Back to Journals » Journal of Asthma and Allergy » Volume 18
A 21-Practice Evaluation of an Asthma and COPD Quality Improvement Program
Authors Blakey JD, Bosnic-Anticevich S, Cvetkovski B, Hancock KL ![]() , Le Cheng P
, Le Cheng P ![]() , Tyrer F, Townend J, Hew M, Del Fante P, Ranasinghe K, Thompson PJ, Smith PK, Soumakiyan M, Stewart D, Sharma A
, Tyrer F, Townend J, Hew M, Del Fante P, Ranasinghe K, Thompson PJ, Smith PK, Soumakiyan M, Stewart D, Sharma A ![]() , Willet B, Abutalieva-Lechner K
, Willet B, Abutalieva-Lechner K ![]() , Le Lievre C
, Le Lievre C ![]() , Roussos A, Accalai P
, Roussos A, Accalai P ![]() , Botini F, Bushell N, Carter V, Le T, Price D
, Botini F, Bushell N, Carter V, Le T, Price D ![]()
Received 20 December 2024
Accepted for publication 10 September 2025
Published 11 November 2025 Volume 2025:18 Pages 1599—1613
DOI https://doi.org/10.2147/JAA.S513477
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Luis Garcia-Marcos
John D Blakey,1,2 Sinthia Bosnic-Anticevich,3,4 Biljana Cvetkovski,3,4 Kerry L Hancock,5 Porsche Le Cheng,6 Freya Tyrer,7 John Townend,7 Mark Hew,8,9 Peter Del Fante,10 Kanchanamala Ranasinghe,11,12 Philip J Thompson,13,14 Peter K Smith,15 Majella Soumakiyan,16 Deb Stewart,17 Anita Sharma,18 Bruce Willet,19 Kamila Abutalieva-Lechner,20 Chantal Le Lievre,6 Alexander Roussos,6 Paola Accalai,7 Fabio Botini,6 Nicholas Bushell,6 Victoria Carter,6,7 Thao Le,6 David Price6,7,21 On behalf of the Australia Research Group
1Respiratory Medicine, Sir Charles Gairdner Hospital, Nedlands, Western Australia, 6009, Australia; 2Curtin University Medical School, Bentley, Western Australia, 6102, Australia; 3Woolcock Institute of Medical Research, Sydney, New South Wales, Australia; 4Macquarie Medical School, Faculty of Medicine, Health and Human Sciences, Macquarie University, Sydney, New South Wales, Australia; 5Allergy and Lung Health Unit, Melbourne School of Population and Global Health, The University of Melbourne, Melbourne, Victoria, Australia; 6Optimum Patient Care Australia, Brisbane, Queensland, 4000, Australia; 7Observational Pragmatic Research Institute, Aylsham, Norfolk, NR11 6UN, UK; 8Allergy, Asthma & Clinical Immunology Service, Alfred Health, Melbourne, Australia; 9Public Health and Preventive Medicine, Monash University, Melbourne, Australia; 10Hutt Street General Practice, Adelaide, South Australia, 5000, Australia; 11School of Medicine, Griffith University, Gold Coast, Australia; 12Cannon Hill Family Doctors, Cannon Hill, Queensland, 4170, Australia; 13The Lung Health Clinic, Hollywood Medical Centre, Nedlands, 6009, Australia; 14The University of Western Australia, Perth, Western Australia, 6009, Australia; 15Griffith University, Southport, Queensland, Australia; 16A2 Health Solutions, Raby, Australia; 17School of Medicine, University of Tasmania, Hobart, Tasmania, 7005, Australia; 18Platinum Medical Centre, Chermside, Queensland, 4032, Australia; 19Victoria Point Surgery, Victoria Point, Queensland, 4165, Australia; 20The University of Sydney, Sydney, Australia; 21Observational & Pragmatic Research Institute, Midview City, 573969, Singapore
Correspondence: David Price, Optimum Patient Care Australia, Office 1, Level 10, 320 Adelaide Street, Brisbane, Queensland, 4000, Australia, Tel +61 0405 764 842, Email [email protected]
Purpose: To evaluate the Achieving Clinical Audits with Electronic Records (ACAER) program in supporting primary care providers in quality improvement initiatives across asthma and COPD.
Patients and methods: This observational cohort study included individuals aged ≥ 12 years with documented diagnosis of asthma or COPD, receiving asthma or COPD therapy, at high risk of exacerbation and hospitalization. Data were derived from the intervention, linked patient questionnaires completed as part of practice evaluation and quality improvement, and routine primary care electronic medical records (EMR) within the Optimum Patient Care Research Database Australia (OPCRDA). Changes in exacerbation rates and maintenance treatment were evaluated.
Results: 7512 asthma and 6526 COPD patients were evaluated with EMR collection. A subset of 1327 asthma patients and 629 COPD patients were classified as active and high-risk. Patient questionnaires and evaluation reports were sent out between 29 October 2019 and 21 September 2021, the intervention period. For those at risk during the entire study period (2018– 2023; N=1276), 48.4% and 59.3% of patients in the high-risk asthma and COPD populations, respectively, had maintenance therapy change in the first year post-intervention. Exacerbation rates fell after the intervention period in the high-risk asthma (74.8 to 32.4 per 1000 per month) and COPD (122.9 to 91.2 per 1000 per month) populations. High-risk asthma patients had increasing rates of exacerbations in the 2 years prior to the intervention period (linear trend: 2.79 exacerbations per 1000 per month [1.34, 4.24]; p=0.001), which declined and remained stable after the intervention (p=0.87; up to 2023). Exacerbation rates for high-risk COPD patients were stable pre-intervention (p=0.29). Post-intervention rates initially declined and then showed a marginal non-statistically significant increase (p=0.28).
Conclusion: Our findings support the potential for the ACAER asthma and COPD program to drive treatment change and improve long-term outcomes in high-risk patients in primary care settings.
Keywords: Optimum Patient Care Australia, exacerbations, patient questionnaire, electronic medical records, primary care practices
Introduction
Asthma and COPD are common respiratory conditions. In Australia in 2022 an estimated 2.8 million people (about 11% of the population) had asthma and 638,000 (about 2.5% of the population) COPD. Asthma contributed to 1.3% of all deaths in Australia in 2022, and COPD was a leading underlying cause of death, representing 4% of all deaths that year.1 These figures are high by international standards,1,2 and collectively suggest that there are opportunities to improve asthma and COPD management and patient outcomes in patients who are living with these conditions in Australia. This is further underscored by the high severe exacerbation rates and steroid-related burden in patients living with asthma in Australia in comparison to other higher-income countries,3 and the geographic variation seen in asthma and COPD control evidenced by substantial differences in hospitalization rates for these conditions across the country.4,5
Available literature points to a need to improve familiarity and adherence to guidelines in relation to the management of both asthma and COPD in Australian primary care.6–12 A 2017 Australian study of primary care management of patients living with asthma or COPD reported that inappropriate prescribing relative to evidence-based guidelines was a common occurrence.6 Observational data demonstrate over-prescription of SABA to treat asthma across the severity spectrum in Australia,13 while approximately 40% of high-risk patients were not prescribed any COPD maintenance therapy across a 5-year period.14
Quality improvement initiatives at the level of the medical practitioner, including clinical audits, could be beneficial. Assessment of current performance and comparing this to established best-practice guidelines15,16 can identify evidence-practice gaps which exist in the management of asthma in Australian primary care. Audit and feedback initiatives are conducted at local, regional and national levels and are usually focused on effectiveness and/or safety indicators, which are easiest to measure using administrative databases and/or electronic medical records.17 A recently-updated Cochrane review highlighted that these initiatives can be effective in facilitating improvements in clinical practice, particularly when designed to help clinicians identify and take action on high priority clinical issues.18
Nearly all global healthcare systems recognize the importance of patient-centered care in quality improvement (QI) initiatives;19,20 this is key for asthma and COPD owing to the need for early diagnosis, identifying the right treatment and effective self-management to prevent exacerbations.21,22 Despite the potentially important improvements in professional practice afforded by clinical audits, challenges such as knowledge gaps, shortage of required skills and difficulty setting targets exist, and often deter clinicians from undertaking them.23 Supported clinical audits such as those offered by the non-profit and social enterprises Optimum Patient Care (OPC) and Optimum Patient Care Australia (OPCA) have the potential to help overcome these barriers. OPC was founded in 2005 to support the delivery of sustainable QI activities for primary care practice physicians across the UK. OPCA was founded in 2017 and has since established the Achieving Clinical Audits with Electronic Records (ACAER) asthma and COPD program.
The ACAER asthma and COPD program was designed to support primary care providers in QI initiatives across asthma and COPD care in quality improvement. More specifically, the program identifies patients with asthma and COPD at high risk of exacerbation and hospitalization and encourages enhanced care and implementation of beneficial changes at a patient and practitioner level. Notably, the ACAER asthma and COPD program has been accredited by the Royal Australian College of General Practitioners and follows an evidenced-based approach to quality improvement that is centered around a 5-step evaluation cycle (Figure 1).23 Step 1 supports practices in understanding the current state of care provision and potential areas for improvement, utilizing tools such as electronic medical records (EMR) and patient questionnaires (patient reported outcomes/information – PRO/I). Step 2 reflects on current standards by summarizing guidelines/standards and reviewing these against the data collected from the practice. Step 3 establishes reasonable targets for change, using the collected practice and patient information and comparing this to local, national or international standards. Step 4 involves the implementation of change with reports and templates that are designed to be embedded in routine care and support everyday decision making. Step 5 consists of re-evaluation of practice, with a view to demonstrating the improvements gained and their clinical value.23
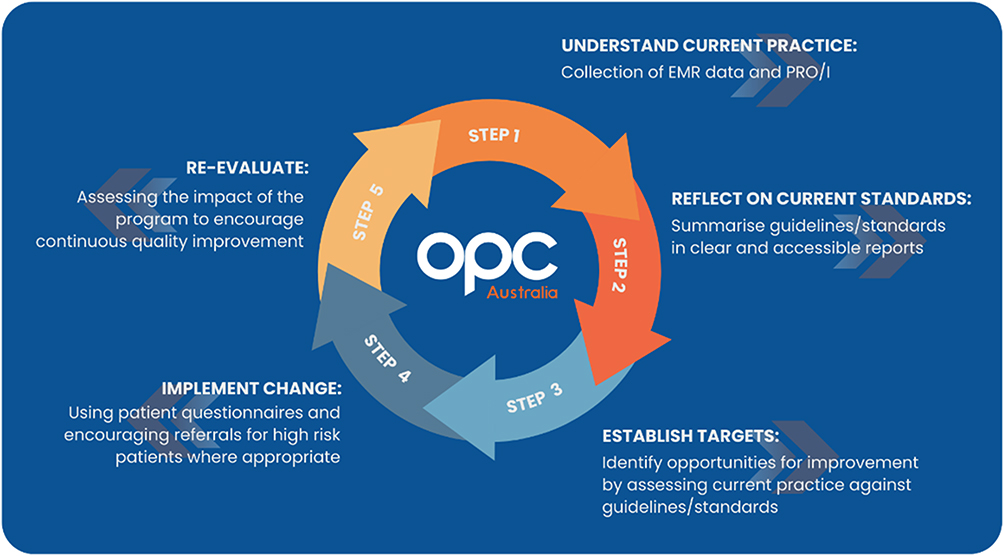 |
Figure 1 The cycle of quality improvement in primary care. Adapted from Evans A, Soremekun S, Stanley B, et al. Strategies that promote sustainability in quality improvement activities for chronic disease management in healthcare settings: A practical perspective. Quality in Primary Care. 2020;28(6):55–60. Licensed under CC BY 4.0.23 |
For the purposes of this study, we will focus on Steps 4 and 5 of the OPCA cycle of quality improvement above. That is, implementing change using patient questionnaires, and assessment of the program to encourage continuous quality improvement. The ACAER asthma and COPD program collected EMR data to provide reports to each primary care practice, comparing current clinical practice against quality standards. These EMR data were supplemented with PRO/I data collected through the provision of patient questionnaires, which were designed to be completed prior to the patient’s clinic visit and supply GPs with useful clinical information that might not be well reported in the EMR, in the form of a patient report.
The aim of the present investigation was to evaluate the ACAER asthma and COPD program in supporting primary care in the subset of patients who had both EMR reporting and received a pre-consultation questionnaire and were deemed to be at high risk of exacerbations (having had one or more exacerbations in the 2 years prior to being sent the questionnaire). The primary outcome was reduced exacerbations rates; treatment changes were also assessed as a secondary outcome.
Methods
Study Design and Population
This was an observational cohort study that utilized data from the Optimum Patient Care Research Database Australia (OPCRDA).24,25 The OPCRDA was established, and is maintained, by the OPCA for the purpose of providing anonymized datasets for ethically approved studies. It is a real-world, longitudinal, research database that contains anonymized EMR data from over a million patients from primary care and respiratory and allergy specialist practices across Australia. Australia has a universal healthcare system, available to all residents,26 however this does not fully cover general practices, which often charge top-up fees.27 Participating practices set up their electronic health record system to allow only patient data that has been de-identified to flow to OPCA. This excludes any individual patients who have opted out of data sharing.24 For the purposes of our study, patient data was collected from primary care only, from 21 practices across 5 Australian states or territories, Queensland (8), New South Wales (9), Australian Capital Territory (1), Victoria (1) and South Australia (2) who participated in the ACAER asthma and COPD program. The majority of practices included in the study were from metropolitan regions, and so the patient sample used may be less representative of the rural and remote primary care practice patient population.
Eligible patients were individuals aged ≥12 years with a documented diagnosis of asthma or COPD and who had received asthma or COPD therapy in the last 2 years. Patients were excluded from the study if they had a diagnosis of any chronic respiratory condition other than asthma or COPD, for example cystic fibrosis, in addition to asthma or COPD. Code lists utilized in operationalization of measures can be made available for replication analyses.
The intervention consisted of linked questionnaires that were completed by patients as part of practice evaluation and quality improvement (Figure 2A and B). The questionnaires were structured to include questions on exacerbations including hospital or emergency department visits, symptom control, current medication use and smoking history. Questionnaires were mailed to patients, who had the option to complete them on paper or online via a link provided. The intervention date varied between individuals; eligible patients received a questionnaire between 29 October 2019 and 21 September 2021. This period is treated as the intervention period for the purposes of this study. Participating practices sent the de-identified questionnaires to OPCA who manually entered the data into the database; these data were then linked with the EMR data. GPs were given reports comprising EMR data supplemented with PRO/I data from the patient questionnaires.
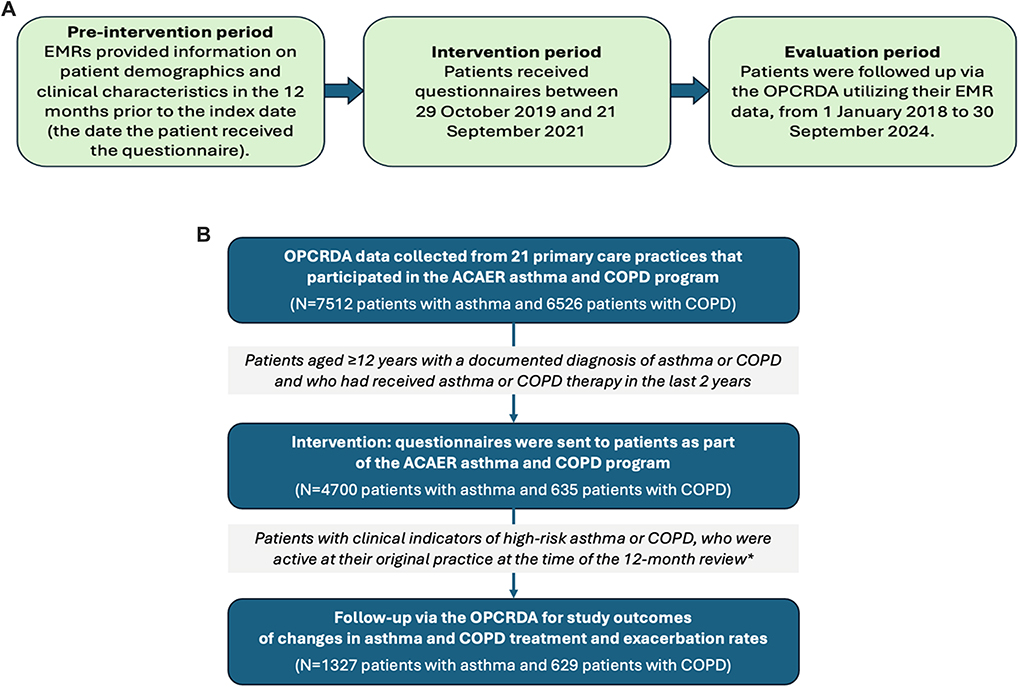 |
Figure 2 Study design. (A) Study periods. (B) Patient recruitment, intervention and follow-up. *“High risk” was defined as one or more exacerbations in the 2 years prior to the index date (the date the questionnaire was sent). “Active” was defined as the presence of at least one documented primary care consultation in a given year or subsequent year. |
Patients were followed up via the OPCRDA utilizing their EMR data. For inclusion in this evaluation period, patients were required to have clinical indicators associated with a high risk of exacerbation and hospitalization: one or more exacerbations in the 2 years prior to the index date (the date the questionnaire was sent). They were also required to be active patients at their original practice at the time of the 12-month review. Patients were defined as being “active” if they had at least one documented primary care consultation and/or therapy record in that year or were active both before and after a given year. The evaluation period describes the time frame over which patients who were sent the questionnaire were followed up via the OPCRDA utilizing their EMR data. This evaluation period extended from 1 January 2018 to 30 September 2024.
Variables Collected and Study Outcomes
EMRs provided information on demographics (age, gender) and clinical characteristics including comorbidities, biomarkers (eg eosinophil blood count) and exacerbations in the preceding 12 months. Asthma exacerbation was defined as a prescription listed in the EMR for a course of acute OCS (defined as ≥20 mg/day for a minimum of 3 days) in a 12-month period. COPD exacerbations were defined by EMR codes, key words or free text denoting COPD exacerbations or a prescription of acute OCS (≥20 mg/day for a minimum of 3 days), and/or a respiratory antibiotic in the absence of an alternative indication. Patient-completed questionnaires captured information on sociodemographic factors, body mass index (BMI), hospitalizations, emergency room visits, current medications, symptom frequency and smoking.
The primary study outcome was change in exacerbation rate, with changes in maintenance inhaled asthma and COPD treatment evaluated as a secondary outcome. We restricted to individuals who were active between 1 January 2018 to 31 December 2023 to evaluate trends over time in the same cohort of individuals. Exacerbation rate was calculated from exacerbations recorded in the EMR, and did not include those reported by the patient. Patients were followed up for exacerbations throughout the evaluation period, from 2018 to 2023. A change in therapy was defined as any change in asthma or COPD medication (ICS, LABA, LAMA and combinations), doses or device types (DPI, MDI) in the first 12 months post-intervention (ie from the index date) versus the most recent therapy received in the 12 months pre-intervention. Free and fixed inhaled combination therapy were grouped together. Any changes in therapy in the 2-, 3-, 4-years post-intervention were also recorded. To note, descriptions of how therapy was changed and guideline concordance were not specifically evaluated.
Statistical Analysis
Statistical analysis was performed using Stata statistical software (version 15.1). We described the characteristics of the study population by age, gender and BMI, stratified by COPD, asthma and high-risk asthma status.
For both high-risk asthma and COPD patients, exacerbation rates (per 1000) pre- and post-intervention with (exact Poisson) 95% confidence intervals were described. Exacerbation rates (per 1000 population) were plotted by month from 2018 to 2023 using fitted linear regression lines to evaluate trends pre- and post-intervention. As the intervention date varied between individuals, pre-intervention trend lines were plotted from Jan 2018 to Sep 2019 and post-intervention trend lines from May 2021 to Dec 2023 when most patients (92% for both severe asthma and COPD cohorts) had received the intervention. We repeated the analyses to report the exacerbations by year. To assess whether the intervention had prompted a change in maintenance therapy, the proportion of patients that changed therapy (and exact binomial 95% confidence intervals) for each year post-intervention was plotted, also stratifying by asthma/COPD status.
Results
Patient Demographics and Clinical Characteristics
OPCRDA data were collected from 7512 patients with asthma, of whom 4700 received a questionnaire (Figure 2B). Of these, 1463 were identified as high-risk; a subset of 1327 patients were classified as active and high-risk asthma intervention patients (92.4% of the total high-risk asthma patients). The mean age of high-risk asthma patients was 47.6 years (SD 20.6) and 68.1% of this population were female (31.7% male and 0.2% not recorded). Blood eosinophil counts are presented in Table 1. A total of 47.3% were prescribed acute OCS in the 12 months before the index date; long-term OCS were prescribed in 4.4%.
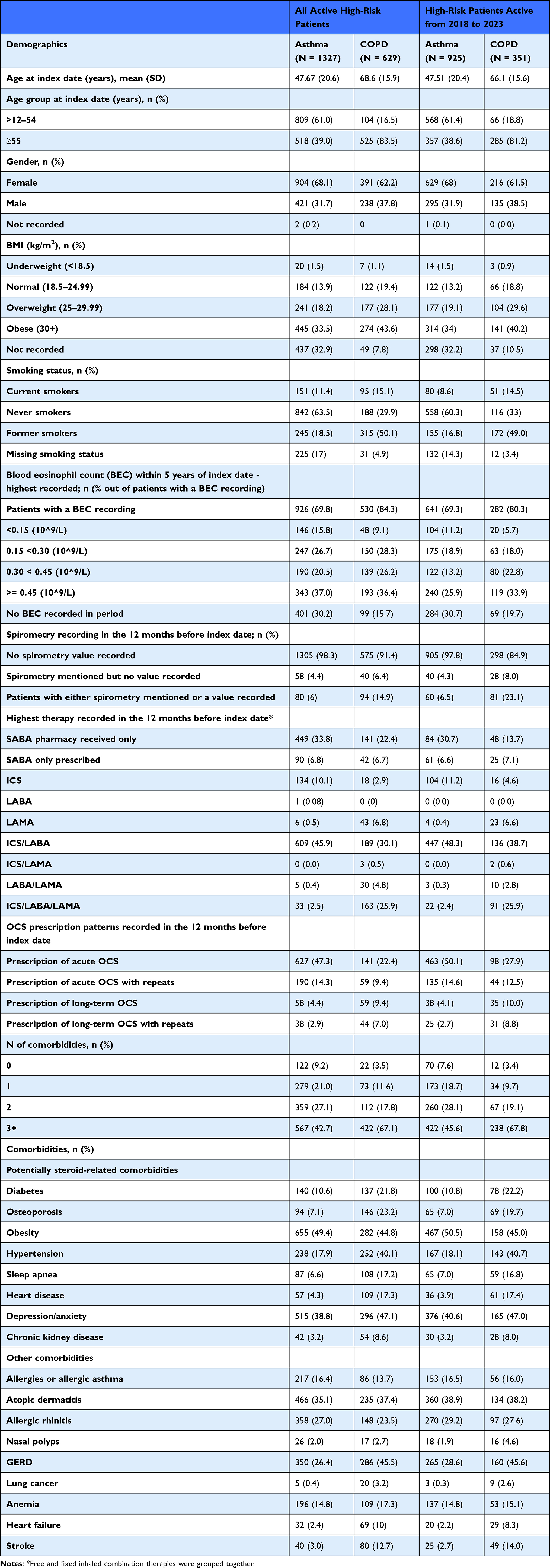 |
Table 1 Patient Characteristics |
OPCRDA data were collected from 6526 patients with COPD; 635 of these patients received a questionnaire (Figure 2B). Of these, 629 were identified as high-risk COPD patients, and all the high-risk COPD patients were found to be active. The mean age of high-risk COPD patients was 68.6 years (SD 15.9) and the majority were female (62.2%; 37.8% were male). In the 12 months before the index date, 22.4% were prescribed acute OCS and 9.4% were prescribed long-term OCS. Baseline demographics and clinical characteristics of the asthma and COPD cohorts are presented in Table 1. Spirometry reporting was very low; just 6.0% of high-risk asthma patients and 14.9% of high-risk COPD patients had mention of spirometry or a value recorded in their EMR. This meant that diagnoses of asthma or COPD could not be confirmed with spirometry.
Exacerbation Rates in High-Risk Asthma and COPD Patients
The overall rate of exacerbations among high-risk asthma patients in the entire study population (N=1327) was 776.9 per 1000 (730.2, 825.9) in the 1-year period pre-intervention. In the year post-intervention, this lowered to 368.5 per 1000 (336.5, 402.7). The rate of exacerbations in those active between 2018 and 2023 (N=925; see Table 1 for characteristics) by month is shown in Figure 3. The rate of exacerbations pre-intervention was 74.8 per 1000 per month ([95% CI] 71.1, 78.6) and post-intervention was 32.4 per 1000 per month (30.4, 34.6). Among patients with high-risk asthma, there was an increase in exacerbation rates in the pre-intervention period (linear regression trend: 2.79 exacerbations per 1000 per month [1.34, 4.24]; p=0.001). Exacerbation rates dropped after the intervention and did not rise again for the remainder of the evaluation period (p=0.87; up to 2023). For COPD patients, the overall rate of exacerbations in the entire sample (N=629) was 965.0 per 1000 (889.8, 1044.9) in the 1-year period pre-intervention. In the year post-intervention, this lowered to 756.8 per 1000 (690.2, 827.9). The rate of exacerbations in those active between 2018 and 2023 (N=351; see Table 1 for characteristics) by month is presented in Figure 4. The rate of exacerbations reported among high-risk COPD patients was higher than that reported among asthma patients and was also higher pre-intervention compared with post-intervention: 122.9 per 1000 per month (115.2, 131.0) pre-intervention vs 91.2 per 1000 per month (84.1, 98.3) post-intervention. Among patients with high-risk COPD, the exacerbation rate was stable in the pre-intervention period (p=0.29), and was lower, but also stable (p=0.28) for the remainder of the evaluation period.
 |
Figure 3 Rate (per 1000) of exacerbations among active high-risk asthma patients: 2018 to 2023 (N=925). Note: The greyed-out area represents the date of the intervention period: that is, the date that the first questionnaire was sent out (29 October 2019) to the date the last questionnaire was sent out (21 September 2021). |
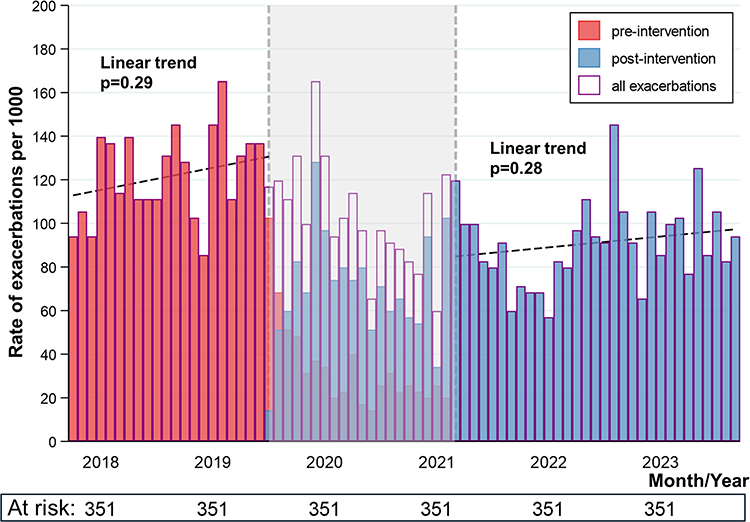 |
Figure 4 Rate (per 1000) of exacerbations among active high-risk COPD patients: 2018 to 2023 (N=351). Note: The greyed-out area represents the date of the intervention period: that is, the date that the first questionnaire was sent out (29 October 2019) to the date the last questionnaire was sent out (3 June 2021). |
Therapy Changes in High-Risk Asthma and COPD Patients
Maintenance therapy changes for both the high-risk asthma (N=925) and COPD (N=351) patient populations at risk between 2018 to 2023 were high post-intervention (Figure 5). In the first year following the intervention, 48.4% (95% CI: 45.2, 51.7) of high-risk asthma patients changed asthma therapies. This reduced to 38.9% (35.8, 42.1) and 29.7% (26.8, 32.8) in year 2 and 3 post-intervention. The rate of therapy change was higher among the high-risk COPD patients, but a similar pattern was observed over time: 59.3% (53.9, 64.4) in year 1, followed by 51.0% (45.6, 56.3) and 39.6% (34.4, 44.9) in years 2 and 3, respectively. Of the high-risk asthma patients, 68.1% (N=630) had changed therapy at least once during the 4-year follow-up period. A higher proportion of patients with therapy change (80.6%; N=283) was observed in the high-risk COPD patients.
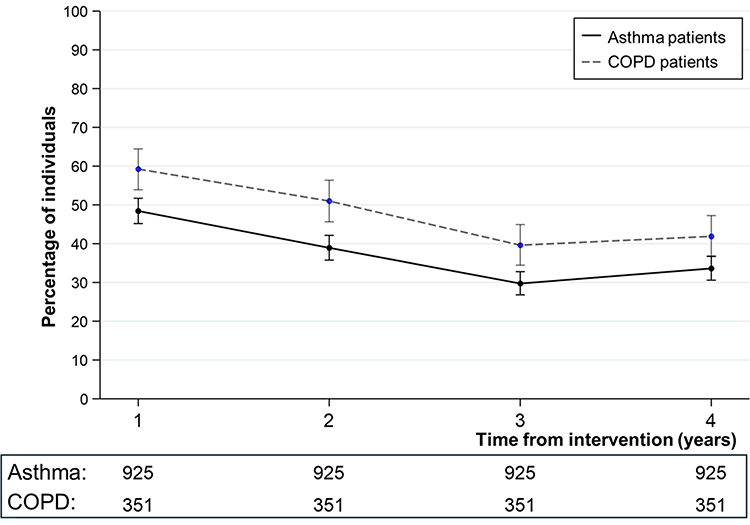 |
Figure 5 Percentage of active high-risk asthma (N=925) and COPD patients (N=351) changing therapy in the first five years post-intervention. |
Discussion
Our findings highlight the potential of the ACAER asthma and COPD program to support GPs in asthma and COPD care, with reductions in exacerbations observed in the post-intervention evaluation period. The program was provided to 21 primary care practices across Australia, resulting in 7512 patients with asthma and 6526 patients with COPD being identified, of whom 1463 and 629, respectively, were flagged to the GP as being high risk and requiring optimization of care.
The reduction in exacerbation rate post-ACAER implementation supports a role for the ACAER asthma and COPD program in real-world primary care practice. The mean rate of exacerbations fell after the intervention period in both the high-risk asthma and COPD populations, with a more pronounced reduction seen in patients with asthma (74.8 to 32.4 per 1000 per month) than in those with COPD (122.9 to 91.2 per 1000 per month). Prior to the ACAER implementation, a trend for increase in exacerbation rates (p=0.001) was observed in the high-risk asthma population; after the intervention period a pronounced reduction was observed, and rates remained stable over the follow-up period up till 2023 (p=0.87). In the high-risk COPD population, the exacerbation rate was stable prior to the ACAER implementation (p=0.29). Post-intervention exacerbation rates initially declined and then remained stable (p=0.28).
Reductions in exacerbation rate may reflect improvements in management of asthma and COPD. Identification of high-risk asthma and COPD patients was followed by changes in treatment regimen among the majority of patients post-intervention. Around half (48.4%) of patients in the high-risk asthma population and more than half (59.3%) in the high-risk COPD population had a therapy change in the first year post-ACAER implementation, with this figure declining year-on-year for the subsequent four years. Of those high-risk patients who remained in the cohort for 4 years following the intervention, most individuals (68.1% of the asthma patients and 80.6% of the COPD patients) had at least one therapy change.
Primary care providers are at the forefront of asthma management and have a critical role in the early identification and management of uncontrolled asthma and COPD.28,29 As such, it is imperative that they are supported with QI programs similar to the ACAER asthma and COPD program that can use EMR data and algorithms to identify high-risk patients early in their clinical journey. Identification of these patients allows them to be targeted for referral and review, adjusting maintenance regimens as appropriate with a view to enhancing outcomes. The findings reported here are consistent with those of a COPD QI program implemented by the OPC in the UK. A 20% reduction was demonstrated in the proportion of high-risk patients having a COPD exacerbation in the 12 months following the start of this program, compared to a reduction of 10% in all practices not actively performing QI.23
Existing literature highlights the important role of QI in supporting GPs with the early identification of at-risk patients, helping to ensure the provision of timely and quality care with the end goal of enhancing patient outcomes.23,30,31 Previous studies have demonstrated the effectiveness of QI programs in reducing exacerbations amongst patients with asthma and COPD. The Giving Asthma Support to Patients (GASP) program was a nurse-led asthma review program conducted in GP practices across Australia and showed a 21.6% decrease in exacerbations 12 months after receiving the program.30 This study differed to ours as we did not provide nurse intervention and relied solely on the GPs to implement changes. The UK Standardising Asthma Reviews and Reducing SABA overuse in Greater Manchester (STARRS-GM) study used clinical auditing to identify high-risk asthma patients and a computer-guided consultation (CGC) system to enhance the outcomes of asthma patients in primary care. This study found that 44% of patients enrolled in the program underwent a change in asthma therapy following the CGC review; of these patients, 82% received an escalation in their therapy.31 This study shows the value of using collected EMR data to flag high-risk patients eligible for treatment reviews, a model that mirrors the ACAER asthma and COPD program. A primary care audit on COPD care in Hong Kong aimed to identify service gaps and implement a series of quality improvement strategies. Improvements in all criteria evaluated following the year-long implementation phase were reported, including spirometry performance and acute exacerbations leading to hospital admissions.32
Our study had several limitations. We assessed whether the intervention prompted an overall change in maintenance therapy, rather than specifically evaluating guideline concordance. This was, in part, due to the potential for guideline adherence and doctor-specific factors to confound any potential relationship observed. Our study was completed during the COVID-19 pandemic, and this could have influenced the post ACAER asthma and COPD program results. On average the number of patients participating in the study decreased and it can be expected that lifestyle changes could have affected the control of their asthma or COPD. A number of studies across the globe report substantial reductions in exacerbations of both asthma33–35 and COPD36–38 associated with lockdown over the COVID-19 pandemic. Several potential explanations for this have been proposed, including reduced infection exposure with social distancing and occupational changes and improvements in self-management of these conditions over the lockdown period.34,35,37 Reporting on COPD exacerbations in France, Germany, Italy, the UK and the US, Martinez et al found that the reported decline in 2020 compared with 2019 was followed by a subsequent rise in exacerbation rates in most countries in 2021.38 In contrast to this, our study appeared to show sustained reductions over the post-intervention years up until 2023, supporting a tangible effect of the intervention on patient outcomes. Nonetheless, our findings may not be generalizable to other time periods and further research is required to support our initial findings here. An additional limitation of our study is the exclusion of patients with respiratory diagnoses other than asthma or COPD may have made our findings less generalizable to the general population of patients with asthma or COPD, as many of them may have respiratory comorbidity. Finally, the population size was small, rates were not adjusted for confounders and the study did not report on a control group, making it challenging to ascertain the true effectiveness of the program. We were unable to examine the same longitudinal patterns in patient outcomes in the control group as this group received a delayed intervention which, when taking COVID into consideration, made it unsuitable for comparison. For this reason, only the intervention population was examined longitudinally to demonstrate the sustained effects of our QI program.
Future Research
To counteract the lack of control group, future research could analyze available and forthcoming data using a stepped-wedge-type approach, with a type of control group essentially being offered by the practices that had not yet joined by a particular date. Reporting of relative rate ratios of exacerbations would help to better understand any improvements in the management of asthma and COPD. Future studies could explore the differences between pediatric and adult asthma patients, the decrease in morbidity and hospital admissions and the improvement in activities of daily living with the suggested changes in management, as well as quality improvement among asthma–COPD overlap patients. The therapy change of stopping chronic OCS could also be examined, and an exploration of patient experiences of ACAER and analysis of cost-effectiveness may offer additional insights.
Conclusions
Our findings support the potential of the ACAER asthma and COPD program to facilitate sustained reductions in exacerbation rates among patients with high-risk asthma and COPD. The implementation of the program was followed by changes in care in the majority of high-risk patients identified, which appear to have been reflected in the reductions in exacerbation rate in the years following the intervention. Importantly, the ACAER asthma and COPD program was designed to be highly sustainable in primary care practice, with reports and templates that can be embedded in routine care so as to support everyday clinical decision making. While additional research is required to confirm our preliminary insights, the adoption of QI initiatives such as the ACAER program more broadly across the country may help to improve patient outcomes and reduce the burden of disease.
Abbreviations
ACAER, Achieving Clinical Audits with Electronic Records; BMI, body mass index; COPD, chronic obstructive pulmonary disease; EMR, electronic medical record; GINA, Global Initiative for Asthma; GP, general practitioner; ICS, inhaled corticosteroid; LABA, long-acting beta agonist; OPCRDA, Optimum Patient Care Research Database Australia; OCS, oral corticosteroid; QI, quality improvement.
Data Sharing Statement
The data cannot be shared publicly, and authors do not have the authority to share the data. However, the data can be made available to researchers who meet the criteria for access to confidential data and have appropriate data-sharing agreements in place. Requests for access to these datasets should be directed to: https://www.optimumpatientcare.org.au/opcrda or via the enquiries Email [email protected].
Ethics Approval
The OPCRDA has ethical approval from The Royal Australian College of General Practitioners (RACGP) National Research and Evaluation Ethics Committee (NREEC) to hold and process anonymized research data (NREEC Reference: 18-013). Approval for this study was granted by the Anonymised Data Ethics Protocols and Transparency (ADEPT) committee – the independent scientific advisory committee for the OPCRDA (ADEPT1820). Registration of the OPCRDA database and study with the European Union Electronic Register of Post-Authorization studies were also undertaken (ENCEPP/DSPP/38991; EUPAS1000000426). The dataset used within this study was provided via the OPCRDA. The OPCRDA employs an opt out approach to patient consent in adherence with section 2.3.6 of the Australian national statement on ethical conduct in human research (2023).
Acknowledgments
Writing, editorial support, and/or formatting assistance in the development of this manuscript was provided by Shilpa Suresh, MSc, of the Observational and Pragmatic Research Institute, Singapore. Data from OPCRDA was collected through the Achieving Clinical Audits with Electronic Records Asthma and COPD program, which is part-funded by GlaxoSmithKline (GSK), AstraZeneca, Novartis, and Optimum Patient Care Australia (OPCA). Funding for this study was partially provided by OPCA and GSK. GSK was provided the opportunity to review a preliminary version of this publication for factual accuracy, but the authors are solely responsible for final content and interpretation.
Collaborators
We wish to acknowledge and thank Joseph Doan, Russell Wiseman, Ata Kichkin, Chi Ming Lau, Dominique Novic, Ian Miles, John Pakos, Josephine Samuel-King, Lisa Sugg, Majella Soumakiyan, Marion Magee, Nicole O’Sullivan, Ondrej Rejda, Rob Campbell, Sheryl Bradley, Ying Liu in Australia Research Group for their valuable contributions in making this publication possible.
Funding
Funding for this study was partially provided by Optimum Patient Care Australia and GlaxoSmithKline (GSK).
Disclosure
John D. Blakey has received grants or contracts from Asthma Australia, MRFF, FHRI, Telethon Kids Institute, International Primary Care Respiratory Group, and the Charlies Foundation for Research. He has received payment or honoraria for lectures, presentations, or speaker bureaus from Chiesi, The Limbic, Boehringer Ingelheim, GlaxoSmithKline, AstraZeneca, and Sanofi. He has received support for attending meetings and/or travel from GlaxoSmithKline, Centre for Research Excellence in Treatable Traits, AstraZeneca, and The George Institute. He has participated in the study steering committee of GlaxoSmithKline, unrelated to this work. He has taken a leadership role in the Thoracic Society of Australia and New Zealand, and Asthma Australia. He has received medical writing/equipment from GlaxoSmithKline, and Novartis. Biljana Cvetkovski has received honoraria from GSK, SAnofi and Viatris for educational presentations and advisory boards. Prof Peter Smith has advisory board membership with Viatris, Hyloris, and Menarini. He has an unrestricted funding for investigator-initiated studies with GSK and Sanofi. He has NH&MRC funding for research. Philip J Thompson served on advisory boards & provided consultancies for Astra Zeneca, CSL Behring, Boehringer Ingelheim, Grifols, GlaxoSmithKline, and Novartis. In the last 12 months, he received honoraria from GlaxoSmithKline and Sanofi for presentations. Mark Hew is a steering committee of the ERS CONNECT Clinical Research Collaboration. He declares grants and other advisory board fees (made to his institutional employer) from AstraZeneca, Aravax, GlaxoSmithKline, Chiesi, Novartis, Stallergenes, Seqirus, Sanofi, and Teva, for unrelated projects. Kerry L. Hancock has received speakers fees, consulting honoraria and/or travel grants from AstraZeneca, Chiesi, Cipla,GlaxoSmithKline, and Sanofi. She receives fees from a spirometry training program for health care workers. Sinthia Z. Bosnic-Anticevich has received honorarium for participation in expert advisory boards and given lectures for Teva Pharmaceuticals, AstraZeneca, GlaxoSmithKline, Meda/Mylan, Sanofi, Mylan, Chiesi, Menarini, Sanofi, Boehringer Ingelheim, Abbvie and received unrestricted research grants from Mylan, AstraZeneca, Teva, AstraZeneca, GlaxoSmithKline, and Viatris. Anita Sharma is a practising Primary Care Physician and Senior Lecturer, School of ClinicalMedicine-Primary Care Clinical Unit, University of Queensland. She supervizes clinical training of primary care doctors and serves on advisory boards for Diabetes, Heart Failure and Osteoporosis for Novartis, Merck Sharp & Dohme and Boehringer Ingelheim, Eli Lilley and Amgen. Freya Tyrer and John Townend are employees of Observational Pragmatic Research Institute, United Kingdom. Porsche Le Cheng, Chantal Le Lievre, Alexander Roussos, Nicholas Bushell, Fabio Botini, Paola Accalai and Thao Le are employees of Optimum Patient Care, Queensland, Australia. Victoria Carter is an employee of Optimum Patient Care Australia and has 5% shareholding of Optimum Patient Care Australia. David Price has advisory board membership with AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, Viatris, Teva Pharmaceuticals; consultancy agreements with AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, Viatris, Teva Pharmaceuticals; grants and unrestricted funding for investigator-initiated studies (conducted through Observational and Pragmatic Research Institute Pte Ltd) from AstraZeneca, Chiesi, Viatris, Novartis, Regeneron Pharmaceuticals, Sanofi Genzyme, and UK National Health Service; payment for lectures/speaking engagements from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, Inside Practice, GlaxoSmithKline, Medscape, Viatris, Novartis, Regeneron Pharmaceuticals and Sanofi Genzyme, Teva Pharmaceuticals; payment for travel/accommodation/meeting expenses from AstraZeneca, Boehringer Ingelheim, Novartis, Medscape, Teva Pharmaceuticals.; owns 74% of the social enterprise Optimum Patient Care Ltd (Australia and UK), 92.61% of Observational and Pragmatic Research Institute Pte Ltd (Singapore) and 5% shareholding in Timestamp which develops adherence monitoring technology; is peer reviewer for grant committees of the UK Efficacy and Mechanism Evaluation programme, and Health Technology Assessment; and was an expert witness for GlaxoSmithKline. The authors report no other conflicts of interest in this work.
References
1. Chronic respiratory conditions, About. Australian Institute of Health and Welfare; 2024. Available from: https://www.aihw.gov.au/reports/chronic-respiratory-conditions/chronic-respiratory-conditions/contents/about.
2. What is severe asthma. Severe Asthma Toolkit. Available from: https://toolkit.severeasthma.org.au/severe-asthma/overview/.
3. Hancock KL, Bosnic-Anticevich S, Blakey JD, et al. Characterisation of the Australian adult population living with asthma: severe - exacerbation frequency, long-term OCS use and adverse effects. Pragmat Obs Res. 2022;13:43–58. doi:10.2147/POR.S360044
4. Geographic distribution of asthma and chronic obstructive pulmonary disease hospitalisations in Australia: 2007–08 to 2009–10, Summary. Australian Institute of Health and Welfare; 2013. Available from: https://www.aihw.gov.au/reports/chronic-respiratory-conditions/geographic-distribution-of-asthma-and-chronic-obst/summary.
5. Chronic disease and infection: potentially preventable hospitalisations. Australian Commission on Safety and Quality in Health Care. Available from: https://www.safetyandquality.gov.au/our-work/healthcare-variation/fourth-atlas-2021/chronic-disease-and-infection-potentially-preventable-hospitalisations.
6. Reddel HK, Valenti L, Easton KL, Gordon J, Bayram C, Miller GC. Assessment and management of asthma and chronic obstructive pulmonary disease in Australian general practice. Aust Fam Physician. 2017;46(6):413–419.
7. Australian asthma handbook. Available from: https://www.asthmahandbook.org.au/.
8. Reddel HK, Foxley GJ, Davis SR. How to step down asthma preventer treatment in patients with well-controlled asthma - more is not always better. Aust Prescr. 2022;45(4):125–129. doi:10.18773/austprescr.2022.033
9. Price D, Bjermer L, Bergin DA, Martinez R. Asthma referrals: a key component of asthma management that needs to be addressed. J Asthma Allergy. 2017;10:209–223. doi:10.2147/JAA.S134300
10. Chung LP, Hew M, Bardin P, McDonald VM, Upham JW. Managing patients with severe asthma in Australia: current challenges with the existing models of care. Intern Med J. 2018;48(12):1536–1541. doi:10.1111/imj.14103
11. Bereznicki B, Walters H, Walters J, Peterson G, Bereznicki L. Initial diagnosis and management of chronic obstructive pulmonary disease in Australia: views from the coal face. Intern Med J. 2017;47(7):807–813. doi:10.1111/imj.13418
12. Perera B, Barton C, Osadnik C. General practice care following acute exacerbations of COPD: a survey of Australian general practitioners. PLoS One. 2023;18(4):e0284731. doi:10.1371/journal.pone.0284731
13. Price D, Jenkins C, Hancock K, et al. The association between short-acting β2-agonist over-prescription, and patient-reported acquisition and use on asthma control and exacerbations: data from Australia. Adv Ther. 2024;41(3):1262–1283. doi:10.1007/s12325-023-02746-0
14. Evans A, Hancock K, Dickens AP, et al. Identifying opportunities for optimising the management of high-risk COPD patients in Australia: an observational study. 2023. Available from: https://abdn.elsevierpure.com/en/publications/identifying-opportunities-for-optimising-the-management-of-high-r.
15. Ullman AJ, Ray-Barruel G, Rickard CM, Cooke M. Clinical audits to improve critical care: part 1 Prepare and collect data. Aust Crit Care. 2018;31(2):101–105. doi:10.1016/j.aucc.2017.04.003
16. Esposito P, Dal Canton A. Clinical audit, a valuable tool to improve quality of care: general methodology and applications in nephrology. World J Nephrol. 2014;3(4):249–255. doi:10.5527/wjn.v3.i4.249
17. Jamtvedt G, Flottorp S, Ivers N. Audit and feedback as a quality strategy. In: Improving Healthcare Quality in Europe: Characteristics, Effectiveness and Implementation of Different Strategies. European Observatory on Health Systems and Policies; 2019.
18. Ivers N, Yogasingam S, Lacroix M, et al. Audit and feedback: effects on professional practice. Cochrane Database Syst Rev. 2025;3(3). doi:10.1002/14651858.CD000259.pub4
19. Burgers JS, van der Weijden T, Bischoff EWMA. Challenges of research on person-centered care in general practice: a scoping review. Front Med. 2021;8:669491. doi:10.3389/fmed.2021.669491
20. World Health Organization. Monitoring the building blocks of health systems: a handbook of indicators and their measurement strategies. World Health Organization; 2010. Available from: https://iris.who.int/handle/10665/258734.
21. Patient Centred Health Care in Primary Care - National Asthma Council Australia. Available from: https://www.nationalasthma.org.au/living-with-asthma/resources/health-professionals/information-paper/patient-centred-health-care-in-primary-care.
22. COPD-X plan guidelines. COPD-X; 2015. Available from: https://copdx.org.au/copd-x-plan/.
23. Evans A, Soremekun S, Stanley B, et al. Strategies that promote sustainability in quality improvement activities for chronic disease management in healthcare settings: a practical perspective. Qual Primary Care. 2020;28(6):55–60. CC BY 4.0. doi:10.36648/1479-1064.28.6.124
24. OPCRDA. OPC Australia. Available from: https://www.optimumpatientcare.org.au/opcrda.
25. Optimum Patient Care Research Database Australia (OPCRDA). HMA-EMA Catalogues of real-world data sources and studies. Available from: https://catalogues.ema.europa.eu/node/986/data-flows-and-management.
26. Australian Government Department of Health, Disability and Ageing Care. The Australian health system. 2025. Available from: https://www.health.gov.au/about-us/the-australian-health-system.
27. Medicare bulk billing of GP attendances: monthly data, Dashboard. Australian Institute of Health and Welfare; 2025. Available from: https://www.aihw.gov.au/reports/medicare/medicare-bulk-billing-gp-attendances-monthly-data/contents/dashboard.
28. Chung LP, Johnson P, Summers Q. Models of care for severe asthma: the role of primary care. Med J Aust. 2018;209(2). doi:10.5694/mja18.00119
29. Walters J. COPD - Diagnosis, management and the role of the GP. Aust Fam Physician. 2010;39(3):100–103.
30. Zwar NA, Hasan I, Hayen A, et al. Giving Asthma Support to Patients (GASP) program evaluation. Aust J Gen Pract. 2022;51(4):257–261. doi:10.31128/AJGP-04-21-5942
31. Chakrabarti B, Kane B, Barrow C, et al. The feasibility and impact of implementing a computer-guided consultation to target health inequality in Asthma. NPJ Prim Care Respir Med. 2023;33(1):6. doi:10.1038/s41533-023-00329-8
32. Chen XRC, Fu SN, Leung WK, et al. Clinical audit on Chronic Obstructive Pulmonary Disease (COPD) management in primary care: a quality improvement project from Hong Kong. Int J Chron Obstruct Pulmon Dis. 2021;16:1901–1911. doi:10.2147/COPD.S304527
33. Shah SA, Quint JK, Sheikh A. Impact of COVID-19 pandemic on asthma exacerbations: retrospective cohort study of over 500,000 patients in a national English primary care database. Lancet Reg Health Eur. 2022;19:100428. doi:10.1016/j.lanepe.2022.100428
34. Salciccioli JD, She L, Tulchinsky A, Rockhold F, Cardet JC, Israel E. Effect of COVID-19 on asthma exacerbation. J Allergy Clin Immunol Pract. 2021;9(7):2896–2899.e1. doi:10.1016/j.jaip.2021.04.038
35. Chan AHY, Tomlin A, Chan E, Harrison J, Beyene KA. Effect of the COVID-19 pandemic on asthma exacerbations in New Zealand: an interrupted time series analysis. J Allergy Clin Immunol. 2023;2(4):100157. doi:10.1016/j.jacig.2023.100157
36. Alsallakh MA, Sivakumaran S, Kennedy S, et al. Impact of COVID-19 lockdown on the incidence and mortality of acute exacerbations of chronic obstructive pulmonary disease: national interrupted time series analyses for Scotland and Wales. BMC Med. 2021;19(1):124. doi:10.1186/s12916-021-02000-w
37. Awatade NT, Wark PAB, Chan ASL, et al. The Complex Association between COPD and COVID-19. J Clin Med. 2023;12(11):3791. doi:10.3390/jcm12113791
38. Martinez FJ, Papi A, Welte T, et al. COPD exacerbations before and during COVID-19 in France, Germany, Italy, the UK and the US. Int J Chron Obstruct Pulmon Dis. 2024;19:1433–1445. doi:10.2147/COPD.S451009
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.