Back to Journals » Drug Design, Development and Therapy » Volume 20
0.06% Ropivacaine Combined with Double-Hole Dural Puncture Epidural Analgesia in Labor for Primiparous Women: A Prospective Randomized Controlled Trial
Authors Piao G ![]() , Li H, Jin S, Feng L, Zhao Y, Jiang M, Zhou T, Jin M
, Li H, Jin S, Feng L, Zhao Y, Jiang M, Zhou T, Jin M
Received 16 April 2026
Accepted for publication 3 July 2026
Published 10 July 2026 Volume 2026:20 617452
DOI https://doi.org/10.2147/DDDT.S617452
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Solomon Tadesse Zeleke
Guangtian Piao,1,* Huiling Li,2,* Shengyu Jin,1 Lina Feng,3 Yan Zhao,1 Meishuang Jiang,1 Tingting Zhou,4 Meihua Jin1
1Department of Anesthesiology, Dalian Women and Children’s Medical Group, Dalian, Liaoning, People’s Republic of China; 2Laboratory Animal Center, Dalian Medical University, Dalian, Liaoning, People’s Republic of China; 3Zhongshan Hospital Affiliated to Dalian University, Dalian, Liaoning, People’s Republic of China; 4Hebei Key Laboratory of Integrated Traditional and Western Medicine in Osteoarthrosis Research, Cangzhou Hospital of TCM-WM·Hebei, Cangzhou, Hebei, People’s Republic of China
*These authors have contributed equally to this work
Correspondence: Tingting Zhou, Hebei Key Laboratory of Integrated Traditional and Western Medicine in Osteoarthrosis Research, Cangzhou Hospital of TCM-WM, Cangzhou, Hebei, People’s Republic of China, Email [email protected] Meihua Jin, Department of Anesthesiology, Dalian Women and Children’s Medical Group, Dalian, Liaoning, People’s Republic of China, Email [email protected]
Background: Ultra-low concentration local anesthetics (ULCLA) preservation of labor progress is superior to low-concentration local anesthetics (LCLA), yet their analgesic efficacy remains suboptimal. While dural puncture epidural analgesia (DPEA) enhances traditional epidural (EP) efficacy, the clinical impact of the number of dural perforations during ULCLA maintenance remains unclarified.
Objective: This study aims to evaluate the clinical efficacy and safety of 0.06% ropivacaine administered via programmed intermittent epidural bolus (PIEB) combined with double-perforation DPEA (D-DPEA) in primipara.
Methods: 270 healthy primiparous women were randomized to EP (0.1% ropivacaine), single DPEA with 0.06% ropivacaine (S-DPEA) and double DPEA with 0.06% ropivacaine (D-DPEA). All received PIEB. The main outcome was the rate of breakthrough pain (pain requiring extra medication). Labor analgesia was maintained using the PIEB mode in all three groups. The primary outcome was the incidence of the breakthrough pain. Secondary outcomes included time to adequate analgesia, characteristics of sensory and motor blockade, labor progression, mode of delivery, and maternal-neonatal safety profiles.
Results: A total of 224 primipara were included (EP group, n=74; S-DPEA group, n=74; D-DPEA group, n=76). The incidence of the breakthrough pain was significantly lower in D-DPEA group than in S-DPEA group (40.8% vs 77.0%, P < 0.001) and was comparable to that in the EP group (40.8% vs 45.9%, P = 0.524). Compared with S-DPEA, D-DPEA was associated with significantly faster analgesia onset and enhanced sacral block quality. Furthermore, compared with traditional EP, the D-DPEA group demonstrated reduced total anesthetic consumption, shorter labor durations, lower instrumental delivery rates, and a decreased incidence of maternal complications, such as hypotension and postpartum hemorrhage. Neonatal outcomes were similar among the groups.
Conclusion: The regimen of 0.06% ropivacaine combined with D-DPEA and PIEB is associated with improved obstetric outcomes compared with EP, and may mitigate the insufficient analgesia associated with ULCLA maintenance in S-DPEA.
Keywords: labor analgesia, double-hole dural puncture epidural analgesia, ultra-low concentration local anesthetic, programmed intermittent epidural bolus, breakthrough pain
Introduction
Epidural analgesia (EP) is widely recognized as a highly effective method for labor pain management owing to its definitive efficacy and titratability.1–3 Nevertheless, conventional labor EP protocols routinely utilize low-concentration local anesthetics (LCLA), such as 0.1% ropivacaine. While effective for pain relief, LCLA maintenance has been implicated in certain clinical drawbacks, including potential delays in labor progression, elevated instrumental delivery rates, maternal intrapartum fever, and an increased risk of emergency cesarean section, which may interfere with maternal-infantile safety and clinical outcomes.4–9
With the continuous promotion of Enhanced Recovery After Surgery (ERAS) concepts in obstetrics, achieving the “minimum effective concentration and dose” has become a primary target in modern labor analgesia.10 A systematic review by Halliday et al11 showed that, compared with traditional LCLA, ultra-low concentration local anesthetics (ULCLA) such as 0.06% ropivacaine can alleviate motor block, reduce the risk of circulatory depression, and minimize interference with the course of labor. However, ULCLA has limitations including short duration of analgesia, high incidence of breakthrough pain, and frequent need for rescue medication, which restrict its widespread application.
Dural puncture epidural analgesia (DPEA) is a modified technique that improves analgesic efficiency, shortens onset time, and reduces drug dosage by creating a microchannel through dural puncture before epidural catheter placement.12–14 Existing studies have shown that single-hole DPEA (S-DPEA) using 25G or 26G Whitacre needles is more effective than conventional EP,15–17 but certain research gaps persist in obstetric anesthesia practice:12,18,19 (1) the effect of different numbers of dural perforations (single vs double) on labor analgesia quality has not been systematically compared; (2) the effectiveness of ULCLA combined with DPEA is unclear; and (3) the synergistic mechanism between the number of puncture holes and local anesthetic concentration is unknown.
Based on this, we hypothesized that double-hole DPEA (D-DPEA) can enhance the central nervous system delivery efficiency of ULCLA by enlarging the transmembrane permeation area, thus overcoming the bottleneck of insufficient analgesia of ULCLA. In this study, a prospective, three-arm parallel, randomized, double-blind, placebo-controlled trial was designed to comprehensively evaluate the combined effects of “0.06% ropivacaine + double-hole DPEA + PIEB” in primiparous women.
Materials and Methods
Ethical Approval and Registration Information
This study was approved by the Ethics Committee of Dalian Women’s and Children’s Medical Center (Group) (Approval No. 2022029) and registered with the Chinese Clinical Trial Registry (ChiCTR) (Registration No. ChiCTR2400090854, website: https://www.chictr.org.cn). The study followed the principles of the Declaration of Helsinki and the CONSORT guidelines.20 All participants signed written informed consent.
Study Design
This study was a single-center, prospective, three-arm parallel, randomized, double-blind, placebo-controlled trial. The study period was from November 2024 to November 2025, conducted in the maternity ward of Dalian Women’s and Children’s Medical Center.
Inclusion and Exclusion Criteria
Inclusion criteria: (1) American Society of Anesthesiologists (ASA) physical status II in primiparous women; (2) Gestational age 37–42 weeks, singleton cephalic presentation, spontaneous labor; (3) Cervical dilatation 2–3 cm and visual analog scale (VAS) score ≥40 mm; (4) Age 18–40 years; (5) Voluntary participation and signed informed consent.
Exclusion criteria: (1) Contraindications to neuraxial anesthesia (coagulation disorders, spinal deformity, severe hypovolemia, local anesthetic allergy); (2) Use of opioids or sedatives within 4 hours before delivery; (3) High-risk pregnancy (gestational hypertension, pre-eclampsia, placenta previa, gestational diabetes, etc.); (4) BMI >40 kg/m2, estimated fetal weight ≥4000 g, or ultrasound suggesting biparietal diameter ≥100 mm and head circumference ≥350 mm; (5) Refusal to participate or presence of communication disorders, history of mental illness; (6) Accidental dural puncture during epidural placement or delivery within 1 hour of catheter placement.
Criteria for withdrawal and exclusion: Women with failed analgesia requiring re-catheterization, those who underwent intrapartum cesarean section (their labor process data were excluded from labor duration analysis, but safety data were retained), and those who did not complete the primary outcome assessment for any reason were excluded from the final analysis.
Sample Size Calculation
Based on pilot data and previous study,11 we estimated a breakthrough pain rate of 70% in the S-DPEA group and 40% in the D-DPEA group. Setting α = 0.017 (Bonferroni correction for three pairwise comparisons) and power (1-β) = 0.80, we calculated that 65 patients per group were needed. Accounting for a 20% dropout rate, we planned to enroll 75 patients per group, totaling 225 patients. The final numbers completing the study were 74, 74, and 76 in the three groups, meeting the required power.
Randomization and Blinding
SPSS 27.0 was used to generate a block randomization sequence, which allocated patients in a 1:1:1 ratio to the following three groups: EP group (0.1% ropivacaine combined with EP); S-DPEA group (0.06% ropivacaine combined with single-hole DPEA); and D-DPEA group (0.06% ropivacaine combined with double-hole DPEA). Randomization numbers were sealed in opaque envelopes and opened by an independent coordinator before analgesia administration. Only the anesthesiologist performing the neuraxial procedure was unblinded, but not involved in subsequent research evaluation. All outcome assessors, obstetric and midwifery staff, and participants remained blinded.
Anesthesia Procedure
After the laboring woman was admitted to the delivery room, an intravenous line was established, and maternal heart rate, blood pressure, pulse oximetry, respiratory rate, fetal heart rate, and uterine contractions were continuously monitored. The description of fetal heart rate and uterine contractions is stated only once for clarity. The observation time points were defined as follows (Figure 1): 10 min before neuraxial block (T0), 20 min after neuraxial block (T1), latent phase (T2), active phase (T3), second stage of labor (T4), 1 h after delivery (T5), and 72 h after delivery (T6, extended to capture delayed post-dural puncture headache). Women were placed in the left lateral position. The L3/L4 interspace was localized under ultrasound guidance (Mindray Bio-Medical Electronics Co., Ltd., model MT5). After standard disinfection and draping, an epidural puncture was performed using a 17G Tuohy needle (Camelot Medical Devices Group Co., Ltd., model AS-E/SII).
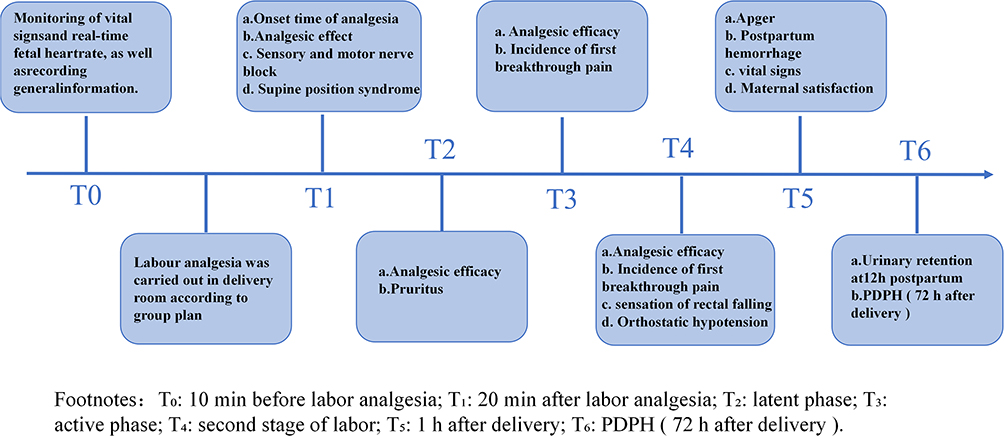 |
Figure 1 Study timeline and key milestones. T0: 10 min before labor analgesia; T1: 20 min after labor analgesia; T2: latent phase; T3: active phase; T4: second stage of labor; T5: 1 h after delivery; T6: PDPH (72h after delivery). |
EP group: only a 19-gauge epidural catheter was inserted 3 cm.
S-DPEA group: a 25G Whitacre needle was introduced through the Tuohy needle to puncture the dura mater (withdrawn after cerebrospinal fluid flow was seen), then the epidural catheter was inserted.
D-DPEA group: after the first successful puncture, the Tuohy needle was withdrawn about 2 cm, the angle was adjusted (tilted 10–15° cephalad or caudad parallel), and a second dural puncture was made. After confirming cerebrospinal fluid outflow, the epidural catheter was inserted (Figure 2). After negative aspiration for blood or cerebrospinal fluid, 3 mL of 1.5% lidocaine was given as a test dose, and the catheter position was confirmed by 5 minutes of observation.
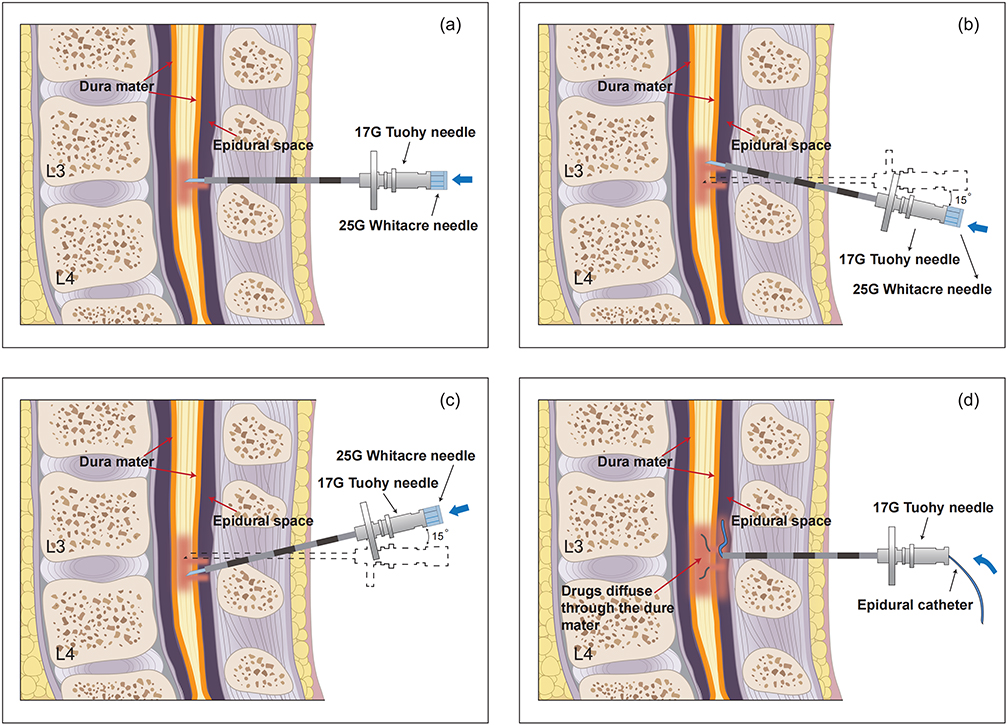 |
Figure 2 Double-hole dural puncture epidural analgesia (D-DPEA) procedure. (a) Routine epidural puncture with a 17G Tuohy needle, then a 25G Whitacre needle is introduced through the Tuohy needle to puncture the dura mater (first hole). (b and c) After the first puncture, the Tuohy needle is withdrawn ~2 cm, the angle is adjusted (10–15° cephalad or caudad), and a second dural puncture is made. (d) A 19-gauge epidural catheter is inserted 3 cm into the epidural space. |
Analgesic Regimen and Parameter Settings
Loading dose
EP group received 15 mL of 0.1% ropivacaine + 0.3 μg/mL sufentanil citrate mixture manually via the epidural catheter; S-DPEA and D-DPEA groups received 15 mL of 0.06% ropivacaine + 0.3 μg/mL sufentanil citrate mixture manually.
Maintenance Mode
All three groups used a PIEB pump (Jiangsu Aipeng Medical Technology Co., Ltd., model ZZB-IV) that delivered 10 mL of the respective concentration mixture every 40 min (EP group: 0.1% ropivacaine; S-DPEA and D-DPEA groups: 0.06% ropivacaine).21,22
Rescue
If VAS ≥40 mm, 10 mL of 0.1% ropivacaine + 0.3 μg/mL sufentanil was manually injected; if pain remained unrelieved after 20 min (VAS ≥40 mm), an additional 6 mL of 0.15% ropivacaine was injected. If still ineffective after two rescue attempts, analgesia was considered to have failed, requiring re-catheterization and exclusion from the study.
Outcome Measures
Primary Outcome
Incidence of first breakthrough pain, defined as VAS ≥40 mm requiring additional analgesic intervention. The cervical dilatation at the time of first breakthrough pain was also recorded.
Secondary Outcomes
Analgesia-related indicators: Time to achieve VAS ≤20 mm (Kaplan-Meier analysis); VAS scores at T0-T5; total local anesthetic consumption; maternal satisfaction (VAS 0–100 mm).
Nerve block characteristics: Sensory block level (loss of cold sensation by alcohol swab); motor block (modified Bromage score: 0 = no block, 1 = unable to lift leg, 2 = unable to flex knee, 3 = unable to move ankle); sacral nerve block quality (VAS score for anal tenesmus during the second stage of labor).
Labor and delivery outcomes: Duration of latent phase, active phase, second stage, and time from analgesia initiation to full cervical dilatation; fetal position and rate of manual rotation; rate of episiotomy, instrumental delivery (vacuum/forceps), and intrapartum cesarean section.
Safety Indicators
Maternal: hypotension (<80% of baseline), supine hypotension syndrome, orthostatic hypotension; pruritus, intrapartum fever (temperature ≥38°C), postpartum hemorrhage (≥500 mL); urinary retention at 12 h postpartum; post-dural puncture headache (PDPH) assessed daily until hospital discharge and up to 72 h after delivery to capture delayed cases.
Neonatal: 1-min and 5-min Apgar scores, umbilical artery blood gas analysis.
Statistical Analysis
SPSS 27.0 was used. Normality was tested with the Kolmogorov–Smirnov test. For non-normally distributed continuous variables and ordinal data, comparisons among three groups were performed using the Kruskal–Wallis test. Categorical variables were compared using the chi-square test or Fisher’s exact test. For pairwise post-hoc comparisons, P values were adjusted using the Bonferroni method, with a corrected significance threshold of α = 0.017 (0.05/3). Time to achieve VAS ≤20 mm was analyzed using Kaplan-Meier survival analysis and compared among groups with the Log rank test. Overall between-group differences were considered significant at P < 0.05; pairwise comparisons were considered significant only when Bonferroni-adjusted P < 0.017.
Results
Baseline Characteristics
A total of 300 nulliparous parturients were screened for eligibility, of whom 270 were randomized into the three study arms (90 per group). 224 parturients completed the entire protocol and were included in the final data synthesis (Figure 3). Reasons for withdrawal/exclusion were: intrapartum cesarean section (EP group n=7, S-DPEA group n=1, D-DPEA group n=2), macrosomia (EP n=5, S-DPEA n=7, D-DPEA n=5), failed puncture (S-DPEA group n=3, D-DPEA group n=4), rapid delivery (EP group n=3, S-DPEA group n=4, D-DPEA group n=3) and incomplete postpartum data (EP n=1, S-DPEA n=1). There were no statistically significant differences among the three groups with respect to maternal age, gestational age, BMI, baseline cervical dilation, fetal biparietal diameter, estimated fetal weight, or baseline mean arterial pressure (P > 0.05) (Table 1).
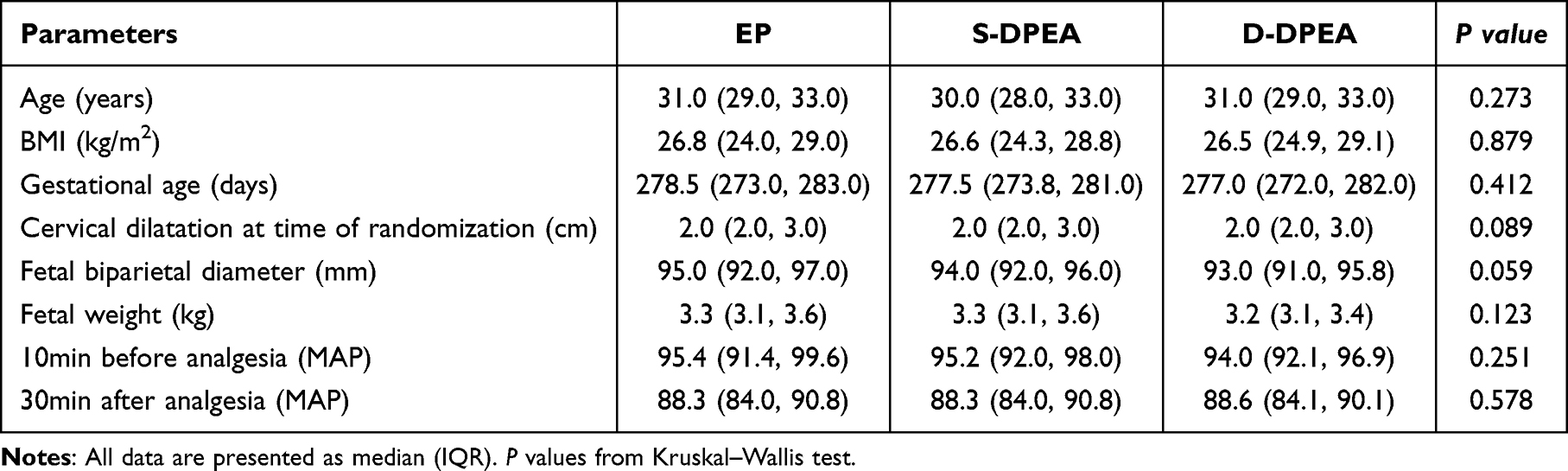 |
Table 1 Demographic Characteristics |
 |
Figure 3 CONSORT flow diagram. |
Primary Outcome: Incidence of First Breakthrough Pain
The incidence of first breakthrough pain was 40.8% in the D-DPEA group, which was significantly lower than the 77.0% observed in the S-DPEA group (adjusted P < 0.001) and not statistically different from the EP group (45.9%, adjusted P = 0.524). The cervical dilatation at first breakthrough pain was 8.0 cm (IQR: 6.0–10.0) in the D-DPEA group, 8.0 cm (IQR: 8.0–10.0) in the EP group, and 6.0 cm (IQR: 5.0–10.0) in the S-DPEA group. Breakthrough pain occurred significantly earlier in the S-DPEA group than in the EP group (adjusted P = 0.006) and D-DPEA group (adjusted P = 0.408, not significant) (Figures 4 and 5).
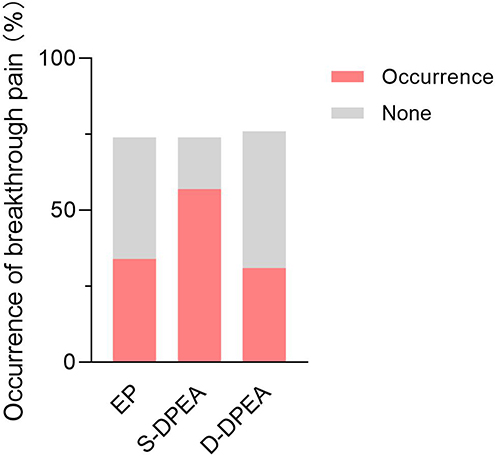 |
Figure 4 Comparison of the incidence of first breakthrough pain among the three groups. Breakthrough pain was defined as VAS ≥40 mm requiring additional local anesthetic. D-DPEA vs EP: adjusted P = 0.524; D-DPEA vs S-DPEA: adjusted P < 0.001. |
 |
Figure 5 Cervical dilatation at first breakthrough pain. S-DPEA group had significantly earlier breakthrough pain than EP (adjusted P = 0.006); D-DPEA vs S-DPEA: adjusted P = 0.408 (not significant); D-DPEA vs EP: adjusted P = 0.408. |
Time to Onset of Analgesia (VAS ≤20 Mm)
Kaplan-Meier analysis demonstrated that the overall cumulative block onset rate to achieve adequate analgesia (VAS ≤ 20 mm) differed significantly among the three groups. The onset of analgesia in the D-DPEA group was 9.72 min (95% CI: 9.39–10.06), significantly faster than in the S-DPEA group (14.49 min, 95% CI: 14.14–14.84, log-rank P < 0.001), and comparable to the EP group (9.38 min, 95% CI: 9.01–9.74, P = 0.218) (Figure 6).
 |
Figure 6 Time to onset of analgesia (VAS ≤20 mm). Kaplan-Meier curves. Overall log-rank P < 0.001; D-DPEA vs EP: P = 0.218; D-DPEA vs S-DPEA: P < 0.001. |
Quality of Sacral Nerve Block
The VAS scores for anal tenesmus during the second stage of labor were 6.5 (IQR: 6.0, 7.0) cm in the D-DPEA group, 7.5 (IQR: 7.0, 8.0) cm in the S-DPEA group, and 7.0 (IQR: 7.0, 7.5) cm in the EP group. Overall between-group difference P < 0.001; pairwise comparisons: D-DPEA vs S-DPEA adjusted P < 0.001, D-DPEA vs EP adjusted P = 0.003 (Table 2). Post-hoc pairwise comparisons with Bonferroni correction confirmed that the quality of sacral nerve blockade in the deep pelvic floor was significantly superior in the D-DPEA group compared with both the S-DPEA group (P < 0.001) and the traditional EP group (P = 0.003).
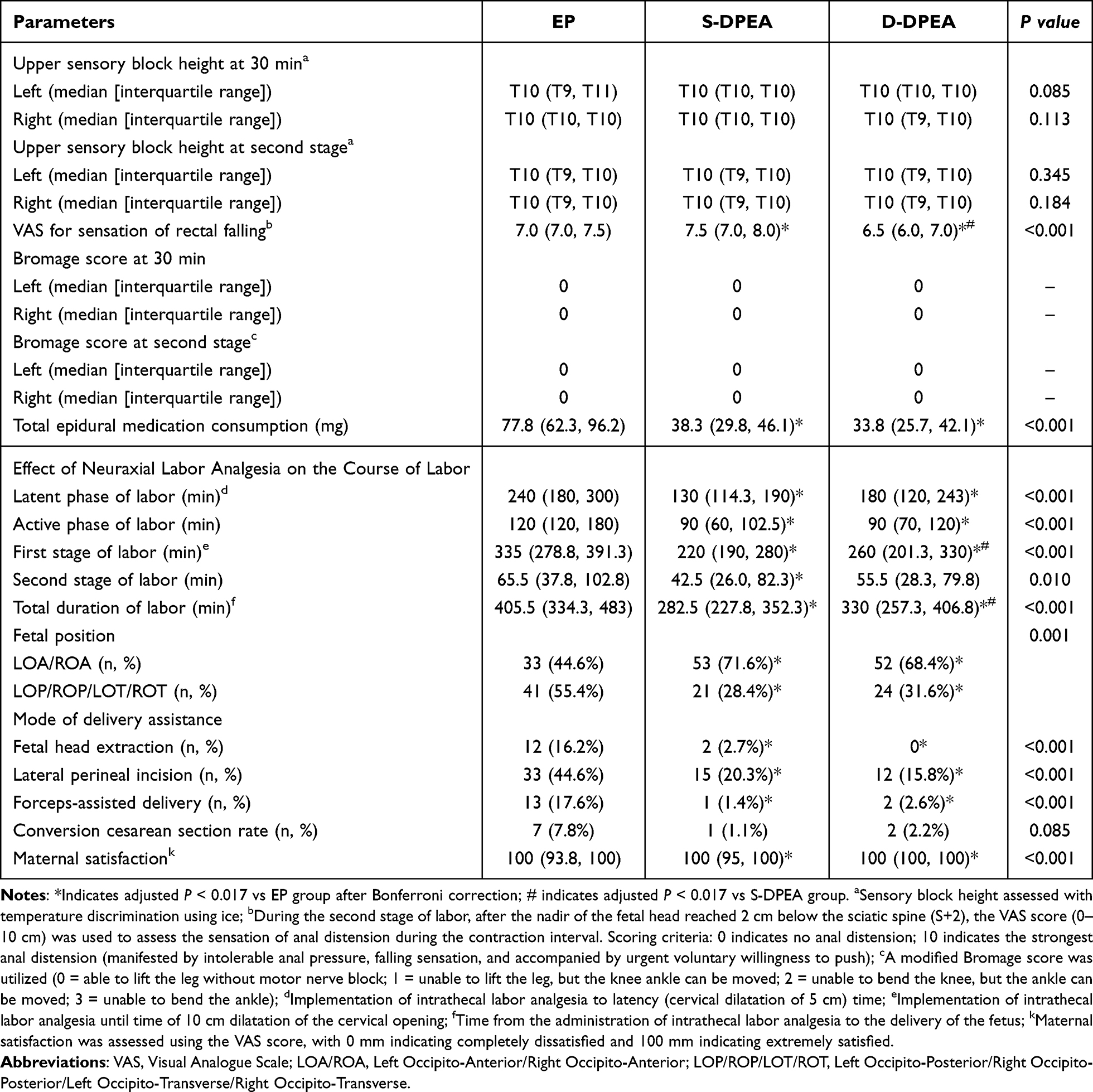 |
Table 2 Block Quality Characteristics and Obstetric Delivery Features |
Drug Consumption and Maternal Satisfaction
The total cumulative dose of ropivacaine consumed during labor was 33.8 (IQR: 25.7, 42.1) mg in the D-DPEA group, 38.3 (IQR: 29.8, 46.1) mg in the S-DPEA group, and 77.8 (IQR: 62.3, 96.2) mg in the EP group. Ropivacaine consumption was significantly lower in both the D-DPEA and S-DPEA groups than in the traditional EP group (P < 0.001), while no significant difference was identified between the D-DPEA and S-DPEA groups (P = 0.932). Maternal satisfaction scores were 100 (IQR: 100, 100) mm in the D-DPEA group, 100 (IQR: 95, 100) mm in the S-DPEA group, and 100 (IQR: 93.8, 100) mm in the EP group. Parturients in the D-DPEA and S-DPEA groups reported significantly higher satisfaction scores than those in the traditional EP group (adjusted P < 0.001), with no significant difference between the two DPEA techniques (adjusted P = 1.000) (Table 2).
Labor Progress and Obstetric Delivery Outcomes
The latent phase was significantly shorter in the D-DPEA group than in the EP group (180 vs 240 min, adjusted P < 0.001), with no significant difference compared to the S-DPEA group (180 vs 130 min, adjusted P = 0.051). The active phase was significantly shorter in the D-DPEA group than in the EP group (90 vs 120 min, adjusted P < 0.001), with no difference versus the S-DPEA group (90 vs 90 min, adjusted P = 0.243). The time from analgesia initiation to full cervical dilatation was significantly shorter in the D-DPEA group than in the EP group (260 vs 335 min, adjusted P < 0.001) but significantly longer than in the S-DPEA group (260 vs 220 min, adjusted P = 0.032). The duration of the second stage of labor did not differ significantly among the three groups (P = 0.121).
The combined rate of occiput posterior/transverse position with manual rotation was significantly lower in the D-DPEA group than in the EP group (31.6% vs 55.4%, adjusted P = 0.009), with no difference compared to the S-DPEA group (31.6% vs 28.4%, adjusted P = 0.669). Rates of episiotomy (15.8% vs 44.6%), vacuum extraction (0 vs 16.2%), and forceps delivery (2.6% vs 17.6%) were all significantly lower in the D-DPEA group than in the EP group (adjusted P = 0.0003, 0.0003, and 0.006, respectively), with no differences versus the S-DPEA group (P = 0.475, 0.242, and >0.999). The rate of intrapartum cesarean section showed a decreasing trend in the D-DPEA group compared to EP (2.2% vs 7.8%, adjusted P = 0.255), but the difference was not statistically significant (Table 2).
Safety Outcomes
Maternal-neonatal safety data are presented in Table 3. The incidence of definitive post-dural puncture headache (PDPH) within 72 hours after delivery was 1.4% (1/74) in the EP group, 1.4% (1/74) in the S-DPEA group, and 1.3% (1/76) in the D-DPEA group, with no statistically significant differences identified across the three arms (P = 1.000). The single case of headache reported in the EP group was formally evaluated by a consulting neurologist and confirmed to be a tension-type headache secondary to intranatal exhaustion and orthostatic hypotension, completely unrelated to dural mechanical trauma. The incidence of supine hypotensive syndrome was significantly lower in the D-DPEA group (0%) than in the traditional EP group (8.1%, adjusted P = 0.024), with no difference versus S-DPEA (2.7%, adjusted P > 0.999). Similarly, the incidence of orthostatic hypotension was significantly reduced in the D-DPEA group (1.3%) compared with the EP group (39.2%, adjusted P < 0.001), with no difference versus S-DPEA (4.1%, adjusted P > 0.999). No significant differences were observed among the three groups in pruritus (P = 0.680) or intrapartum fever (P = 0.230). Postpartum hemorrhage was lower in the D-DPEA group (0%) than in the EP group (13.5%, adjusted P = 0.002). Although the overall comparison of urinary retention showed a difference (P = 0.033), after Bonferroni correction none of the pairwise comparisons reached significance. All neonates across the three groups exhibited stable 1-min, 5-min, and 10-min Apgar scores ($>8$), and their umbilical artery blood gas parameters (pH) remained entirely within normal physiological limits. (Table 3).
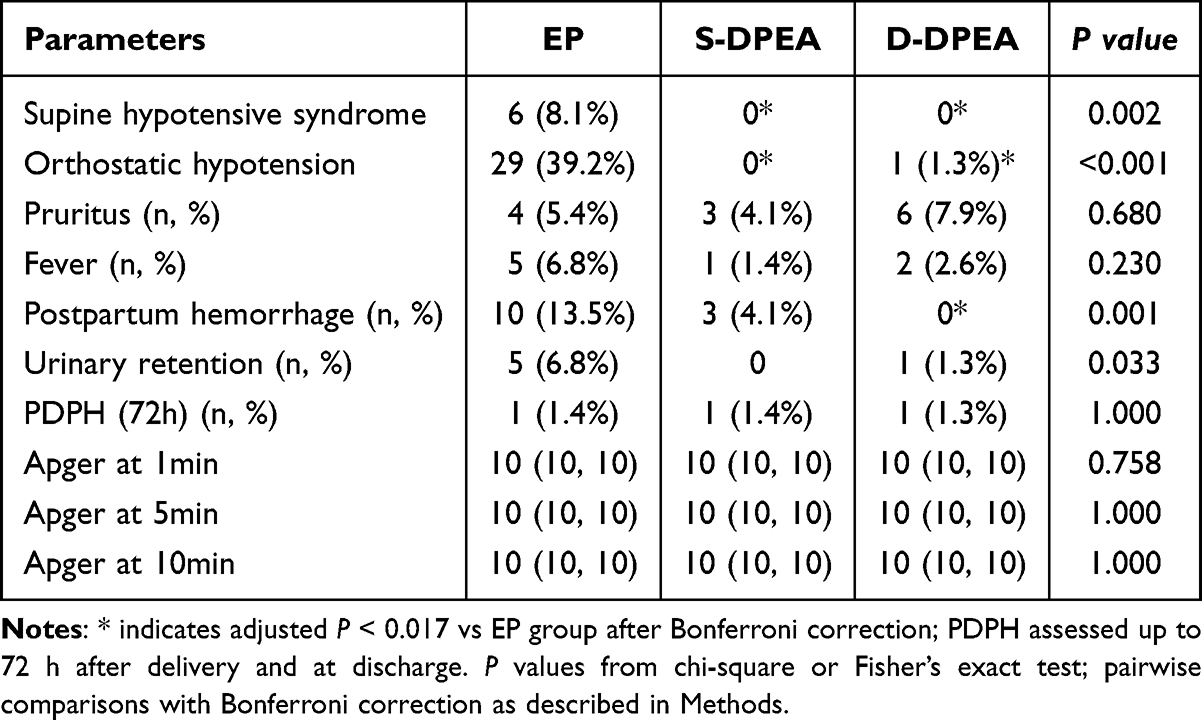 |
Table 3 Maternal and Infant Safety |
Discussion
D-DPEA Enhances Analgesic Stability of ULCLA
The core finding of this study is that D-DPEA reduced the incidence of breakthrough pain with 0.06% ropivacaine ULCLA maintenance from 77.0% to 40.8%, approaching the level of traditional EP (45.9%). This finding addresses the clinical challenge that ultra-low concentration local anesthetic techniques are typically accompanied by an increased risk of poor analgesic quality and frequent breakthrough pain. The underlying anatomical and physical mechanism is primarily attributed to the creation of dual dural microchannels. By doubling the number of perforations, D-DPEA significantly enlarges the effective surface area for drug exchange across the dura-arachnoid mater.
This modification enhances the transmeningeal translocation efficiency of local anesthetics, allowing dilute 0.06% ropivacaine to accumulate more rapidly in the subarachnoid space to reach the required minimum effective analgesic concentration.23 Our findings expand upon the work of Yu et al, who reported that double-perforation DPEA using 25-gauge Whitacre needles enhanced the analgesic quality of standard 0.1% ropivacaine.24 In this study, we successfully applied this technical approach to ultra-low concentration regimens, which aligns with contemporary obstetric ERAS principles. Furthermore, the timing of breakthrough pain in the D-DPEA group was delayed from 6 cm (S-DPEA) to 8 cm of cervical dilatation, suggesting that the double-hole design provides more durable sensory blockade and reduces late active-phase analgesic attenuation. Simultaneously, despite using an ultra-low concentration, the block onset time in the D-DPEA group (9.72 min) was equivalent to that of the traditional EP group and significantly faster than that of the S-DPEA group (14.49 min), illustrating a technique-optimized analgesia model.25 Importantly, parturients in the D-DPEA group reported lower rectal tenesmus scores during the second stage of labor (VAS 6.5 cm), indicating that this technique achieves superior blockade of deep pelvic nociceptive pathways (S2–S4 segments), which optimizing conditions for vaginal delivery.
Previous studies comparing S-DPEA with EP using spinal needles of various gauges (25G, 26G, or 27G) have reported inconsistent findings.18 Thomas et al found that S-DPEA with a 27-gauge needle provided no clinical improvement over conventional EP with 0.11% bupivacaine.26 Chau et al and Wilson et al reported that S-DPEA with 25-gauge and 26-gauge needles hastened block onset and improved sacral spread.15,16 Tan et al observed that 25-gauge S-DPEA did not improve labor analgesia quality in obese parturients receiving 0.1% ropivacaine.19 The primary explanation for these discrepancies lies in the inherent fibroelastic properties of the human dura mater. The dense bundles of dural collagen fibers possess substantial elastic recoil, which can naturally close up to 80% of a single needle perforation tract shortly after needle withdrawal. This elastic closure creates vast individual variations in the actual patency of single microchannels, frequently resulting in inconsistent transmeningeal drug diffusion and minor clinical advantages over standard EP.27,28 By adopting the D-DPEA approach—utilizing a 25-gauge Whitacre needle to introduce two parallel, distinct perforations—we successfully stabilized the transmeningeal conduit, ensuring consistent drug diffusion even under ultra-low concentration conditions.
Optimization of Obstetric Delivery and Labor Progression Outcomes
Compared with the traditional EP group, the D-DPEA group demonstrated a reduction in the duration of labor, shortening the latent phase by nearly 60 minutes and the active phase by approximately 30 minutes. Concurrently, the rates of persistent occiput malposition, lateral episiotomy, and instrumental delivery (vacuum extraction and forceps) were significantly decreased.
This optimization of obstetric outcomes is driven by distinct physiological mechanisms: 1) The ultra-low local anesthetic concentration (0.06% ropivacaine) successfully achieves differential nerve block, selectively interrupting nociceptive sensory fibers while leaving maternal motor function completely unimpaired. This preserves maternal pelvic floor muscle tone and preserves endogenous uterine contractility, which facilitates spontaneous fetal head rotation during the second stage of labor;29 2) Effective pain relief reduces stress-induced sympathetic activation, maintaining uterine blood flow;30 3) Better analgesia enhances maternal pushing efficiency.31 Although we observed a clinical trend toward a reduced intrapartum cesarean section rate in the D-DPEA group vs the EP group (2.2% vs 7.8%), this difference did not reach statistical significance within the current sample size, which warrants further verification in large multicenter trials.
Safety Analysis and Technical Feasibility Within the ERAS Framework
Regarding headache incidence, we extended PDPH surveillance to 72 hours and discharge. The incidence of PDPH in the D-DPEA group was 1.3%, which was no significance with the S-DPEA group (1.4%) and EP group (1.4%). Although double-hole puncture theoretically might increase dural injury, the 25G Whitacre needle has excellent self-sealing properties due to its pencil-point design, and with parallel orientation and adequate spacing, the actual injury may not be additive.32 The identification of a single tension headache in the EP group underscores that postpartum headaches are multifactorial, frequently arising from dehydration or physical exhaustion independent of dural trauma. Importantly, as this was a single-center study with a limited sample size, the power to detect low-incidence adverse events such as PDPH is limited; larger multicenter studies are needed to confirm these safety findings.
Orthostatic hypotension was significantly less frequent in the D-DPEA group (1.3% vs 39.2%), supporting the suitability of this technique for ambulatory labor analgesia.33 Postpartum hemorrhage was also significantly reduced (0 vs 13.5%), suggesting minimal impact on sympathetic tone and uterine contractility, which may be particularly beneficial for hemodynamically unstable women.34,35
Innovations and Clinical Implications
This investigation provides three innovative contributions to modern obstetric anesthesia: 1) It provides the first clinical demonstration that the number of dural perforations is an effective, controllable technical variable capable of regulating ULCLA block efficiency, illustrating that technical refinements can compensate for reduced drug concentrations; 2) It establishes a triple-optimized model of “ULCLA + D-DPEA + PIEB” that balances effective analgesia, low labor disruption, and high safety; 3) It refines the evaluation framework for labor analgesia by newly increased breakthrough pain timing and specific sacral nerve block scores. Based on these findings, we recommend the “0.06% ropivacaine + D-DPEA + PIEB” protocol as a potential labor analgesia strategy for nulliparous women, particularly for individuals who prioritize a natural delivery process, seek to minimize medicalized obstetric interventions, and wish to maintain mobility during labor.
Limitations and Future Directions
Several limitations of this study must be considered: 1) Single-center design and limited sample size – the results need confirmation in larger, multicenter studies, and the power to detect rare adverse events (eg, PDPH) was insufficient. 2) Population restriction – only healthy, non-obese, non-macrosomic primiparous women were included; extrapolation to high-risk populations (eg, obesity, pre-eclampsia) requires caution. 3) Subjective assessment of block quality – our evaluation of sacral and sensory blockade relied primarily on clinical tests and subjective maternal scoring; future investigations should incorporate objective assessment modalities, such as neurophysiological testing or advanced magnetic resonance imaging (MRI) tracking of drug spread. 4) Technical difficulty – the double-hole technique requires operator skill and standardized training for widespread adoption. 5) Mechanistic exploration – the influence of different puncture angles and inter-hole distances on drug spread was not analyzed; pharmacokinetic modeling would be valuable.
Future Directions
Future research directions should focus on initiating large-scale, multicenter randomized controlled trials (RCTs). Additionally, integrating individualized dural puncture configurations with automated, closed-loop intelligent epidural infusion devices represents a promising avenue toward achieving precise labor analgesia systems.
Conclusion
The implementation of a combined “0.06% ropivacaine + D-DPEA + PIEB” protocol for labor analgesia in nulliparous parturients significantly decreases the incidence of breakthrough pain, hastens block onset, and provides improved pelvic floor sacral blockade quality. Concurrently, this strategy protects labor progression, minimizes instrumental assisted delivery rates, reduces local anesthetic mass requirements, and maintains optimal maternal-neonatal safety profiles. Compared with traditional LCLA EP, this regimen successfully preserves labor progress; compared with single-perforation DPEA, it overcomes the therapeutic limitations of inadequate analgesia associated with ULCLA maintenance, offering a refined clinical pathway for modern labor pain management.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Doctoral Startup Fund of Dalian Women and Children’s Medical Group.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Hawkins JL. Epidural analgesia for labor and delivery. N Engl J Med. 2010;362(16):1503–14. doi:10.1056/NEJMct0909254
2. Kearns RJ, Lucas DN. Neuraxial analgesia in labour and the foetus. Best Pract Res Clin Anaesthesiol. 2023;37(1):73–86. doi:10.1016/j.bpa.2023.02.005
3. Carter MV, Yu TM, Burton BN. Trends in neuraxial labor analgesia utilization: comment. Anesthesiology. 2025;143(3):781–782. doi:10.1097/ALN.0000000000005574
4. Maaløe N, Kujabi ML, Nathan NO, et al. Inconsistent definitions of labour progress and over-medicalisation cause unnecessary harm during birth. BMJ. 2023;383:e076515. doi:10.1136/bmj-2023-076515
5. Patel S, Ciechanowicz S, Blumenfeld YJ, et al. Epidural-related maternal fever: incidence, pathophysiology, outcomes, and management. Am J Clin Exp Obstet Gynecol. 2023;228(5):S1283–S1304.e1. doi:10.1016/j.ajog.2022.06.026
6. Callahan EC, Lee W, Aleshi P, et al. Modern labor epidural analgesia: implications for labor outcomes and maternal-fetal health. Am J Obstet Gynecol. 2023;228(5s):S1260–s1269. doi:10.1016/j.ajog.2022.06.017
7. Stockert E, Siadat S, Bateman BT, et al. Trends in neuraxial labor analgesia utilization by race and ethnicity among nulliparous individuals undergoing spontaneous vaginal delivery, United States, 2007 to 2022. Anesthesiology. 2025;142(2):409–411. doi:10.1097/ALN.0000000000005274
8. Butwick AJ, Wall-Wieler E. Evidence mounts refuting an association between epidural use and neurodevelopmental adverse outcomes in children. JAMA Network Open. 2021;4(10):e2131722. doi:10.1001/jamanetworkopen.2021.31722
9. Kearns RJ, Shaw M, Gromski PS, et al. Association of epidural analgesia in women in labor with neonatal and childhood outcomes in a population cohort. JAMA Network Open. 2021;4(10):e2131683. doi:10.1001/jamanetworkopen.2021.31683
10. Peng Q, Yang Z, Zhang W, et al. Comparison of median effective concentration of ropivacaine in multiparas or primiparas during epidural labor analgesia: STROBE compliant. Medicine. 2020;99(1):e18673. doi:10.1097/MD.0000000000018673
11. Halliday L, Kinsella M, Shaw M, et al. Comparison of ultra-low, low and high concentration local anaesthetic for labour epidural analgesia: a systematic review and network meta-analysis. Anaesthesia. 2022;77(8):910–918. doi:10.1111/anae.15756
12. Singh PM, Monks DT, Bhat AD, et al. Epidural analgesia versus dural puncture epidural analgesia in labouring parturients: a meta-analysis of randomised controlled trials. Br J Anaesth. 2025;134(5):1402–1414. doi:10.1016/j.bja.2025.01.033
13. Lin W, Lin J, Yang Y, et al. Dural puncture epidural with 25-G spinal needles versus conventional epidural technique for labor analgesia: a systematic review of randomized controlled trials. Technol Health Care. 2024;32(2):495–510. doi:10.3233/THC-230059
14. Walker S, Fernando R. Dural puncture with a 26-gauge spinal needle affects spread of epidural anesthesia. Anesth Analg. 1997;84(1):228. doi:10.1213/00000539-199701000-00046
15. Wilson SH, Wolf BJ, Bingham K, et al. Labor analgesia onset with dural puncture epidural versus traditional epidural using a 26-gauge whitacre needle and 0.125% bupivacaine bolus: a randomized clinical trial. Anesth Analg. 2018;126(2):545–551. doi:10.1213/ANE.0000000000002129
16. Cappiello E, O’Rourke N, Segal S, et al. A randomized trial of dural puncture epidural technique compared with the standard epidural technique for labor analgesia. Anesthesia Analg. 2008;107(5):1646–1651. doi:10.1213/ane.0b013e318184ec14
17. Contreras F, Morales J, Bravo D, et al. Dural puncture epidural analgesia for labor: a randomized comparison between 25-gauge and 27-gauge pencil point spinal needles. Reg Anesth Pain Med. 2019;44(7):750–753. doi:10.1136/rapm-2019-100608
18. Segal S, Pan PH. Dural puncture epidural for labor analgesia: is it really an improvement over conventional labor epidural analgesia? Anesthesiology. 2022;136(5):667–669. doi:10.1097/ALN.0000000000004187
19. Tan HS, Reed SE, Mehdiratta JE, et al. Quality of labor analgesia with dural puncture epidural versus standard epidural technique in obese parturients: a double-blind randomized controlled study. Anesthesiology. 2022;136(5):678–687. doi:10.1097/ALN.0000000000004137
20. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. PLoS Med. 2010;7(3):e1000251. doi:10.1371/journal.pmed.1000251
21. Yao H-Q, Huang J-Y, Deng J-L, et al. Randomized assessment of the optimal time interval between programmed intermittent epidural boluses when combined with the dural puncture epidural technique for labor analgesia. Anesthesia Analg. 2022;136(3):532–539. doi:10.1213/ANE.0000000000006201
22. Xiao F, Yao H-Q, Qian J, et al. Determination of the optimal volume of programmed intermittent epidural bolus when combined with the dural puncture epidural technique for labor analgesia: a random-allocation graded dose-response study. Anesthesia Analg. 2023;137(6):1233–1240. doi:10.1213/ANE.0000000000006451
23. Mo X, Yu J, Qin Z, et al. Comparison of the dural puncture epidural and conventional epidural analgesia maintained using programmed epidural boluses for labor analgesia. Drug Des Devel Ther. 2025;19:4373–4382. doi:10.2147/DDDT.S521681
24. Yu H, Wang J-F, Wang S, et al. Double dural puncture epidural improves quality of labour analgesia without increasing adverse effects in primipara: a randomised controlled trial. Eur J Anaesthesiol. 2025;42(9):774–782. doi:10.1097/EJA.0000000000002198
25. Reina MA, Lopez A, Badorrey V, De Andres JA, Martin S. Dura-arachnoid lesions produced by 22 gauge Quincke spinal needles during a lumbar puncture. J Neurol Neurosurg Psychiatry. 2004;75(6):893–897. doi:10.1136/jnnp.2003.017624
26. Thomas JA, Pan P, Harris L, et al. Dural puncture with a 27-gauge Whitacre needle as part of a combined spinal-epidural technique does not improve labor epidural catheter function. Anesthesiology. 2005;103(5):1046–1051. doi:10.1097/00000542-200511000-00019
27. Reina MA, Puigdellívol-Sánchez A, Gatt SP, et al. Electron microscopy of dural and arachnoid disruptions after subarachnoid block. Reg Anesth Pain Med. 2017;42(6):709–718. doi:10.1097/AAP.0000000000000667
28. Song Y, Du W, Zhou S, et al. Effect of dural puncture epidural technique combined with programmed intermittent epidural bolus on labor analgesia onset and maintenance: a randomized controlled trial. Anesth Analg. 2021;132(4):971–978. doi:10.1213/ANE.0000000000004768
29. Verhaeghe C, Corroenne R, Spiers A, et al. Delivery mode after manual rotation of occiput posterior fetal positions: a randomized controlled trial. Obstet Gynecol. 2021;137(6):999–1006. doi:10.1097/AOG.0000000000004386
30. Wang JJ, Yang F-PG, Tsai -C-C, et al. The neural basis of pain during labor. Am J Obstet Gynecol. 2023;228(5s):S1241–s1245. doi:10.1016/j.ajog.2023.02.012
31. Youssef A, Brunelli E, Azzarone C, et al. Fetal head progression and regression on maternal pushing at term and labor outcome. Ultrasound Obstet Gynecol. 2021;58(1):105–110. doi:10.1002/uog.22159
32. Reina M, de Leon-Casasola OA, Lopez A, De Andres J, Martin S, Mora M. An in vitro study of dural lesions produced by 25-gauge quincke and whitacre needles evaluated by scanning electron microscopy. Reg Anesth Pain Med. 2000;25(4):393–402. doi:10.1097/00115550-200007000-00013
33. Zang Y, Lu H, Zhang H, Huang J, Zhao Y, Ren L. Benefits and risks of upright positions during the second stage of labour: an overview of systematic reviews. Int J Nurs Stud. 2021;114:103812.
34. Walker KF, Kibuka M, Thornton JG, et al. Maternal position in the second stage of labour for women with epidural anaesthesia. Cochrane Database Syst Rev. 2018;2018(11). doi:10.1002/14651858.CD008070.pub4
35. de Sena Fraga CD, de Araújo RC, de Sá L, et al. Use of a peanut ball, positioning and pelvic mobility in parturient women shortens labour and improves maternal satisfaction with childbirth: a randomised trial. J Physiother. 2024;70(2):134–141. doi:10.1016/j.jphys.2024.02.017
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.