Back to Journals » Journal of Blood Medicine » Volume 15
A Case of Pernicious Anemia with Concurrent Beta-Thalassemia Minor
Authors Yuan F, Huang Z, Yao D, Sun J ![]()
Received 23 April 2024
Accepted for publication 23 July 2024
Published 7 August 2024 Volume 2024:15 Pages 351—357
DOI https://doi.org/10.2147/JBM.S473075
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Fuzhen Yuan,1 Zhenhua Huang,1,2 Dingye Yao,1,2 Junsheng Sun1,2
1Department of General Practice, Longgang District Central Hospital of Shenzhen, Shenzhen, 5181116, People’s Republic of China; 2Shenzhen Clinical College of Medicine, Guangzhou University of Chinese Medicine, Shenzhen, 5181116, People’s Republic of China
Correspondence: Junsheng Sun, Department of General Practice, Longgang District Central Hospital of Shenzhen, No. 6082, Longgang Avenue, Longgang District, Shenzhen, Guangdong Province, 518100, People’s Republic of China, Tel +86-15338897372, Email [email protected]
Abstract: Vitamin B12 is essential for various bodily functions, and its deficiency may cause hematological manifestations. We report a case of a previously healthy 65-year-old female who was admitted to our hospital with reduced sense of taste and painful tongue. The serum level of vitamin B12 was decreased. However, her complete blood count did not show any evidence of macrocytosis, instead, her mean corpuscular volume was low. Gene sequencing indicated an β-thalassemia minor and that probably masked the megaloblastic features of vitamin B12 deficiency.
Keywords: pernicious anemia, autoimmune gastritis, thalassemia, glossitis
A 65-year-old woman presented with reduced sense of taste, painful tongue, decreased appetite, fatigue and dizziness that had developed 10 months earlier. She had been confused for a long time because of tasteless eating and loss of appetite due to the reduced sense of taste. She referred to the outpatient department of stomatology several times without definite diagnosis. She had no signs of infection or bleeding, no family history of hematologic disorders, and a medical history significant only for hypertension. Her bowel movements were normal with no evidence of blood. There was no surgical history or alcohol consumption.
On physical examination, the patient appeared pale but fully oriented, with stable vital signs and no fever. She had a smooth, red tongue without lingual papillae, suggestive of glossitis (Figure 1A). She had no palpable hepatosplenomegaly or lymphadenopathy, and no deficits were found on neurologic examination.
 |
Figure 1 (A) An image of a 65-year-old Chinese woman with glossitis (smooth and red tongue dorsum without lingual papillae) caused by pernicious anemia. (B) Her tongue appears normal three month after starting treatment with methylcobalamin. |
Laboratory detection indicated normocytic anemia (hemoglobin 78 g/L, MCV 85.5 fL [normal range 82–100], MCH 27.6 pg [normal range 27–34], MCHC 322 g/L [normal range 316–354], RDW 27.5%, platelets 361×109 /L, and white blood cells 3.52×109 /L). A complete blood count conducted six months prior did not show any irregularities. Additionally, high-sensitivity troponin levels and electrocardiography results were unremarkable, and renal function was within normal parameters.
The additional laboratory tests (Table 1) were intended to narrow the differential diagnosis of anemia in our patient. According to a peripheral blood smear, the mature erythrocyte size differed slightly and some areas had weak staining. Target erythrocytes, teardrop-shaped red blood cells and oval-shaped red blood cells could be seen (Figure 2). Bone marrow aspiration was compatible with hyperplastic anemia, and morphologic signs of megaloblastic anemia (Figure 3). The reticulocyte count was 1.58%, indicating active erythroid proliferation. Therefore, malignant hematological disorders such as myelodysplastic syndromes, leukemia, lymphoma and aplastic anemia could be excluded. An elevated ferritin eliminated iron deficiency or occult bleeding, while a high lactate dehydrogenase and hyperbilirubinemia suggested hemolysis. However, a negative direct Coombs test in our patient could rule out autoimmune hemolytic anemia (AIHA). Furthermore, the presence of target erythrocytes in the peripheral blood, high levels of lactate dehydrogenase and indirect bilirubin, and morphological changes in bone marrow were the potential clues pointing towards thalassemia. Indeed, hemoglobin electrophoresis showed hemoglobin A2 and F were 6.00% [normal range 2.5–3.2] and 7.80% [normal range 0–0.5]. Gene sequencing showed that the codon 41/42 (-CTTT) mutation in this patient caused β-thalassemia. Most notably, vitamin B12 level was 104.9 pg/mL, significantly below the lower limit of detection [normal range 197–771], but the folate (18.26 ng/mL) concentration was normal. Homocysteine level was significantly elevated (165.3 umol/L [normal range 4.0–15.4]). Serum anti-gastric parietal cell antibody (PCA) and anti-intrinsic factor antibody (IFA) were positive. Thyroid-stimulating hormone level was normal. Thyroglobulin antibody and antithyroid peroxidase antibody were negative. A gastroscopy revealed showed chronic atrophic gastritis (Figure 4). Infection with Helicobacter pylori was excluded. Taken together, we diagnosed the patient with both pernicious anemia due to vitamin B12 deficiency caused by autoimmune gastritis, and thalassemia.
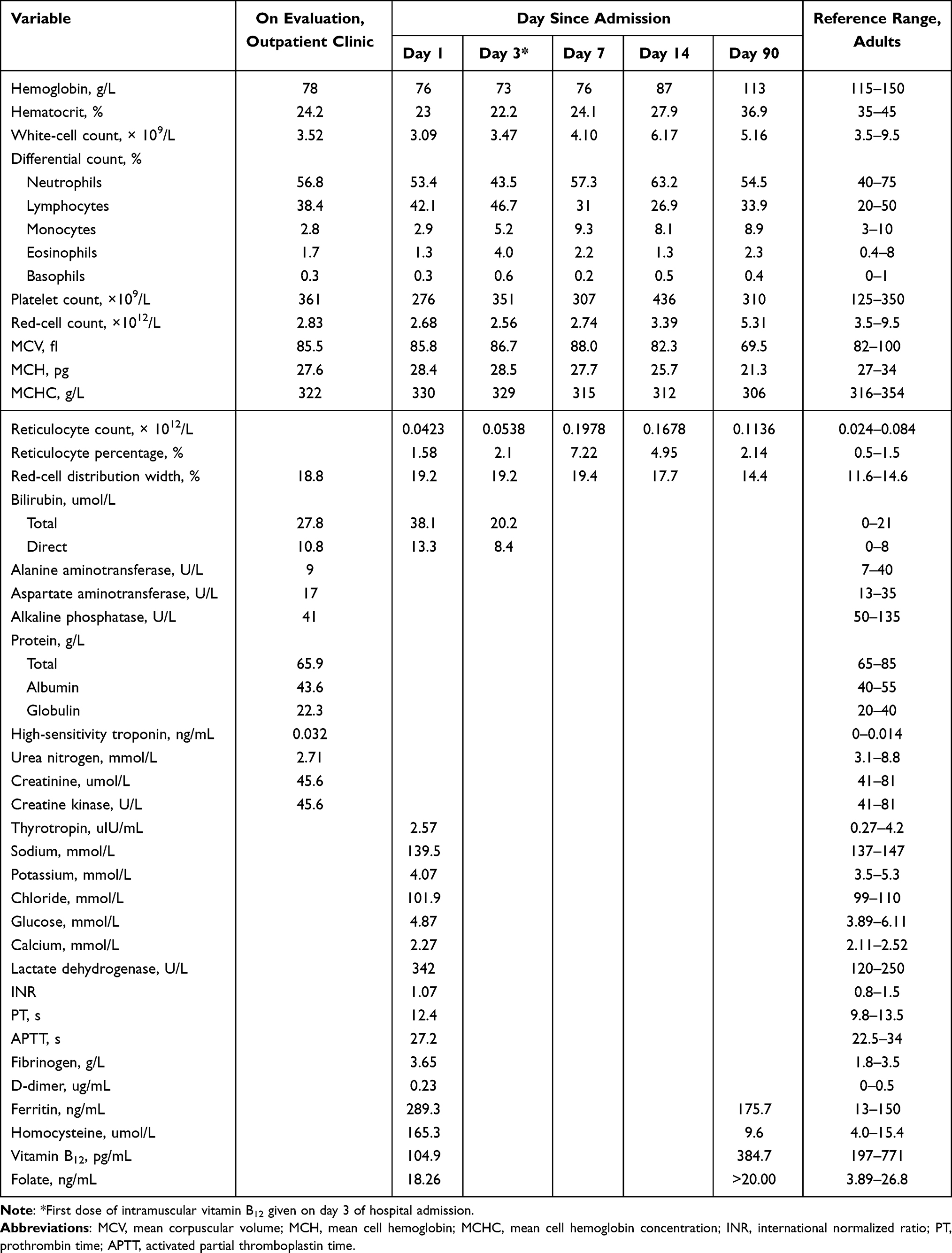 |
Table 1 Laboratory Data |
 |
Figure 2 Peripheral blood smear examination showed poikilocytosis: with target erythrocytes, teardrop-shaped red blood cells and oval-shaped red blood cells. Green arrow indicate oval-shaped red blood cell; red arrow indicate teardrop-shaped red blood cell; black arrow indicate target erythrocyte. |
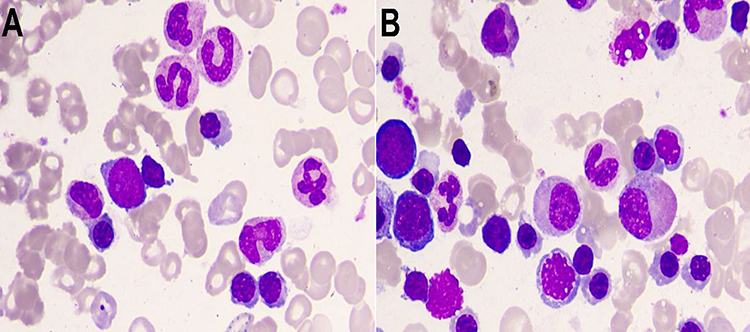 |
Figure 3 (A and B) Smears of bone marrow aspirates demonstrating megaloblastic changes: nuclear-cytoplasmic dyssynchrony and nuclear irregularity in erythroid lineage cells, and also nuclear-cytoplasmic dyssynchrony, hypersegmentation, and giant metamyelocytes. |
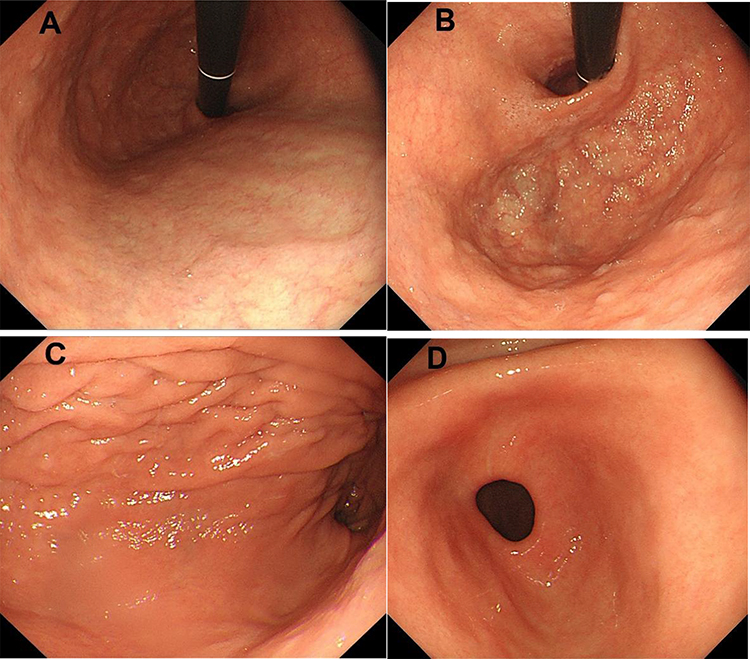 |
Figure 4 Endoscopic images of the stomach. (A–C) The typical endoscopic features of atrophic gastritis are apparent, including loss of rugal folds and pallorous-appearing gastric mucosa; due to the thinned gastric mucosa, there is the increased prominence of submucosal blood vessels in the gastric body. (D) There is no atrophy of the mucosa of the gastric antrum. |
We prescribed intramuscular vitamin B12 (500 µg daily) for our patient’s pernicious anemia beginning on the second day of admission, and oral folic acid supplementation. According to several studies, there has been no difference in outcomes between orally and parenterally administered vitamin B12.1,2 Therefore, switching to orally administered vitamin B12 (1.5 mg/day) at discharge is reasonable. Although the patient’s blood work abnormalities did not improve significantly during her 7-day hospitalization, her symptoms of painful tongue and reduced sense of taste were resolved. Three months after discharge, at a follow-up visit, her tongue regained its normal appearance (Figure 1B), and her vitamin B12 level were normal. However, substitution therapy must be continued indefinitely.
Discussion
We report a case of a patient with pernicious anemia presenting as glossitis in which the diagnosis was delayed because of concomitant thalassemia. Pernicious anemia is a megaloblastic anemia (MA) and mean corpuscular volume (MCV) is the most important parameter in routine blood test data for diagnosing MA. It is easy to diagnose MA when a high MCV occurs in a patient with MA alone. However, MA combined with thalassemia can be masked by the loss of macrocytosis. The prevalence of thalassemia in China is 4–8%, and MA combined with thalassemia is even rarer and easily missed.3 Pernicious anemia also presents with hemolysis, which is due to the breakdown of abnormal and fragile RBC precursors leads to intramedullary hemolysis and resulting abnormalities in hemolysis tests. However, it still needs to be differentiated from AIHA and requires a relatively extensive work-up. In our patient, AIHA was ruled out due to a negative direct Coombs test, but in rare cases, AIHA can coexist with PA.4 With continued vitamin B12 supplementation, her improvement further suggests that concurrent AIHA was unlikely since true AIHA usually requires glucocorticosteroids, immunosuppressive agents or splenectomy for adequate response.
Autoimmune gastritis (AIG), as a non-self-limiting chronic inflammatory disorder, leads to the destruction of parietal cells in the stomach, resulting in reduced acid output and loss of intrinsic factor, that results in malabsorption of vitamin B12 and iron, which cause pernicious anemia and iron deficiency anaemia.5 In AIG, micronutrient malabsorption causes a wide range of clinical manifestations, causing substantial diagnostic delays, resulting in life-threatening and irreversible complications. However, it has been widely accepted for several years that pernicious anemia is a synonym for AIG, which leads to confusion between the two, since pernicious anemia is only one aspect of AIG’s clinical picture. Other clinical manifestations such as gastrointestinal symptoms (eg, early satiety, postprandial fullness, nausea, and weight loss) are also very common in patients with AIG. In addition, severe vitamin B12 deficiency in patients with AIG may result in neurological damage, causing symptoms such as impaired peripheral nerve function and sensory, abnormal proprioception, ataxia, paresthesia, numbness, mood disorders, cognitive impairment and psychosis. Hyperhomocysteinaemia, infertility, and recurrent miscarriages are other infrequent symptoms of AIG.5 Despite the fact that patients with AIG can experience unspecific or subtle upper gastrointestinal symptoms, mostly commonly dyspepsia, the majority are asymptomatic before anemia or neurological symptoms develop.
Vitamin B12 is essential for various bodily functions, including DNA synthesis, nervous system regulation, amino acid metabolism, and red blood cell maturation in the bone marrow.6 The most common cause of severe vitamin B12 deficiency is autoimmune gastritis, which manifests as pernicious anemia, as seen in our patient. Additionally, vitamin B12 deficiency can also occur as a result of other malabsorptive conditions (such as inflammatory bowel disease, or pancreatic insufficiency), after certain procedures (such as bariatric surgery, or ileal resection), restricted diets (such as veganism), or the use of certain medications (such as metformin or proton-pump inhibitors).
Upper gastrointestinal endoscopy and biopsy of the gastric body and antrum are necessary for diagnosing autoimmune gastritis. Clinicians should also consider testing for anti-parietal cell antibodies and anti-intrinsic factor antibodies in patients with histology compatible with autoimmune gastritis. The prevalence of PCAs is estimated at 85–90% among adults with pernicious anemia and AIG, while IFAs are found in 35–60% of these patients.7,8 Many case series, however, diagnosed AIG solely based on serological markers such as IFAs or PCAs, pepsinogen levels or gastrin-17, without confirmatory biopsy.9 In addition, patients with iron or vitamin B12 deficiency caused by AIG may not show symptoms, and anemia is usually treated without further investigation into its cause.10
Currently, there is no cure for AIG, and immunosuppressive therapy for AIG patients does not currently have long-term trials. Supplementation with micronutrients is the mainstay of treatment for AIG patients. Vitamin B12 supplementation is the treatment of choice, regardless of the cause of vitamin B12 deficiency. Hematological alterations can be reversed with treatment. It is recommended that newly diagnosed vitamin B12 deficiency patients, particularly in patients with critically low levels of serum vitamin B12 or with neurological deficits, receive parenteral supplementation to improve their condition rapidly.5 In theory, oral supplementation with vitamin B12 and parenteral administration can both be equally effective for maintenance. According to a Cochrane review comparing oral and intramuscular vitamin B12 treatments, both treatments are comparable in the ability to normalize serum vitamin B12 levels.2 There is, however, the possibility that oral supplementation might hinder adherence to treatment because it requires strict monitoring of the patient’s treatment and high-dose daily intake, compared to a monthly injection or fewer administering.
Conclusion
In clinical practice, the clinical manifestations of autoimmune gastritis are often not apparent, and even when they are, especially in the early stages, delays in diagnosis are common. Therefore, clinicians should be aware of best practices in diagnosis and management to reduce the possibility of adverse outcomes.
Consent to Publish Statement
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. Consent to publication has been obtained: the Medical Ethics Committee of Shenzhen Longgang Central Hospital approved the publication of the case.
Acknowledgments
The authors are indebted to the patient’s family for their willingness to participate in this case report. Thanks to Dr Si-man Chen of Longgang District Central Hospital of Shenzhen, Shenzhen, China for providing the peripheral blood smear and bone marrow smear photo.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Longgang Medical Discipline Construction Fund and Guangdong Provincial Undergraduate Colleges and Universities Teaching Quality and Teaching Reform Project, Guangdong Education Higher Letter [2023] No. 4.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Groth A, Rudiger A, Herren T. Grave and pernicious anemia presenting as pancytopenia. Am J Med. 2020;133(6):e302–e303. doi:10.1016/j.amjmed.2019.11.013
2. Wang H, Li L, Qin LL, Song Y, Vidal-Alaball J, Liu TH. Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency. Cochrane Database Syst Rev. 2018;2018(3). doi:10.1002/14651858.CD004655.pub3
3. Lai K, Huang G, Su L, He Y. The prevalence of thalassemia in mainland China: evidence from epidemiological surveys. Sci Rep. 2017;7(1):920.
4. Romero KN, Patel F, Rai O, Quan A, Reddy P. A case of pernicious anemia presenting with severe hemolysis. Cureus. 2023. doi:10.7759/cureus.50534
5. Lenti MV, Rugge M, Lahner E, et al. Autoimmune gastritis. Nat Rev Dis Prim. 2020;6(1). doi:10.1038/s41572-020-0187-8
6. Socha DS, DeSouza SI, Flagg A, Sekeres M, Rogers HJ. Severe megaloblastic anemia: vitamin deficiency and other causes. Cleveland Clin J Med. 2020;87(3):153–164. doi:10.3949/ccjm.87a.19072
7. Rustgi SD, Bijlani P, Shah SC. Autoimmune gastritis, with or without pernicious anemia: epidemiology, risk factors, and clinical management. Therap Adv Gastroenterol. 2021;14:175628482110387. doi:10.1177/17562848211038771
8. Massironi S, Zilli A, Elvevi A, Invernizzi P. The changing face of chronic autoimmune atrophic gastritis: an updated comprehensive perspective. Autoimmun Rev. 2019;18(3):215–222. doi:10.1016/j.autrev.2018.08.011
9. Wathieu H, Bateman KM. A case of pseudothrombotic microangiopathy associated with pernicious anemia. J General Intern Med. 2021;36(6):1775–1777. doi:10.1007/s11606-020-06588-2
10. Lahner E, Zagari RM, Zullo A, et al. Chronic atrophic gastritis: natural history, diagnosis and therapeutic management. A position paper by the Italian Society of Hospital Gastroenterologists and Digestive Endoscopists [AIGO], the Italian Society of Digestive Endoscopy [SIED], the Italian Society of Gastroenterology [SIGE], and the Italian Society of Internal Medicine [SIMI]. Digest Liver Dis. 2019;51(12):1621–1632. doi:10.1016/j.dld.2019.09.016
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.