Back to Journals » International Medical Case Reports Journal » Volume 19
A Case of Vaginal Leiomyoma: Physical Examination Outperforms Imaging
Authors Dong ZX ![]() , Xu XY, Wang XY, Zhang WQ, Cong JH, Li J
, Xu XY, Wang XY, Zhang WQ, Cong JH, Li J
Received 14 April 2026
Accepted for publication 23 June 2026
Published 26 June 2026 Volume 2026:19 616836
DOI https://doi.org/10.2147/IMCRJ.S616836
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gates Colbert
Zhao-Xiang Dong, Xin-Yu Xu, Xiu-Ying Wang, Wen-Qing Zhang, Jia-Hui Cong, Jing Li
Department of Obstetrics and Gynecology, Dalian Women and Children’s Medical Group/Dalian University of Technology Affiliated Women and Children’s Hospital, Dalian, Liaoning, People’s Republic of China
Correspondence: Xiu-Ying Wang, Email [email protected] Wen-Qing Zhang, Email [email protected]
Background: Vaginal leiomyoma is a rare condition, and the most common site of occurrence is the anterior vaginal wall. Medical imaging plays a critical role in preoperative diagnosis and surgical decision-making, particularly ultrasonography and magnetic resonance imaging (MRI).
Case Presentation: We report a case of an anterior vaginal wall leiomyoma in a reproductive-age woman. Preoperative multimodal imaging consistently yielded a diagnosis of a cervical myoma, while clinical examination and surgical exploration confirmed the lesion to be a primary vaginal leiomyoma.
Conclusion: Even in the era of highly advanced imaging technology, clinicians should still prioritize physical examination in clinical practice and integrate the advantages of high-precision imaging equipment to enhance the accuracy of diagnosis. A careful palpation may be more precise than imaging in ascertaining the anatomical origin of the lesion. Meanwhile, clinicians should rationally address the limitations of imaging examinations and mitigate imaging misinterpretation through multi-dimensional approaches.
Keywords: leiomyoma, vaginal leiomyoma, cervical leiomyoma, medical imaging, Imaging
Introduction
Uterine leiomyoma represents one of the most common benign gynecological tumors in women of reproductive age, whereas vaginal leiomyoma is relatively rare. Since its initial documentation by Denys de Leyden in 1733, only slightly over 300 cases have been reported globally, with an estimated incidence rate of about two per 10,000 individuals.1 Studies indicate that the majority of affected individuals are between 35 and 50 years of age.1,2 Anatomically, the anterior vaginal wall is the most frequently involved site, accounting for 69.5% of cases, followed by the posterior wall, which accounts for 17%, and the lateral wall, which accounts for 13.5%.3 These lesions are thought to arise from smooth muscle tissue in various structures, such as the vaginal submucosa, vascular walls, arrector pili muscles, or the round ligament, though their exact pathogenesis remains unclear. The preoperative misdiagnosis rate of vaginal leiomyoma is exceedingly high. In a 2014 domestic report in China, a total of six cases of vaginal leiomyoma over the previous four-year period were tallied, and all of them were misdiagnosed prior to surgery. Another Chinese report published in 2009 documented six cases of vaginal leiomyoma that occurred over the past 22 years, and five of them were misdiagnosed prior to surgery. Imaging plays a pivotal role in the auxiliary diagnosis of vaginal leiomyoma and is routinely utilized in clinical practice, particularly ultrasound and MRI, both of which have excellent safety profiles and do not involve ionizing radiation. We recently encountered a case of an anterior vaginal wall leiomyoma in a reproductive-age woman. Preoperative multimodal imaging modalities consistently yielded misleading results. We present this case to emphasize the significance of clinical physical examination. A thorough gynecological examination might be more effective in identifying the anatomical location of the lesion compared to imaging examination. Clinicians should integrate the advantages of imaging examination to enhance the accuracy of preoperative diagnosis and rationally address the limitations of imaging examination.
Case Presentation
The patient was a 41-year-old woman presenting with prolonged menstrual periods persisting for nearly six months. At her initial presentation, transvaginal color Doppler ultrasonography revealed an irregular endometrial thickness measuring 15 mm (Figure 1) and a hypoechoic mass (33×50×28 mm) located adjacent to the lower segment of the anterior cervical lip (Figure 2), initially suggestive of a subserosal uterine leiomyoma. Color Doppler flow imaging (CDFI) demonstrated short linear vascular signals within the lesion. Additionally, three intramural leiomyomas, each approximately 1 cm in diameter (Figures 3 and 4), were detected. The ultrasonography was performed by a chief physician. The patient did not present with any subjective symptoms apart from alterations in menstruation. A careful bimanual vaginal examination revealed a firm, palpable mass approximately 5.5 cm in diameter located in the anterior vaginal wall near the anterior fornix, independent of the cervix. Upon insertion of the vaginal speculum, the cervix appeared smooth and intact. However, complete visualization of the mass on the anterior vaginal wall was limited due to its deep anatomical location. After the gynecological examination, a vaginal wall mass was considered. Given that the patient presented with uneven endometrial thickening, to determine the presence of intrauterine vegetation, oral dydrogesterone was administered for 10 days to facilitate complete endometrial exfoliation, analogous to drug curettage. Following menstruation, pelvic three-dimensional color Doppler ultrasound and MRI were performed. The ultrasound revealed a hypoechoic solid mass measuring 40×56×30 mm on the anterior cervical wall near the external os, suggestive of cervical leiomyoma (Figure 5). The ultrasonography was also performed by a chief physician. During the examination, dynamic ultrasonography was conducted, and a specific assessment was made of the relationship between the lesion and the cervix. Nevertheless, neither of the ultrasonograms was reviewed by a specialized gynecologic radiologist. Pelvic MRI confirmed a 60×36×34 mm leiomyoma projecting into the cervical canal (Figure 6). In addition, both imaging modalities identified endometrial polyps approximately 1 cm in diameter (Figures 7 and 8).
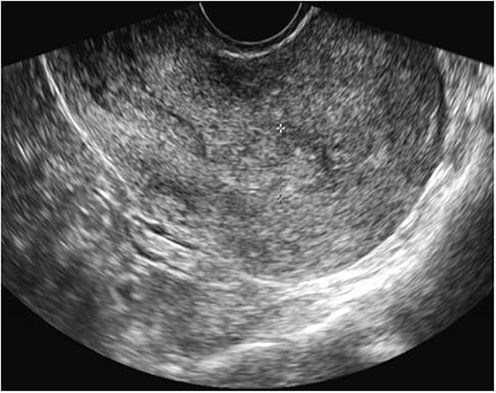 |
Figure 1 The endometrium was measured via ultrasound. |
 |
Figure 2 Vaginal leiomyoma was measured via ultrasound. |
 |
Figure 3 Intramural leiomyomas located in the posterior wall of the uterus were measured via ultrasound. |
 |
Figure 4 Intramural leiomyomas located in the anterior wall of the uterus were measured via ultrasound. |
 |
Figure 5 Manifestation of vaginal leiomyoma in transvaginal ultrasound images. |
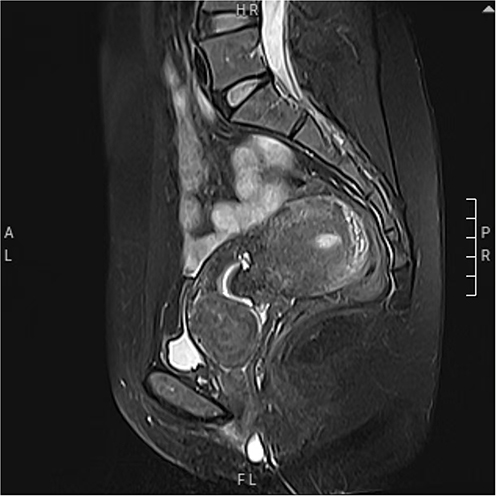 |
Figure 6 Manifestation of vaginal leiomyoma on pelvic magnetic resonance imaging (MRI). |
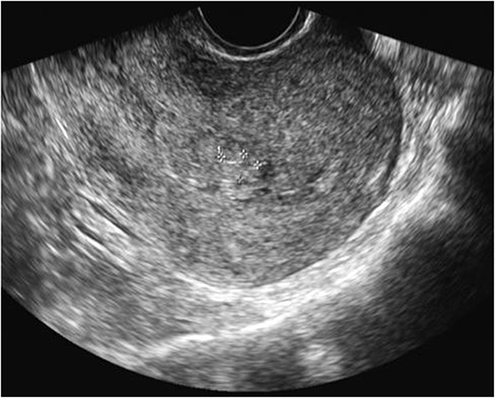 |
Figure 7 The endometrial polyps were measured via transvaginal ultrasound. |
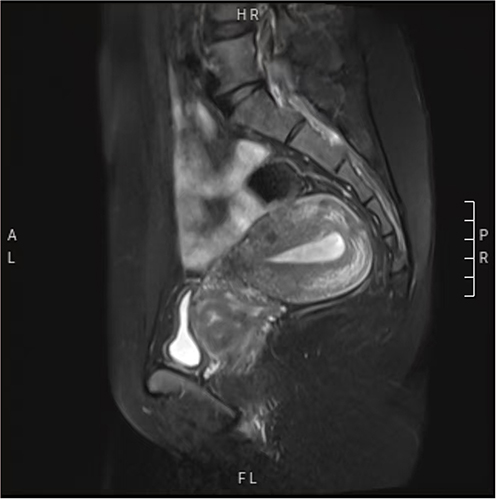 |
Figure 8 The endometrium as visualized in MRI. |
The patient was admitted to the hospital on October 27, 2025. She underwent a multidisciplinary consultation involving several experienced gynecologists. There was unanimous agreement that the lesion originated from the vaginal wall and was likely a benign tumor, with a high probability of being a leiomyoma. Imaging findings were unable to precisely reflect the location of the mass, and clinical examination should serve as the primary reference for decision-making. Based on this assessment, transvaginal tumor resection under general anesthesia combined with hysteroscopic endometrial polypectomy was performed. During the vaginal surgery, the lower half of the anterior vaginal wall was elevated using a retractor to achieve full exposure of the tumor. Despite the irregular morphology of the vaginal wall mass, a longitudinal incision was made in the overlying vaginal mucosa to optimize access and facilitate subsequent suturing. After complete visualization of the lesion, sharp dissection was performed gradually with long curved scissors, combined with blunt dissection, enabling straightforward and complete en bloc excision of the tumor. Following excision of the vaginal wall mass, precise suturing using absorbable sutures was meticulously performed on both the vaginal submucosal tissue and the anterior vaginal wall to achieve hemostasis and prevent iatrogenic bladder injury. Gross examination revealed a vaginal wall mass measuring 5.5×4.0×3.5 cm and weighing approximately 100g. The specimen was gray-yellow, firm in consistency, and exhibited a characteristic whorled and interwoven cut surface (Figure 9). In view of the fact that the specimen was a manifestation of leiomyoma, frozen pathological examination was not carried out. Postoperative paraffin pathology confirmed a diagnosis of leiomyoma (Figure 10).
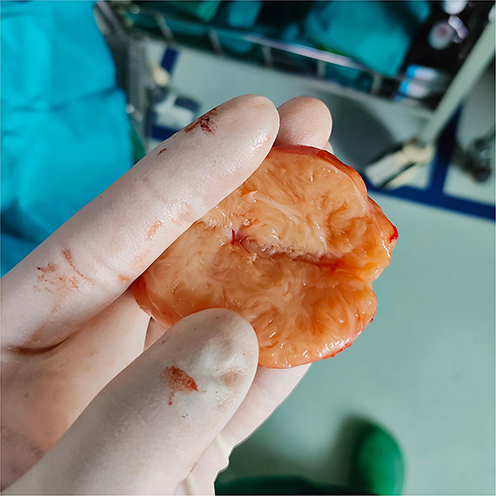 |
Figure 9 Cross-sectional photograph of an ex vivo specimen of vaginal leiomyoma. |
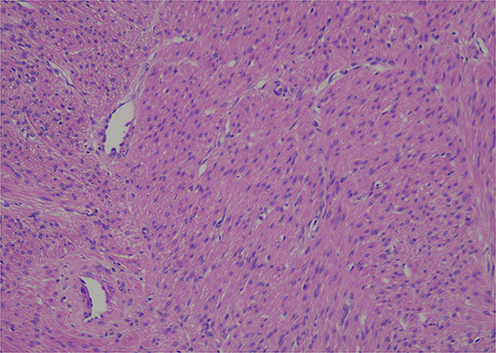 |
Figure 10 100-magnification microscopic photograph of a pathological section of vaginal leiomyoma stained with hematoxylin-eosin (HE). |
The patient has demonstrated an uneventful postoperative recovery with no evidence of recurrence to date.
Discussion
Vaginal leiomyomas are typically solitary tumors, measuring 0.5 to 15 cm in diameter, with the most common location being the midline of the anterior vaginal wall.1 Evidence indicates that tumors exceeding 6 cm in diameter are more frequently associated with symptomatic presentation, including vaginal bleeding, lower abdominal pain, and low back pain.4 Distinct tumor growth sites may give rise to diverse symptoms. For instance, tumors located on the anterior wall may compress the bladder, leading to urinary symptoms including frequency, urgency, dysuria, and incomplete voiding. In contrast, tumors on the posterior vaginal wall may exert pressure on the rectum, resulting in obstructive defecatory symptoms such as constipation, incomplete evacuation, and a sensation of anal heaviness. In certain cases, patients with large tumors may exhibit sexual dysfunction as a result of tumor-related anatomical or physiological alterations. The vaginal mucosa is soft and highly distensible, particularly in women of reproductive age, allowing small vaginal leiomyomas to remain asymptomatic in most cases. These lesions are typically incidentally detected either by the patient or a sexual partner during physical contact or during routine gynecological examination.
A review of the patient’s medical history indicated that the underlying etiology was not a vaginal wall neoplasm, but rather an endometrial polyp manifesting as menstrual irregularities. Consequently, despite the substantial size of her vaginal leiomyoma, she remained asymptomatic, for which several plausible explanations exist. Anatomically, the tumor was situated deep within the vaginal cavity and adjacent to the anterior fornix, the widest and most distensible region of the vagina, allowing for substantial expansion without eliciting symptoms. Second, with respect to innervation, vaginal nerve density decreases with increasing distance from the introitus, meaning that tumors arising near the vaginal apex, as in this case, are more likely to remain undetected due to lower sensory sensitivity in this region. Third, the patient had abstained from sexual activity for an extended period, thereby lacking mechanical stimulation through intercourse that might otherwise have prompted clinical evaluation. Finally, the patient had no history of regular professional gynecological examinations, which resulted in the delayed detection of the vaginal tumor. Therefore, this case further highlights the importance of routine gynecological examinations for the majority of women.
Clinically, vaginal leiomyoma requires differentiation from a range of conditions, including vaginal cysts, vaginal fibroma, vaginal sarcomas, cystoceles, paraurethral cysts, urethral leiomyomas, cervical leiomyomas, vaginal malignancies, Bartholin’s gland cysts, and endometriosis.1,5 Generally, vaginal leiomyomas share the same histological features as uterine leiomyomas. As a result, their clinical presentations typically include well-defined margins, uniform consistency, and firm texture. However, when degeneration occurs, such as cystic, myxoid, or fatty changes, or calcification, the texture may become either soft or hard, leading to atypical manifestations. In such cases, imaging is required to aid diagnosis, as it allows for assessment of the tumor’s relationship with deep tissue structures and its internal architecture. Ultrasound and MRI exhibit high accuracy in the preoperative diagnosis of vaginal leiomyoma, with three-dimensional ultrasound potentially outperforming MRI. This is supported by research indicating that the sensitivity and specificity of ultrasound are 98% and 100%, respectively, whereas those of MRI are 76% and 83%, respectively.6
Common ultrasonographic features of leiomyomas consist of well-circumscribed margins, a hypoechoic internal echotexture, and minimal peripheral vascularity. On MRI, leiomyomas typically demonstrate well-defined borders, homogeneous T2 hypointensity, early arterial enhancement with prominent heterogeneous enhancement, persistent enhancement in venous and delayed phases, and peripheral rim enhancement. Ultrasonography offers a cost-effective and convenient means of assessing tumor activity and vascularity, making it the preferred initial imaging technique.6 In our case, while both ultrasound and MRI correctly identified the tumor’s histologic nature, neither accurately localized its anatomical origin. Plausible explanations include the tumor’s proximity to the cervix, with progressive enlargement leading to tighter adherence to the cervical tissue, and the challenge of clearly delineating the tumor’s origin during imaging performed in the vagina’s natural state. In addition, radiologists may enhance their diagnostic capability for rare conditions such as vaginal leiomyoma through strengthened theoretical training and refined clinical skills. In numerous challenging cases, the utilization of contrast-enhanced imaging proves beneficial for preoperative diagnosis. For instance, in our case, transabdominal ultrasonography and vaginography with sterile saline perfusion can be carried out, or MRI with sterile saline or gel vaginography can be conducted. A simpler and more cost - effective approach could be the employment of a Foley catheter. First, use a water balloon to occlude the vaginal opening, and then inject fluid into the vagina until complete visualization is achieved. Regrettably, this method was not employed for preoperative assessment in our case, as the specific location of the lesion had already been identified through vaginal palpation. Consequently, the aforementioned methods are merely theoretical analyses.
Currently, surgical resection of the tumor is the primary approach for the treatment of vaginal leiomyoma. Owing to its infrequent occurrence, it is challenging to establish a definitive preoperative diagnosis, and confirmation is typically achieved only through postoperative pathological examination.7 Similar to the surgical principles of uterine leiomyoma, the emphasis lies on the complete resection of the tumor to prevent short-term recurrence. Transvaginal resection serves as the main method. Given the special location of the tumor, the “water pad” method in the tissue space can be employed to delineate the boundary of the tumor and mitigate the risk of adjacent organ damage.
For certain patients with large tumors, extremely deep tumor locations, and challenges in vaginal exposure, laparoscopic surgery or transvaginal natural orifice endoscopic surgery can be selected.8,9 If required, gonadotropin-releasing hormone agonists or antagonists can be administered before the operation to reduce the tumor size and facilitate the surgical procedure.10 When malignancy is suspected preoperatively or intraoperatively, a frozen section may be sent for pathological analysis during surgery. In this case, despite the deep location of the tumor adjacent to the vaginal vault, it was successfully excised via a vaginal approach. Key procedural elements included: complete exposure of the surgical field under anesthesia, use of a longitudinal incision and suturing technique, and meticulous tumor dissection using a combination of blunt and sharp methods close to the tumor surface to minimize bleeding. This approach may provide a useful reference for gynecologists.
Imaging examination has certain limitations, particularly in the case of rare diseases. It is essential for radiologists to possess a highly solid theoretical foundation and practical experience in order to reduce the misdiagnosis rate. On the one hand, clinicians should recognize the significance of clinical physical examination and integrate the advantages of imaging examination to enhance the accuracy of diagnosis. On the other hand, the limitations of imaging examination should be regarded rationally. Through a substantial amount of theoretical learning and practical accumulation, multi-dimensional approaches can be employed to minimize imaging misinterpretation.
Data Sharing Statement
The references cited in this article are true and reliable.
Ethics Approval and Consent to Participate
This case has received approval from the Medical Ethics Committee of Dalian Women and Children’s Medical Group (No. FEJT-KY-2026-09), and the patient has given consent for publication.
Consent for Publication
The patient for this case report gave written consent for the publication of this article. All the authors have given written consent for the publication of this manuscript.
Author Contributions
Zhao-Xiang Dong was the major contributor in writing the manuscript. Xin-Yu Xu, listed as co-first author, made substantial and equal contributions to this work. Xiu-Ying Wang serves as the corresponding author, while Wen-Qing Zhang acts as the co-corresponding author. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No special funding.
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Lugata J, Makower L, Rapheal A, et al. Unusual presentation of recurrent vaginal leiomyoma in pregnancy: a rare case report and review of current literature. Clin Case Rep. 2025;13:e70344. doi:10.1002/ccr3.70344
2. Deepika, Goyal S, Garg P, Kanwat J, Kaur N. Vaginal leiomyoma in a perimenopausal woman: a rare case report and review of the literature. J Family Med Prim Care. 2024;13:2161–9. doi:10.4103/jfmpc.jfmpc_1229_23
3. Giovannopoulou E, Kogeorgos S, Lazaridis A, Pistofidis G. Vaginal leiomyomas - safe steps for laparoscopic removal: feasibility from 3 case reports. Facts Views Vis Obgyn. 2023;15:161–165. doi:10.52054/FVVO.15.2.067
4. Gonzatti P, Sousa G, Gonçalves J, et al. Mioma vaginal. Rev Eletrônica Acervo Saúde. 2025;25:32–34. doi:10.25248/reas.e196902025
5. Errmili K, Essebbagh Y, Idoubba S, Benaouicha N, Zeraidi N, Baidada A. Management of vaginal leiomyomas during pregnancy - a case report. Int J Surg Case Rep. 2025;128:110964. doi:10.1016/j.ijscr.2025.110964
6. Do Amaral CC, Castro PT, Frota R, et al. Vaginal leiomyoma: advantages of clinical sonovaginography and ultrasound dynamic evaluation of uterine cervix-related lesions. J Clin Ultrasound. 2023;51:1509–1511. doi:10.1002/jcu.23580
7. Muhammad H, Rashid R, Othman S. Vaginal leiomyoma: a case report. Int J Surg Open. 2026;4:4–6. doi:10.1016/j.ijso.2023.100663
8. Zhang NN, Li D, Chen SL, Zuo N, Sun TS, Yang Q. An effective method using laparoscopy in treatment of upper vaginal leiomyoma. Fertil Steril. 2020;114:185–186. doi:10.1016/j.fertnstert.2020.03.026
9. Liu JH, Zheng Y, Wang YW. Transvaginal natural orifice transluminal endoscopic surgery (vNOTES) as treatment for upper vaginal leiomyoma: a case report. Medicine. 2021;100:e25969. doi:10.1097/MD.0000000000025969
10. Liu Y, Wang X, He Y. GnRH analogue followed by surgery in treatment of vaginal leiomyoma-a case report. Medicine. 2021;100:e24911. doi:10.1097/MD.0000000000024911
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.