")
Back to Journals » Nature and Science of Sleep » Volume 15
Sleep Quality is Associated with Axial Length Elongation in Myopic Children Receiving Orthokeratology: A Retrospective Study
Authors Yu D, Wang L, Zhou X , Liu L, Wu S, Tang Q, Zhang X
Received 15 May 2023
Accepted for publication 14 November 2023
Published 29 November 2023 Volume 2023:15 Pages 993—1001
DOI https://doi.org/10.2147/NSS.S421407
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Valentina Alfonsi
Dongyi Yu,1,2,* Libo Wang,2,* Xin Zhou,2,* Lili Liu,2 Shuang Wu,2 Qing Tang,3 Xiaofeng Zhang1
1Department of Ophthalmology, Dushu Lake Hospital Affiliated to Soochow University, Suzhou, 215006, People’s Republic of China; 2Department of Ophthalmology, Kunshan First People’s Hospital Affiliated to Jiangsu University, Suzhou, Jiangsu, 215300, People’s Republic of China; 3Department of Neurology, Kunshan First People’s Hospital Affiliated to Jiangsu University, Suzhou, Jiangsu, 215300, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaofeng Zhang, Email [email protected]
Purpose: To identify potential demographic and lifestyle factors associated with progression of myopia with orthokeratology (ortho-k) treatment via follow-up of axial length (AL).
Methods: In this retrospective observational study, demographics, ocular parameters, near-work distance, outdoor activities, and sleep quality were analyzed in 134 children with myopia aged 8~15 years using ortho-k and a follow-up for one year.
Results: Compared with the slow progression group, the participants in the fast progression group were younger in age (10.55 ± 1.70 years vs 9.90 ± 1.18 years, P = 0.009), demonstrated higher spherical equivalent (SE) value (− 2.52 ± 0.63 diopters (D) vs − 3.05 ± 0.89 D, P < 0.001), shorter near-work distance (P = 0.010), and poorer sleep quality (Pittsburgh sleep quality index [PSQI], 4.79 ± 1.29 vs 3.81 ± 1.38, P < 0.001) in the one-year follow-up. Furthermore, multivariate linear regression analyses showed that baseline age (B =− 0.020, P = 0.020), SE (B = 0.0517, P < 0.001), and total PSQI (B=0.026, P = 0.001) were associated with axial elongation. Advanced logistic regression analyses demonstrated that shorter average near-work distance (P = 0.034), higher SE value (P = 0.023), and poorer sleep quality (P = 0.003) were associated with fast axial elongation.
Conclusion: Sleep quality is one of the key factors associated with axial elongation in children with myopia after using ortho-k for one year. Further studies are required to confirm this observation and expand its practical applications.
Keywords: orthokeratology, myopia, axial length, sleep quality, retrospective study
Introduction
Globally, myopia is one of the most common refractive errors; its prevalence is rapidly increasing1 and is projected to reach approximately 49% by 2050 without effective prevention and control measures.2 The prevalence rate of myopia was particularly high in East and Southeast Asia. Epidemiological studies conducted on high school students in China demonstrated that 90% of students suffer from myopia, posing a significant healthcare burden.3 In 2015, uncorrected myopia caused potential productivity losses worth 24.4 billion USD globally, and the World Health Organization (WHO) has listed myopia among the ten priority diseases in the VISION 2020 campaign.
Myopia had serious impacts in the short and long term. In the short term, myopia leads to poor visual function that affects learning, work, and social interaction.4 In the long term, myopia, especially high myopia, can result in a series of pathological consequences, such as glaucoma, retinal detachment, myopic macular degeneration, choroidal neovascularization, posterior staphyloma, and retinal schisis.5,6 Therefore, controlling the development of myopia will not only improve patients’ refractive status and visual function but also reduce the risk of long-term complications, which will be of remarkable public health value.5
There have been advances in myopia control in clinical practice and clinical trials. Low-dose atropine, optical glasses, orthokeratology (ortho-k), and outdoor activities are widely used methods for preventing and controlling myopia and have proven to be effective.6,7 In addition, red-light therapy and nutrient supplementation have expanded avenues for myopia control.8,9 Compared with other methods, ortho-k has gained popularity due to its noninvasiveness and rapid positive outcomes.10 However, some patients receiving ortho-k treatment demonstrated poor outcomes, and thus, advanced analysis of potential influencing factors is urgently required.
Previous studies have analyzed the efficacy of ortho-k in controlling the progression of myopia. A 2-year follow-up study revealed that corneal biomechanics was associated with axial length (AL) progression in children wearing ortho-k.10 In addition, multiple studies have reported that age, ortho-k wearing time, and baseline refractive error level were correlated with subsequent myopia control and axial elongation in patients wearing ortho-k.11–13 Furthermore, a previous report demonstrated that poor sleep quality was closely related to refractive errors in children and a potential target for myopia progression;14 however, the debate continues on the relationship between sleep quality and the occurrence or development of myopia. Till recently, the potential role of sleep quality on the efficacy of ortho-k treatment remained unclear. The identification of the correlation between sleep quality and axial elongation after ortho-k treatment would provide novel insights for optimizing treatment in this field.
Therefore, this study retrospectively analyzed the ocular parameters, indoor and outdoor work activities, and sleep quality questionnaire to identify factors that affect the efficacy of ortho-k treatment through a 1-year follow-up. Furthermore, we also analyzed the impact of sleep quality on the ability of ortho-k treatment to control myopia progression.
Methods
Study Design
This is a retrospective clinical study conducted at Kunshan First People’s Hospital, Jiangsu Province, China. We collected data from 134 participants from underage patients who received ortho-k treatment from September 2019 to March 2022 and followed-up for one year to observe axial elongation. Although both eyes of the patients were examined, only the data of the right eye were analyzed. Before the ortho-k fitting process, the guardians of the participants were fully informed of the benefits and risks and received education on the proper use of ortho-k, including ortho-k maintenance and care. Refractory examination, ortho-k fitting, questionnaires, and follow-up were conducted by two trained doctors. This study was conducted in accordance with the Declaration of Helsinki, and the study protocol was approved by the Ethics Committee of Kunshan First People’s Hospital, Jiangsu Province, China before initiation (approval number:2019-06–007-K01). We obtained informed consent from the patients and their respective guardians.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) patients in the age range of 8–15 years; (2) those diagnosed with myopia, with a myopic spherical degree of equivalent in the range of −1.00–−6.00 diopters (D) and astigmatism degree <−1.50 D; (3) those willing to receive ortho-k treatment for 12 months; and (4) those able to complete questionnaire surveys and follow-up studies.
The exclusion criteria were as follows: (1) patients with significant strabismus or amblyopia; (2) those with ocular or systemic diseases that prevented them from adhering to ortho-k treatment, such as severe allergic conjunctivitis; (3) those who accepted other methods of therapeutic management for myopia; (4) those with complications, such as severe corneal epithelial damage and keratitis after ortho-k treatment; (5) those with chronic diseases, tumors, or injuries that will hamper the follow-up process; and (6) those patients and guardians unwilling to cooperate with the study.
Ortho-k Type and Design
The ortho-k lenses (Euclid Systems, USA) were fitted using standardized criteria. After completing the refractory examination and evaluating the ocular health, corneal morphology, lens parameters, and ortho-k lens fitting, the appropriate ortho-k was selected. Follow-up visits were appropriately arranged, and routine examinations of uncorrected visual acuity and the anterior segment were performed before ortho-k and after 1 and 7 days. Thereafter, a monthly visit was conducted for all the patients.
Ocular Examinations
All optometric tests were performed after three parallel administrations of 0.5% tropicamide (Santen Pharmaceutical Co., Ltd.) at 5-minute intervals. The spherical equivalent (SE) was calculated using the formula: SE = sphere power + ½ cylindrical power. Three independent measurements were conducted, and the mean value was used for further analysis.
Ocular AL was measured using the IOL-Master anterior segment analyzer (Haag-Strei, Switzerland) before and after one year of ortho-k treatment. Five independent measurements were obtained, and the mean value was used for subsequent analysis. The signal-to-noise ratio of a single AL measurement was >2.0, and the combined signal-to-noise ratio was >32.
Corneal surface parameters were measured using the Oculus Pentacam system based on corneal topography (Oculus, Wetzlar, Germany). The corneal topography parameters were determined using flat keratometry (Kf) and steep keratometry (Ks), and the difference between Kf and Ks (ΔK) was calculated. The corneal eccentricity was determined by constructing a difference map using the corneal tangential maps obtained before and after 3 months of wearing ortho-k lenses., as reported previously.15,16 In addition, central corneal thickness (CCT), anterior chamber depth, and pupil diameter were also measured.
Follow-Up
Monthly follow-ups were conducted for patients who wore ortho-k, and slit-lamp microscopy was performed to detect any complications from wearing ortho-k that could have caused discomfort. The last follow-up time was conducted at 12 months, and AL was measured using the IOL-Master. The AL in the follow-up duration was corrected for the decreased CCT with the following formula: ALfollow-up =ALfollow-up + (CCTbaseline − CCTfollow−up).17
Sleep Questionnaire
The Pittsburgh sleep quality index (PSQI) is a self-reported questionnaire for evaluating sleep quality in patients with sleep or psychiatric disorders, as well as for assessing sleep quality in the general population.18 In this study, the subjective sleep quality, latency, duration, efficiency, and disturbances; hypnotic medication; and daytime dysfunction were analyzed. A total score ≥6 indicates poor sleep quality.14 None of the patients used hypnotic medication, and thus, this parameter was excluded from further analysis.
Other Questionnaires
Participants’ near-work distance and outdoor physical activity were recorded through questionnaires. The information on average near-work distance, average near-work duration, and average outdoor time per day were recorded, graded, and assigned values. Based on the average near-work distance recorded per day, the patients were divided into three groups: <33 cm, score 1; 33–40 cm, score 2, and >40 cm, score 3. Based on the average near-work duration per day the patients were divided into three groups: >5 h, score 1; 2–5 h, score 2, and <2 h, score 3. Based on average outdoor time per day, patients were divided into four groups: <30 min, score 1; 30–60 min, score 2; 61–120 min, score 3, and >120 min, score 4.
Statistical Analysis
GraphPad Prism 8 statistical software (San Diego, California, USA) was used for statistical analysis. Categorical data were expressed as counts and percentages, and intergroup differences were analyzed by chi-square test. Continuous data were expressed as mean ±standard deviation (SD), and differences between two groups were analyzed by independent sample t-test. Pearson correlation coefficient was used to analyze the correlation between changes in AL after one year of wearing ortho-k lenses. The fast progression group was defined as AL elongation exceeding 0.19 mm, and both multiple linear regression and logistic regression analyses were used to identify the factors associated with changes in AL and AL fast progression after one year of wearing ortho-k lenses. A p-value of <0.05 was considered statistically significant.
Results
Basic Information of the Study
In this study, initially, a total of 207 patients with myopia were retrospectively screened. After excluding 43 patients who fulfilled the exclusion criteria, the eye examination and questionnaire results of 164 patients were used for further analysis. After one-year of follow-up, a total of 134 patients were finally included in the analysis after excluding 30 patients (Figure 1).
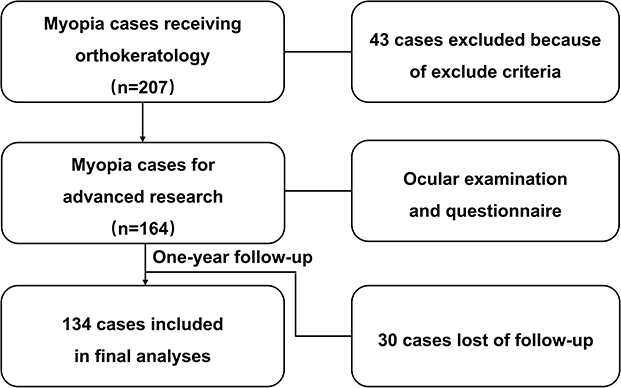 |
Figure 1 Schematic plot showing the possible factors contributing to the progression of myopia with ortho-k treatment. |
Baseline Characteristics of Participants in Different Axial Lengthening Groups
Based on the comparison of AL and corrected AL after one year of wearing ortho-k, 134 participants were divided into slow progression group (< 0.2 mm, n = 62) and fast progression group (≥ 0.2 mm, n = 72). Compared with the slow progression group, the fast progression group had participants who were of younger age (10.55 ±1.70 vs 9.90 ±1.18, P = 0.009), demonstrated higher SE value (−2.52 ±0.63 vs −3.05 ±0.89, P < 0.001), higher near-work distance rate (P = 0.010), and poorer sleep quality (PSQI, 4.79 ±1.29 vs 3.81 ±1.38, P < 0.001). No differences in gender, eye examination results, and outdoor activity time were observed between the two groups (Table 1).
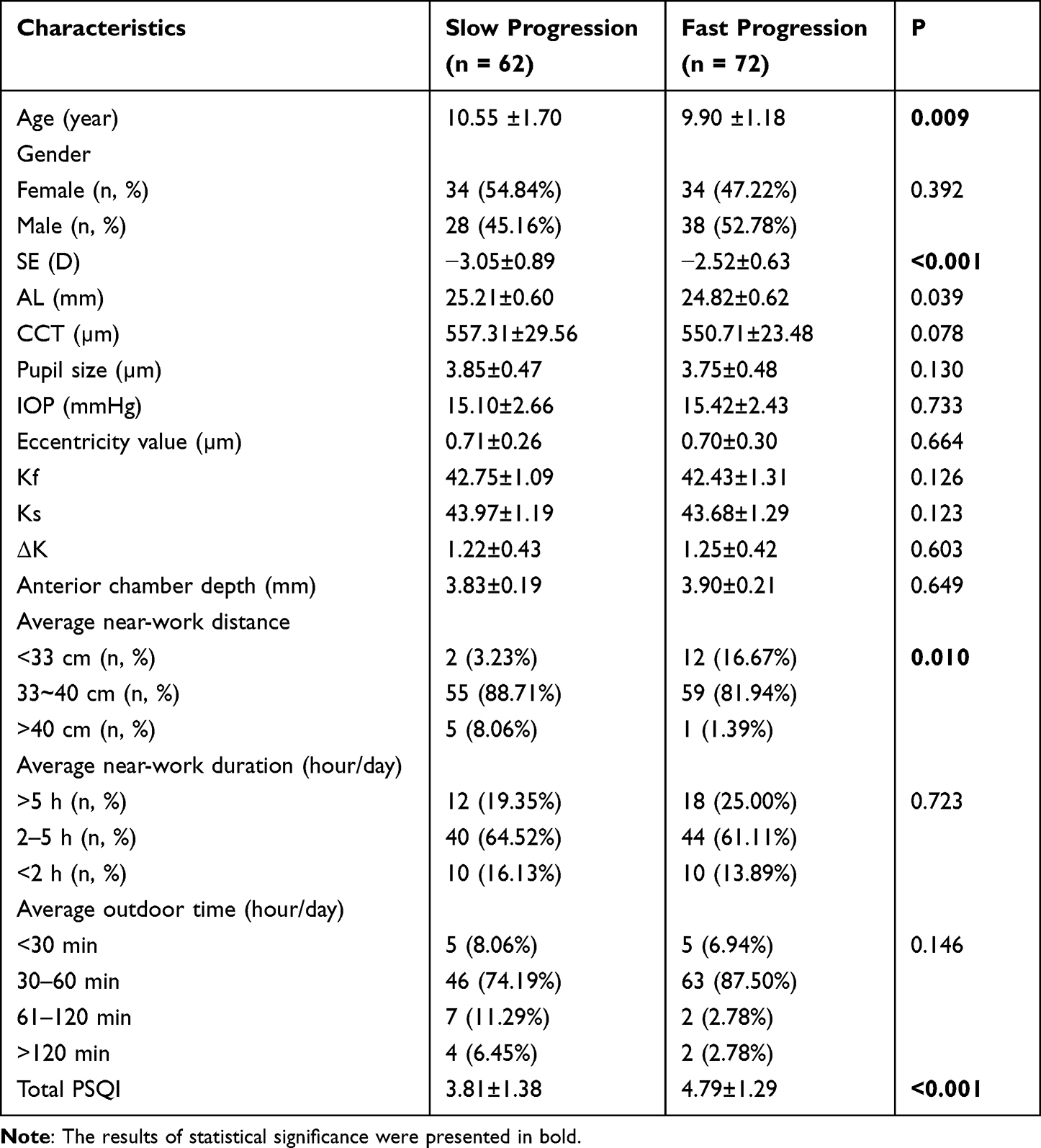 |
Table 1 Comparisons of the Baseline Demographics Characteristics and Ocular Biometric Parameters Between Slow and Fast Progressions |
Potential Factors Related to AL Elongation
As the intergroup differences using the chi-square test showed that age, SE, average near-work distance/day and PSQI had statistically significant differences between the slow progression and the fast progression groups, we further analyzed the correlation between each factor and changes in AL. Pearson correlation analysis showed that increased age (R = −0.448, P < 0.001) and average near-work distance (R = −0.250, P = 0.004) were negatively correlated with AL change, whereas SE and total PSQI were positively correlated with AL change (R = 0.513, P < 0.001 and R = 0.417, P < 0.001, respectively), demonstrating that the four factors were associated with AL changes (Figure 2).
Furthermore, multiple linear regression analysis was used to explore whether age, SE, average near-work distance, and PSQI could be independent risk factors for AL elongation after one year of ortho-k treatment. The results showed that age at the beginning of wearing ortho-k lenses, baseline SE value, and total PSQI value were significantly associated with AL change (P < 0.05, Table 2).
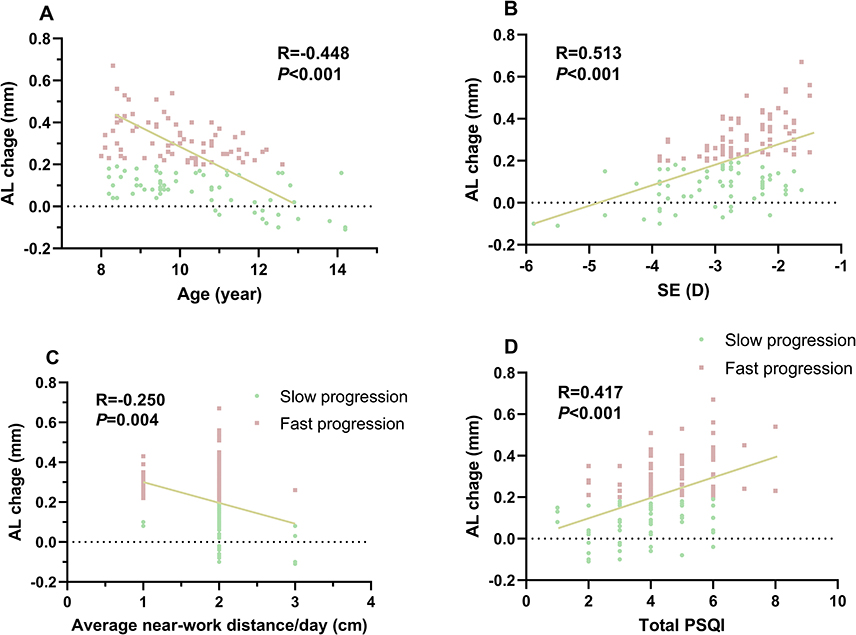 |
Figure 2 Simple linear regression analysis between AL change and (A) baseline age, (B) baseline SE, (C) average near-work distance per day and (D) total PSQI. Trend lines are fitted using binary linear regression (yellow–green lines). Abbreviations: D, diopter; PSQI, Pittsburgh Sleep Quality Index; AL, axial length; SE, spherical equivalent. |
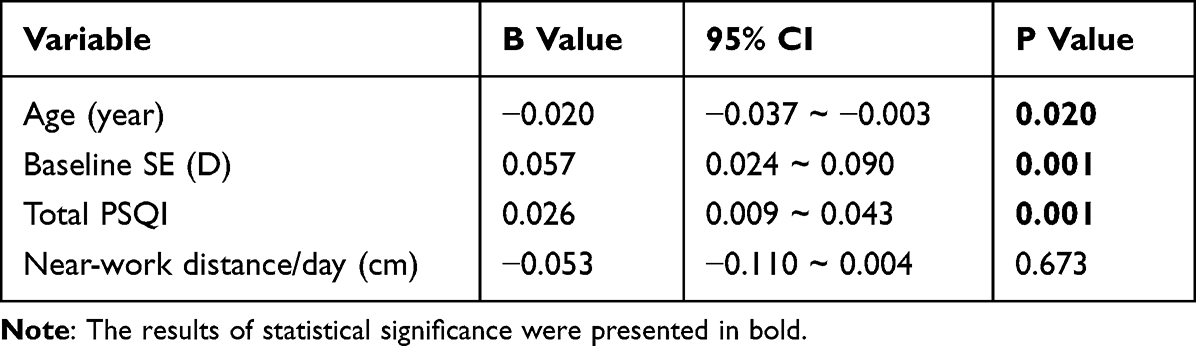 |
Table 2 Multivariable Regression Analysis Showing the Strength of the Factors Related with Axial Length Growth |
Identification of Factors Related to Abnormally Fast AL Progression Incidence
Multivariate logistic regression analysis was performed to detect the effects of age, SE value, near-work distance per day and total PSQI on abnormally fast AL progression. The results showed that factors related to fast axial elongation included lower baseline SE (P = 0.023), average near-work distance per day (P = 0.034) and total PSQI (P = 0.003). No statistical differences were observed in baseline age (P = 0.902, Table 3).
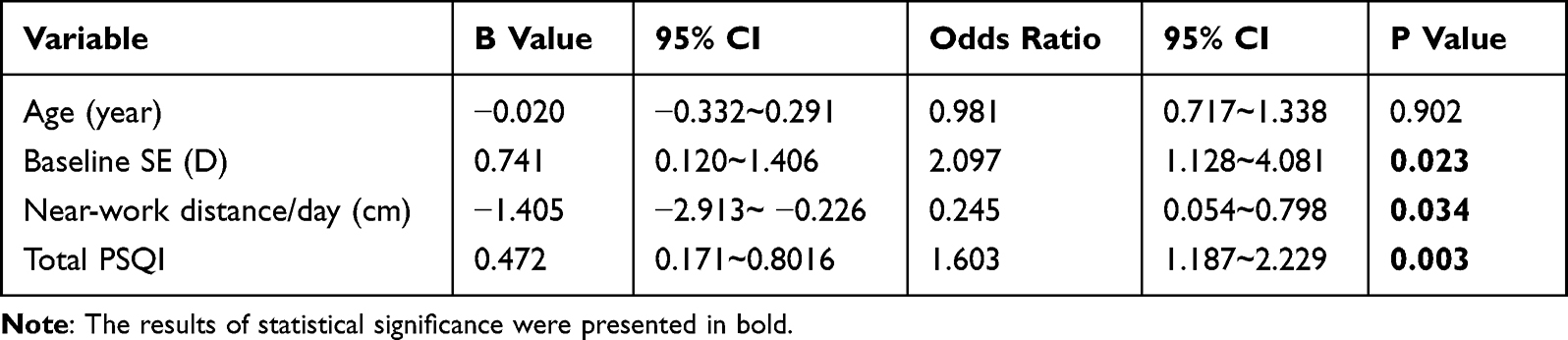 |
Table 3 Multivariable Regression Analysis Showing the Strength of the Factors Related with Fast Axial Elongation Incidence |
Sleep Quality of Participants in Different AL Progression Groups
As sleep quality was identified as a key factor affecting the extent of AL changes and abnormal AL elongation, we considered the specific indicators of sleep quality in different AL progression groups. As shown in Table 4, the analysis of the PSQI subscale showed that sleep latency and daytime dysfunction were poorer in the fast progression group (P = 0.031 and P = 0.002, respectively). In addition, total PSQI was poorer in the fast progression group (P < 0.001). Furthermore, using total PSQI ≥6 as an indicator of poor sleep quality, the sleep quality of the two groups of children was analyzed. The results showed that poor sleep quality was significantly more common in the fast progression group (P = 0.025).
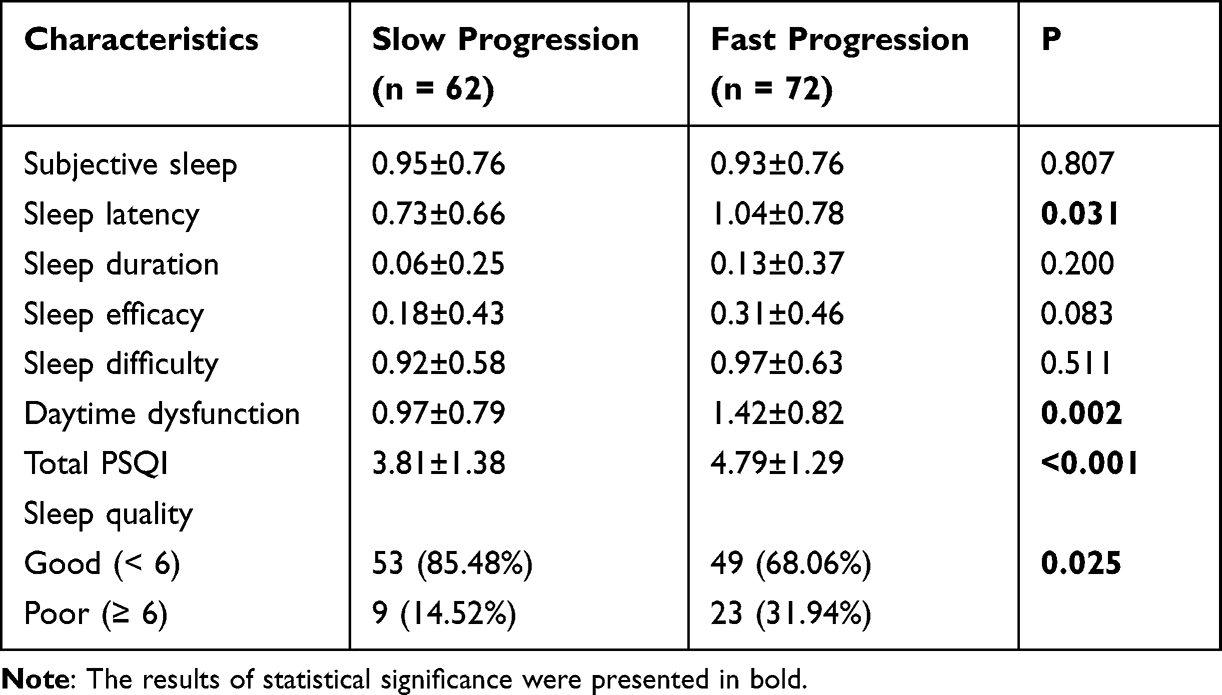 |
Table 4 Subscales of PSQI in Slow and Fast Progression Groups of the Myopia Cases |
Discussion
Ortho-k has been widely used in the management of myopia and regarded as one of the most effective treatments for controlling myopia. Although their efficacy is well-established, their ability to control myopia progression is influenced by various factors. The results of this study show that baseline age, baseline SE, near-work distance, and sleep quality are related to the AL elongation after ortho-k treatment. Furthermore, sleep quality was an independent risk factor for AL change and abnormal fast AL progression, which warrants further investigation.
Several previous studies have analyzed the factors related with ortho-k efficacy in controlling myopia progression. The most common factors are age and baseline SE, with studies from China and Japan suggesting that older age and higher baseline SE are protective factors.19–21 The increase in age and SE in patients with myopia is a key process that is closely related to AL elongation, which could cause a decrease in the potential for AL growth, thus slowing the progression of myopia. In addition, higher SE is closely related to longer AL and steeper corneas, which can lead to better corneal reshaping effects and control myopia progression.22 Therefore, our study is in agreement with several previous studies, providing consistent evidence that age and baseline SE play a role in the effectiveness of ortho-k in controlling AL lengthening.
In addition, we also investigated the relationship between near-work distance, near-work duration, outdoor activity time, and AL lengthening in patients with myopia undergoing ortho-k treatment. Our study found that only near-work distance was related to AL fast progression. Patients receiving ortho-k treatment should be informed of the importance of maintaining healthy and reasonable eye usage during treatment. However, a prospective study by Chen et al revealed that daily near-work of ≤5 h was associated with better control of myopia during a 2-year ortho-k treatment period.23 Numerous studies have focused on the role of outdoor activity in myopia prevention and control. A cluster randomized trial of primary school students in Guangzhou, China, showed that 40 min of outdoor activity time at school decreased myopia incidence in the following 3 years.24 Consistent with our study, a machine-learning based model found no correlation between outdoor activity and the effectiveness of ortho-k treatment.24 Our study only stratified near-work and outdoor activities, and thus, more well-designed and detailed studies are needed in the future.
As AL elongation was a normal process in children, a one-year AL change of >0.2 mm was considered as fast AL progression, a value used in several previous studies.25,26 Through multiple regression analyses, age, SE, and PSQI were associated with AL change, whereas baseline SE, near-work distance per day, and PSQI were related to fast AL progression incidence. There were several inconsistencies in AL change and abnormal AL progression in this study; thus, more information was obtained. Age and near-work distance per day were different in these two fields; thus, they might demonstrate differentiated functions. Baseline young age was associated with a faster AL change, and it can be explained by the role of age in physiological AL lengthening. Additionally, near-work distance per day was related to abnormal AL progression and highlighted its role in pathological AL progression. In this study, baseline SE and PSQI were associated with both AL lengthening and abnormal fast AL progression. As baseline SE had been reported to be related to the effects of ortho-k treatment,27,28 more advanced analyses were conducted on sleep quality.
Notably, our study found that poor sleep quality was related to AL elongation and abnormally fast AL progression after ortho-k treatment. Baseline sleep quality was related to both AL change and AL fast progression, and further analysis showed that sleep latency and daytime dysfunction were more severe in the AL fast progression group. Previous studies from China and Japan revealed that poor sleep quality was related to an increased incidence of myopia;14,29 thus, sleep quality demonstrated a potential risk factor for myopia incidence. An epidemiological study on multiple ethnic groups in Xinjiang revealed that longer sleep time was associated with lower myopia incidence;30 however, several other studies do not support this observation. For example, a cross-sectional study in Singapore found that sleep quality, duration, timing, as well as specific sleep factors were not independently associated with myopia, SE, or AL.31 Furthermore, the longitudinal Raine Study did not support the hypothesis of a relationship between sleep behavior and myopia.32 However, our study did not focus on the relationship between sleep quality and myopia incidence but rather on its impact on the effectiveness of ortho-k treatment, providing novel insights in this field.
Sleep quality is a key factor affecting circadian rhythm and melatonin levels.33,34 Recent studies suggest that prolonged exposure to LED light may induce myopia by disrupting the retinal circadian rhythm, which may also be associated with sleep quality. In addition, sleep quality may cause decreased melatonin levels, and melatonin is a potential myopia control drug and endogenous regulatory factor in subsequent myopia development.35 We focused on the relationship between sleep quality and ortho-k treatment for myopia. Ortho-k treatment is performed during sleep, and its effect on sleep quality should be considered. Sleep quality itself affects myopia development through multiple potential pathways, which should be explored in future research.
This study had several limitations. First, this study had a retrospective design with a short follow-up time. Prospective cohort study with a larger number of participants and longer follow-ups are needed to validate the results obtained in this study. Second, only baseline sleep quality was considered, and changes in sleep quality during follow-up were not obtained, which should be a parameter included in future analyses. Third, the combination of ortho-k treatment with other myopia control methods, including atropine treatment, should be simultaneously performed. Considering the limitations, caution should be exercised in treatment decision-making.
Conclusions
In conclusion, our results suggest that the effectiveness of ortho-k in controlling myopia is influenced by patient age, baseline SE, near-work distance, and sleep quality. Sleep quality is one of the key factors related with AL elongation and abnormal AL progression incidence one year after ortho-k treatment. This study highlights the impact of sleep quality on the treatment of myopia with ortho-k, and further research is needed to confirm our observations and expand its practical application.
Acknowledgment
This work was supported by the Suzhou Science and Technology Development Plan (No. SYSD2019025). The language used in this study has been professionally edited by ExEditing.com.
Disclosure
The authors declare no competing interests in this work.
References
1. Modjtahedi BS, Abbott RL, Fong DS, Lum F, D.Tan M. task force on, reducing the global burden of myopia by delaying the onset of myopia and reducing myopic progression in children: the academy’s task force on myopia. Ophthalmol. 2021;128(6):816–826.
2. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmol. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
3. Jiang D, Shi B, Gao H, Guo Y, Zhou S, Zhang Y. Associations between reading and writing postures and myopia among school students in Ningbo, China. Front Pub Health. 2022;10:713377. doi:10.3389/fpubh.2022.713377
4. Philipp D, Vogel M, Brandt M, et al. The relationship between myopia and near work, time outdoors and socioeconomic status in children and adolescents. BMC Pub Health. 2022;22(1):2058. doi:10.1186/s12889-022-14377-1
5. Bullimore MA, Ritchey ER, Shah S, Leveziel N, Bourne RRA, Flitcroft DI. the risks and benefits of myopia control. Ophthalmol. 2021;128(11):1561–1579. doi:10.1016/j.ophtha.2021.04.032
6. Wang CY, Hsu NW, Yang YC, Chen YL, Shyong MP, Tsai DC. Premyopia at preschool age: population-based evidence of prevalence and risk factors from a serial survey in Taiwan. Ophthalmol. 2022;129(8):880–889. doi:10.1016/j.ophtha.2022.03.017
7. Walline JJ, Lindsley KB, Vedula SS, et al. Interventions to slow progression of myopia in children. Cochrane Database Syst Rev. 2020;1(1):CD004916. doi:10.1002/14651858.CD004916.pub4
8. Pan M, Zhao F, Xie B, et al. Dietary omega-3 polyunsaturated fatty acids are protective for myopia. Proc Natl Acad Sci U S A. 2021;118(43). doi:10.1073/pnas.2104689118
9. Dong J, Zhu Z, Xu H, He M. Myopia control effect of repeated low-level red-light therapy in Chinese children: a randomized, double-blind, controlled clinical trial. Ophthalmol. 2023;130(2):198–204. doi:10.1016/j.ophtha.2022.08.024
10. Xiang K, Chen J, Zhao W, et al. Changes of corneal biomechanics in children using orthokeratology and their roles in predicting axial length progression-A prospective 2-year study. Acta Ophthalmol. 2023;101(7):755–765. doi:10.1111/aos.15662
11. Guo X, Xie PY. Effection of tear film stability on orthokeratology. Zhonghua Yan Ke Za Zhi. 2023;59(3):237–241. doi:10.3760/cma.j.cn112142-20221017-00517
12. Tang T, Li X, Chen S, et al. Long-term follow-up of changes in ocular biometric parameters in orthokeratology lens wearers with relatively large-scale axial length reduction. Eye Vis. 2023;10(1):6. doi:10.1186/s40662-022-00324-z
13. Lin W, Li N, Lu K, Li Z, Zhuo X, Wei R. The relationship between baseline axial length and axial elongation in myopic children undergoing orthokeratology. Ophthalmic Physiol Opt. 2023;43(1):122–131. doi:10.1111/opo.13070
14. He J, Lin YY, Chen J, et al. Association of sleep quality with myopia based on different genetic risk levels. Int J Ophthalmol. 2022;15(10):1657–1664. doi:10.18240/ijo.2022.10.14
15. Chu M, Zhao Y, Hu P, Chen D, Yu Y, Ni H. Is orthokeratology treatment zone decentration effective and safe in controlling myopic progression? Eye Cont Lens. 2023;49(4):147–151. doi:10.1097/ICL.0000000000000981
16. Chen MF, Liu XT, Zhang F, Wang YL, Mao XJ. The influencing factors and the effect of myopia control in children treated with orthokeratology. Zhonghua Yan Ke Za Zhi. 2022;58(4):259–264. doi:10.3760/cma.j.cn112142-20210801-00360
17. Jakobsen TM, Sondergaard AP, Moller F. Peripheral refraction, relative peripheral refraction, and axial growth: 18-month data from the randomised study-clinical study of near-sightedness; treatment with orthokeratology lenses (CONTROL study). Acta Ophthalmol. 2023;101(1):e69–e80. doi:10.1111/aos.15217
18. de Feijter M, Kocevska D, Ikram MA, Luik AI. The bidirectional association of 24-h activity rhythms and sleep with depressive symptoms in middle-aged and elderly persons. Psychol Med. 2023;53(4):1418–1425. doi:10.1017/S003329172100297X
19. Wang B, Naidu RK, Qu X. Factors related to axial length elongation and myopia progression in orthokeratology practice. PLoS One. 2017;12(4):e0175913. doi:10.1371/journal.pone.0175913
20. Fang J, Zheng Y, Mou H, Shi M, Yu W, Du C. Machine learning for predicting the treatment effect of orthokeratology in children. Front Pediatr. 2022;10:1057863. doi:10.3389/fped.2022.1057863
21. Nakamura Y, Hieda O, Yokota I, Teramukai S, Sotozono C, Kinoshita S. Comparison of myopia progression between children wearing three types of orthokeratology lenses and children wearing single-vision spectacles. Jpn J Ophthalmol. 2021;65(5):632–643. doi:10.1007/s10384-021-00854-4
22. Chen Z, Xue F, Zhou J, et al. Prediction of orthokeratology lens decentration with corneal elevation. Optom Vis Sci. 2017;94(9):903–907. doi:10.1097/OPX.0000000000001109
23. Chen X, Xiong Y, Liu F, Wang J, Yang B, Liu L. Factors determining the myopia control effect of an orthokeratology lens: a two-year multi-level model. Ophthalmic Physiol Opt. 2022;42(4):786–796. doi:10.1111/opo.12990
24. He M, Xiang F, Zeng Y, et al. Effect of time spent outdoors at school on the development of myopia among children in China: a randomized clinical trial. JAMA. 2015;314(11):1142–1148. doi:10.1001/jama.2015.10803
25. Li X, Hu J, Peng Z, et al. Association between choriocapillaris perfusion and axial elongation in children using defocus incorporated multiple segments (DIMS) spectacle lenses. Eye. 2023. doi:10.1038/s41433-023-02629-2
26. Chang LC, Sun CC, Liao LL. Orthokeratology compliance, digital device use, and myopia control among children with myopia during COVID-19 home confinement in Taiwan. IN J Ophthalmol. 2023;71(3):962–966. doi:10.4103/ijo.IJO_1384_22
27. Wang Z, Meng Y, Wang Z, et al. Crystalline lens thickness change is associated with axial length elongation and myopia progression in orthokeratology. Cont Lens Anterior Eye. 2022;45(4):101534. doi:10.1016/j.clae.2021.101534
28. Zhao W, Wang J, Chen J, et al. The rate of orthokeratology lens use and associated factors in 33,280 children and adolescents with myopia: a cross-sectional study from Shanghai. Eye. 2023;37(15):3263–3270. doi:10.1038/s41433-023-02503-1
29. Ayaki M, Torii H, Tsubota K, Negishi K. Decreased sleep quality in high myopia children. Sci Rep. 2016;6(1):33902. doi:10.1038/srep33902
30. Shi Y, Ma D, Li X, et al. Ethnic disparities in risk factors for myopia among Han and minority schoolchildren in Shawan, Xinjiang, China. Optom Vis Sci. 2023;100(1):82–90. doi:10.1097/OPX.0000000000001949
31. Li M, Tan CS, Xu L, et al. Sleep patterns and myopia among school-aged children in Singapore. Front Pub Health. 2022;10:828298. doi:10.3389/fpubh.2022.828298
32. Stafford-Bell N, McVeigh J, Lingham G, et al. Associations of 12-year sleep behaviour trajectories from childhood to adolescence with myopia and ocular biometry during young adulthood. Ophthalmic Physiol Opt. 2022;42(1):19–27. doi:10.1111/opo.12905
33. Baranwal N, Yu PK, Siegel NS. Sleep physiology, pathophysiology, and sleep hygiene. Prog Cardiovasc Dis. 2023;77:59–69. doi:10.1016/j.pcad.2023.02.005
34. Chakraborty R, Micic G, Thorley L, et al. Myopia, or near-sightedness, is associated with delayed melatonin circadian timing and lower melatonin output in young adult humans. Sleep. 2021;44(3). doi:10.1093/sleep/zsaa208
35. Yu H, Wang Q, Wu W, Zeng W, Feng Y. Therapeutic effects of melatonin on ocular diseases: knowledge map and perspective. Front Pharmacol. 2021;12:721869. doi:10.3389/fphar.2021.721869
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.