")
Back to Journals » Nature and Science of Sleep » Volume 16
The Mediating Role of Family Functions Between Pregnancy-Related Anxiety and Sleep Quality: A Cross-Sectional Study
Authors Zhu J, Li Y, Wang R, Zhang J, Liu C, Li H, Yang D, Ma S, Guan S
Received 3 November 2023
Accepted for publication 18 February 2024
Published 12 March 2024 Volume 2024:16 Pages 279—289
DOI https://doi.org/10.2147/NSS.S443612
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Valentina Alfonsi
Jiashu Zhu,1 Ye Li,1 Rui Wang,1 Jinfang Zhang,2 Can Liu,1 Hongyu Li,1 Deguang Yang,1 Shuqin Ma,2 Suzhen Guan1
1School of Public Health, Ningxia Medical University, Yinchuan City, Ningxia, People’s Republic of China; 2Obstetric Clinic, General Hospital of Ningxia Medical University, Yinchuan City, Ningxia, People’s Republic of China
Correspondence: Suzhen Guan, School of Public Health, Ningxia Medical University, Yinchuan City, Ningxia, 750004, People’s Republic of China, Tel +86 13389511821, Email [email protected] Shuqin Ma, General Hospital of Ningxia Medical University, Yinchuan City, Ningxia, 750004, People’s Republic of China, Tel +86 13895493649, Email [email protected]
Objective: To examine the relationship between pregnancy-related anxiety, family functions, and sleep quality, and to determine whether family functions mediate the relationship between pregnancy-related anxiety and sleep quality.
Methods: A cross-sectional survey was conducted on pregnant women between April to August in 2022 in the obstetrics outpatient clinic of a tertiary care hospital in the Ningxia Hui Autonomous Region of China. A total of 1014 pregnant women aged 18 years and older were surveyed. They completed questionnaires, including: general demographic characteristics, the Pregnancy-related anxiety scale (PAQ), the Family Adaptation, Partnership, Growth, Affection, and Resolve (APGAR), and the Pittsburgh Sleep Quality Index Questionnaire (PSQI). Model 4 in PROCESS was used to analyze the relationships among pregnancy-related anxiety, family functions, and sleep quality, with family functions as a mediator.
Results: Among the 1014 pregnant women, the pregnancy-related anxiety scale score was (21.84 ± 5.64). The total score of the family functions scale was (8.10± 2.26), and the overall sleep quality scale score was (7.89± 2.99). When participants were grouped according to different socio-demographic characteristics, the study showed that all variables differed from anxiety, family functions or sleep quality, except for age, pre-pregnancy BMI and whether or not they had a first birth, which was not associated with anxiety, family functions, or sleep quality (P< 0.05). The pregnancy-related anxiety was positively associated with sleep quality (P< 0.01), while family functions were negatively associated with sleep quality (P< 0.01). In addition, family functions mediate the relationship between pregnancy-related anxiety and sleep quality during pregnancy, on the first and second trimesters, intermediation rate is 9.31% (P< 0.05), and on the third trimesters, intermediation rate is 21.38% (P< 0.05).
Conclusion: Pregnancy- related anxiety is a risk factor for sleep quality, however, family functions are protective factors for sleep quality. Family functions play an intermediary role in sleep quality caused by pregnancy-related anxiety, especially on the third trimesters. This finding may provide a scientific basis for developing intervention strategies to improve the sleep quality of pregnant women.
Keywords: pregnancy-related anxiety, family functions, sleep quality, mediation effect
Introduction
The definition of sleep quality is how satisfied a person is with all aspects of sleep. The four attributes that contribute to sleep quality are efficiency, latency, duration, and arousal after sleep onset.1 Nowadays, it is increasingly recognized that sleep quality affects women’s health and well-being, especially during specific periods such as pregnancy and menopause.2 A recent meta-analysis showed that the prevalence of sleep disorders during pregnancy was 45.7%.3 Additionally, studies have shown that sleep disturbances during pregnancy may increase a woman’s risk of developing gestational diabetes and gestational hypertension.4–6 In addition to the impact on maternal health, poor sleep quality during pregnancy can also affect the immediate and long-term health of the child. Several prospective studies suggest that maternal sleep disturbance during pregnancy may increase the risk of birth preterm in pregnant women.7–9 Qingdong Lu and others conducted a meta-analysis, and the results showed that sleep disorders during pregnancy were significantly related to pregnancy-induced hypertension, gestational diabetes, premature delivery and stillbirth;10 Sanapo L, Hackmetahal et al made a systematic evaluation and meta-analysis on the relationship between sleep apnea of pregnant mothers and the growth outcome of their offspring. The results showed that the research results supported the international norm that obstructive sleep apnea was related to the increased risk of small for gestational age infants.11 Therefore, considering the adverse effects of sleep disturbances, it is crucial to identify factors associated with decreased sleep quality that could be potential clinical targets for intervention in pregnant women.
There are many factors that affect sleep quality. Previous epidemiological studies have shown that the sleep quality of pregnant women is closely related to their age, gestational age, lifestyle, physical and mental health.12–14 Among them, the psychological state of pregnant women is considered to have an important impact on the occurrence of sleep disorders.15 A survey showed that anxiety and depressive symptoms in late pregnancy increased the risk of developing sleep disturbances in pregnant women.16 It follows similar work by Rubio et al who conducted a cross-sectional study of women in Lima, Peru, and found that poor sleep quality in pregnant women was associated with prenatal depression, and generalized anxiety symptoms.17 In addition to the influence of the above factors, family factors are important for individuals to maintain good sleep quality. Some studies have shown that good family functions improve sleep quality.18,19 Up to now, there is clear evidence that pregnancy-related anxiety and family functions are related to maternal sleep quality during pregnancy, but no studies have yet examined these variables together to test for potential interactions. To fill the above research gap, our study set out to examine whether family functions play a mediating role in the relationship between pregnancy-related anxiety and sleep quality. The hypothesis tested here is that good family functions would mitigate the effects of pregnancy anxiety on sleep quality during pregnancy. We expect this study will provide useful insights into the development of prevention and intervention strategies to improve sleep quality in pregnant women. The hypothetical model is shown in Figure 1.
 |
Figure 1 The mediating effect model of family functions on the relationship between pregnancy-related anxiety and sleep quality. |
Materials and Methods
Participants and Procedures
From April 2022 to August 2022, we conducted a cross-sectional survey in the obstetrics outpatient clinic of a tertiary care hospital in the Ningxia Hui Autonomous Region of China. Inclusion criteria were: women over 18 years of age with singleton pregnancies without underlying disease. Exclusion criteria were: women with a diagnosed memory or psychiatric disorder, or women with an infectious disease (viral hepatitis or human immunodeficiency virus infection). And exclude pregnant women with other diseases that affect sleep quality (such as restless legs syndrome); Memory impairment or psychiatric disorder was defined as a self-reported history of prior psychiatric illness or current treatment such as antidepressant or anxiolytic medication use. All pregnant women received a set of questionnaires when they visited the hospital’s obstetric clinic for antenatal checkups. The survey included general demographic characteristics, psychological status during pregnancy, level of family functions, and sleep quality. We distributed a total of 1200 questionnaires and finally collected 1014 valid questionnaires. The effective response rate was 84.50%. Signed informed consent was obtained from all subjects prior to data collection. Ethical approval for the study was obtained from the Ethics Committee of Ningxia Medical University (No. 2022-G007) before the start of the study.
Questionnaire Measures
Demographic and Socio-Economic Characteristics
Demographic data include the following: residence (urban/rural); per capita monthly income of family (<¥2000/¥2000–¥5000/>¥5000); occupation (unemployed/farmers or workers/enterprise/others); Educational level (middle school and below/high school or junior college/college or Bachelor/postgraduate and above); gestational age at interview (in weeks); Personality(introverted/moderate/extrovert); Pregnancy intention(Planned Pregnancy/Let nature take its course/accidental Pregnancy); age; only child (yes/no); Whether the first birth (yes/no); Spontaneous abortions (yes/no); height; Pre-pregnancy weight; Pre-pregnancy body mass index (BMI) (kg/m2) was calculated based on participants’ pre-pregnancy self-reported weight to the nearest 0.1 kg and height to the nearest 0.1 cm and categorized as: <18.5, 18.5–23.9, ≥24 kg/m2.
Pregnancy-Related Anxiety
The Pregnancy-related anxiety scale (PAQ), which was developed by Xiao Limin et al at Anhui Medical University in China was used to evaluate the pregnancy-related anxiety of pregnant women in this study.20 The scale included a total of 13 items and was divided into three subscales: concern for self, concern for fetal health, and concern for delivery. The items were rated on a 4-point Likert scale, ranging from 1 = “no worries” to 6 = “always worried”. The total score ranges from 13 to 52. The higher the score, the more likely the subject was to suffer from pregnancy-related anxiety. A score of more than 23 indicates that the mother is suffering from pregnancy-related anxiety. In the present study, Cronbach’s α of the scale was 0.81.
Family Functions
The family functions of pregnant women were measured by family adaptation, partnership, growth, affection, and resolve (APGAR), which was compiled by Smilkstein in 1978.21 The scale included a total of 5 items and was divided into five subscales: adaptation, partnership, growth, affection, and resolution. The items were rated on a 3-point Likert scale, ranging from 0 = “hardly ever” to 2 = “almost always”. The total score is calculated by adding the results of all questions. A total score of 7–10 indicates normal family functioning. A total score of 4–6 indicates a moderately dysfunctional family. A total score of 0–3 indicates that the respondent’s family is very dysfunctional. The Cronbach’s α of the scale was 0.81.
Sleep Quality
We assessed sleep quality using the Pittsburgh Sleep Quality Index (PSQI), which was developed by Buysse et al in 1989 and is now used relatively frequently in psychiatric practice and clinical research.22 The PSQI consists of a total of 24 questions, of which 19 are self-assessed and the rest are rated by the bed partner or roommate. The self-assessment questions were mainly related to various factors involved in sleep quality. These factors were further categorized into seven sections These factors were further categorized into seven sections, each weighted equally on a 0–3 scale. The seven component scores are then summed to yield a global PSQI score, which has a range of 0–21; higher scores indicate worse sleep quality. Cronbach’s α of the scale was 0.83. Liu Xianchen et al validated the reliability and validity of the Pittsburgh Sleep Quality Index using psychological testing and statistical techniques. The results showed that the Pittsburgh Sleep Quality Index (PSQI) had good internal consistency and retest reliability, as well as high consistency and criterion-related validity. The diagnostic sensitivity of a total PSQI score of more than 7 was 98.3% and the specificity was 90.2% in distinguishing normal individuals from patients with sleep quality problems.23 Therefore, we analyzed the data using PSQI≥8 as the threshold value.
Data Analysis
We use SPSS 23.0 and Amos 26.0 to sort out and analyze the data. First, we use descriptive statistics to analyze the general demographic characteristics of the participants. Normally distributed variables were expressed as mean and standard deviation (SD). Non-normally distributed variables were expressed as the median and interquartile range (IQR). The comparison between groups is made by t–test or analysis of variance (ANOVA), the counting data is represented by the number of cases or percentage, and the comparison between groups is made by chi-square test. Secondly, Pearson correlation analysis aims to test the correlation between pregnancy-related anxiety, family function and sleep quality of pregnant women. Next, Model 4 in PROCESS, a macro program of SPSS 23.0 by Hayes, was used to model and verify the relationship between variables and model-mediated effects using the self-sampling method (Bootstrap). Finally, modeling and mediated effect path mapping using Amos 26.0 software. All p values were two-tailed with a statistically significant level of 0.05.
Results
Participant Characteristics
The characteristics of the sample pregnant women are shown in Table 1. The sample consisted of 1014 pregnant women aged 18–43 years. The mean age of the pregnant women was 30.18 (SD = 4.40), with 11.44% of the pregnant women of advanced age (age >35 years). The mean body mass index (BMI) of the pregnant women was 22.16 (SD = 3.28), with 114 (11.24%) being thin, 644 (63.51%) being medium and 256 (25.25%) being obese. The number of pregnancies in the sample ranged from 1 to 8 with a mean of 2.03 (SD=1.14). Although the gestational age of the participants ranged from 4 to 44 weeks, the mean gestational week of the study participants was 26.48 (SD=9.32). Among the study participants, 889 (87.67%) had completed high school or higher education. The majority of them lived in urban areas. According to the week of gestation, 81 (7.99%) of the participants were in early gestation, 448 (44.18%) in middle gestation, and 485 (47.83%) in late gestation.
 |
Table 1 General Demographic Characteristics of Participants (N=1014) |
Pregnancy-Related Anxiety, Family Functions, and Sleep Quality
Among the 1,014 pregnant women, 346 had pregnancy-related anxiety, with an incidence of 34.12%. The pregnancy-related anxiety scale score was (21.84 ± 5.64). The concern for oneself score was (8.00±2.28), the concern for fetus score was (10.24±3.33), and the concern for the delivery score was (3.61±1.40). A total of 258 participants with family dysfunction, including 33 participants with severe family dysfunction, accounting for 3.25% of all participants, 225 participants with moderate family dysfunction, accounting for 22.19% of all participants, and 756 participants with good family dysfunction, accounting for 74.56% of all participants. The total score of the family functions scale was (8.10±2.26), with adjustment score of (1.57±0.56), cooperation score of (1.59±0.586), maturity score (1.63±0.56), affectivity score (1.58±0.57), and closeness score (1.72±0.49). The number of participants with sleep disturbances (scale score > 7) was 508, and the incidence was as high as 50.10%. The overall sleep quality scale score was (7.89±2.99), with a subjective sleep quality score of (1.07±0.69), time to fall asleep score of (1.57±1.44), sleep duration score of (0.18±0.50), sleep efficiency score of (2.84±0.49), sleep disturbance score of (1.23±0.58), hypnosis medication score was (0.01±0.10), and daytime dysfunction score was (0.99±0.84).
Single-Factor Analysis of Pregnancy-Related Anxiety, Family Functions, and Sleep Quality
We summarized the relationship between the socio-demographic characteristics of the participants and their anxiety level, family functions and sleep quality, and the results are shown in Table 2. When participants were grouped according to different socio-demographic characteristics, the study showed that all variables differed from anxiety, family functions, or sleep quality, except for age, pre-pregnancy BMI and whether or not they had a first birth, which was not associated with anxiety, family functions or sleep quality (P<0.05). Participants who were jobless, had an unplanned pregnancy, had a history of miscarriage, and had a monthly per capita household income of <¥2000 were more likely to have pregnancy-related anxiety. In terms of family functions, participants with unplanned pregnancies who were only children, had lower literacy levels, were more introverted, were farmers or workers by profession, and had lower per capita monthly incomes scored lower. In addition to this, late-pregnancy participants with unplanned pregnancies had poorer sleep quality.
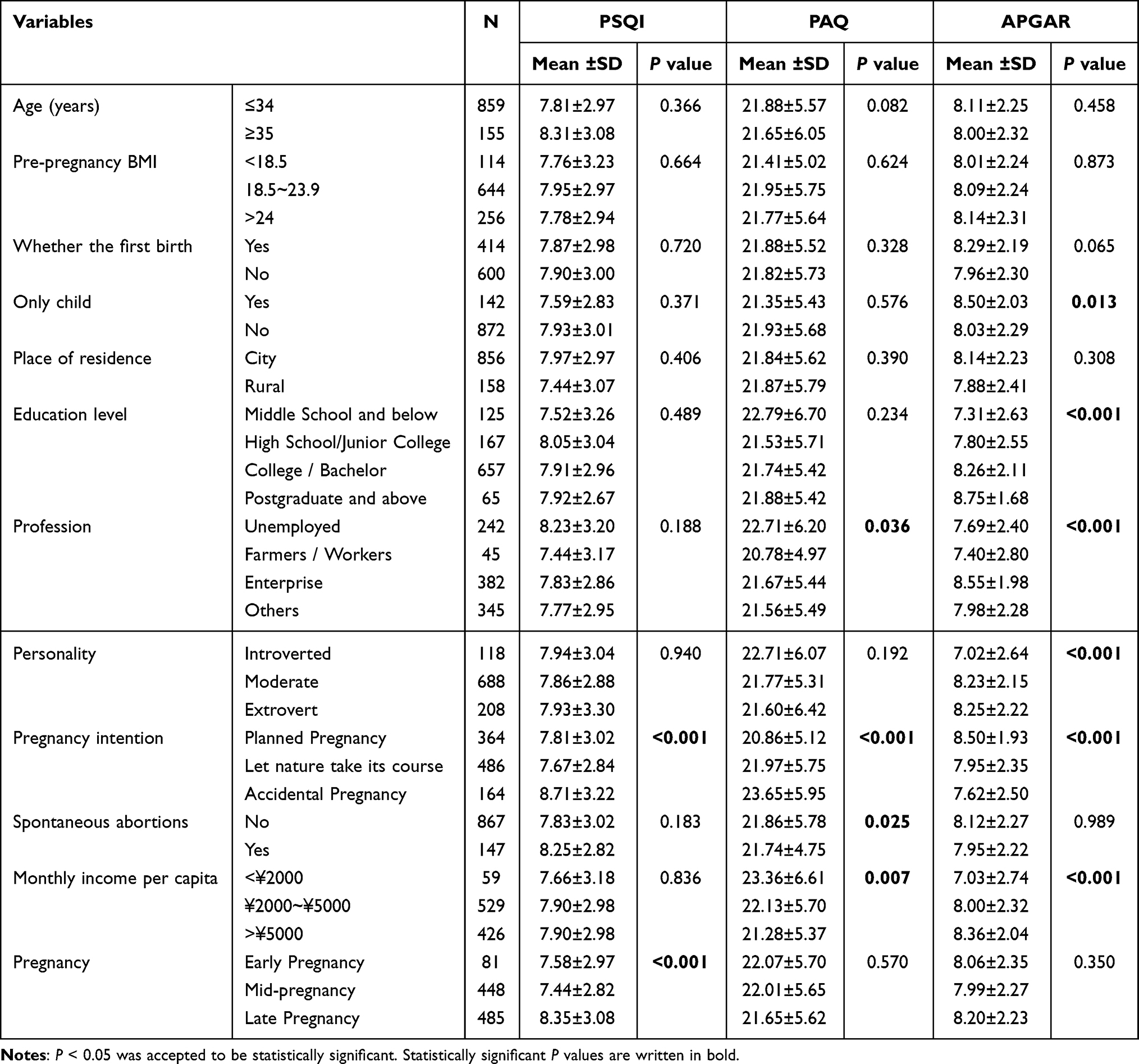 |
Table 2 The Relationship of Descriptive Socio-Demographics with Pregnancy-Related Anxiety Scale (PAQ), Family Adaptation, Partnership, Growth, Affection and Resolve, (APGAR), and Pittsburgh Sleep Quality Index (PSQI) |
Pearson’s Correlations
Correlations between all variables are shown in Figure 2. There was a small negative correlation between the pregnancy-related anxiety and the family functions (both the full-scale and subscales) indicating that the higher the family dysfunction of a pregnant woman, the more likely she is to develop pregnancy-related anxiety (P<0.01). The association between the family functions and the sleep quality indicated that the better a pregnant woman’s family functions, the better quality of sleep she would get. There was also a significant association between the pregnancy-related anxiety, the sleep quality, and its subscales which suggested that the more anxious a pregnant woman was, the worse her sleep quality would be.
 |
Figure 2 Correlations between the pregnancy-related anxiety, family functions, sleep quality, and their subscales. |
Mediating Effect Test
To determine whether family functions play a mediating role in the relationship between pregnancy-related anxiety and sleep quality among pregnant women, a Bootstrap method was used. We examined the mediating effect of family functions separately for different trimesters, and the results are presented in Tables 3 and 4. First of all, no matter what pregnancy a pregnant woman is in, family functions have a partial mediating effect between pregnancy-related anxiety and sleep quality.
 |
Table 3 Mediating Model Test of Family Functions in Anxiety and Sleep Quality During Pregnancy on the First and Second Trimesters |
 |
Table 4 Mediating Model Test of Family Functions in Anxiety and Sleep Quality During Pregnancy on the Third Trimesters |
On the first and second trimesters, pregnancy-related anxiety has a significant positive predictive effect on sleep quality (β = 0.1440, P < 0.001) and a significant negative predictive effect on family functions (β = - 0.0863, P < 0.001). When pregnancy-related anxiety and family functions simultaneously predict sleep quality, family functions can also significantly negatively predict sleep quality (β = - 0.1552, P< 0.0001), and pregnancy-related anxiety can significantly positively predict sleep quality (β=0.1306, P < 0.0001). On the third trimesters, pregnancy-related anxiety has a significant positive predictive effect on sleep quality (β = 0.1361, P < 0.0001) and a significant negative predictive effect on family functions (β = - 0.0975, P < 0.0001). When pregnancy-related anxiety and family functions simultaneously predict sleep quality, family functions can also significantly negatively predict sleep quality (β = - 0.2988, P< 0.0001), and pregnancy-related anxiety can significantly positively predict sleep quality (β=0.1070, P < 0.0001).
After the initial validation, the significance of the mediating effect of pregnancy-related anxiety was further tested by the Bootstrap self-sampling method, with a sample size of 5000 and a confidence interval (CI) of 95%. On the first and second trimesters, the indirect effect of pregnancy-related anxiety on sleep quality via family functions was observed (95% CI = (0.0036, 0.0269)). The confidence interval for indirect effect did not contain zero, which suggested that family functions played a mediating role between pregnancy-related anxiety and sleep quality. In addition, when family functions was entered to the model as a mediator, the direct effect of pregnancy-related anxiety on sleep quality was still significant (95% CI = (0.0889, 0.1724)). Therefore, family functions had a partial mediating effect in the relationship between pregnancy-related anxiety and sleep quality for pregnant women. On the third trimesters. The results showed that the 95% confidence interval of Bootstrap for the indirect effect of pregnancy-related anxiety on sleep quality was (0.0139, 0.0473), which did not contain 0, indicating a significant mediating effect; the Bootstrap 95% confidence interval for the direct effect of pregnancy-related anxiety on sleep quality was (0.0591, 0.1548), which did not contain 0, indicating a significant direct effect. With family functions as the mediating variable, pregnancy-related anxiety as the independent variable, and sleep quality as the dependent variable. We calculated the proportion of the total effect of pregnancy-related anxiety on sleep quality that was mediated by family functions. The proportion of mediation of family functions was 9.31% on the first and second trimesters, the proportion of mediation of family functions was 21.38% on the third trimesters. This leads to the conclusion that maternal family functions play a partial mediating role in the relationship between pregnancy-related anxiety and sleep quality during pregnancy, especially in late pregnancy. Amos to establish a structural equation model and the visualization of the model was shown in Figure 3.
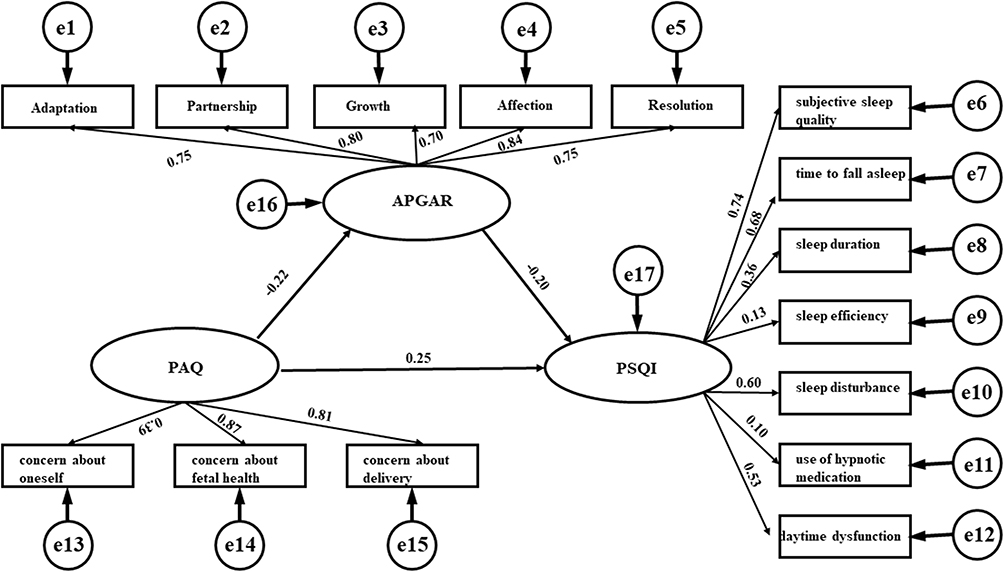 |
Figure 3 Path diagram of the mediating effect of family functions in the relationship between pregnancy-related anxiety and sleep quality (N = 1014). |
Discussion
The present study explored the associations of pregnancy-related anxiety, family functions with sleep quality, as well as examined the mediating effect of family functions between them among pregnant women. Our study reveals that maternal family functioning mediates the relationship between pregnancy-related anxiety and sleep quality, especially on the third trimesters.
In this study, more than half (50.10%) of the pregnant women had sleep disturbances. This may be closely related to the pregnant woman’s sleep environment, lifestyle habits, and changes in hormone levels. Pregnant women in late pregnancy were more likely to have sleep disorders compared to those in mid- or early pregnancy, similar to previous findings. Okun et al24 reported poor sleep quality in 49.14% of 116 pregnant women. Tsai et al25 found poor sleep quality in 45.1% of women during pregnancy in a prospective cohort study. Hung et al26 reported that 58% of pregnant women had poor sleep quality in mid-pregnancy and up to 66% in late pregnancy. Polo-Kantola et al16 reported poor overall sleep quality, difficulty falling asleep, and increased nightly awakenings in late pregnancy.
The results of this study also showed that more than one-third (34.12%) of pregnant women develop pregnancy-related anxiety during pregnancy, fear for the health of the fetus was the highest rating, which means that fear for the health of the fetus was the main psychological stressor. In an analysis of pregnant women with different socio-demographic characteristics, it was found that pregnancy-related anxiety scores were higher among pregnant women who were jobless, had an unplanned pregnancy, and had a history of miscarriage, suggesting that pregnant women with these characteristics are more likely to suffer from pregnancy-related anxiety.
Our study shows that pregnancy-related anxiety is positively correlated with sleep quality. These data supported the findings of earlier studies of pregnant women. Felder et al27 found through a survey that poor pregnancy sleep quality was common in low-income families and that poor sleep quality during pregnancy was associated with maternal psychological distress. Osnes et al28 showed that anxiety disorders are prevalent in the perinatal period and that insomnia during pregnancy was associated with perinatal anxiety. The negative impact of pregnancy-related anxiety on poor sleep quality may be due to increased cortisol arousal response and overactive hypothalamic-pituitary-adrenal (HPA) axis.
The current study investigated pregnancy-related anxiety, family functions, and sleep quality to verify whether pregnancy-related anxiety has an impact on a pregnant woman’s sleep quality through her family functions. Not surprisingly, the partial mediating effect of family functioning on pregnancy-related anxiety and sleep quality showed that women who were more anxious during pregnancy had greater family dysfunction and therefore poorer sleep quality. Conversely, pregnant women with less prenatal maternal anxiety had better family functions and therefore had better sleep quality.
The current study found consistent results with previous studies in which the level of anxiety was associated with good family functions,29–31 and family functions were closely related to the individual’s psychological and physical health.32 The mediating role of family functions on the anxiety profile and sleep quality of prenatal mothers provided new insights into the factors that influence sleep quality. Family functioning factors can be taken into account in clinical treatment to improve maternal sleep quality by improving family functions in women with pregnancy-related anxiety and, consequently, maternal sleep quality.
Although there are many studies on the relationship between psychological status during pregnancy and sleep quality of pregnant women, there are few articles about family function. This study discusses the relationship between pregnancy-related anxiety and sleep quality from the perspective of family function, which provides a new idea for improving the sleep disorder of pregnant women. However, no one is perfect, this study also had some limitations. Firstly, the sample was primarily drawn from an obstetrics clinic at a hospital in northwest China, and it is unclear whether these findings would extend to other ethnic groups. Secondly, this study was a cross-sectional study and it is difficult to determine the causal logic between pregnancy-related anxiety, family functions, and sleep quality among pregnant women; family functions partially mediate the relationship between pregnancy-related anxiety and sleep quality, with other factors affecting pregnancy-related anxiety to be explored subsequently.
Conclusion
Pregnancy-related anxiety is a risk factor for sleep disorders, which means that pregnant women with pregnancy-related anxiety have more serious sleep disorders during pregnancy. Family function plays a mediating role in the influence of pregnancy-related anxiety on sleep quality, especially on the third trimesters. Therefore, during pregnancy, husbands or family members should pay more attention to pregnant women. For example, if pregnant women encounter problems, family members or husbands can help them solve them more, or when pregnant women choose to engage in new activities or development, family members can accept or give support, increase family care, achieve the purpose of improving family functions, and then improve sleep quality. Future research should also investigate and explain the mechanism of the relationship between pregnancy-related anxiety and pregnant women’s sleep quality by influencing family function, because this mechanism may be the key goal of intervention and prevention strategies.
Data Sharing Statement
The data are not publicly available due to privacy and research ethical restrictions.
Statement of Ethics
This study is in line with the Declaration of Helsinki. Ethical approval for the study was obtained from the Ethics Committee of Ningxia Medical University (No. 2022-G007) before the start of the study, and all participants provided written informed consent prior to their study enrolment.
Institutional Review Board Statement
This study was approved by the Research Ethics Committee of Ningxia Medical University. (10 March 2022, #2022-G007).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We thank all the project participants in this study.
Author Contributions
All authors have contributed significantly to the reported work, whether in conceptualization, study design, execution, data acquisition, analysis, and interpretation, or in all of these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by National Natural Science Foundation of China, grant number 82260647, Ningxia Natural Science Foundation Project, grant number 2022AAC02030 and Western Light Talent Program (2022).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Nelson K, Davis J, Corbett C. Sleep quality: an evolutionary concept analysis. Nurs Forum. 2022;57(1):144–151. doi:10.1111/nuf.12659
2. Kloss J, Perlis M, Zamzow J, et al. Sleep, sleep disturbance, and fertility in women. Sleep Med Rev. 2015;22:78–87. doi:10.1016/j.smrv.2014.10.005
3. Sedov I, Cameron E, Madigan S, et al. Sleep quality during pregnancy: a meta-analysis. Sleep Med Rev. 2018;38:168–176. doi:10.1016/j.smrv.2017.06.005
4. Tang Y, Zhang J, Dai F, et al. Poor sleep is associated with higher blood pressure and uterine artery pulsatility index in pregnancy: a prospective cohort study. BJOG. 2021;128(7):1192–1199. doi:10.1111/1471-0528.16591
5. Cai S, Tan S, Gluckman P, et al. Sleep quality and nocturnal sleep duration in pregnancy and risk of gestational diabetes mellitus. Sleep. 2017;40(2):1–8. doi:10.1093/sleep/zsw058
6. Zhong C, Chen R, Zhou X, et al. Poor sleep during early pregnancy increases subsequent risk of gestational diabetes mellitus. Sleep Med. 2018;46:20–25. doi:10.1016/j.sleep.2018.02.014
7. Nakahara K, Michikawa T, Morokuma S, et al. Association of maternal sleep before and during pregnancy with preterm birth and early infant sleep and temperament. Sci Rep. 2020;10(1):11084. doi:10.1038/s41598-020-67852-3
8. Felder J, Baer R, Rand L, et al. Sleep disorder diagnosis during pregnancy and risk of preterm birth. Obstet Gynecol. 2017;130(3):573–581. doi:10.1097/AOG.0000000000002132
9. Li R, Zhang J, Zhou R, et al. Sleep disturbances during pregnancy are associated with cesarean delivery and preterm birth. J Matern Fetal Neonatal Med. 2017;30(6):733–738. doi:10.1080/14767058.2016.1183637
10. Lu QD, Zhang XY, Wang YH, et al. Sleep disturbances during pregnancy and adverse maternal and fetal outcomes: a systematic review and meta-analysis. Sleep Med Rev. 2021;58:101436. doi:10.1016/j.smrv.2021.101436
11. Sanapo L, Hackethal S, Bublitz MH, et al. Maternal sleep disordered breathing and offspring growth outcome: a systematic review and meta-analysis. Sleep Med Rev. 2023;73:101868. doi:10.1016/j.smrv.2023.101868
12. Yang Y, Mao J, Ye ZY, et al. Determinants of sleep quality among pregnant women in China: a cross-sectional survey. J Matern Fetal Neonatal Med. 2018;31(22):2980–2985. doi:10.1080/14767058.2017.1359831
13. Jemere T, Getahun B, Tadele F, et al. Poor sleep quality and its associated factors among pregnant women in Northern Ethiopia, 2020: a cross sectional study. PLoS One. 2021;16(5):e0250985. doi:10.1371/journal.pone.0250985
14. Danilov M, Issany A, Mercado P, et al. Sleep quality and health among pregnant smokers. J Clin Sleep Med. 2022;18(5):1343–1353. doi:10.5664/jcsm.9868
15. Teoh A, Kaur S, Mohd Shukei N, et al. Psychological state during pregnancy is associated with sleep quality: preliminary findings from MY-CARE cohort study. Chronobiol Int. 2021;38(7):959–970. doi:10.1080/07420528.2021.1902338
16. Polo-Kantola P, Aukia L, Karlsson H, et al. Sleep quality during pregnancy: associations with depressive and anxiety symptoms. Acta Obstet Gynecol Scand. 2017;96(2):198–206. doi:10.1111/aogs.13056
17. Rubio E, Levey E, Rondon M, et al. Poor sleep quality and obstructive sleep apnea are associated with maternal mood, and anxiety disorders in pregnancy. Matern Child Health J. 2022;26(7):1540–1548. doi:10.1007/s10995-022-03449-8
18. Israelsson-Skogsberg Å, Persson C, Markstöm A, et al. Children with home mechanical ventilation-Parents’ health-related quality of life, family functioning and sleep. Acta Paediatr. 2020;109(9):1807–1814. doi:10.1111/apa.15177
19. Chang L, Chiang TL; Medicine. Family environment characteristics and sleep duration in children: maternal mental health as a mediator. Soc Sci Med. 2022;314:115450. doi:10.1016/j.socscimed.2022.115450
20. Zhang JL, Hao JH, Tao FB, et al. Analysis of factors influencing pregnancy-related anxiety in early pregnancy. China Public Health. 2011;27(08):969–971.
21. Smilkstein G. The Family APGAR: a proposal for family function test and its use by physicians. J Fam Pract. 1978;6(6):1231–1239.
22. Buysse DJ, Reynolds CF, Monk TH, et al. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
23. Xianchen L, Maoqin T, Lei H, et al. Reliability and validity of Pittsburgh Sleep Quality Index. Chin j psy. 1996;02:103–107.
24. Okun M, Mancuso R, Hobel C, et al. Poor sleep quality increases symptoms of depression and anxiety in postpartum women. J Behav Med. 2018;41(5):703–710. doi:10.1007/s10865-018-9950-7
25. Tsai S, Lee P, Gordon C, et al. Objective sleep efficiency but not subjective sleep quality is associated with longitudinal risk of depression in pregnant women: a prospective observational cohort study. Int J Nurs Stud. 2021;120:103966. doi:10.1016/j.ijnurstu.2021.103966
26. Hung H, Ko S, Chen C. The association between prenatal sleep quality and obstetric outcome. J Nurs Res. 2014;22(3):147–154. doi:10.1097/jnr.0000000000000039
27. Felder J, Laraia B, Coleman-Phox K, et al. Poor sleep quality, psychological distress, and the buffering effect of mindfulness training during pregnancy. Behav Sleep Med. 2018;16(6):611–624. doi:10.1080/15402002.2016.1266488
28. Osnes R, Roaldset J, Follestad T, et al. Insomnia late in pregnancy is associated with perinatal anxiety: a longitudinal cohort study. J Affect Disord. 2019;248:155–165. doi:10.1016/j.jad.2019.01.027
29. Dolz-Del-Castellar B, Oliver J. Relationship between family functioning, differentiation of self and anxiety in Spanish young adults. PLoS One. 2021;16(3):e0246875. doi:10.1371/journal.pone.0246875
30. Kitt E, Lewis K, Galbraith J, et al. Family accommodation in pediatric anxiety: relations with avoidance and self-efficacy. Behav Res Ther. 2022;154:104107. doi:10.1016/j.brat.2022.104107
31. Yen C, Yanc P, Wu Y, et al. The relation between family adversity and social anxiety among adolescents in Taiwan: effects of family function and self-esteem. J Nerv Ment Dis. 2013;201(11):964–970. doi:10.1097/NMD.0000000000000032
32. Shao R, He P, Ling B, et al. Prevalence of depression and anxiety and correlations between depression, anxiety, family functioning, social support and coping styles among Chinese medical students. BMC Psychol. 2020;8(1):38–57. doi:10.1186/s40359-020-00402-8
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.