without signs of posterior retinal ischemia.
Case Presentation: A 56-year-old patient developed marked iris neovascularization after surgery for rhegmatogenous retinal detachment due to a giant retinal tear had been performed 40 years earlier. With repeatedly applied intravitreal injections of an anti-VEGF drug being unsuccessful, anterior retinal cryocoagulations with deep indentation by the cryoprobe to somehow touch and coagulate the detached anterior flap of giant tear were carried out. Subsequently, the vitreous hemorrhage cleared without any further intervention, and iris neovascularization subsided. Retinal fluorescein angiogram did not reveal signs of ischemia of the attached central retina.
Conclusion: Marked iris neovascularization can disappear after applying peripheral retinal cryocoagulation and laser coagulation. It may lead to the question whether neovascular AMD, potentially associated with macular ischemia, might theoretically be addressable by ablative procedures of the peripheral retina.
Keywords: iris neovascularization, rubeosis iridis, vitreous hemorrhage, ischemic retinopathy, intravitreal anti-VEGF injections, retinal cryo- and lasercoagulation
Iris neovascularization and vitreous hemorrhages are typical sequels of ischemic retinopathies, such proliferative diabetic retinopathy, ischemic central retinal vein occlusion, and ischemic ophthalmopathy, to name only a few.1,2 Together with their underlying disease, they have usually been treated by intravitreal applications of anti-vascular endothelial growth factor (VEGF) antibodies.3,4 We here report about a patient who developed marked rubeosis iridis (iris neovascularization) in his eye without signs of posterior retinal ischemia. Since it is a retrospective description of the clinical course of a disorder taken care in clinical routine, approval by an ethics committee was not necessary.
The 56-year-old male patient in good general health presented with a sudden loss in vision to light perception in a painful eye. Consent was obtained from the patient to publish the case details. Slit-lamp examination of the anterior segment revealed a marked rubeosis iridis, aphakia, hyphema and vitreous hemorrhage without a view to the ocular fundus. The intraocular pressure (IOP) was 35 mm Hg. Upon sonography, the retina was attached. Duplex sonography of the carotid arteries was unremarkable, and both vertebral arteries showed an orthograde perfusion. The patient was under topical anti-glaucomatous therapy due to primary open-angle glaucoma in this eye.
Forty years earlier, this eye had undergone rhegmatogenous retinal detachment surgery due to a giant retinal tear extending over 165° from 8 o´clock through 12 o´clock to 3:30 o´clock. There was no preceding ocular trauma. The flap was overhanging. Two additional retinal horseshoe tears with collateral retinal detachment and an equatorial retinal lattice degeneration were detected in the inferior fundus periphery (Figure 1). The treatment of this detachment consisted in small steps: first of a retinal argon laser coagulation applied to the attached posterior edge of one of the inferior horseshoe tears and of the inferior lattice degeneration; second with the small gas bubble technique, by applying the balloon-gas procedure, 0.8 mL of C3H8 could be injected without drainage and being combined with a backwards rotation of the patient for unfolding the overhanging flap.5,6 After the posterior flap of the giant tear got unfolded and the gas bubble had reached a larger volume of about 3.2 mL; third the posterior edge of the giant tear was reattached by the enlarged gas bubble and treated with transscleral retinal cryopexy, and forth a radial scleral buckle with transscleral retinal cryopexy, limited to the two inferior horseshoe tears and without drainage, was applied (Figure 2). The cryopexy spots were applied under ophthalmoscopical control for a duration of about 3 seconds. The cryo procedure was stopped as soon as the retinal tissue started to whiten due to the freezing effect. Visual acuity improved to 20/30 at two months after surgery and eventually to 20/25 at four years later.
 |
Figure 1 Schematic drawing of the retinal detachment including the superior giant tear posterior to the equator with irregular edges and overhanging posterior flap, and two inferior retinal horseshoe tears with collateral retinal detachment; the “x” in the image center marks the foveola (From: Kreissig I: A Practical Guide to Minimal Surgery for Retinal Detachment: Part 2, 2000, pg 205, Figure 10.37a with permission of Thieme Stuttgart, New York Publisher). |
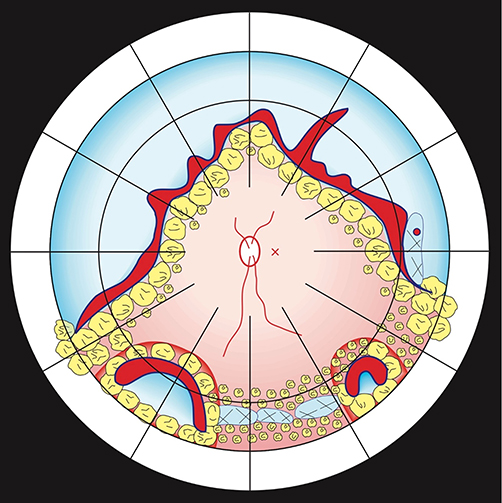 |
Figure 2 Schematic drawing of the retina after therapy of the retinal giant tear detachment as shown in Figure 1. This included laser coagulation to the attached posterior edge of one horseshoe tear and to the lattice degeneration; intraocular gas injection to unfold the inverted and overhanging retinal flap; multiple cryocoagulations and laser applications to fixate the re-attached posterior edge of the giant tear; and eventual application of a segmental buckle and cryopexy to the two inferior horseshoe tears; the “x” in the image center marks the foveola. (From: Kreissig I: A Practical Guide to Minimal Surgery for Retinal Detachment: Part 2, 2000, pg 207, Figure 10.37b with permission of Thieme Stuttgart, New York Publisher). |
As first treatment for this painful eye, three intravitreal injections of an anti-VEGF drug were applied, however with only a temporary decrease of iris neovascularization. IOP remained elevated despite topical and systemic anti-glaucomatous medical therapy including carboanhydrase inhibitors. At that moment the patient, whose giant tear detachment surgeon I was, contacted me and thus, I got involved into the treatment of this difficult eye. I recalled an earlier report from 1994, applying anterior pancryopexy in eyes with a high grade rubeosis iridis and vitreous hemorrhage which resulted in a decrease of rubeosis iridis from stage 4 to 1 and with resolving of the vitreous hemorrhage.7 This approach was used as treatment for this eye with massive rubeosis iridis and vitreous hemorrhage, ie, the anti-VEGF-injections were discontinued and instead anterior pancryopexy coagulations discussed. The rational for this was that somewhere in this eye an area of ischemic retina must exist causing the massive rubeosis iridis. It was considered that the reason for the rubeosis iridis could be located in the large detached anterior flap of the giant tear. Therefore, anterior cryocoagulations were carried out with the intention to coagulate the detached anterior flap of the giant tear by the most possible deep indentation with the cryoprobe. Subsequently, the vitreous hemorrhage cleared without any further intervention, and the rubeosis iridis decreased. Now retinal laser coagulations could be added and were applied in the region of the attached retina, hereby preferably placed in the inferior area. A retinal fluorescein angiogram did not reveal any signs of ischemia or impaired blood perfusion of the central retina. IOP returned to normal values under the earlier applied topical anti-glaucomatous therapy due to primary open-angle glaucoma. Visual acuity improved to 2/20 at two years of follow-up. An internal medical examination did not reveal any hint of an internal carotid artery stenosis or occlusion.
The clinical course and observations suggest that the ischemic areas may have eventually developed in parts of the retina peripheral to the former giant retinal tear, apparently within the large detached flap, leading to the rubeosis iridis and IOP elevation. The destruction of peripheral retinal tissue by anterior pancryocoagulation by deep indentation with the cryoprobe and subsequent retinal laser coagulation led to the sufficient resolution of the peripheral retinal ischemia as source of VEGF and of the secondary iris neovascularization. The findings may make one thinking that in clinical situations in which repeated intravitreal anti-VEGF injections did not result in a permanent disappearance of iris neovascularization, then cryo- or lasercoagulation of peripheral retina may be considered.
Based on this experience that a marked rubeosis iridis can disappear by peripheral retinal cryo- and laser coagulation (as shown in the clinical course of the patient presented in this report), one may question and start to re-think over the treatment of neovascular age-related macular degeneration (AMD). The secondary macular choroidal neovascularization in neovascular AMD may perhaps indicate ischemia within the highly specialized macular tissue which is most sensitively reacting to nutritive deficiencies and therefore, instead by frequent intravitreal injections of anti-VEGF drugs, this may be addressable by extensive ablative procedures of the peripheral retina, applied with laser- or transconjunctival cryocoagulation, as also mentioned by Mansour et al.8 Our presented challenging concept may perhaps initiate further research and studies to analyze the present treatment of neovascular AMD or to analyze the occurrence of neovascular AMD in diabetic eyes after panretinal photocoagulation (PRP) or in eyes after a retinal detachment with a prolonged macula off resulting in the reduction of the cones in this area, the most sensitive photoreceptors. This was described as manifesting in a reduction of color vision and visual acuity.9,10 The suggested ablative procedures of the peripheral retina might just cause a reduction of the over-all nutritive need for the entire retina, which in case of an AMD might be in favor of the jeopardized macula.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lee P, Wang CC, Adamis AP. Ocular neovascularization: an epidemiologic review. Surv Ophthalmol. 1998;43(3):245–269. doi:10.1016/s0039-6257(98)00035-6
2. Antonetti DA, Silva PS, Stitt AW. Current understanding of the molecular and cellular pathology of diabetic retinopathy. Nat Rev Endocrinol. 2021;17(4):195–206. doi:10.1038/s41574-020-00451-4
3. Rosenfeld PJ, Brown DM, Heier JS, et al; MARINA Study Group. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419–1431. doi:10.1056/NEJMoa054481
4. Wells JA, Glassman AR, Ayala AR, et al; Diabetic Retinopathy Clinical Research Network. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N Engl J Med. 2015;372(13):1193–1203. doi:10.1056/NEJMoa1414264
5. Lincoff H, Kreissig I. Modifizierte Gasblasentechnik zur Behandlung eines umgeschlagenen Riesenrisses. A modified gas bubble technique for treating an overhanging flap of a giant tear. Klin Mbl Augenheilk. 1982;180:29–34. doi:10.1055/s-2008-1055007
6. Kreissig I. The balloon-gas-procedure: another move towards minimum surgery. Dev Ophthal. 1987;13:99–106.
7. Kreissig I, Türmer KH, Hipp E. The management of persistent vitreous hemorrhage in the diabetic eye by pancryopexy: clinical study with longterm follow-up. Greek Ann Ophthalmol. 1994;31(2–3):165–171.
8. Mansour AM, Tripathy K, Parodi MB. A hypothetical therapeutic effect of light peripheral panretinal photocoagulation in neovascular age-related macular degeneration. Med Hypothesis Discov Innov Ophthalmol. 2022;11:137–143. doi:10.51329/mehdiophthal1457
9. Kreissig I. Prognosis of return of macular function after retinal reattachment. Mod Probl Ophthalmol. 1977;18:415–442.
10. Kreissig I, Lincoff H, Witassek B, Kolling G. Color vision and other parameters of macular function after retinal reattachment. Dev Ophthal. 1981;2:77–85.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.