Back to Journals » Clinical Interventions in Aging » Volume 14
12-Month Teriparatide Treatment Reduces New Vertebral Compression Fractures Incidence And Back Pain And Improves Quality Of Life After Percutaneous Kyphoplasty In Osteoporotic Women
Authors Kong M ![]() , Zhou C, Zhu K
, Zhou C, Zhu K ![]() , Zhang Y, Song M, Zhang H
, Zhang Y, Song M, Zhang H ![]() , Tu Q, Ma X
, Tu Q, Ma X
Received 25 July 2019
Accepted for publication 15 September 2019
Published 1 October 2019 Volume 2019:14 Pages 1693—1703
DOI https://doi.org/10.2147/CIA.S224663
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Meng Kong, 1, 2 Chuanli Zhou, 1 Kai Zhu, 1 Yiran Zhang, 1 Mengxiong Song, 1 Hao Zhang, 1 Qihao Tu, 1 Xuexiao Ma 1, 2
1Department of Spinal Surgery, Affiliated Hospital of Qingdao University, Qing’dao, Shandong Province 266000, China; 2Department of Medicine, Qingdao University, Qing’dao, Shandong Province 266000, China
Correspondence: Xuexiao Ma
Department of Spinal Surgery, Affiliated Hospital of Qingdao University, No. 59, Hai Er Road, Qing’dao, Shandong Province 266000, People’s Republic of China
Tel +86 532 18661807895
Email [email protected]
Purpose: Define the effectiveness of teriparatide (TPTD) treatment on reducing the incidence of new vertebral compression fractures (NVCFs) and back pain and improving quality of life after percutaneous kyphoplasty (PKP).
Methods: Two years of clinical follow-up data from primary osteoporotic women who had experienced initial osteoporotic vertebral compression fractures (OVCFs) and received PKP plus 12-month TPTD (n=113) or basic treatment (BT) of calcium and vitamin D supplements (n=208) were retrospectively collected. The risk of NVCFs over each 6-month period in the TPTD group was evaluated and compared with the BT group using a logistic regression. Health-related quality of life (HRQoL, EQ-5D questionnaire), back pain [100 mm visual analog scale (VAS)] and bone mineral density (BMD) of the spine were analyzed using linear mixed models for repeated measures (LMMRM).
Results: Logistic regression analysis adjusting for baseline characteristics showed that patients in the TPTD group had a lower risk of NVCFs compared with those receiving BT during the final three observation intervals (6– 12 months, OR=0.189, 95% CI=0.030– 0.681, p=0.046; 12– 18 months, OR=0.009, 95% CI=0.0001– 0.111, p=0.001; 18– 24 months, OR=0.024, 95% CI=0.0009– 0.264, p=0.009, respectively). Significant improvements in adjusted EQ-5D and back pain VAS scores were identified in the TPTD group compared with the BT group, and this improvement was sustained for at least 12 months after teriparatide treatment was discontinued (both p< 0.001). The BMD of the spine also showed a higher T-value in the TPTD group compared with the BT group (p< 0.001).
Conclusion: In routine clinical practice, for patients with OVCFs who receive the PKP procedure, TPTD treatment may be a preferable subsequent therapy because of its ability to reduce the incidence of NVCFs and sustain a high quality of life and back pain alleviation.
Keywords: teriparatide, osteoporosis vertebral fractures, quality of life, back pain, PKP
A Letter to the Editor has been published for this article.
A response to a letter has been published for this article.
Introduction
Osteoporosis is a disease characterized by microarchitectural deterioration of bone tissue and low bone mass,1 which increases the risk of fractures. Osteoporotic vertebral compression fracture (OVCF) is a major cause of morbidity and high health care costs among elderly patients.2 This kind of fracture induces the loss of independence and a poor quality of life in patients.3 The objective of treatment is to enable the patient to function normally again and improve quality of life.
Percutaneous kyphoplasty (PKP) is a minimally invasive technique where polymethylmethacrylate (PMMA) is injected through a needle into the compressed vertebra to stabilize the fracture, and this procedure has been shown to facilitate substantial pain relief, improve the mobility of patients, and restore bone height since its initial application in the treatment of OVCFs in the mid-1990s.4,5 Several complications related to PKP have been reported, ranging from recollapse of already stabilized vertebrae to adjacent segment fractures (ASFs) of vertebrae, persistent mild to moderate residual pain, postoperation instability, and several types of injuries caused by cement leakage.6–9 Studies have found that the incidence of new symptomatic compression fractures 1 year after percutaneous vertebroplasty (PVP) is as high as 21.7%.10 Systematic reviews have noted that 10–51% of patients may continue to suffer from residual pain after successful vertebral augmentation procedures.11,12 Some investigators believe that the occurrence of new vertebral compression fractures (NVCFs), especially ASFs, should be regarded as the consequence of improvements in stiffness achieved by augmentation with bone cement, whereas others believe that these fractures are simply the result of the natural progression of osteoporosis.13 Thus, the reoccurrence of fractures is an important issue that requires urgent attention by orthopedic surgeons. While antiresorptive treatment such as bisphosphonates as an pharmacologic option for subsequent treatment of osteoporosis fracture has been approved by FDA14 because of its effectiveness in reducing the risk of vertebral fracture when given with calcium and vitamin D supplements, several objective factors, for example, aging associated decline in renal function and gastrointestinal adverse events, may potentially limit its efficacy and safety.15,16
Teriparatide, TPTD [recombinant human PTH-(1–34)], a subcutaneously administered anabolic bone formation agent, has been approved for increasing bone mass in the treatment of osteoporosis in postmenopausal women and in men with hypogonadal or idiopathic osteoporosis.17 Several international, multicenter trials have confirmed the effect of TPTD on improving health-related quality of life (HRQoL) and reducing fracture risk in postmenopausal women with severe osteoporosis18,19 with well toleration and adverse events that tend to be slight.16 However, in terms of the subsequent treatment in post-PKP period of OVCFs, which seems to have altered biomechanical characteristics,20,21 published data regarding the positive role of teriparatide in avoiding refracture are limited, particularly in a real-life clinical practice setting.
In this paper, we retrospectively evaluated the prospective follow-up of a sequential cohort of OVCF patients undergoing a PKP protocol with concurrent TPTD or basic treatment (BT), with the goal of examining the effectiveness of teriparatide injection on lowering the incidence of new vertebral compression fractures and improving quality of life during postoperative convalescence of the augmented PMMA procedure. This paper also explored the minimum usage course of this medicine and the maintained efficacy after discontinuation of treatment.
Methods
Patient Selection
A retrospective study was performed on patients treated with PKP in our department. All radiologic data and relevant clinical objective outcome scores were collected from the regular registry. The computerized database was searched to identify standard candidates who matched the inclusion criteria: 1) female patients at least 5 years postmenopause with primary osteoporosis or who suffered from glucocorticoid-induced osteoporosis; 2) experienced vertebral compression fractures and PKP for more than one time; 3) low bone mineral density (BMD) with T-value≤–2.5; and 4) patients with a persistent, subsequent treatment strategy, including teriparatide treatment or simple basic treatment of calcium and vitamin D supplementation.
The exclusion criteria were as follows: 1) patients who underwent PKP due to pathologic vertebral fractures secondary to metastatic disease, breast cancer, lung cancer, or multiple myeloma; 2) patients with complications such as osteogenesis imperfecta, hypercalcemia, Paget disease, human immunodeficiency virus (HIV), or parathyroid diseases; 3) patients with preindex period hormonal therapy; and 4) patients who received TPTD treatment before PKP or other antiosteoporosis treatments except calcium and vitamin D supplementation pre-, postoperation, and post-TPTD treatment, including bisphosphonates, estrogen, selective estrogen receptor modulators (SERMs), calcitonin, and RANK-ligand inhibitors.
The criteria for the usage and reimbursement of teriparatide in our country: 1) fits one of the following: a) postmenopausal women who suffered from more than one OVCF or OHF (osteoporotic hip fracture); b) women older than 65 with a history of VCFs (vertebral compression fractures) or BMD≤-2.5; and c) BMD≤-3.5, with no osteoporosis fractures history; and 2) meets all the following: a) fasting blood calcium at the range of 2.2–2.7 mmol/L, serum inorganic phosphorus between 0.97–1.45 mmol/L and 25-Hydroxyvitamin D 30–150 ng/mL; and b) without metabolic bone disease. Local resident female patients were included who were diagnosed with osteoporosis, prescribed 12-month TPTD and covered by health insurance, which required them to have at least 12 months of continuous enrollment with pharmacy benefits preceding an additional 12 months from the discontinuation date. TPTD was administered at a dosage of 20 μg daily by subcutaneous self-injection.
The research date of the study was from September 2010 to December 2018.
Clinical And Radiographic Examinations
According to the treatment strategy after the operation, patients who met the criteria were divided into two groups: 1) TPTD group and 2) BT group. The cost and hesitation about its effectiveness were the main reasons that patients did not receive TPTD after PKP. As TPTD was covered by health insurance of Qingdao from October 1, 2013, patients of the BT group were mainly included in the prior period of the research. The routine examination protocol for operation patients in our department was as follows: BMD, radiography, and MRI of the general spine were measured on admission; plain X-ray films of the general spine were conducted 1 day and 3 months postoperation; the importance of diet and exercise in the prevention of osteoporosis was emphasized; and daily supplements of calcium (1000 mg) and vitamin D (400–1200 IU) were all prescribed as the strategy of basic treatment during the postindex period. BMD was analyzed by the same dual-energy X-ray absorptiometry (PIXImus2; Lunar, GE, USA) in all patients, and the PKP treated vertebrae was excluded when calculating the T-values postoperation.
Data on incident clinical fractures, health-related quality of life (HRQoL by the Chinese version of EQ-5D-5L questionnaire)22,23 and back pain [100 mm visual analog scale (VAS)] during the follow-up period (first day after operation or baseline, 3 months, 6 months, 1 year, 18 months, and 2 years) were collected to document the clinical response.
Fracture Ascertainment
Patients with a sudden recurrent increase in back pain were asked to return to the hospital for medical and MRI examinations to determine whether an NVCF existed. A new fresh compression fracture was diagnosed according to clinical features related to the loss of vertebral height on X-ray and the MRI features; hypointensity on T1-weighted (T1WI) MRI images and hyperintensity on T2-weighted (T2WI) MRI images; and fat saturation (FS) within the vertebral body indicating active edema. Since systematic radiologic follow-up was not available for all eligible patients in the study, asymptomatic vertebral fractures were not detected. The retrospective study declares that the evaluations were done according to the double blind principle.
Analysis
Demographic and clinical baseline variables during the hospitalization period of patients who returned for at least one visit postoperation were assessed, and group differences were examined with Student’s t-test, Mann–Whitney U-test and χ2 test, as applicable. Continuous variables are described as mean value with standard deviation [SD] or median with interquartile ranges [Q1, Q3] and as frequency for categorical outcomes.
The number and proportion of patients with one or more NVCFs occurring in the postoperation period were summarized for every 6-month interval. The risk of new vertebral fracture over each 6-month period in the TPTD group was evaluated and compared with that in the BT group using a logistic regression.24,25 The models for the odds of fracture were adjusted for visit and for the following covariates: age, BMI, BMD at baseline, glucocorticoid usage, site and number of initial vertebral fracture in the past (including the last fracture). The site of fracture was classified as thoracic (between T5 and T10), T-L junction (T11–L2), and lumbar (below L3) regions. The results are presented as odds ratios (OR), 95% confidence intervals (95% CI) and p-values. After examining the interaction effect of TPTD treatment with glucocorticoid usage, secondary subgroup analyses were also conducted on patients with or without glucocorticoid-induced osteoporosis. According to the daily dosage and treatment time of glucocorticoid, patients were assigned to four categories: a) No glucocorticoid use; b) Used previously, but discontinued during the study period; c) Still on low-dose glucocorticoid during the study (i.e., <7.5 mg per day of prednisolone or equivalent, no more than 3 months); and d) Still on higher dose glucocorticoid during the study (i.e., at least 7.5 mg per day of prednisolone or equivalent, more than 3 months). Further logistic regression analysis was conducted considering this covariate.
EQ-5D and back pain VAS scores were analyzed using linear mixed models for repeated measures (LMMRM) adjusting for selected prespecified variables, which included baseline value, age, BMI, BMD, number of vertebral fracture, glucocorticoid usage, and diagnosis of rheumatological disorder or degenerative disc disease.26
The BMD of the spine was also analyzed using LMMRM adjusted for baseline value, age, BMI, and glucocorticoid usage.
All statistical analyses were performed using R programming language, version 3.6.0 (R Foundation), where p-values of <0.05 were considered to be statistically significant.
Results
In total, 321 eligible patients met the selection criteria. According to the type of initial strategy, 113 patients were assigned to the TPTD group and 208 to the BT group. During the follow-up, a total of 23 patients in the BT group switched to anti-osteoporosis treatment after another OVCF and subsequent PKP. These patient were excluded from the study during the next interval period according to the per protocol analysis, and the number of patients with observations at each follow-up period for the total study cohort are summarized in Figure 1.
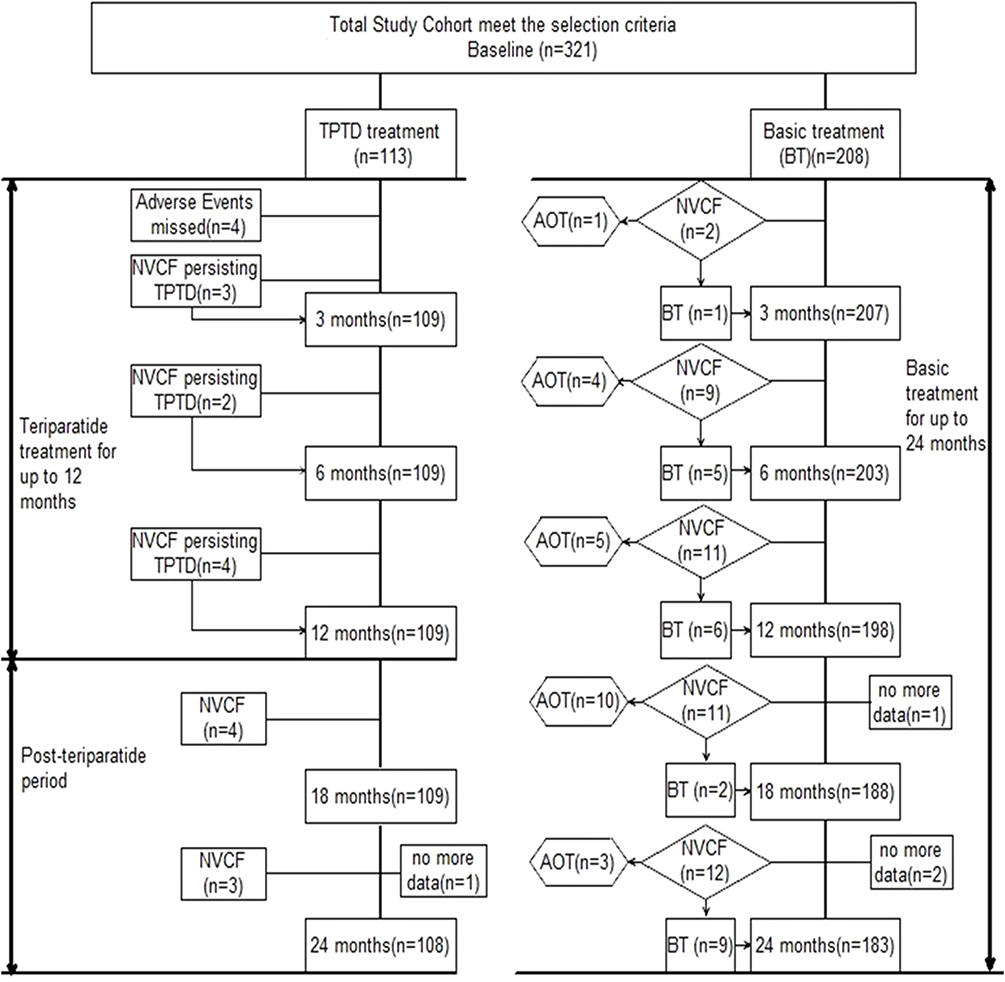 |
Figure 1 Study flow and patient disposition during the study. Abbreviations: TPTD, Teriparatide; AOT, anti-osteoporosis treatment; NVCF, new vertebral compression fracture. |
All but four patients claimed favourable treatment adherence and persistence for daily injection during 12 months. The reasons for patients discontinuing TPTD treatment in this study were palpitation (n=1), nausea (n=2), and headache (n=1). One patient in the TPTD group was lost during the final interval.
The demographic and baseline characteristics of patients in the two groups are shown in Table 1.
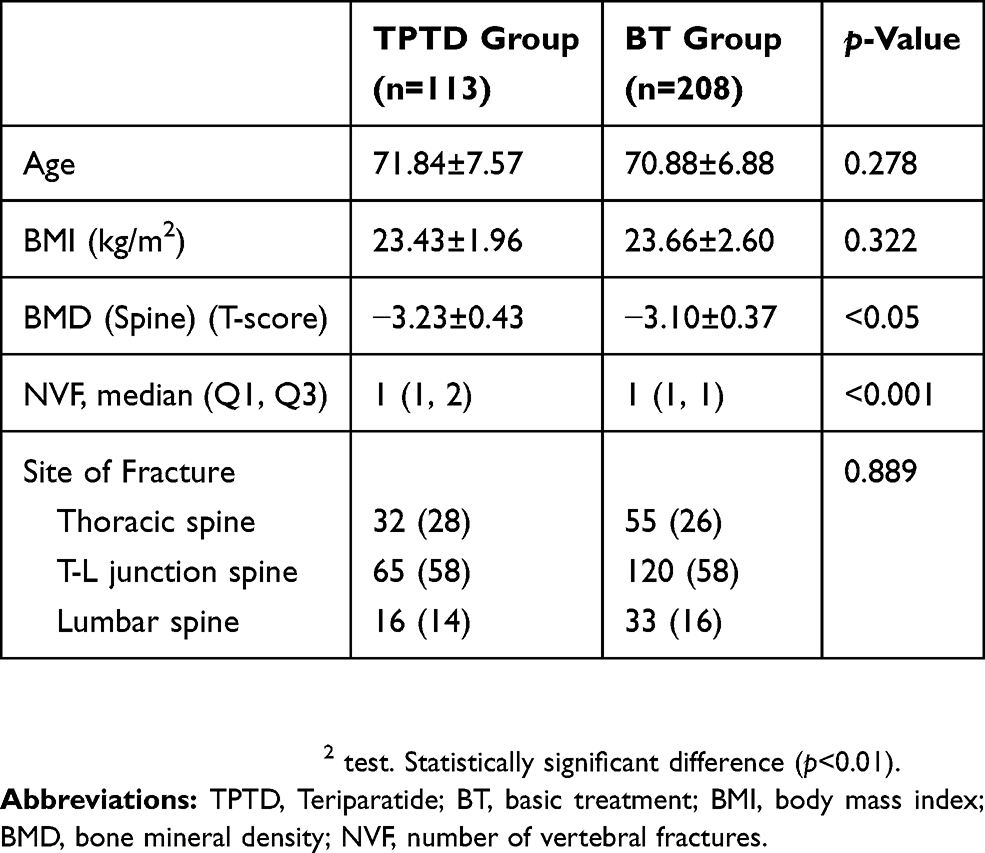 |
Table 1 The Demographic And Baseline Characteristics Of Patients In Two Groups |
Fractures
Figure 2 (Attachment 1) shows the incidence of NVCFs during the 2-year follow-up period. In models fully adjusted for age, BMD at baseline, site, and number of initial vertebral fracture in the past and glucocorticoid usage, TPTD treatment caused significant reduction in risk of NVCFs on the whole (Estimate=−2.59, p<0.001). In total, 16 patients (14.2%) sustained a single NVCF between the start and end of the follow-up period in the TPTD group; these patients all completed TPTD injection for 12 months; 45 NVCFs were identified in 43 patients (21.6%) in the BT group, among which two patients recurred NVCFs twice. All patients diagnosed with NVCFs in the two groups requested and underwent PKP again. The TPTD group demonstrated a significant reduction in the risk of new vertebral compression fractures during the final three observation intervals compared with the BT group (6–12 months, OR=0.189, 95% CI=0.030–0.681, p=0.046; 12–18 months, OR=0.009, 95% CI=0.0001–0.111, p=0.001; 18–24 months, OR=0.024, 95% CI=0.0009–0.264, p=0.009, respectively).
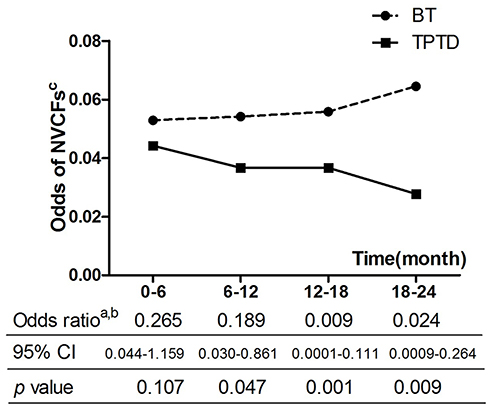 |
Figure 2 Incident NVCFs during four follow-up intervals for the total study cohort. Notes: aAdjusted model by age, BMI, BMD at baseline, glucocorticoid usage, site and number of initial vertebral fracture in the past time. bCompared with BT group. cCalculated by number of patients with NVCFs (not number of NVCFs). Abbreviations: TPTD, Teriparatide; BT, basic treatment; NVCFs, new vertebral compression fractures. |
Since the statistical interaction of the effect between TPTD and glucocorticoid (GLU) usage relative to the odds of fracture was significant by logistic regression analysis (Estimate=−2.72, p<0.05) (Attachment 2), subanalyses were conducted in the two subgroups, with or without glucocorticoid usage, demonstrating greater risk reduction in the GLU group than in the non-GLU group (OR=0.0062, 95% CI=0.0000–0.2092 vs OR=0.1023, 95% CI=0.0263–0.3279) (Table 2). Further analysis conducted according to dosage based classification showed that the risk of NVCFs rose with the increase of glucocorticoid dosage compared with no glucocorticoid usage (estimate was, respectively, b, 2.33, p<0.05; c, 2.75, p<0.0001; d, 4.35, p<0.0001, subgroup a as the reference) (Attachment 3). Because of the minor specimen of glucocorticoid induced subjects (13/113 in TPTD group and 22/208 in BT group), the research was not conducted in the four observation intervals separately. Several covariates had a potential influence on the relative risk of new vertebral compression fractures, including advanced age, lower BMD, glucocorticoid-induced osteoporosis, and initial thoracolumbar junction level fracture.
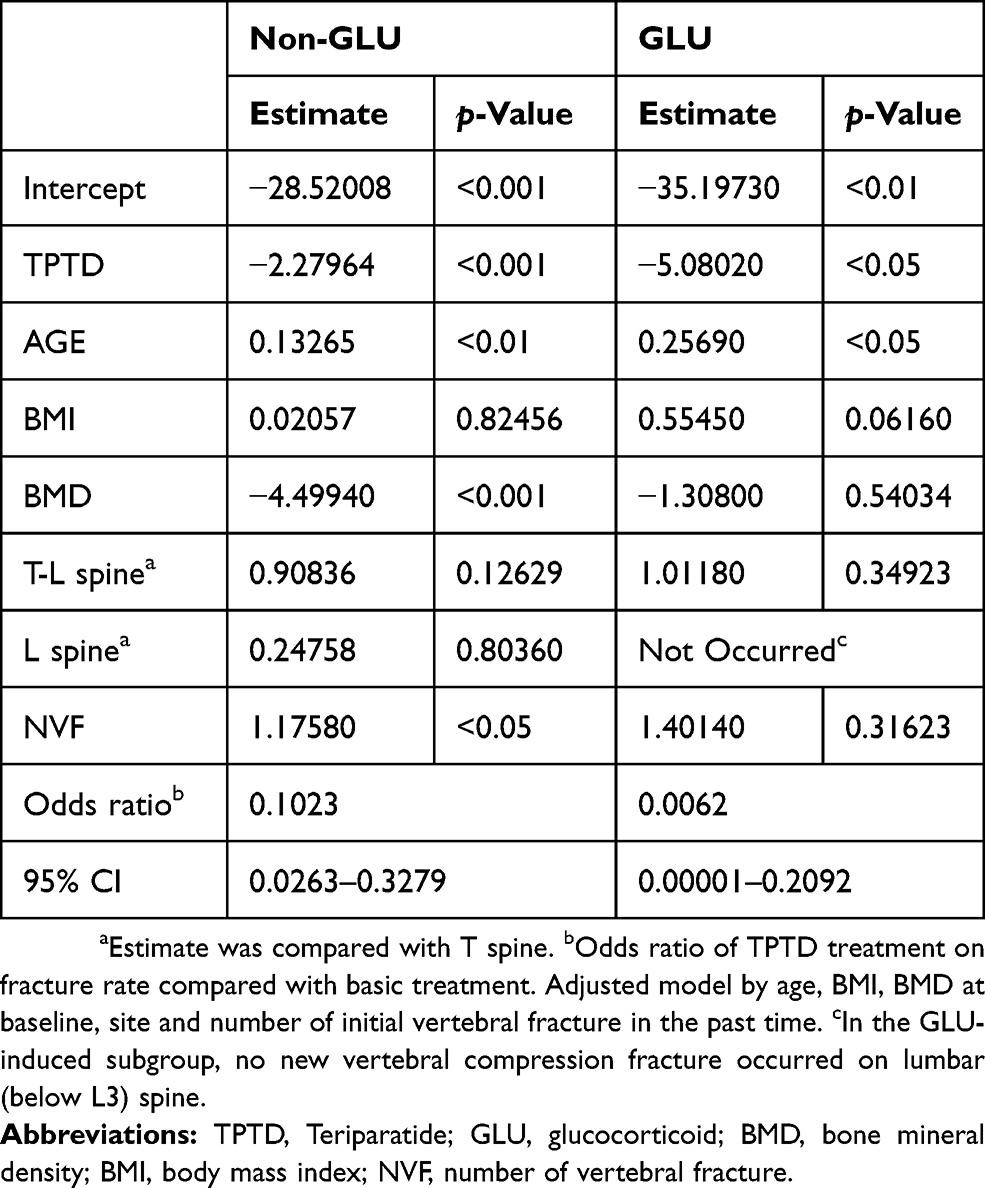 |
Table 2 Logistic Regression Examining Effect Of TPTD Treatment On Odds Of Fractures Of Two Subgroups |
Patient Reported Outcomes
Figure 3 shows the significant improvement in the adjusted EQ-5D and back pain VAS scores during follow-up in the TPTD group compared with the BT group. In models fully adjusted for age, number of past vertebral fractures, BMD at baseline, glucocorticoid usage, and diagnosis of rheumatological disorder or degenerative disc disease, increased EQ-5D and reduced VAS scores were confirmed in patients who received TPTD compared with patients in the other group (at rates of +0.0428 per interval, p<0.001 and −4.0154 per interval, p<0.001, respectively) (Table 3). Further analysis on the breakdown of EQ-5D results showed that TPTD treatment could exert a positive effect on all five dimensions to different extents (Attachment 4).
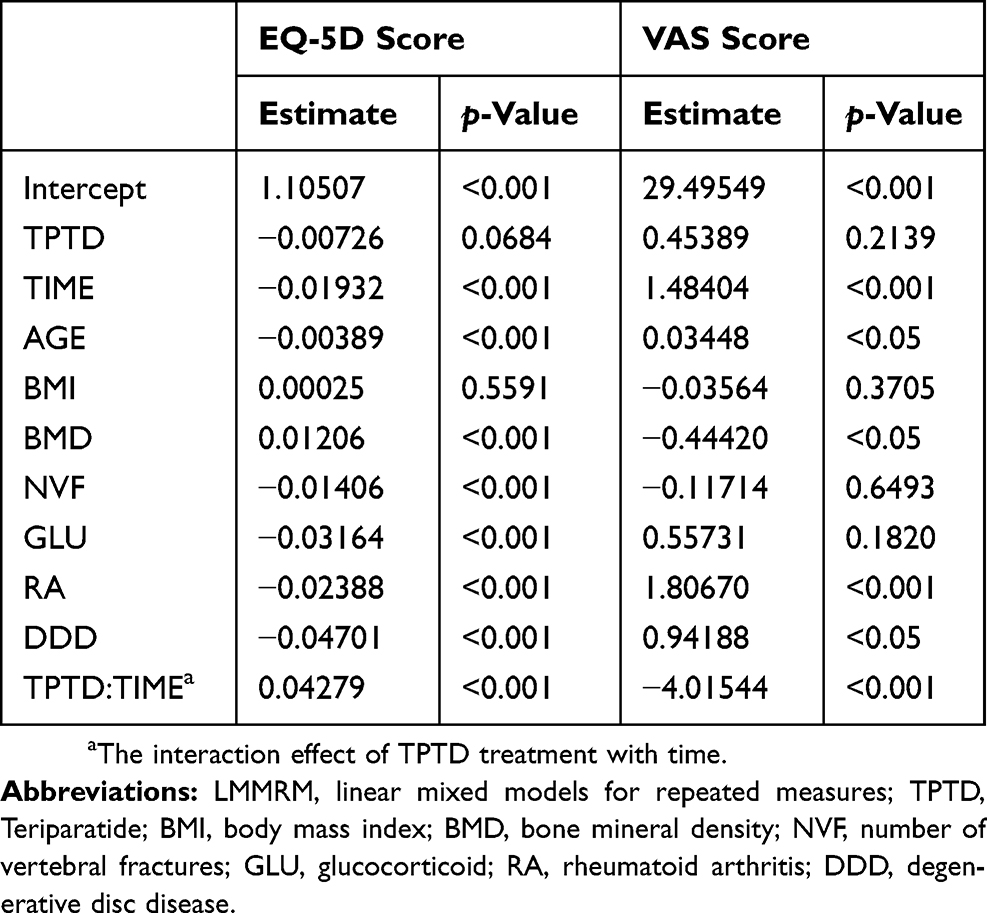 |
Table 3 LMMRM Examining Effect Of TPTD Treatment On Patient Reported Outcomes |
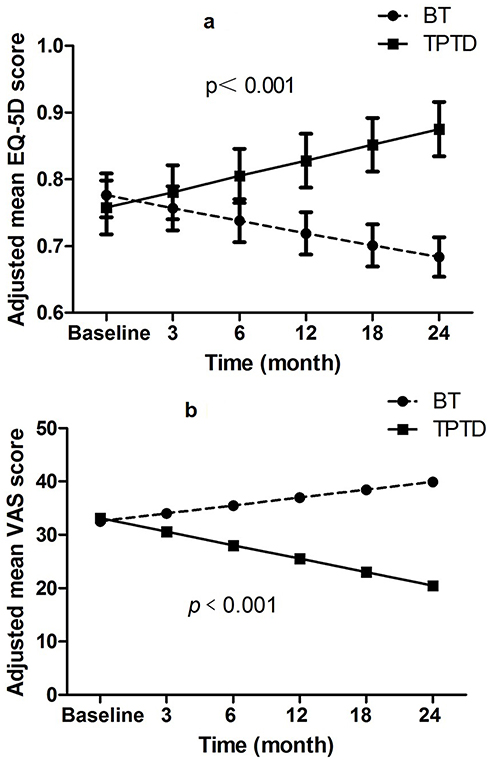 |
Figure 3 Changes in adjusted EQ-5D (A) and VAS (B) scores following TPTD compared with BT. Notes: Data presented is from LMMRM analysis. Model included age, number of vertebral fractures before, BMD at baseline, glucocorticoid usage, and diagnosis of rheumatological disorder or degenerative disc disease before starting teriparatide. Abbreviations: TPTD, Teriparatide; BT, basic treatment; EQ-5D, EuroQol-5 Dimensions; VAS, visual analog scale. |
BMD Of The Spine
Figure 4 confirmed that, when corrected for covariates, patients in the TPTD group had an excellent mean adjusted spine BMD result (−3.23±0.24 to −2.88±0.24) compared with patients in the BT group (−3.42±0.22 to −3.50±0.22), p<0.001.
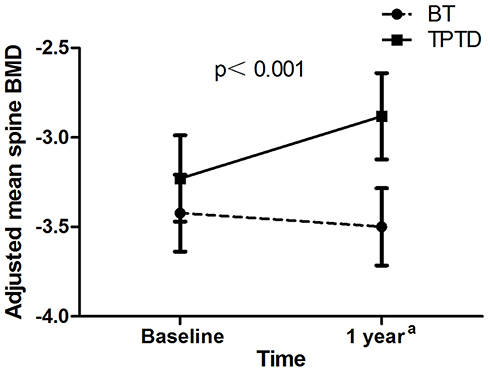 |
Figure 4 Changes in adjusted spine BMD following TPTD compared with BT. Notes: Data presented is from LMMRM analysis. Adjusted model by age, BMI, BMD at baseline, glucocorticoid usage. aAs post-BMD measurement was not completed of patients without NVCFs in BT group, data only include values when NVCFs occurs (n=43). Abbreviations: TPTD, Teriparatide; BT, basic treatment; BMD, bone mineral density. |
Discussion
The immediate efficacy of percutaneous kyphoplasty in the treatment of OVCFs has long been widely recognized, but the recurrence of clinical symptoms is a prevalent issue during the course of follow-up.27 Systematic reviews concerning long-term outcomes after cement augmentation suggest that the analgesic effect will be discounted as time passes, especially when NVCFs occur.6,28 Here, in the BT group, we calculated that the overall cohort incidence of NVCFs was over 20% during the 2-year follow-up period, which was significantly higher than that in the TPTD group. The positive effects of TPTD injection on patients with severe osteoporosis have been researched by previous investigations in routine clinical practice.25 To our knowledge, comparisons of the literature concerning the efficacy of TPTD treatment in the postoperative period of PKP are limited.
This study confirms the effectiveness of up to 12 months of teriparatide treatment on reducing the incidence of new vertebral compression fractures, improving HRQoL and promoting back pain relief in patients after receiving PKP. Beneficial effects on the odds of NVCFs were identified during TPTD application and the post-teriparatide period compared with effects in the BT group. The trend of reduced incidence of NVCFs was accompanied by the improvement in HRQoL and the relief of back pain at all postbaseline visits during teriparatide treatment. Our findings suggest the positive impact of TPTD therapy in a real-world setting of patients with a follow-up period of up to 2 years.
Analyzing the risk factors related to NVCFs is significantly necessary for treatment. Our work has important implications for verifying previous results. Some investigators believe that the occurrence of NVCFs should be regarded as the consequence of improvements in stiffness achieved by augmentation with bone cement. These investigators reported an increase in the incidence of NVCFs, especially adjacent vertebral compression fractures, after bone cement augmentation compared with conservative treatment.29 Augmented vertebrae alter the biomechanics of load transfer to adjacent vertebrae due to increased stiffness and strength, which increases the stress on other vertebrae, especially adjacent vertebrae, making them more prone to fracture.30 Others believe these fractures are simply due to the natural progression associated with osteoporosis.31 Patients with a prevalent osteoporotic vertebral fracture history were more likely to have recurrence of an incident vertebral fracture at the non-treated or treated vertebra during the study, which probably reflects an important risk factor for new fracture in observational studies.32 Some studies described that there were spinal zones where risk was considered to be increased across several levels simultaneously, especially in the thoracolumbar junction region.31,33 Usually, the PKP procedure is not sufficient to restore vertebral height and improve sagittal alignment anatomically; the remaining deformity and kyphosis will constantly alter the vectors of the forces acting throughout the spine and redistribute the load to each vertebra.34 Simultaneously, this slight change will accelerate the degenerative changes in the spinal ligaments, muscles, fascia, and other soft tissues. In vertebral bodies, PMMA fills the cancellous portion of the vertebra with an interdigitated pattern, and the loosening PMMA-cement connection is also one complication accompanied by deterioration of the bone condition.35
The association between deteriorated bone quality and the increased rate of new fractures is also evident. Like previous research,36 a significant founding in this study was that the risk of NVCFs was closely related to the dose of glucocorticoids usage. Several studies also have suggested that individuals with lower baseline BMD of the lumbar spine are at greater risk of new fractures after vertebroplasty (Attachment 1).37 A person with a severe osteoporotic spine may tolerate altered biomechanics poorly and suffer gradual malformation of the general spine. These above factors are considered to be the main mechanisms of fracture recurrence and persistent back pain after surgery. It is an urgent issue that support be provided to patients to address these problems.
The predominant treatment strategy for osteoporosis consists of medication to inhibit osteoclastic bone resorption and of anabolic drugs that stimulate bone formation. The fundamental mechanism by which TPTD acts is in the stimulation of bone formation to a greater extent than bone resorption.38 Patients with previous OVCF history usually suffer from severe osteoporosis characterized by poor osteogenesis and low BMD. TPTD should be an attractive option for first-line treatment.39 TPTD was also identified as appropriate for subjects with forced glucocorticoid use to inhibit bone formation.40 Consistently, our subgroup analysis of patients with glucocorticoid-induced osteoporosis demonstrated a visible reduction in the adjusted risk of new fracture (OR=0.0062 versus 0.1023, as described in Table 2) after 1 year of continued injection. Owing to its potential qualitative function of improving the ability to resist the mechanical pressure of vertebrae, TPTD application will minimize the shortening and kyphosis of the spine, delay following progressive bone deterioration and microarchitectural collapse gradually and induce back pain relief as well as lower the risk of NVCF. At the end of the final dose, we observed an obvious increase in the adjusted BMD value of the general spine compared to baseline BMD values in the TPTD group; similar conditions were not found in the BT group (Figure 4).
Analysis of the clinical outcomes also included data from a post-teriparatide cohort, a necessary approach that allowed us to focus more specifically on further results. We observed not only an improvement in back pain from baseline during teriparatide treatment but also a maintained effect for at least 1 year after teriparatide was discontinued. This finding is similar to the results of previous randomized controlled trials about teriparatide treatment in severe osteoporosis patients.41,42 The Chinese version of EQ-5D-5L questionnaire was adopted in this study since it has been used in health economics evaluations and considered as an important tool for drug pricing and reimbursement in Chinese health policy, which were according to the health of general population.22 Osteoporotic fractures involve physical, psychological, and social implications related to HRQoL, a significant outcome measure by means of the EQ-5D questionnaire, which has been demonstrated to be associated with changing fracture status.43 The adjusted EQ-5D score changes from baseline in the TPTD group remained significant across all five domains (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) (Attachment 4). The results showed a similar trend consistent with those of the VAS score, which was probably ascribed to the causal relationship between persisting backache and the dimensions of anxiety/depression (AD). Notably, the improvements in HRQoL and back pain were not considerable in the presence of NVCFs, and the effect returned after a further PKP procedure and following TPTD treatment. A network meta-analysis and systematic review suggested that percutaneous vertebroplasty may be an optimal choice to relieve acute pain, whereas conventional antiosteoporotic treatment would be the key point to reduced incidence of NVCFs and improve quality of life. The management of patients with vertebral compression fractures after PKP should always conclude the prevention of additional fractures and treatment of osteoporosis.44 Similarly, our results indicate that comprehensive therapy of operation and TPTD may provide optimal outcomes in the treatment of OVCFs.
In the present paper, the ratio of NVCF in the TPTD group during the first 6 months seemed to be lower than that expressed in the BT group (Figure 2), but no significant difference was found, suggesting that the protective effects of TPTD injection on NVCFs are apparent beginning in the second interval and remain throughout the 12-month cessation phase. These results appear to be similar to those demonstrated by a previous observational study45 and provide evidence for the usage of TPTD for a duration of at least 6 months, given the poor compliance and persistence of daily injection in some patients.46
Limitations
Since previous studies found that almost two thirds of vertebral fractures are symptomatic, systematic radiologic follow-up for all eligible patients may be more reasonable to ensure that asymptomatic vertebral fractures are identified.47 The retrospective approach to analysis is a limitation in that the BMD data during the follow-up period were only included in patients with TPTD treatment and those occurred NVCFs in the BT group; thus, an important comparative indicator was lacking. Furthermore, BMD in spine can be falsely normal or high due to osteoarthritis, but we failed to correct the interference. Also, no relevant data was available to analyse whether the operator/surgeon performing PKP influences the outcome. And the high costs of TPTD made patients always refuse to fulfil the recommended using course of 24 months since Health Insurance in Qingdao only cover 12 months of expenses. So we conducted analysis about patients data with a duration of TPTD of 12 months for its clinical effects. Glucocorticoid subgroup classification was also not seriously detailed because of the complexity in real-world clinical settings. The procedure of PMMA injection (unipedicular or bipedicular) and PVP, another minimally invasive technique, may confound the study results more or less, although previous literature has identified their equal safety and effectiveness in the treatment of OVCF.48 The prevalence of diabetes (DM) was also not available in the clinical database, that is an inherent limitation of retrospective study. Further prospective data and substantial long-term follow-up data, as well as information from men with severe osteoporosis, are needed to corroborate the favorable effect of TPTD in the treatment of progressive osteoporosis in post-PKP patients.
Conclusion
In conclusion, this study suggests that, although teriparatide in routine clinical practice does not fully protect against imminent new vertebral fracture risk in women after PKP, patients will experience a significantly reduced risk of symptomatic NVCFs, accompanied by improved quality of life and sustained alleviation of back pain. These beneficial impacts demonstrated during the duration of therapy were maintained for at least 12 months after teriparatide discontinuation.
In our country, patients with severe osteoporosis experience the burden of healthcare costs during the majority of the 12 month period of TPTD treatment. Because patients are worried about this burden, they are less prone to choose or continue TPTD treatment, resulting in an increased risk of new clinical fracture and subsequent reoperation, which will further aggravate the economical and societal burden on the country;49 thus, we believe that urgent attention is needed by the government and hope our work could aid those writing treatment guidelines.
Statement Of Human Rights
This study was approved by the ethics committees of Affiliated Hospital of Qingdao University. All patients involved gave written informed consent to review their medical records. All personal details were erased before analysis to cover patient data confidentiality and comply with the Declaration of Helsinki.
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of China (81672200, 81871804). We are grateful to the Orthopedic Medical Center of the Affiliated Hospital of Qingdao University and the special procedures team.
Disclosure
The authors report that they have no conflicts of interest in this work.
References
1. Alexandra H. [Osteoporosis: prevention, diagnosis and therapy]. Medizinische Monatsschrift Für Pharmazeuten. 2002;25(5):164.
2. Bliuc D, Nguyen ND, Milch VE, Nguyen TV, Eisman JA, Center JR. Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. Jama. 2009;301(5):513–521.
3. Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporosis Int. 2006;17(12):1726–1733.
4. Atalay B, Caner H, Gokce C, Altinors N. Kyphoplasty: 2 years of experience in a neurosurgery department. Surg Neurol. 2005;64(Suppl 2):S72–76.
5. Lieberman I, Reinhardt MK. Vertebroplasty and kyphoplasty for osteolytic vertebral collapse. Clin Orthop Relat Res. 2003;415 Suppl:S176–186.
6. Georgy BA. Interventional techniques in managing persistent pain after vertebral augmentation procedures: a retrospective evaluation. Pain Physician. 2007;10(5):673–676.
7. Nagad P, Rawall S, Kundnani V, Mohan K, Patil SS, Nene A. Postvertebroplasty instability. J Neurosurg Spine. 2012;16(4):387–393. doi:10.3171/2011.12.SPINE11671
8. Boger A, Heini P, Windolf M, Schneider E. Adjacent vertebral failure after vertebroplasty: a biomechanical study of low-modulus PMMA cement. Eur Spine J. 2007;16(12):2118–2125. doi:10.1007/s00586-007-0473-0
9. Lin CC, Chen IH, Yu TC, Chen A, Yen PS. New symptomatic compression fracture after percutaneous vertebroplasty at the thoracolumbar junction. AJNR Am J Neuroradiol. 2007;28(6):1042–1045. doi:10.3174/ajnr.A0520
10. Syed MI, Patel NA, Jan S, Harron MS, Morar K, Shaikh A. New symptomatic vertebral compression fractures within a year following vertebroplasty in osteoporotic women. AJNR Am J Neuroradiol. 2005;26(6):1601–1604.
11. Boswell MV, Trescot AM, Sukdeb D, et al. Interventional techniques: evidence-based practice guidelines in the management of chronic spinal pain. Pain Physician. 2007;10(1):7–111.
12. Taylor RS, Taylor RJ, Fritzell P. Balloon kyphoplasty and vertebroplasty for vertebral compression fractures: a comparative systematic review of efficacy and safety. Spine. 2006;31(23):2747–2755. doi:10.1097/01.brs.0000244639.71656.7d
13. Lee BG, Choi JH, Kim DY, Choi WR, Lee SG, Kang CN. Risk factors for newly developed osteoporotic vertebral compression fractures following treatment for osteoporotic vertebral compression fractures. Spine J. 2019;19(2):301–305.
14. Cosman F, de Beur SJ, LeBoff MS, et al. Clinician’s guide to prevention and treatment of osteoporosis. Osteoporosis Int. 2014;25(10):2359–2381. doi:10.1007/s00198-014-2794-2
15. Vondracek SF, Linnebur SA. Diagnosis and management of osteoporosis in the older senior. Clin Interv Aging. 2009;4:121–136.
16. Vandenbroucke A, Luyten FP, Flamaing J, Gielen E. Pharmacological treatment of osteoporosis in the oldest old. Clin Interv Aging. 2017;12:1065–1077. doi:10.2147/CIA.S131023
17. Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344(19):1434–1441. doi:10.1056/NEJM200105103441904
18. Gallagher JC, Genant HK, Crans GG, Vargas SJ, Krege JH. Teriparatide reduces the fracture risk associated with increasing number and severity of osteoporotic fractures. J Clin Endocrinol Metab. 2005;90(3):1583–1587. doi:10.1210/jc.2004-0826
19. Fahrleitner-Pammer A, Langdahl BL, Marin F, et al. Fracture rate and back pain during and after discontinuation of teriparatide: 36-month data from the European Forsteo Observational Study (EFOS). Osteoporosis Int. 2011;22(10):2709–2719. doi:10.1007/s00198-010-1498-5
20. Yan L, Chang Z, Xu Z, Liu T, He B, Hao D. Biomechanical effects of bone cement volume on the endplates of augmented vertebral body: a three-dimensional finite element analysis. Chin Med J. 2014;127(1):79–84.
21. Heary RF, Parvathreddy NK, Agarwal N. Biomechanical analysis of range of motion and failure characteristics of osteoporotic spinal compression fractures in human cadaver. Indian J Orthop. 2017;51(6):672–676. doi:10.4103/ortho.IJOrtho_147_16
22. Luo N, Liu G, Li M, Guan H, Jin X, Rand-Hendriksen K. Estimating an EQ-5D-5L value set for China. Value Health. 2017;20(4):662–669. doi:10.1016/j.jval.2016.11.016
23. Luo N, Li M, Liu GG, Lloyd A, de Charro F, Herdman M. Developing the Chinese version of the new 5-level EQ-5D descriptive system: the response scaling approach. Qual Life Res. 2013;22(4):885–890. doi:10.1007/s11136-012-0200-0
24. Diggle PJ. Introduction to Liang and Zeger (1986) Longitudinal Data Analysis Using Generalized Linear Models. Breakthroughs in Statistics. 1997; 463–482.
25. Langdahl BL, Ljunggren O, Benhamou CL, et al. Fracture rate, quality of life and back pain in patients with osteoporosis treated with teriparatide: 24-month results from the extended forsteo observational study (ExFOS). Calcif Tissue Int. 2016;99(3):259–271. doi:10.1007/s00223-016-0143-5
26. Natarajan RCLJPR. Modeling covariance strueture in the analysis of repeated measures data. Statistics in Medicine. 2000;19(13):1793.
27. Lin H, Bao LH, Zhu XF, Qian C, Chen X, Han ZB. Analysis of recurrent fracture of a new vertebral body after percutaneous vertebroplasty in patients with osteoporosis. Orthop Surg. 2010;2(2):119–123. doi:10.1111/j.1757-7861.2010.00074.x
28. Tanigawa N, Kariya S, Komemushi A, et al. Percutaneous vertebroplasty for osteoporotic compression fractures: long-term evaluation of the technical and clinical outcomes. AJR Am J Roentgenol. 2011;196(6):1415–1418. doi:10.2214/AJR.10.5586
29. Farrokhi MR, Alibai E, Maghami Z. Randomized controlled trial of percutaneous vertebroplasty versus optimal medical management for the relief of pain and disability in acute osteoporotic vertebral compression fractures. J Neurosurg Spine. 2011;14(5):561–569. doi:10.3171/2010.12.SPINE10286
30. Han SL, Wan SL, Li QT, et al. Is vertebroplasty a risk factor for subsequent vertebral fracture, meta-analysis of published evidence? Osteoporosis Int. 2015;26(1):113–122. doi:10.1007/s00198-014-2848-5
31. Yi X, Lu H, Tian F, et al. Recompression in new levels after percutaneous vertebroplasty and kyphoplasty compared with conservative treatment. Arch Orthop Trauma Surg. 2014;134(1):21–30. doi:10.1007/s00402-013-1886-3
32. Cooper C, Jakob F, Chinn C, et al. Fracture incidence and changes in quality of life in women with an inadequate clinical outcome from osteoporosis therapy: the Observational Study of Severe Osteoporosis (OSSO). Osteoporosis Int. 2008;19(4):493–501. doi:10.1007/s00198-007-0488-8
33. Yu W, Xu W, Jiang X. et al. Risk factors for recollapse of the augmented vertebrae after percutaneous vertebral augmentation: a systematic review and meta-analysis. World Neurosurg;2018. 119–129. doi:10.1016/j.wneu.2017.12.019
34. Barr JD, Barr MS, Lemley TJ, McCann RM. Percutaneous vertebroplasty for pain relief and spinal stabilization. Spine. 2000;25(8):923–928. doi:10.1097/00007632-200004150-00005
35. Nuchterlein M, Bail HJ. [A rare complication of kyphoplasty is PMMA-cement loosening - case report and literature review]. Z Orthop Unfall. 2013;151(5):463–467. doi:10.1055/s-0033-1350861
36. Chitre MM, Hayes W. 3-year results of a member and physician intervention to reduce risk associated with glucocorticoid-induced osteoporosis in a health plan. J Managed Care Pharm. 2008;14(3):281–290. doi:10.18553/jmcp.2008.14.3.281
37. Hey HW, Tan JH, Tan CS, Tan HM, Lau PH, Hee HT. Subsequent vertebral fractures post cement augmentation of the thoracolumbar spine: does it correlate with level-specific bone mineral density scores? Spine. 2015;40(24):1903–1909. doi:10.1097/BRS.0000000000001066
38. Gallacher SJ, Dixon T. Impact of treatments for postmenopausal osteoporosis (bisphosphonates, parathyroid hormone, strontium ranelate, and denosumab) on bone quality: a systematic review. Calcif Tissue Int. 2010;87(6):469–484. doi:10.1007/s00223-010-9420-x
39. Oswald AJ, Berg J, Milne G, Ralston SH. Teriparatide treatment of severe osteoporosis reduces the risk of vertebral fractures compared with standard care in routine clinical practice. Calcif Tissue Int. 2014;94(2):176–182. doi:10.1007/s00223-013-9788-5
40. Saag KG, Zanchetta JR, Devogelaer JP, et al. Effects of teriparatide versus alendronate for treating glucocorticoid-induced osteoporosis: thirty-six-month results of a randomized, double-blind, controlled trial. Arthritis Rheum. 2009;60(11):3346–3355. doi:10.1002/art.24879
41. Nevitt MC, Chen P, Dore RK, et al. Reduced risk of back pain following teriparatide treatment: a meta-analysis. Osteoporosis Int. 2006;17(2):273–280. doi:10.1007/s00198-005-2013-2
42. Nevitt MC, Chen P, Kiel DP, et al. Reduction in the risk of developing back pain persists at least 30 months after discontinuation of teriparatide treatment: a meta-analysis. Osteoporosis Int. 2006;17(11):1630–1637. doi:10.1007/s00198-006-0177-z
43. Borgstrom F, Zethraeus N, Johnell O, et al. Costs and quality of life associated with osteoporosis-related fractures in Sweden. Osteoporosis Int. 2006;17(5):637–650. doi:10.1007/s00198-005-0015-8
44. Catalano A, Martino G, Morabito N, et al. Pain in osteoporosis: from pathophysiology to therapeutic approach. Drugs Aging. 2017;34(10):755–765. doi:10.1007/s40266-017-0492-4
45. Langdahl BL, Rajzbaum G, Jakob F, et al. Reduction in fracture rate and back pain and increased quality of life in postmenopausal women treated with teriparatide: 18-month data from the European Forsteo Observational Study (EFOS). Calcif Tissue Int. 2009;85(6):484–493. doi:10.1007/s00223-009-9299-6
46. Foster SA, Foley KA, Meadows ES, et al. Adherence and persistence with teriparatide among patients with commercial, medicare, and medicaid insurance. Osteoporosis Int. 2011;22(2):551–557. doi:10.1007/s00198-010-1297-z
47. Layton KF, Thielen KR, Koch CA, et al. Vertebroplasty, first 1000 levels of a single center: evaluation of the outcomes and complications. AJNR Am J Neuroradiol. 2007;28(4):683–689.
48. Wang H, Sribastav SS, Ye F, et al. Comparison of percutaneous vertebroplasty and balloon kyphoplasty for the treatment of single level vertebral compression fractures: a meta-analysis of the literature. Pain Physician. 2015;18(3):209.
49. Salaffi F, Cimmino MA, Malavolta N, et al. The burden of prevalent fractures on health-related quality of life in postmenopausal women with osteoporosis: the IMOF study. J Rheumatol. 2007;34(7):1551–1560.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.