Back to Journals » International Medical Case Reports Journal » Volume 18
A Case of Vasa Previa Diagnosed at Term: Elective Caesarean Section with Good Feto-Maternal Outcomes
Authors Nathania N ![]() , Gurnadi JI, Rinaldi A, Rahmanita T
, Gurnadi JI, Rinaldi A, Rahmanita T
Received 26 September 2024
Accepted for publication 27 November 2024
Published 21 January 2025 Volume 2025:18 Pages 145—150
DOI https://doi.org/10.2147/IMCRJ.S459911
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Video abstract presented by Nathania.
Views: 723
Nathania Nathania,1 Jeffry Iman Gurnadi,2 Andi Rinaldi,1 Triana Rahmanita1
1Department of Obstetrics and Gynecology, Universitas Padjadjaran, Bandung, Indonesia; 2Department of Obstetrics and Gynecology, Cibabat District Hospital, Cimahi, Indonesia
Correspondence: Nathania Nathania, Email [email protected]
Abstract: Vasa previa is a condition where unprotected fetal vessels, neither by placenta nor umbilical cord, lie within the membranes over the internal cervical ostium and beneath the presenting part of the fetus. Due to this condition, the membranous vessels pose a higher risk of being compressed or ruptures and could lead to fetal demise, exsanguination, or even fetal death. In this case report, we reported a case of a 36-year-old woman, G3P2A0, at term gestation and oblique lie. Early prenatal diagnosis using transvaginal ultrasound could increase the survival rate of the fetus if followed by sufficient management after diagnosis. Caesarean birth is the safest mode of delivery even before the clinical signs or onset of labor occur.
Keywords: vasa previa, early diagnosis, caesarean section
Introduction
Vasa previa is defined as a condition where unprotected fetal vessels, neither by placenta nor umbilical cord, lie within the membranes over the internal cervical ostium and beneath the presenting part of the fetus. Vasa previa comes from the Latin words, “vasa” means blood vessel, “prae” is before, and “via” means channel. Vasa previa is a rare condition, with incidence of 1 in 1,275–5,000 births.1 However, vasa previa needs special attention because of its high perinatal mortality rate during delivery, approximately 56% of all deliveries, especially when rupture of membranes occur.2 The high mortality rate can be reduced to zero if appropriate prenatal diagnosis is followed by appropriate management.3,4 Screening during antenatal care in the second and third trimesters using transvaginal ultrasound, colour flow mapping, and pulsed-wave Doppler to examine the blood vessel through the internal cervical ostium is an essential step.5,6 In this case report, we present a case of vasa previa that was detected early and treated appropriately resulting in good maternal and perinatal outcomes.
Materials and Methods
A case report of vasa previa in secondary health care in West Java, Indonesia.
Case Presentation
A 36-year-old woman, G3P2A0, was referred to secondary health care with term pregnancy and oblique lie. The general practitioner who referred this patient suspected other condition such as vasa previa due to an oblique lie in nonplacenta previa term pregnant patient. On transabdominal ultrasound examination we found the fetus was in oblique lie and the placenta was not covering the birth canal. We conducted a further method using transvaginal ultrasound and discovered the presence of fetal vessels within the chorio-amniotic membranes above the internal cervical ostium (Figure 1A and B). Pulsed-wave Doppler of the artery was correlated with the fetal heart rate (Figure 1C). These findings confirmed the diagnosis of vasa previa.
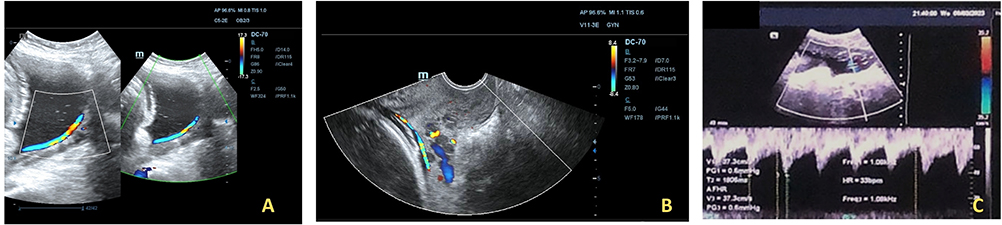 |
Figure 1 (A) A crossing blood vessel runs through the birth canal, (B) transvaginal ultrasonography, (C) Doppler examination (author’s personal collection). |
A male baby was born by an elective caesarean section, with a body weight of 2,910 grams and a body length of 48 cm with an APGAR score of 7 at the 1st minute and 9 at the 5th minute after birth. After the baby was delivered, the unprotected umbilical blood vessels were visible in the membranes and located above the internal cervical os across the internal ostium (Figure 2A and B). The placenta was delivered completely and observation was carried out. There were two placental lobules (bilobulated) with marginal umbilical cord insertion. There was a bridging vessel connecting the two placental lobules and caused vasa previa (Figure 3).
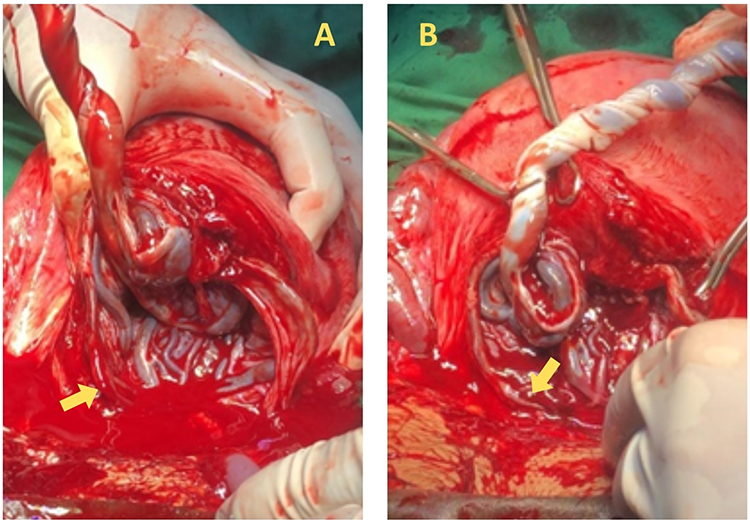 |
Figure 2 (A and B) Visible blood vessel (yellow arrow) runs through the birth canal during cesarean section (author’s personal collection). |
 |
Figure 3 Bilobulated placenta (yellow dotted line) with bridging blood vessel that connects the two lobules and causes vasa previa (blue arrow) (author’s personal collection). |
In this case, the diagnosis of type 2 vasa previa was confirmed after the gross examination of the placenta. The postoperation period was uneventful, with no complications and stable puerperium condition. The patient and the baby were discharged at the third postoperative day.
Discussion
Vasa previa is characterized by unprotected umbilical vessels running across the internal cervical ostium.5,7 Vasa previa is an uncommon condition, occurring in approximately 1 in 1,000–5,000 pregnancies.5 However, the perinatal mortality rate was found to be high due to the tear of the vessels during cervical dilation or membrane rupture.3 The etiology of vasa previa is still unknown,8 however the risk factors that are already known are diverse, such as twins or higher-order multiple gestation, umbilical cord infiltration (velamentous cord insertion, high risk of rupture or compression),6,9 low lying placenta or placenta previa, bilobulated placenta or succenturiate placenta and in vitro fertilization or other assisted reproductive technology.1,7 About 83% of vasa previa cases had at least one risk factor,7 as observed in this case. During operation, it is visible that the patient had a bilobulated placenta and marginal insertion of placental tissue. Multisegmented placenta was one of the main risk factor for vasa previa.1 A history of cesarean section or curettage was also considered as an indirect risk factor.7,8,10,11
Vasa previa can be classified into two distinct categories (Figure 4). Type 1 refers to the condition where the blood arteries of the umbilical cord or placenta, which are not protected, run through or near the cervical ostium (Figure 4A).12 Approximately 25–62% of vasa previa cases are classified as type 1. Type 2 vasa previa presents in 33–76% of vasa previa cases. It is characterized by blood vessels that are positioned similarly to type 1 vasa previa, but in addition these blood vessels also run in between the placental lobes (Figure 4B).12 Furthermore, the blood vessels which connecting the placental lobes are located at or beyond the cervix.5,7,8 Our patient was diagnosed with vasa previa type 2 due to the presence of blood vessels located between the two placental lobes.
 |
Figure 4 Classification of vasa previa: (A) vasa previa type 2, (B) vasa previa type 2.10 |
Vasa previa could cause antepartum haemorrhage, which manifests as abrupt and painless vaginal bleeding, varying in volume. Patients presenting with antepartum haemorrhage and amniotic rupture should be evaluated for vasa previa, particularly when accompanied by slowing of the fetal heart rate and bradycardia.5,7 The fetal mortality rate in such cases is at least 60%, even when emergency caesarean section was carried out.6 Bleeding in the vasa previa may occur in the second or third trimester.7 On physical examination, blood vessels with pulsation can be observed at the opening of the cervix during digital examination or speculum examination.5 The occurrence of bleeding in vasa previa is the primary factor contributing to the elevated fetal mortality in this case. The mortality rate of infants caused by undetected vasa previa ranges from 60–70%, and in some cases, it can even approach 100%.4,5 Morbidity in the fetus can occur when there is bleeding as much as 100 mL, as this amount is equivalent to the total fetal blood volume, which is typically around 100 mL/kg body weight.4
Transvaginal ultrasound, colour flow mapping, and pulsed-wave Doppler is the gold standard for detecting vasa previa during antenatal examination. It is recommended to perform it as early as feasible.6 This examination greatly decreases the occurrence of death and illness in the period surrounding childbirth.1,5 The fetal survival rate can reach 95% in cases of vasa previa that are diagnosed early and at the time of delivery, which occurs after 35 weeks.7,8 Prenatal ultrasound examination is generally done at the age of 18–28 weeks of pregnancy.8 The diagnosis of vasa previa is established if arteries with pulsation consistent with fetal heartbeat are observed above the cervix, either just above the internal ostium or nearby.8 A condition that needs to be identified in early detection of prenatal vasa previa is the presence of blood vessels covering the internal cervical ostium, although this can also mean umbilical cord presentation. These two conditions can be distinguished by observing their relative positions on repeated ultrasound examinations with position changes. The position of the blood vessels could possibly different on the umbilical cord presentation, while in vasa previa the blood vessels remain at the same location.1,5 Insertion of the umbilical cord and the location of the placenta should also be ascertained as an assessment of risk factors and consideration of efforts that must be made to rule out the possibility of vasa previa.3,5,7,13 In a certain condition in which vasa previa is suspected, such as in pregnancy with high risk of vasa previa, or in conditions where transabdominal ultrasound cannot identify the location of umbilical cord insertion, transvaginal ultrasound with 2D and 3D Doppler should be considered.1 Measurement of the cervical length using transvaginal ultrasound may be helpful in determining the timing of hospitalization and delivery.
Detection of vasa previa or identifying risk factors that can lead to vasa previa by ultrasound screening can be a beneficial factor in managing both maternal and fetal well-being. Data from the UK found that routine screening can identify 1 to 2 cases of vasa previa in maternity units in the UK each year.5 Once the diagnosis of vasa previa has been established, the patient should be observed on an ongoing basis and admitted electively at week 34 or sooner, to monitor for possible signs of labor and plan elective delivery in a timely manner.5,8 Previous studies recommended that mothers begin to be offered elective labor at 35 weeks of gestation or after administration of corticosteroids for fetal lung maturation is done. It is also mentioned in other literature that the majority perform the caesarean section at 38 weeks. However, most literature agreed that the delivery should be done between 34 and 37 weeks of gestation. Another study indicated that the risk of adverse events resulting from premature birth at 35 weeks of gestations is lower than the risk of complication occurrence if the membranes rupture.5 Therefore, for symptomatic patients, it is recommended to plan an elective caesarean section at 35 weeks for singleton and between 32 and 34 weeks for twins. Vasa previa in these patients is detected by ultrasound examination in term pregnancy before signs of labor appear. Once detected, the patient is hospitalized for observation and planned for elective cesarean section. In literature, the decision to hospitalize a patient should be individualized and based on clinical findings. In woman with twin pregnancy or higher multiple pregnancies and a short cervix, admission at 30 weeks or even earlier may need to be considered.4,6 In woman with singleton pregnancies and no adverse complication, admission at 32 weeks can be considered.
During the caesarean section, the unprotected fetal vessels which are located near or under the uterine incision could iatrogenically ruptured, resulting in fetal exsanguination which prompted intensive neonatal care, including blood transfusion. It is necessary to locate the fetal vessels and placenta during the antenatal care as one of the essential preparations before surgery.
In general, perinatal outcomes are excellent in a patient with vasa previa that has been diagnosed during antenatal care. A meta-analysis reported that the total survival rate in patients with vasa previa that has been diagnosed during antenatal period is 99%. It is different from patients with absent antenatal diagnosis, in which the total survival rate only reaches 72%. Other than that, the risk of neonatal transfusion is higher in cases which are not diagnosed during antenatal period. It is more preferred to have a planned delivery rather than emergency delivery as it could affect the neonatal outcomes.
The management of vasa previa includes close observation of pregnancy, preventing rupture of membranes, and delivery before the signs of labor commenced.5,7 Pregnancy which is complicated by vasa previa is suggested to undergo an elective cesarean section for the delivery method.1 Such cases could not wait until the signs of labor occurred due to the risk of profused bleeding and fetal exsanguination. The exposed fetal vessels might be compressed by fetal movements or descent of the presenting part and decelerations of fetal heart rate might occur.5 Delivery should be done at tertiary hospital with comprehensive facility and multidisciplinary resources to handle neonates, including blood reserves for transfusion and neonatal intensive care unit.7,8 A patient that has been diagnosed with vasa previa during the antenatal period should be counseled that the risk of prematurity does not outweigh the risk of emergency caesarean section due to tear of fetal vessels during labor. An appropriate neonatology team and intensive care unit is needed to insure the optimal neonatal outcomes. In this case report, the patient underwent an elective cesarean section at a tertiary hospital at term based on ultrasonography finding. The termination was performed before there were signs of labor, the tear of vessels, or rupture of membranes. The maternal and perinatal outcome was optimal.
Conclusion
Vasa previa is a rare condition, however it is associated with a high fetal morbidity and mortality if prompt diagnosis and management is lacking. The perinatal outcome is significantly improved with an early detection using ultrasonography, careful observation, and elective cesarean section before any signs of labor appear.
Learning Points
- The transvaginal ultrasound, cervical length measurement, colour mapping and pulsed-wave Doppler should be done to confirm the diagnosis of vasa previa.
- The timing for hospitalization of women with vasa previa is 32 weeks of gestation for singleton pregnancy, or before 32 weeks of gestation for women with risk factors such as multiple gestation and cervical length less than 2.5 cm.
- A caesarean delivery is performed at 35 weeks 0 days to 35 weeks 6 days in women with vasa previa and a singleton pregnancy. While in women with twin pregnancy, a caesarean delivery is performed at 33 weeks 0 days to 34 weeks 6 days of gestation.
Ethical Approval
This study is exempt from ethical approval, as determined by the institutional and departmental review board. The authors’ institution does not require ethical approval for publication of single case report.
Consent for Publication
The patient provided written informed consent for publication of the case report and the accompanying images.
Acknowledgments
We would like to acknowledge and express our gratitude to our teachers in the Obstetrics and Gynecology Department of Hasan Sadikin for their help with this case study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Norvilaitė K, Peštenytė A, Bužinskienė D, Drąsutienė G, Arlauskienė A, Poškus T. Vasa praevia: a case report and literature review. Acta Med Litu. 2016;23(1):11–16. doi:10.6001/actamedica.v23i1.3265
2. Srinivasan D, Daly-Jones E, Oyelese Y, Papanikolaou K, Lees CC. Challenging common misconceptions in vasa previa screening and diagnosis. Ultrasound Obstet Gynecol. 2024;64(4):435–442. doi:10.1002/uog.27567
3. Redline RW. The Umbilical Cord. The Placenta. 2011;h.114–21.
4. Degirmenci Y, Steetskamp J, Macchiella D, Hasenburg A, Hasenburg A. Vasa previa: a rare obstetric complication-A case series and a literature review. Clin Case Rep. 2022;10(3):e05608. doi:10.1002/ccr3.5608
5. Mohapatra I, Samantaray S, Sindhuja V. Vasa previa: a case report. Int J Reprod Contraception Obstet Gynecol. 2020;9:4301. doi:10.18203/2320-1770.ijrcog20204329
6. Jain V, Gagnon R. Guideline no. 439: diagnosis and management of Vasa Previa. J Obstet Gynaecol Canada. 2023;45(7):506–518. doi:10.1016/j.jogc.2023.05.009
7. Reichenbach J, Minzola D. Vasa Previa: a case report. Aana J. 2020;88(6):436–438.
8. Putra R, Rachman I, Pradjatmo H. Early finding of Vasa Previa: a case report. Jurnal Kesehatan Reproduksi. 2022;8. doi:10.22146/jkr.65005
9. Kaplan CG. Color Atlas of Gross Placental Pathology. Springer New York; 2007.
10. Rochmaida I, Mufdlilah, Suwoto A. HUBUNGAN PARITAS DENGAN KEJADIAN PLASENTA PREVIA DI RS PKU MUHAMMADIYAH YOGYAKARTA TAHUN 2007 dan 2008. Unisayogya.ac.id. [Tugas Akhir Thesis]. Indonesian. 2009.
11. Ramadhan B. Plasenta Previa: mekanisme dan Faktor Risiko. Jurnal Ilmiah Kesehatan Sandi Husada. 2022;208–219. Indonesian. doi:10.35816/jiskh.v11i1.735
12. Daly-Jones E, John A, Leahy A, McKenna C, Sepulveda W. Vasa Praevia; a preventable tragedy. Ultrasound. 2008;16:8–14. doi:10.1179/174313408X259508
13. Wladimiroff JW, Eik-Nes S. Ultrasound in Obstetrics and Gynaecology. Elsevier; 2009.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.