Back to Journals » Clinical Ophthalmology » Volume 19
A 12-Month Multicenter Postmarketing Clinical Study of a Trifocal Intraocular Lens in a Chinese Population
Authors Liu X, Bao Y, Lu Y, Fan W, Bi H, Zhang H, Chen W, Liu J, Song X, Pang Y, Yao K ![]()
Received 21 May 2025
Accepted for publication 7 October 2025
Published 7 November 2025 Volume 2025:19 Pages 4117—4127
DOI https://doi.org/10.2147/OPTH.S541613
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Xin Liu,1 Yongzhen Bao,2 Yi Lu,3 Wei Fan,4 Hongsheng Bi,5 Hong Zhang,6 Weirong Chen,7 Jiewei Liu,8 Xudong Song,9 Yilin Pang,10 Ke Yao1
1Eye Center of the Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2Department of Ophthalmology, Peking University People’s Hospital, Beijing, People’s Republic of China; 3Department of Ophthalmology, Eye & ENT Hospital of Fudan University, Shanghai, People’s Republic of China; 4Department of Ophthalmology, West China Hospital of Sichuan University, Chengdu, People’s Republic of China; 5Affiliated Eye Hospital of Shandong University of Traditional Chinese Medicine, Jinan, People’s Republic of China; 6Department of Cataract, Ophthalmology, Tianjin Medical University Eye Hospital, Tianjin, People’s Republic of China; 7State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-Sen University, Guangdong Provincial Key Laboratory of Ophthalmology and Visual Science, Guangzhou, People’s Republic of China; 8Department of Cataract, Ophthalmology, Shanxi Eye Hospital, Taiyuan, People’s Republic of China; 9Eye Center, Beijing Tongren Hospital Capital Medical University, Beijing, People’s Republic of China; 10Clinical Development, Alcon (China) Ophthalmic Product Co., Ltd, Beijing, People’s Republic of China
Correspondence: Ke Yao, Eye Center of the Second Affiliated Hospital, Zhejiang University School of Medicine, 1# Xihu Road, Shangcheng District, Hangzhou, Zhejiang Province, 310009, People’s Republic of China, Email [email protected]
Purpose: This 12-month, prospective, single-arm, postmarketing study assessed efficacy, safety, and patient satisfaction for AcrySof IQ PanOptix TFNT00 intraocular lens in a Chinese population.
Patients and Methods: Adults with bilateral cataracts received TFNT00 (286 eyes); visual acuity (VA) was assessed at 12 months. Manifest refraction spherical equivalent (MRSE), corrected and uncorrected distance VA (CDVA, UDVA), distance-corrected and uncorrected intermediate (DCIVA, UIVA) and near (DCNVA, UNVA) VA, and defocus curve were evaluated. Patient-reported outcomes were assessed using questionnaires. Adverse events (AEs) were evaluated.
Results: 134/144 patients (268/286 eyes) completed the study. At 12 months, MRSE was − 0.06± 0.36 D. Monocular and binocular CDVA ≤ 0.3 logMAR was achieved in 99.3% of patients. Mean±SD monocular CDVA, UDVA, DCIVA, UIVA, DCNVA, and UNVA were − 0.01± 0.13, 0.04± 0.13, 0.076± 0.14, 0.089± 0.14, 0.084± 0.13, and 0.096± 0.13 logMAR, respectively. Binocular VA was equal to or better than 0.1 logMAR for defocus range +0.5 to − 3.0 D. Most patients achieved spectacle independence for distance (94%), intermediate (90%), and near (87%) vision; 88% were “satisfied” or “very satisfied.” No device-related AEs were reported. Forty eyes (14%) had posterior capsular opacity (37 were clinically nonsignificant; 1 [0.4%] required posterior capsulotomy). Five cystoid macular edema cases (1.7%) were reported. Severe starbursts, halo, and glare were reported by 15.6%, 4.4%, and 2.3% of patients, respectively, with only 1.5% of patients significantly bothered by each.
Conclusion: TFNT00 was safe and effective in a Chinese population, providing good VA at far, intermediate, and near distances, with high rates of spectacle independence and patient satisfaction.
Keywords: cataract surgery, intermediate visual acuity, PanOptix TFNT00, presbyopia
Introduction
Cataract is a leading cause of blindness worldwide, with prevalence increasing with age.1 Surgery, an effective treatment in patients with cataracts, entails replacing the clouded crystalline lens with an artificial intraocular lens (IOL).2 Monofocal IOLs provide good vision, but only at one focal distance, and patients often desire clearer intermediate and near vision as well.2,3 Presbyopia-correcting multifocal IOLs were designed with multiple focal points, using enhanced materials with the goal of providing better distance, intermediate, and/or near vision and improving spectacle independence.4,5
AcrySof IQ PanOptix IOL (Model TFNT00; Alcon Vision LLC, Fort Worth, TX, USA) is a trifocal IOL designed to provide patients with good visual acuity (VA) at far (5 m), intermediate (60 cm), and near (40 cm) distances.6 Compared with a monofocal IOL, TFNT00 displayed superior monocular distance-corrected near VA (DCNVA) and distance-corrected intermediate VA (DCIVA), as well as comparable corrected distance VA (CDVA).7
Although the TFNT00 IOL has been widely studied in recent years, most of the current clinical studies have a relatively short follow-up time and lack data from the Chinese population. The goal of this multicenter study was to assess efficacy, safety, and patient satisfaction with TFNT00 IOL in a Chinese population during the 12 months after implantation. This study utilized a longer follow-up period than most previously reported TFNT00 IOL clinical trials and is the largest to date in a Chinese population.
Methods
Study Design
This was a prospective, single-arm, multicenter, postmarketing study that enrolled patients from nine hospitals in different regions of China (Figure 1). Patients underwent cataract phacoemulsification combined with TFNT00 IOL implantation. The first eye was implanted on day 0 and the second eye 7 to 28 days after the first eye. Follow-up visits occurred 1 day and 1 week after each surgery and at months 1, 3, 6, and 12 (Figure 1). All patients with a successful IOL implantation in ≥1 eye who underwent ≥1 postoperative efficacy assessment were included in the analysis.
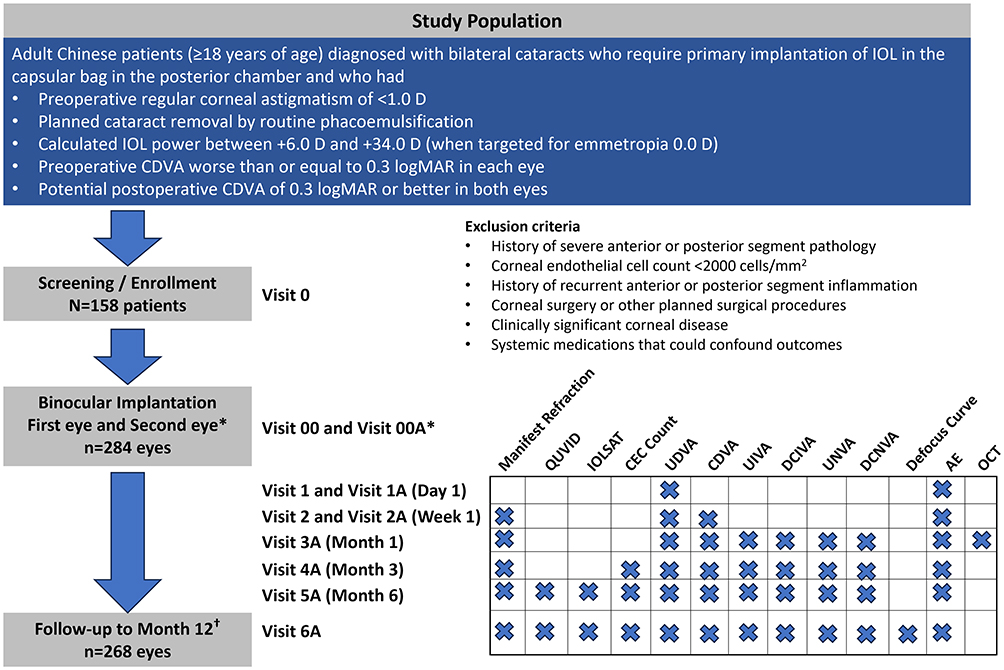 |
Figure 1 Study design. *Implantation in the second eye was performed 7–28 days after implantation in the first eye. †The full set analysis included all patients with successful IOL implantation and at least 1 postoperative efficacy assessment. Abbreviations: AE, adverse events; CDVA, corrected distance visual acuity; CEC, corneal endothelial cell; D, diopter; DCIVA, distance-corrected intermediate visual acuity; DCNVA, distance-corrected near visual acuity; IOL, intraocular lens; IOLSAT, Intraocular Lens Satisfaction questionnaire; logMAR, logarithm of the minimum angle of resolution; OCT, optical coherence tomography; QUVID, Questionnaire for Visual Disturbances; UDVA, uncorrected distance visual acuity; UIVA, uncorrected intermediate visual acuity; UNVA, uncorrected near visual acuity. |
The study (ClinicalTrials.gov identifier: NCT04755231; China registration: ChiCTR2100044482) was conducted in accordance with the Declaration of Helsinki and in compliance with Good Clinical Practice for medical devices and was approved by the Human Research Ethics Committee of the Second Affiliated Hospital of Zhejiang University School of Medicine. All patients provided written informed consent.
IOL Design and Material
TFNT00 is an ultraviolet- and blue-light–filtering, nonapodized, foldable, presbyopia-correcting, trifocal IOL designed to provide good VA at far (5 m), intermediate (60 cm), and near (40 cm) distances by adding a +2.17 diopter (D) and a +3.25 D power at the IOL plane.6 The single-piece IOL has a central biconvex optic, with an inner diffractive and an outer refractive zone and is made of a hydrophobic acrylate/methacrylate copolymer with two open-loop haptics.6 The lens diameter is 13.0 mm with a central 6.0-mm optic and a diopter range of +6.0 to +30.0 D (0.5-D increments) and +31.0 D to +34.0 D (1.0-D increments). The anterior surface is designed with negative spherical aberration to compensate for the positive spherical aberration of the average human cornea.
Patients
Included in the study were adults (≥18 years old) with bilateral cataracts who required primary IOL implantation in the capsular bag in the posterior chamber after cataract removal (Figure 1). Other inclusion criteria were preoperative regular corneal astigmatism <1.0 D, planned cataract removal by routine phacoemulsification, and calculated IOL power between +6.0 D and +34.0 D (when targeted for emmetropia 0.0 D). Patients had preoperative CDVA ≥0.3 logarithm of the minimum angle of resolution (logMAR) in each eye and potential postoperative CDVA ≤0.3 logMAR in both eyes based on the investigator’s expert medical opinion.
Exclusion criteria included history of severe anterior segment (corneal, anterior chamber, sulcus) or posterior segment (uveal, vitreoretinal) pathologic change, including retinal vascular occlusive disease, retinal detachment or peripheral retinal laser photocoagulation, age-related macular degeneration, glaucoma, diabetic retinopathy, retinitis pigmentosa, and any pathologic changes associated with the optic nerve. Additional exclusion criteria were corneal endothelial cell (CEC) count <2000 cells/mm2, clinically significant corneal diseases or severe xerophthalmia, and systemic medications that could confound the outcome or increase patient risk in the opinion of the investigator. Also excluded were patients who desired monovision correction, had other planned surgical procedures, or participated in other investigational studies.
Surgical Procedure
Phacoemulsification or femtosecond laser–assisted cataract surgery was carried out according to the investigator’s standard procedure; briefly, topical anesthesia was used and the IOLs were implanted through a 2-mm limbal corneal incision. IOL power was chosen to target emmetropia within 0.5 D. Postoperative topical therapy included dexamethasone-tobramycin (2 weeks) and pranoprofen (1 month). Any problems arising during surgery (eg, capsular tear, poorly dilated pupils, lens loop stuck in the ciliary sulcus) were evaluated as potential adverse events (AEs), and any additional surgery (eg, anterior vitrectomy, capsular tension ring) was recorded.
Endpoints
Visual acuity testing was conducted using standard logarithm VA charts at 5 m, 60 cm, and 40 cm. Primary efficacy endpoints were the percentage of eyes with CDVA of 0.3 logMAR or better, mean monocular and binocular CDVA, mean monocular and binocular DCIVA (60 cm), and mean monocular and binocular DCNVA (40 cm).
Supportive efficacy endpoints included mean monocular and binocular uncorrected distance VA (UDVA), mean monocular and binocular uncorrected intermediate (UIVA; 60 cm) and near (UNVA; 40 cm) VA, mean power of residual spherical equivalent after surgery, manifest refraction spherical equivalent (MRSE), and binocular defocus curve. Patients’ subjective visual quality, spectacle dependence, and expectation and satisfaction with their visual quality were assessed using the Intraocular Lens Satisfaction (IOLSAT) questionnaire at months 6 and 12 after surgery. Primary safety assessments included rates of ocular AEs and serious AEs (SAEs), rates of secondary surgical interventions, and rates of visual disturbances as reported using the Questionnaire for Visual Disturbances (QUVID).8 For starbursts, halos, glare, and other visual disturbances evaluated using QUVID, patients were asked to grade on a scale of 0 to 4 the frequency of, severity of, and how bothered they were by these disturbances. The proportion of visual disturbances that were reported as “severe” and “most bothersome” were collected as the primary safety endpoints.
Statistical Analysis
Data were analyzed using descriptive statistics. Continuous variables were described using sample size, mean, and standard deviation. The full analysis set (FAS) included all patients who had an IOL successfully implanted in at least one eye and had undergone at least one postoperative efficacy assessment. The safety analysis set included all patients with attempted IOL implantation. Eyes with AEs that occurred after IOL implantation were included in the study. Demographics and baseline characteristics, the primary efficacy endpoints, and supportive efficacy endpoints were statistically described using the FAS. Primary and supportive safety endpoints were analyzed using the safety set.
Results
A total of 144 patients (286 eyes) were included in the study and underwent phacoemulsification of cataract followed by successful TFNT00 IOL implantation in the first eye; 142 patients received the TFNT00 IOL in the second eye. Of those, 134 patients (268 eyes) completed 12 months of follow-up after the surgery, exceeding the planned sample size of 127 patients. Two patients withdrew after the 1-month postoperative visit following the first implantation. Because of the COVID-19 pandemic control policy, nine patients missed the 3-month visit, seven patients missed the 6-month visit, and eight patients missed the 12-month visit.
At baseline, mean ± SD age was 64.4±9.2 years, and 62.5% of patients were female (Table 1). Ten patients discontinued the study after the implantation attempt, including two patients who withdrew after completing monocular implantation (results for discontinuation were loss to follow-up [n=5] and withdrawal of patients [n=5]).
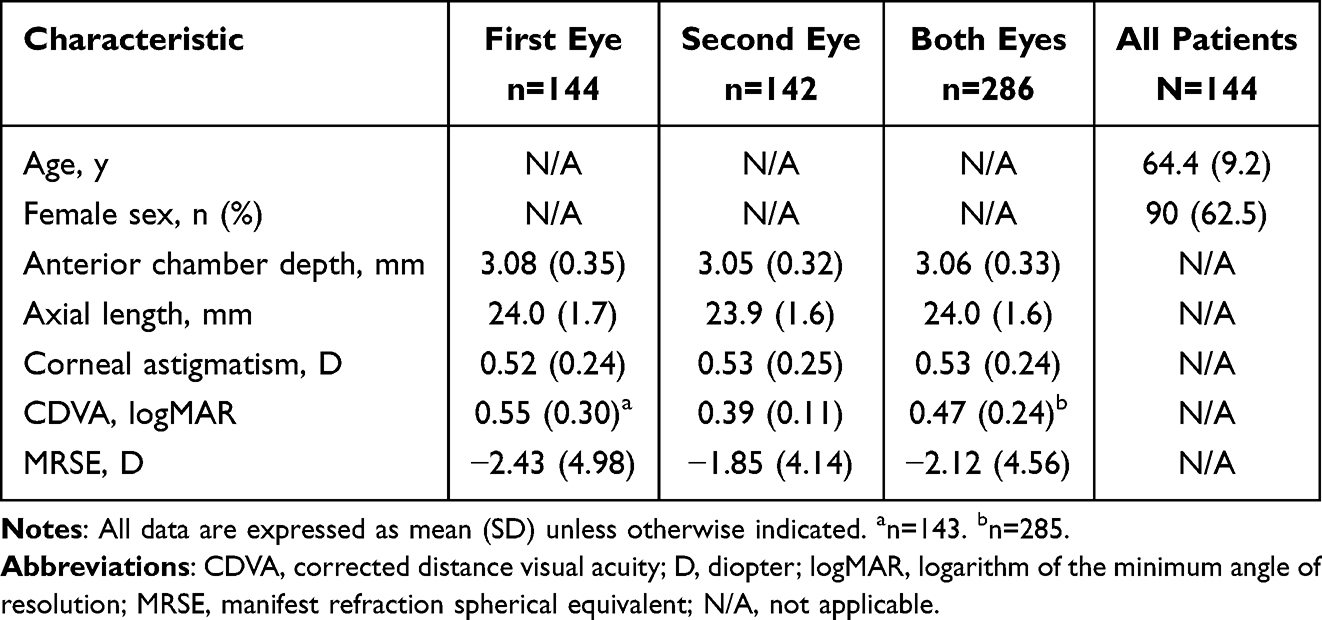 |
Table 1 Baseline Characteristics |
Outcomes After Surgery
At week 1, 99.3% of eyes achieved monocular CDVA of 0.3 logMAR or better (Figure 2A). At 6 and 12 months, 99.3% and 98.5% of patients, respectively, had monocular CDVA of 0.3 logMAR or better. The percentage of eyes with binocular CDVA of 0.3 logMAR or better at 6 and 12 months was 100% for all eyes (vs 50% preoperatively). Monocular CDVA improved from preoperative levels as early as 1 week after surgery and remained stable at 6 and 12 months (−0.02±0.11 and −0.01±0.13 logMAR, respectively; continuous values for each type of VA are all described as mean ± SD; Table 2, Figure 2B). The postoperative binocular CDVA was −0.08±0.10 logMAR (6 months) and −0.06±0.10 logMAR (12 months; Table 2).
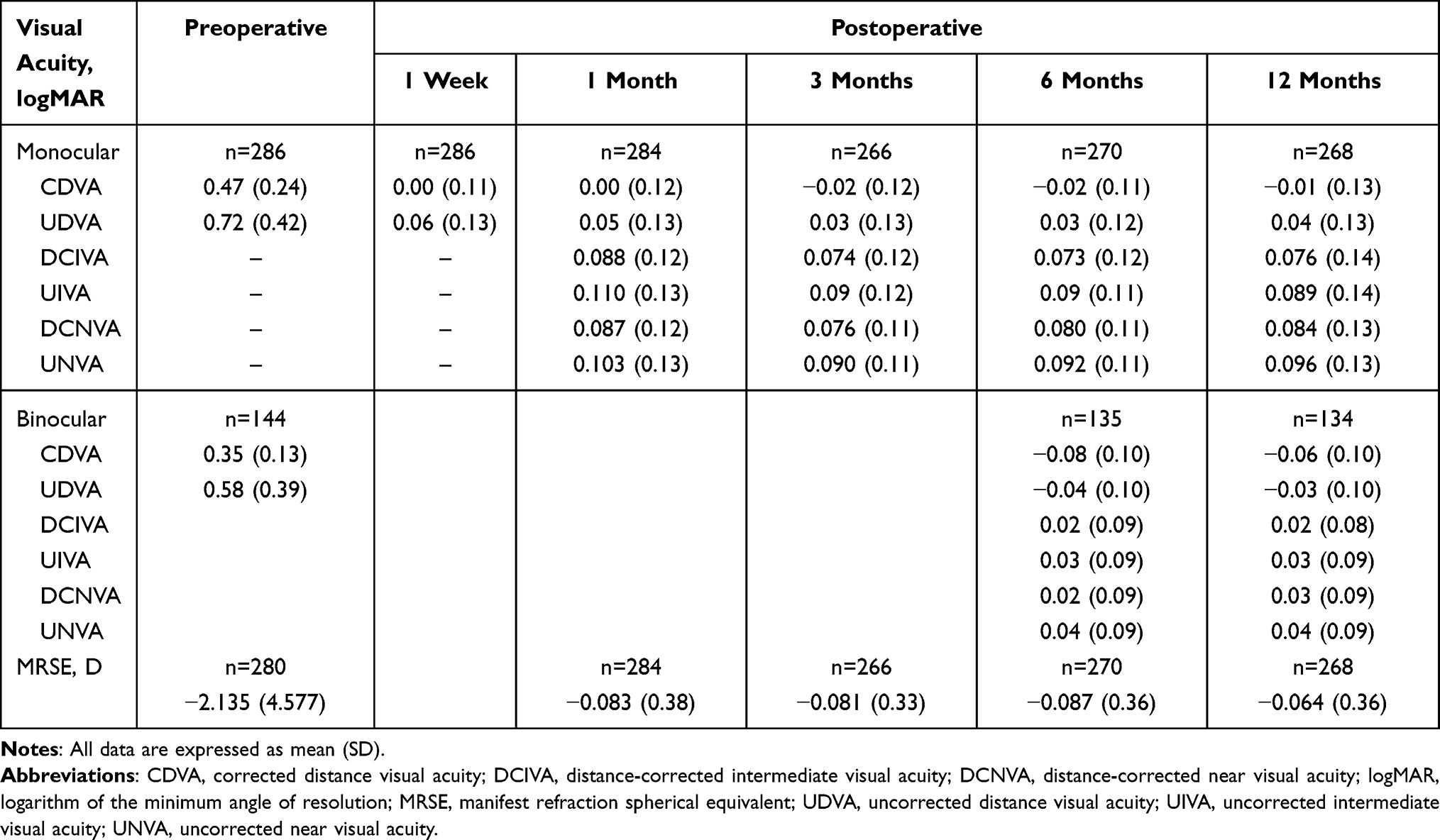 |
Table 2 Monocular and Binocular CDVA, UDVA, DCIVA, UIVA, DCNVA, UNVA; All Eyes |
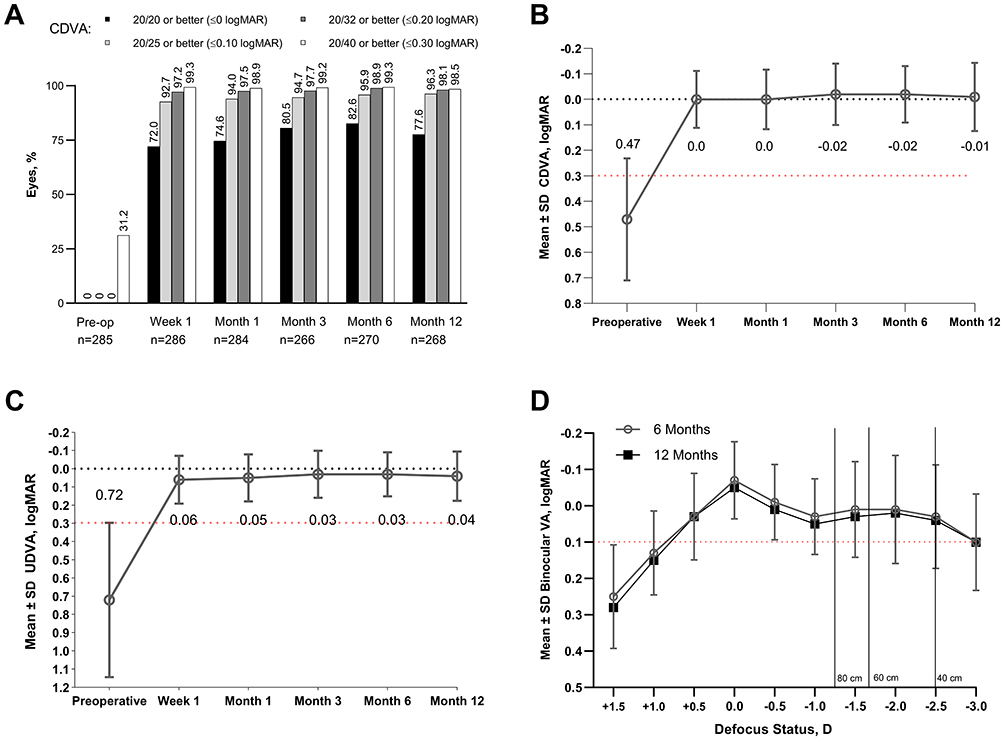 |
Figure 2 Proportion of eyes with preoperative and postoperative monocular CDVA 0.3 logMAR or better (A), monocular CDVA (B), and monocular UDVA (C) as well as binocular defocus curves (logMAR) at 6 and 12 months after surgery (D). Red dotted line is included at 0.3 logMAR (A–C) or at 0.1 logMAR (D) as a reference. Abbreviations: CDVA, corrected distance visual acuity; D, diopter; logMAR, logarithm of the minimum angle of resolution; UDVA, uncorrected distance visual acuity; VA, visual acuity. |
The monocular UDVA also improved from preoperative levels as early as 1 week after surgery; it remained stable at 6 and 12 months (0.03±0.12 and 0.04±0.13 logMAR, respectively; Figure 2C). The postoperative binocular UDVA was −0.04±0.10 logMAR (6 months) and −0.03±0.10 logMAR (12 months; Table 2).
The monocular DCIVA was 0.07±0.12 and 0.08±0.14 at 6 and 12 months, respectively (Supplementary Figure S1A); the monocular UIVA was 0.09±0.12 and 0.09±0.14 logMAR (Supplementary Figure S1B). The binocular DCIVA was 0.02±0.09 and 0.02±0.08 logMAR at 6 and 12 months, respectively, and binocular UIVA was 0.03±0.09 and 0.03±0.09 logMAR (Table 2).
The monocular DCNVA was 0.08±0.11 and 0.08±0.13 logMAR at 6 and 12 months, respectively (Supplementary Figure S1C); the monocular UNVA was 0.09±0.11 and 0.10±0.13 logMAR (Supplementary Figure S1D). The binocular DCNVA was 0.025±0.09 and 0.03±0.09 logMAR at 6 and 12 months, respectively, and binocular UNVA was 0.04±0.09 and 0.04±0.09 logMAR (Table 2).
The monocular MRSE was −2.14±4.58 for all eyes preoperative and −0.08±0.38, −0.08±0.33, −0.09±0.36, and −0.06±0.36 D at the 1-, 3-, 6-, and 12-month visits, respectively.
Analysis of the binocular defocus curves showed mean binocular VA of 0.1 logMAR or better in the defocus range of +0.50 to −3.00 D at 6 and 12 months postoperatively. The peak values of the binocular defocus curves at 6 months were distributed at 0 D (binocular VA of −0.07±0.106 logMAR), −1.5 D (0.01±0.131 logMAR), and −2.0 D (0.01±0.148 logMAR) and remained stable at 12 months (0 D [−0.05±0.135 logMAR], −1.5 D [0.03±0.134 logMAR], and −2.0 D [0.02±0.136 logMAR]), with mean binocular VA better than 0.1 logMAR in the defocus range of +0.50 D to −3.00 D (Figure 2D).
Patient Satisfaction
Compared with the preoperative rates (27%), the proportion of patients who indicated that they “never” needed spectacles for seeing (ie, achieved complete spectacle independence) improved after TFNT00 IOL implantation at 6 months (83%) and 12 months (85%) postoperatively (Figure 3A). Complete spectacle independence at distance, intermediate, and near distances was achieved by 94%, 90%, and 87% of patients, respectively. Results were similar in both dim and bright light conditions. Overall, 88% of patients were “satisfied” or “very satisfied” with postoperative vision at 12 months (Figure 3B), with 92% of patients expressing willingness to recommend TFNT00 IOL to friends and family. For patients who reported being “dissatisfied” on the IOLSAT questionnaire, those who experienced AEs that may have caused dissatisfaction (eg, dry eye and macular hole leading to decreased visual acuity) were treated to address the AE. For cases in which patients reported dissatisfaction but no ocular abnormalities were observed postoperatively, patients received no special treatment.
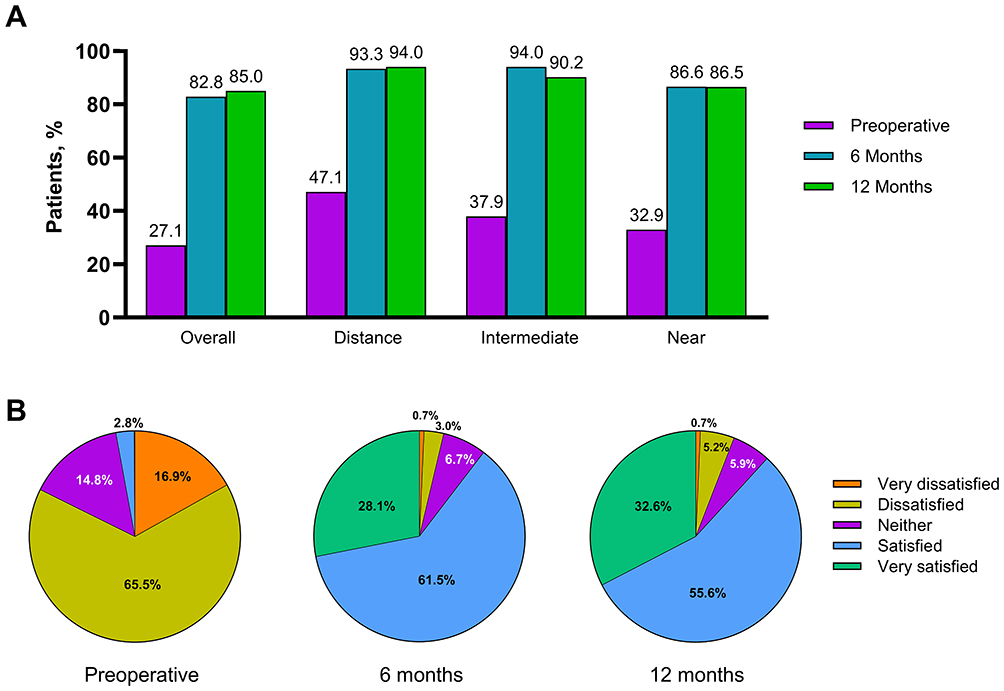 |
Figure 3 Patient-reported spectacle Independence in the past 7 days (A) and patient-reported satisfaction preoperative and 6 months and 12 months postoperative (B). Data were reported from the Intraocular Lens Satisfaction Questionnaire. |
One patient was “very dissatisfied” at 6 months and “dissatisfied” at 12 months postoperatively due to complaints of “no effect after the operation.” This patient had monocular UDVA of 0.0 logMAR and binocular UDVA of −0.1 logMAR at months 6 and 12 postoperatively, and all UIVA and UNVA were better than 0.3 logMAR. The investigator judged that there were no postoperative ocular abnormalities, and no special treatment was provided. Another patient was “neither satisfied nor dissatisfied” at 6 months and “very dissatisfied” at 12 months postoperatively because of complaints of “blurred vision and my eyes hurt if I use them for a long time.” Four patients reported being “dissatisfied” with their vision 6 months postoperatively, and seven were “dissatisfied” 12 months postoperatively. Of the two patients who responded “very dissatisfied” on the IOLSAT questionnaire, one reported good CDVA and functional intermediate VA but reported dry eye (Sjogren syndrome) in both eyes, which may have caused dissatisfaction. Another patient had decreased VA in the right eye at the 12-month visit; optical coherence tomography reported a macular hole of the right eye, which may have caused the decreased VA and dissatisfaction. It was determined that neither of these AEs were related to the TFNT00 IOL, and the patients continued to be treated for the AEs after completion of the study.
Adverse Events
No device-related AEs, secondary surgery intervention, or IOL position change occurred within 12 months after surgery. Seventy eyes (24.5%) experienced 85 ocular AEs (Table 3), and 28 patients (19%) experienced 49 non-ocular AEs (Supplementary Table S1). Dry eye was the most common ocular AE (26 cases in 26 eyes; 9.1%); 17 cases were related to the surgery and none were related to the investigational product. Five eyes (1.7%) experienced an ocular SAE, all of which were cystoid macular edemas (Table 3). The rate of postoperative CEC loss was 9.5% at 12 months.
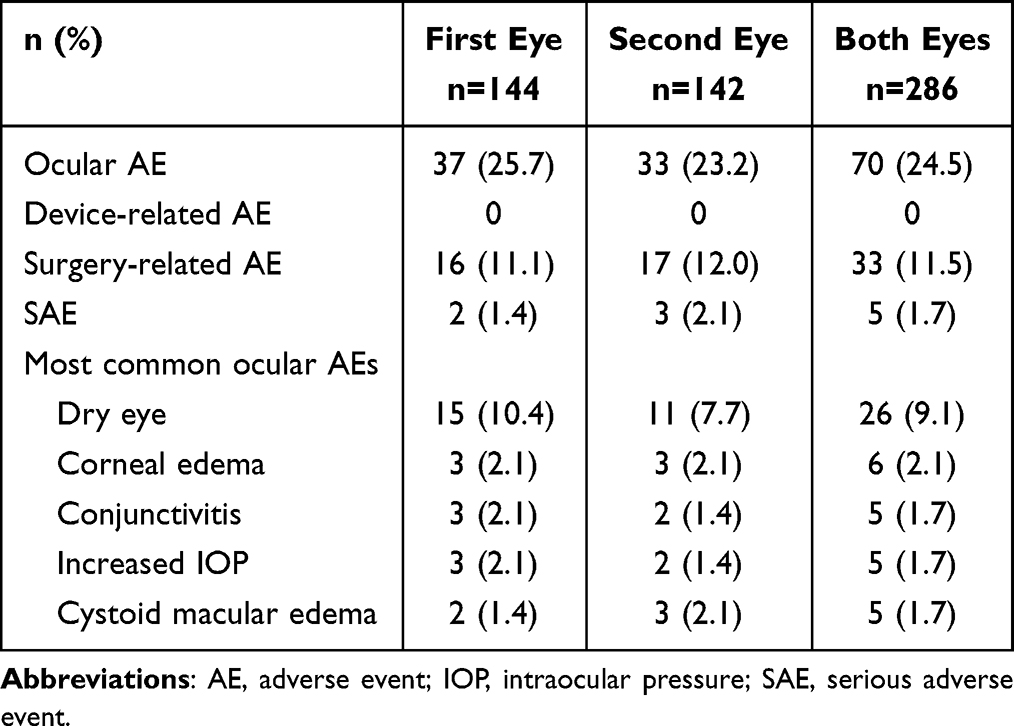 |
Table 3 Ocular AEs and SAEs |
Posterior capsular opacity (PCO) was observed by slit-lamp in 40 cases (14%), 37 of which were clinically nonsignificant; three eyes (1.1%) developed subjective clinically significant PCO. One patient (left eye; 0.4%) required clinical treatment and underwent laser posterior capsulotomy. One patient (0.4%) presented with clinically significant PCO in the left eye at the 12-month visit and underwent neodymium-doped yttrium aluminum garnet (Nd:YAG) laser posterior capsulotomy on the same day.
Compared with the preoperative assessment, the postoperative incidence of severe halos, glare, hazy vision, blurred vision, or double vision decreased at 6 and 12 months (Supplementary Table S2). There was an increase in the proportion of patients reporting starbursts at 12 months (9.9–16%). At month 12, the incidence of severe starbursts, halos, and glare was 15.6%, 4.4%, and 2.3%, respectively; however, the proportion of patients reporting to be bothered by these visual disturbances was 1.5% for each.
Discussion
TFNT00 was safe, effective, and performed as intended when implanted in the posterior chamber in aphakic eyes in a Chinese population.
Our findings were similar to those reported previously for this trifocal IOL in other populations.9,10 In a Korean study, TFNT00 binocular defocus curve showed VA of 0.3 logMAR or better over a +1.0 and −3.50 D defocus range, reaching 0.06, 0.03, and 0.06 logMAR at 80, 60, and 40 cm, respectively, at 3 months.11 In a global pooled analysis, TFNT00 showed a mean VA of 0.1 logMAR or better from far (4–5 m) to near (33 cm), and 99.3% of patients achieved binocular photopic CDVA of 0.14 logMAR or better at 3 to 6 months postoperatively.12 An Australian real-world retrospective evaluation of 254 patients (466 eyes) 3 months after implantation showed that 61% of eyes achieved a UDVA of 20/20 or better, and 94% achieved a UDVA of 20/32 or better.13 The current study showed good long-term VA performance at 12 months after TFNT00 implantation.
In other studies, TFNT00 performed similarly or better than other multifocal IOLs at near and intermediate distances,14–20 which may be important for users of cell phones and other handheld devices. The intermediate focal point at 60 cm is a more natural and comfortable distance for performing routine daily activities versus the focal point at 80 cm for other trifocal and extended depth-of-focus IOLs, such as FineVision Micro F (PhysIOL, Liège, Belgium), AT LISA tri 839MP (Carl Zeiss Meditec AG, Jena, Germany), and TECNIS Symfony (Abbott Medical Optics, Santa Ana, CA, USA).17 In a previous study that compared TFNT00 and AT LISA tri389MP, TFNT00 recipients showed significantly better postoperative UIVA at 60 cm than AT LISA tri389MP recipients at 3 months (0.04±0.12 vs 0.15±0.11 logMAR; P=0.001).21 Another study reported that TFNT00 IOLs provided significantly better near VA compared with Tecnis Symfony ZXR00 IOL (P=0.01),14 and significantly better UIVA and UNVA compared with Trinova IOL (VSY Biotechnology, Amsterdam, Netherlands; P<0.001 for both).20
In the current study, spectacle independence overall or in the far, intermediate, and near distance ranges improved at 6 and 12 months postoperatively (83–94%) compared with preoperatively (27–47%). Similar results were obtained under dim or bright illumination (Supplementary Table S3). Furthermore, 88% of patients were satisfied or very satisfied with their postoperative VA, and 92% of patients expressed willingness to recommend TFNT00 to relatives and friends. These results are in line with previous TFNT00 IOL studies that have reported 93% to 96% spectacle independence and 81% to 100% satisfaction and willingness to recommend TFNT00 to others.10,16,17
Occurrence of AEs was low, and none were considered related to the investigational product. At 12 months, dry eye was the most common ocular AE (9.1%), consistent with a previous TFNT00 IOL study in which dry eye was reported in 8% of eyes 3 months postoperatively.22 Occurrence of dry eye is common after cataract surgery, reported in up to 37% of patients, and is a common cause of patient dissatisfaction after IOL implantation.4,23 Overall, the rate of postoperative cystoid macular edema was 1.7% (5/286 eyes), which is somewhat higher than the incidence reported from the American Academy of Ophthalmology IRIS® (Intelligent Research in Sight) Registry in patients after cataract surgery (0.8%).24 However, the differences in reported incidence of cystoid macular edema may be primarily attributed to differences in examination and diagnostic methods. Based on the ISO 11979-7 and the studies of posterior chamber IOLs approved in the United States (December 1989 to December 1997), the incidence of cystoid macular edema was 3%.25 Furthermore, a meta-analysis reported that the incidence rates of cystoid macular edema 4 to 6 weeks after cataract surgery varied substantially, depending on surgical technique and method of diagnosis, ranging from 0.1% to 20%.26 Therefore, the incidence of macular edema reported in this study is within a reasonable range. The average rate of CEC loss in this study was 9.5%, which is within the lower range of CEC loss rates reported in the literature for phacoemulsification combined with IOL implantation (4–25%).27 The month 12 incidences of severe starbursts (15.6%), halos (4.4%), and glare (2.3%) in this study were generally consistent with previous TFNT00 studies.17,22
Clinically significant PCO was reported in three eyes (3.3%), with one patient (0.4%) requiring Nd:YAG laser posterior capsulotomy. A similar occurrence of PCO that needed Nd:YAG laser posterior capsulotomy was reported previously for TFNT00 at 6 months (n=1 [0.5%]),17 which is lower than reported for other bifocal (eg, n=4 [11%] for AT LISA 801) and trifocal (eg, n=3 [8%] for AT LISA tri 839MP) IOLs at 12 months postoperatively.28 The lower incidence of PCO reported in this study may be the result of the TFNT00 IOL design and improvements in surgical technology.
A strength of this study was the multicenter setting in a Chinese population: this was the largest TFNT00 IOL clinical trial in a Chinese population to date. The 12-month follow-up in the study was longer than some previous TFNT00 studies, which had a ≤6-month follow-up.11,12 A limitation was the single-arm study design without a comparator group. The COVID-19 pandemic affected the study visit schedule for some patients; however, enough patients were included to meet the statistical requirements, thus this was not deemed to affect the statistical analysis. Additional studies are needed to assess the long-term effectiveness and safety of the TFNT00 IOL in the Chinese population and to include direct comparisons with other multifocal IOLs available in China. Future studies will need to address the complex effects of the patient’s biometric characteristics (eg, mesopic pupil size and angle alpha) and the surgeon’s level of experience on visual outcomes, patient satisfaction, and AEs after cataract surgery.
Conclusion
These findings demonstrated that AcrySof IQ PanOptix IOL (model TFNT00) provided good VA at far, intermediate, and near distances; improved visual quality safely and effectively; and had good postoperative rates of spectacle independence and satisfaction in a Chinese population.
Abbreviations
AE, Adverse event; CDVA, Corrected distance visual acuity; CEC, Corneal endothelial cell; D, Diopter; DCIVA, Distance-corrected intermediate visual acuity; DCNVA, Distance-corrected near visual acuity; FAS, Full analysis set; IOL, Intraocular lens; IOLSAT, Intraocular Lens Satisfaction [questionnaire]; logMAR, Logarithm of the minimum angle of resolution; MRSE, Manifest refraction spherical equivalent; Nd:YAG, Neodymium-doped yttrium aluminum garnet; PCO, Posterior capsular opacity; QUVID, Questionnaire for Visual Disturbances; SAE, Serious adverse event; UDVA, Uncorrected distance visual acuity; UIVA, Uncorrected intermediate visual acuity; UNVA, Uncorrected near visual acuity; VA, Visual acuity.
Data Sharing Statement
The data used to support the findings of this study are available upon reasonable request from the study sponsor, Alcon Research LLC.
Acknowledgments
Medical writing assistance was provided by Maria Hovenden, PhD, and Natalia Zhukovskaya, PhD, of ICON plc (Blue Bell, PA, USA), and was funded by Alcon. These data were presented, in part, at the 27th Congress of the Chinese Ophthalmological Society; September 25, 2023; Changsha, China.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study was funded by Alcon Research LLC, Fort Worth, TX, USA.
Disclosure
Yilin Pang is an employee of Alcon Research LLC. The other authors report no other conflicts of interest in this work.
References
1. Fang R, Yu YF, Li EJ, et al. Global, regional, national burden and gender disparity of cataract: findings from the Global Burden of Disease study 2019. BMC Public Health. 2022;22(1):2068. doi:10.1186/s12889-022-14491-0
2. Cao K, Friedman DS, Jin S, et al. Multifocal versus monofocal intraocular lenses for age-related cataract patients: a system review and meta-analysis based on randomized controlled trials. Surv Ophthalmol. 2019;64(5):647–658. doi:10.1016/j.survophthal.2019.02.012
3. MacRae S, Holladay JT, Glasser A, et al. Special report: American Academy of Ophthalmology Task Force consensus statement for extended depth of focus intraocular lenses. Ophthalmology. 2017;124(1):139–141. doi:10.1016/j.ophtha.2016.09.039
4. Salerno LC, Tiveron MC, Alio JL. Multifocal intraocular lenses: types, outcomes, complications and how to solve them. Taiwan J Ophthalmol. 2017;7(4):179–184. doi:10.4103/tjo.tjo_19_17
5. Sachdev GS, Sachdev M. Optimizing outcomes with multifocal intraocular lenses. Indian J Ophthalmol. 2017;65(12):1294–1300. doi:10.4103/ijo.IJO_1072_17
6. Kohnen T, Herzog M, Hemkeppler E, et al. Visual performance of a quadrifocal (trifocal) intraocular lens following removal of the crystalline lens. Am J Ophthalmol. 2017;184:52–62. doi:10.1016/j.ajo.2017.09.016
7. Modi S, Lehmann R, Maxwell A, et al. Visual and patient-reported outcomes of a diffractive trifocal intraocular lens compared with those of a monofocal intraocular lens. Ophthalmology. 2021;128(2):197–207. doi:10.1016/j.ophtha.2020.07.015
8. Lasch K, Marcus JC, Seo C, et al. Development and validation of a visual symptom-specific patient-reported outcomes instrument for adults with cataract intraocular lens implants. Am J Ophthalmol. 2022;237:91–103. doi:10.1016/j.ajo.2021.10.023
9. Garcia-Perez JL, Gros-Otero J, Sanchez-Ramos C, Blazquez V, Contreras I. Short term visual outcomes of a new trifocal intraocular lens. BMC Ophthalmol. 2017;17(1):72. doi:10.1186/s12886-017-0462-y
10. Galvis V, Escaf LC, Escaf LJ, et al. Visual and satisfaction results with implantation of the trifocal PanOptix® intraocular lens in cataract surgery. J Optom. 2022;15(3):219–227. doi:10.1016/j.optom.2021.05.002
11. Kim TI, Chung TY, Kim MJ, Lee K, Hyon JY. Visual outcomes and safety after bilateral implantation of a trifocal presbyopia correcting intraocular lens in a Korean population: a prospective single-arm study. BMC Ophthalmol. 2020;20(1):288. doi:10.1186/s12886-020-01549-z
12. Kohnen T, Lapid-Gortzak R, Ramamurthy D, et al. Clinical outcomes after bilateral implantation of a diffractive trifocal intraocular lens: a worldwide pooled analysis of prospective clinical investigations. Clin Ophthalmol. 2023;17:155–163. doi:10.2147/OPTH.S377234
13. Ackerman M, Lawless M, Levitz L, et al. Visual and refractive efficacy of PanOptix toric intraocular lens in a clinical setting. Clin Ophthalmol. 2022;16:4227–4237. doi:10.2147/OPTH.S390980
14. Farvardin M, Johari M, Attarzade A, et al. Comparison between bilateral implantation of a trifocal intraocular lens (Alcon Acrysof IQ® PanOptix) and extended depth of focus lens (Tecnis® Symfony® ZXR00 lens). Int Ophthalmol. 2021;41(2):567–573. doi:10.1007/s10792-020-01608-w
15. Boris M, Olga F, Nikolay S, et al. Visual results and subjective satisfaction after implantation of two different trifocal diffractive intraocular lenses models (AcrySof IQ PanOptix and AT LISA tri 839 MP). Eur J Ophthalmol. 2024;34(3):726–733. doi:10.1177/11206721231201561
16. Al Fayyadh M, Al Subaie M, El Salamony M, Al Rajhi A, Al Jindan M. Visual performance, spectacle independence, visual disturbances and patient satisfaction after cataract surgery: comparison of 2 diffractive intraocular lenses in a tertiary hospital. Open Ophthalmol J. 2022;16:e187436412209140.
17. Sudhir RR, Dey A, Bhattacharrya S, Bahulayan A. AcrySof IQ PanOptix intraocular lens versus extended depth of focus intraocular lens and trifocal intraocular lens: a clinical overview. Asia Pac J Ophthalmol. 2019;8(4):335–349. doi:10.1097/APO.0000000000000253
18. Gundersen KG, Potvin R. Trifocal intraocular lenses: a comparison of the visual performance and quality of vision provided by two different lens designs. Clin Ophthalmol. 2017;11:1081–1087. doi:10.2147/OPTH.S136164
19. Moshirfar M, Stoakes IM, Theis JS, et al. Assessing visual outcomes: a comparative study of US-FDA premarket approval data for multifocal and EDOF lens implants in cataract surgery. J Clin Med. 2023;12(13):4365. doi:10.3390/jcm12134365
20. Kılıç A, Özpınar A, Tanrıverdi C. Comparison of visual outcomes of two trifocal IOLs. J Refract Surg. 2023;39(8):524–530. doi:10.3928/1081597X-20230424-01
21. Ju RH, Qu HK, Wu ZM, et al. Comparison of visual performance with iTrace analyzer following femtosecond laser-assisted cataract surgery with bilateral implantation of two different trifocal intraocular lenses. Int J Ophthalmol. 2023;16(11):1773–1781. doi:10.18240/ijo.2023.11.06
22. Moshirfar M, Ellis J, Beesley D, et al. Comparison of the visual outcomes of an extended depth-of-focus lens and a trifocal lens. Clin Ophthalmol. 2021;15:3051–3063. doi:10.2147/OPTH.S321779
23. Miura M, Inomata T, Nakamura M, et al. Prevalence and characteristics of dry eye disease after cataract surgery: a systematic review and meta-analysis. Ophthalmol Ther. 2022;11(4):1309–1332. doi:10.1007/s40123-022-00513-y
24. Iftikhar M, Dun C, Schein OD, Lum F, Woreta F. Cystoid macular edema after cataract surgery in the United States: IRIS® Registry (Intelligent Research in Sight) analysis. Ophthalmology. 2023;130(10):1005–1014. doi:10.1016/j.ophtha.2023.06.001
25. International Organization for Standardization. Ophthalmic implants - intraocular lenses - part 7: clinical investigations of intraocular lenses for the correction of aphakia (ISO 11979-7:2018); 2018.
26. Ferro Desideri L, Arun K, Bernardi E, Sagurski N, Anguita R. Incidence, pathogenesis, risk factors, and treatment of cystoid macula oedema following cataract surgery: a systematic review. Diagnostics. 2025;15(6):667. doi:10.3390/diagnostics15060667
27. Walkow T, Anders N, Klebe S. Endothelial cell loss after phacoemulsification: relation to preoperative and intraoperative parameters. J Cataract Refract Surg. 2000;26(5):727–732. doi:10.1016/S0886-3350(99)00462-9
28. Mojzis P, Kukuckova L, Majerova K, Ziak P, Pinero DP. Postoperative visual performance with a bifocal and trifocal diffractive intraocular lens during a 1-year follow-up. Int J Ophthalmol. 2017;10(10):1528–1533. doi:10.18240/ijo.2017.10.08
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.