")
Back to Journals » Nature and Science of Sleep » Volume 15
Sleep Duration and Insomnia with Comorbid Depression and Anxiety Symptoms in Chinese Adults: A Cross-Sectional Study
Authors Hou Z, Chen Y, Sun Y, Song C, Deng H, Cheng N, Han X, Zhang J, Wang Q , Li Y , Yin J , Meng Q
Received 16 September 2023
Accepted for publication 13 December 2023
Published 21 December 2023 Volume 2023:15 Pages 1079—1091
DOI https://doi.org/10.2147/NSS.S440584
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Zhongxin Hou,1,* Yang Chen,1,2,* Yunrui Sun,1 Chongwei Song,1 Haoyuan Deng,3 Nan Cheng,4 Xiaoyu Han,2 Jianghui Zhang,5 Qian Wang,1 Yi Li,1 Jianzhong Yin,1,6 Qiong Meng1
1School of Public Health, Kunming Medical University, Kunming, Yunnan, People’s Republic of China; 2Institute for Acute Communicable Disease Prevention and Control, Yunnan Provincial Center for Disease Control and Prevention, Kunming, Yunnan, People’s Republic of China; 3Medical Department, The First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, People’s Republic of China; 4Department of Hospital Infection, Wuhan Mental Health Center, Wuhan, Hubei, People’s Republic of China; 5AIDS Care Center, Yunnan Provincial Hospital of Infectious Disease, Anning, Yunnan, People’s Republic of China; 6Baoshan College of Traditional Chinese Medicine, Baoshan, Yunnan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiong Meng, School of Public Health, Kunming Medical University, 1168 West Chunrong Road, Yuhua Avenue, Chenggong District, Kunming, Yunnan, 650500, People’s Republic of China, Tel +8615559789771, Email [email protected] Jianzhong Yin, Baoshan College of Traditional Chinese Medicine, Baoshan Longyang District Qingyang District Vocational Education Park, Baoshan, Yunnan, 678000, People’s Republic of China, Tel +8613987645337, Email [email protected]
Purpose: Depression and anxiety are two highly prevalent mental disorders that commonly coexist. However, little is known about the association between sleep and comorbid depressive and anxiety symptoms (CDAS). Therefore, this study aims to explore the relationship between sleep duration, insomnia and CDAS.
Methods: This is a cross-sectional study of 22,004 community adults who participated in the China Multi-Ethnic Cohort (CMEC) study. Chinese version of Patient Health Questionnaire-2 and Generalized Anxiety Disorder-2 were used to screen CDAS in community adults. A positive score on each scale was considered indicative of CDAS. All participants received face-to-face interviews, medical examinations, and biochemical examinations to assess sleep duration and insomnia and collect covariates. The self-reported sleep duration was divided into three groups: < 7 hr, 7– 9 hr and > 9 hr groups. Logistic regression was used to analyze the association between sleep duration, insomnia and CDAS. A restricted cubic spline (RCS) was used to explore the dose–response relationship between sleep duration and CDAS. Stratified analysis based on gender and age was conducted.
Results: Overall, 2.8% (95% CI 2.6%~3.0%) of participants reported having CDAS. After adjusting the potential covariates, sleep duration < 7 hr (OR=1.635, 95% CI=1.335~2.004) was significantly associated with CDAS, compared with sleep 7– 9 hr. After RCS analysis, there was a nonlinear relationship between sleep duration and CDAS. The increase in the number of types of insomnia, the greater the likelihood of CDAS (p for trend< 0.05). In sensitivity analysis, it was found that the results were consistent with those of the main analysis. After stratification by gender and age, the association between sleep duration and CDAS was only observed in female and young and middle-aged adults, not in men and older adults.
Conclusion: Both insufficient sleep duration and insomnia are associated with a higher prevalence of CDAS in Chinese adults.
Keywords: sleep duration1, insomnia2, comorbid depressive and anxiety symptoms3, adults4, cross-sectional study5
Introduction
Sleep plays an important role in maintaining body functions such as consciousness, cognitive function, maintenance of biological rhythms, repair functions and stress relief.1 Poor sleep behavior is associated with many diseases. As far as current research is concerned, sleep related studies have explored two main aspects of sleep duration and sleep disorders. Some studies have shown that sleep had a great impact on the development of chronic disease. For example, people with poor sleeping conditions have a higher prevalence of hypertension and a greater risk of death.2,3 Likewise, sleep duration also affects human health, with some asserting that too long or too short sleep duration can increase the risk of developing diabetes.4,5
As sleep conditions are associated with the development of a wide range of disorders, it is necessary to consider whether sleep has an impact on mental health. Depression and anxiety are both significant mental health disorders, and the increasing number of individuals suffering from anxiety or depression has garnered considerable attention from academics. Currently, there are some studies being conducted to explore the association between sleep and anxiety or depression. For example, some studies with older people in the community suggested that short sleep duration is significantly associated with an increased likelihood of developing depression and relapse.6 Additionally, certain studies7 have shown an u-shaped association between sleep duration and depressive symptoms among older individuals, while others have concluded that there is no relationship in older women.8,9 At the same time, since sleep disorders are often used as one of the important indicators to evaluate sleep quality, at the same time, insomnia is a manifestation type of sleep disorders. Some researchers have focused on the association between insomnia and depressive symptoms. For instance, a study suggested a strong association between insomnia and depression in women individuals.10 Some studies also considered sleep disorders as significant predictors of the onset or recurrence of depression11–13(Whether insomnia, as a type of sleep disorder, also has this relationship is a question worth exploring). Most of these studies have been conducted in areas with relatively developed economies. It should be acknowledged that varying levels of economic development can lead to inconsistencies, which can influence the likelihood of developing various psychological problems. Furthermore, previous studies primarily focused on older individuals with small sample sizes. However, it is important to note that adults under the age of 60 face significant stressors and are more susceptible to experiencing depression and anxiety disorders. Most importantly, previous studies examined the association between sleep and anxiety or depression separately. Currently, there are no reports on the association between sleep and comorbid depressive and anxiety symptoms (CDAS). Anxiety and depression may initially have distinctive features. However, as they are present for an extended period of time, often depression will combine with anxiety episodes. Some studies have found that the combination of the two is often associated with a higher risk of death compared to anxiety or depression alone and that co-morbid conditions are more harmful.14 Understanding the prevalence of CDAS in community population and exploring the association between sleep and CDAS is of practical significance. Therefore, this study aims to understand the prevalence of CDAS and to explore the impact of sleep duration and insomnia on CDAS in adult residents in relatively undeveloped areas of China using baseline data from the Yunnan region of the Chinese Multi-Ethnic Cohort (CMEC), as well as evaluate whether there is difference in this association between older adults and non-elderly young and middle-aged adults.
Materials and Methods
Study Design and Participants
All participants signed informed consent before data collection and this study was approved by Kunming Medical University Medical Ethical Review Board (KMMU2020MEC078). The baseline survey of the CMEC study was conducted from May 2018 to September 2019. Previous studies on CMEC have been described in great detail.15 The data for this study were primarily based on the Yunnan of the CMEC. A multi-stage stratified cluster sampling method was used to obtain samples from community populations in Yunnan Province in this study. In the first stage, four minority communities (Yongsheng County, Heqing County, Yongren County, and Wuding County) were selected as the study sites on the basis of the need to establish natural population cohorts in different places where ethnic minorities gather. Yongsheng County has a total population of 336,832, with 65.07% Han Chinese. Heqing County has a total population of 243,031, with the Bai ethnic group accounting for 59% of the total population. Wuding County has a total population of 236,500, with Yi accounting for 32.08%. Yongren County has 58,573 Yi, accounting for 55.5% of the total population. In the second stage, two to eight communities were selected in each settlement (depending on the size of the community), taking into account the migrant status and local health conditions. In the final stage, all participants who met our inclusion criteria were invited to participate in our study, taking into account the gender ratio and age ratio, estimating a population response rate of 60% (60–90% in rural areas and 40–60% in urban areas). Persons who met the following two conditions: (a)who were between the ages of 30–79 years old (b) who had lived in the above-mentioned four counties of Yunnan Province were selected as the participants. A total of 23,143 community residents were engaged, and then we excluded those who had no information about sleep, anxiety and depression symptom-related indicators survey (204 participants), those who have missing values on the relevant covariates (935 participants) and people with only anxiety or only depressive symptoms were excluded (n=1056). Finally, a total of 20,948 participants were included in this study. The response rate was 95.07%. The detailed process is shown in Figure 1. Power analysis revealed a power level of 1.00 (Z=1.95, α=0.05) in the present study (total sample size=22,004). The study was based on a standardized survey methodology and a variety of rigorous quality control measures.
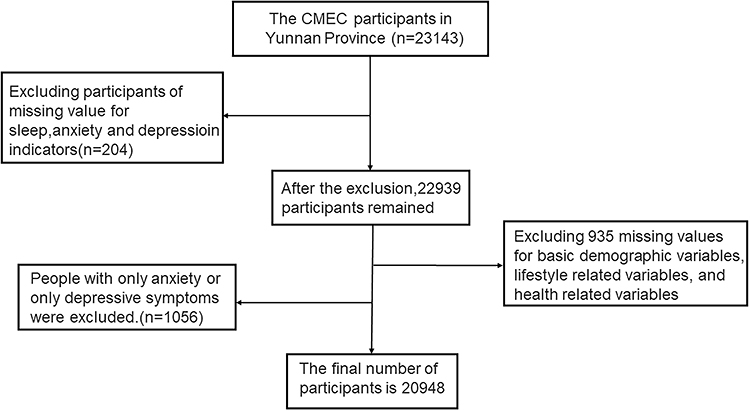 |
Figure 1 Flow diagram of selection of participant (based on CMEC study). |
Data Collection
The face-to-face interviews were conducted using a self-developed questionnaire through an information collection application that had additional logical check and recording functions. The collected information in the questionnaire included demographic variables (such as ethnicity, age, gender, occupations, household income, marital status, educational level), lifestyle habits (such as smoking, alcohol drinking, physical activity), body mass index (BMI), sleep duration, and insomnia. The entire interview was carried out by trained interviewers who were medical staff from local health facilities or medical students from local universities and were particularly familiar with the minority languages spoken in the area.15 The participants all underwent physical examination and laboratory tests on site after the survey. These included measurements of height, weight, blood pressure, heart rate, as well as blood and urine tests. Blood samples were collected from all subjects after an overnight fasting for routine blood tests, fasting blood glucose levels, glycosylated haemoglobin levels, lipid levels and biochemical indexes of hepatic function tests. All medical examinations were conducted by trained medical postgraduates following standard operating procedures.16
Identify of Comorbid Depressive and Anxiety Symptoms (CDAS)
A comprehensive assessment of mental status was conducted for all participants based on two screening questionnaires from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), using the Chinese version of the 2-item Patient Health Questionnaire (PHQ-2) and the 2-item Generalized Anxiety Disorder Scale (GAD-2). The two screening scales improve the efficiency of monitoring depressive symptoms and anxiety symptoms in large population-based epidemiological surveys, and studies have shown good reliability and validity of PHQ-2 in screening for depressive disorders and GAD-2 in screening for anxiety.14 The PHQ-2 contains two items that are asked in questionnaire form: “how often they have been uninterested in doing things in the past two weeks”; “how often they have felt depressed, frustrated or hopeless in the past two weeks” 17 The GAD-2 contains two items: “how often you have felt nervous, anxious or irritable in the past two weeks” and “how often you have not been able to stop or control your worry in the past two weeks”. Each item corresponds to four different levels of response: “not at all”, “a few days”, “more than half of the days” and “almost every day”, which were assigned scores of “0, 1, 2 and 3”, respectively. The total score is calculated by summing up the item scores. Both scales have a total score ranging from 0 to 6. When PHQ-2 and GAD-2 were used to screen for depressive symptoms and anxiety symptoms, a cut-off point of 3 points was employed for positive diagnosis.14,18,19 In this study, a positive score on each scale was considered indicative of CDAS. A healthy reference group was defined as residents who neither had CADS nor exhibited symptoms of anxiety or depression.
Assessment of Sleep Duration
The sleep duration was obtained from the self-reports of participants. We calculated P25 and P75 for the sleep duration of participants, which were 7 hr and 9 hr, respectively. Additionally, these values had been used as a cut-off point in many epidemiological studies6,20,21 conducted in the Chinese population. Therefore, the self-reported sleep duration was divided into three groups: <7 hr, 7~9 hr and >9 hr groups. Participants who slept <7 hr were considered short sleepers, while those who slept >9 hr were considered long sleepers, the optimal sleep duration of 7~9 hr was considered the reference group.
Assessment of Insomnia
The sleep disorder conditions in this study were derived from a questionnaire. Three types of insomnia were identified, and participants answered “yes or no” to of the following questions; ①the disorders of initiation and maintenance (DIMS) was identified if participants answered “Yes” to the question “Do you need more than half an hour to fall asleep at least three days a week?”; ②the Early Morning Waking Disorder (EMA) was identified if participants answered “Yes” to the question “Do you wake up early in the morning at least three days a week and are unable to fall back asleep?”;③ the Daytime Dysfunction (DDF) was identified if participants answered “Yes” to the question “Do you have difficulty sleeping at least three days a week and have difficulty staying awake during the day while working, eating or talking to others?”22,23 The number of types of insomnia present for each participant was accumulated and further graded into a hierarchy of scores according to the number of reported insomnia: 0 for none of the above types of insomnia, 1 for any one type, 2 for any two types, 3 for all three types.
Assessment of Covariates
Most covariates in this study were obtained through survey using questionnaires, while a few were obtained through physical examinations and laboratory testing, such as BMI, blood glucose, blood pressure, and so on.
Firstly, the basic demographic variables include ethnic, age (young and middle-aged adults aged 30~64 years old, older adults aged ≥65 years old), gender, occupation, household income, marital status (married, divorced, widowed, never married), and educational level (not attending school, primary school, junior high school, senior high school, college, university and above).
Secondly, lifestyle-related variables mainly include smoking, alcohol consumption and physical activity. Smoking was measured by asking about the current smoking status and categorized as never smoked, currently smoking and quit (quit was defined as having stopped smoking for 6 months or more). Alcohol consumption was also assessed using the questions “How often did you consume alcohol in the past year” and “On average, how many days per week did you consume alcohol on average in the past year”. The final level of alcohol consumption was categorized as almost never, occasional, 1–2 days/week, 3–5 days/week, and daily.17 Regarding physical activity, it could be classified as occupational physical activity, transportation physical activity, leisure-time physical activity, and domestic physical activity. The sum of these four categories was used as the total daily physical activity and metabolic equivalents (METs) for assessing exercise intensity.17 In this study, we divided it into three groups based on their tertiles. Additionally, we investigated sleep snoring and the presence or absence of napping habits.
Finally, the health-related variables included BMI (thin if BMI <18.5 kg/m2, normal if BMI 18.5~23.9 kg/m2, overweight if BMI 24.0~27.9 kg/m2, obese if BMI ≥28.0 kg/m2) and a history of diseases such as hypertension, diabetes and other chronic diseases (stroke, asthma, coronary artery disease). Hypertension was diagnosed if three or more blood pressure measurements on different days showed a systolic blood pressure ≥140 mmHg and/or a diastolic blood pressure ≥90 mmHg, along with self-reported hypertension.24 Diabetes was diagnosed based on a questionnaire asking for a history of diabetes combined with biochemical indicators. It met one of the following criteria: fasting blood glucose ≥7.0 mmol/L, self-reported history of diabetes, history of taking hypoglycaemic drugs, glycosylated hemoglobin ≥6.5%.17
Statistical Analyses
Categorical variables were expressed as frequencies and percentages, while continuous variables were expressed as means and standard deviations. Chi-square test and univariate logistic analysis were conducted to identify statistically significant covariates, followed by multifactorial logistic regression models to analyze the association between sleep duration, insomnia and CDAS, respectively. The covariates were adjusted hierarchically and divided into three levels, that is to say, three models were constructed. In Model 1, no adjustments were made. In Model 2, we adjusted for basic demographic variables (ethnic, age, gender, occupation, household income, marital status, education level) and lifestyle-related variables that showed statistical significance in the univariate analysis. In Model 3, we further adjusted for health-related variables that demonstrated statistical significance in the univariate analysis based on Model 2. Additionally, a trend analysis was performed to examine the association between sleep disturbance and CDAS. Since gender and age are important confounders, stratified analyses were carried out by different genders and age groups. The young and middle-aged adults group consists of participants aged 30–64 years old, while the older adults group includes participants aged ≥65 years old based on the World Health Organization’s definition, which considers 65 years as the threshold for being considered elderly. The dose–response relationship between sleep duration and CDAS was modeled using restricted cubic splines (RCS) with four selected nodes for this study, also adjusted for the covariates included in Model 3. A hypothesis test of the non-linear relationship (p for nonlinear <0.05) was conducted. To validate the stability of the study, we performed sensitivity analyses by conducting multifactorial logistic regression after excluding participants with a history of sleeping pill use (649 participants were excluded). We considered that some participants who had taken sleeping pills in the past may have influenced the results of this study. All analyses were conducted using SPSS 27.0, R4.1.3 and Excel 2009 software. A two-tailed test of p<0.05 was used.
Results
The characteristics of the research population are recorded in Table 1 and Table S1. The mean age of the study participants was 52.88 ± 10.42 years. Of the total participants 6988 (33.3%) were male and 13,960 (66.7%) were female. Han, Yi and Bai accounted for 45.7%, 26.6% and 27.7%, respectively. 63.8% of them had a junior high school education or below. 67.4% of participants were agricultural workers. 24.2% of participants slept <7 hours and 25.0% of participants slept >9 hours. 36.7% of participants had insomnia. In the total population, 2.8% (95% CI 2.6%~3.0%) individuals had CDAS.
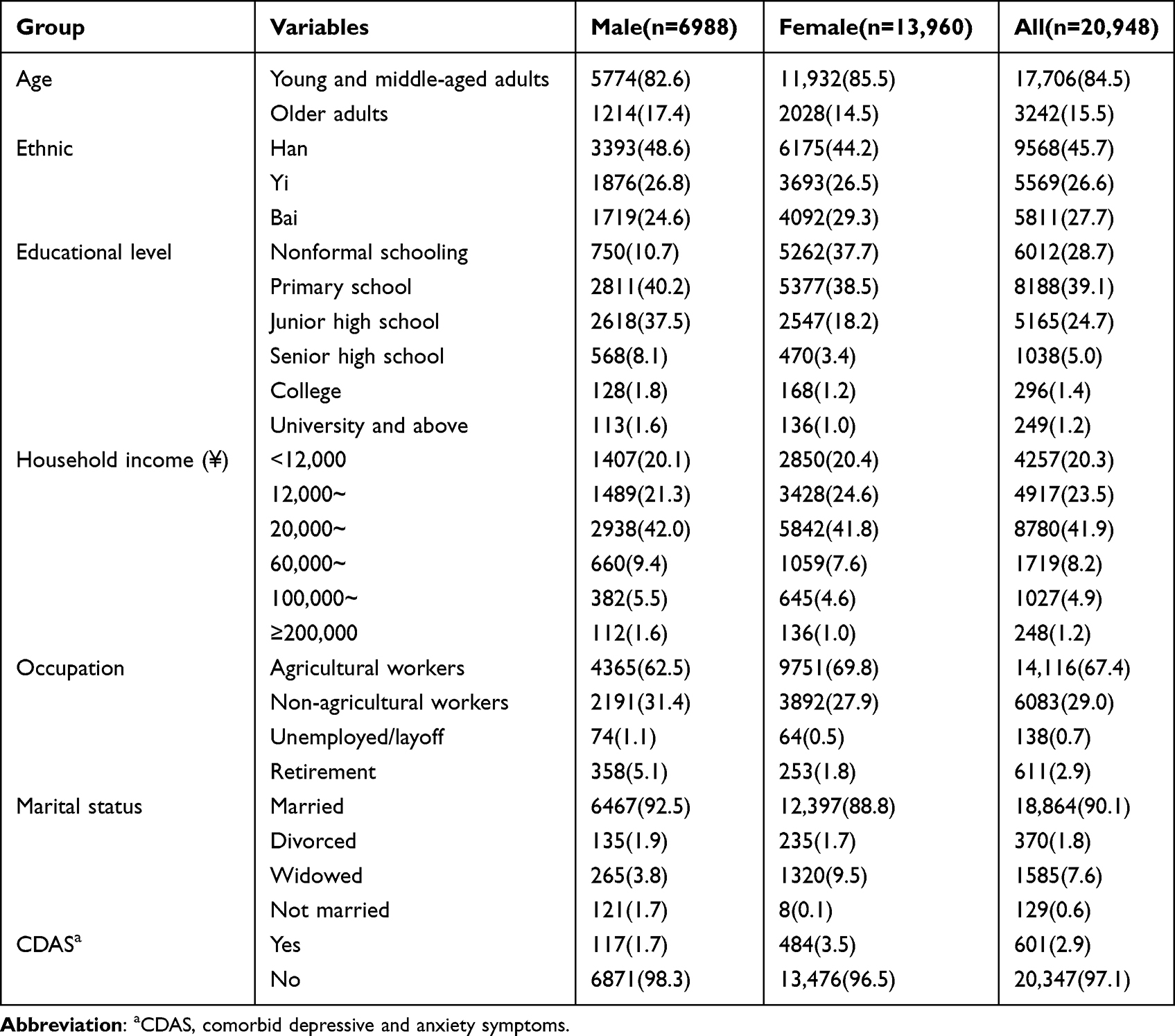 |
Table 1 Description of Demographic Characteristics of the Study Population [n (%)] |
The prevalence of CDAS was 3.0% in older adults and 2.9% in young and middle-aged adults (X2=0.117, p=0.733). The prevalence of CDAS was significantly higher in females than in males (3.5% vs 1.7%, X2=53.709, p<0.001). The prevalence of CDAS was different among residents with different educational level, annual household income, ethnic, occupation, marital status (p<0.05) (Table 2). In addition, univariate logistic regression showed that the factors associated with CDAS included alcohol consumption, smoking, METs, asthma, coronary heart disease, stroke, sleep duration and number of insomnia types (see Table S2).
 |
Table 2 Comparison of Prevalence of CDAS Among Residents with Different Demographic Characteristics [n (%)] |
The above significant variables were included in the multivariate logistic regression analysis model, and the results showed that sleep duration was an independent influencing factor of CDAS. We then sequentially adjusted for participants’ basic demographic variables, lifestyle-related variables, and health-related variables, and found that only too short sleep duration was associated with an increased risk of CDAS. The results in model 3 indicated that the likelihood of CDAS when sleeping <7 hr and >9 hr were higher by a factor of 0.635 (OR=1.635, 95% CI=1.335~2.004) and 0.182 (OR=1.182, 95% CI=0.946~1.478), respectively, compared to sleeping for 7~9 hr (Table 3). Results of association between sleep duration, insomnia and CDAS after adjusting for covariates in Model 3 is visually presented in Figure 2. After stratifying analysis for different genders, we only found that a significant correlation between sleeping <7 hr and CDAS appeared in women, and no correlation was found in men. After stratifying by age, we also found that there was a significant correlation between sleeping <7 hr and CDAS only appeared in young and middle-aged adults. However, it has not been found in older adults (Table 3).
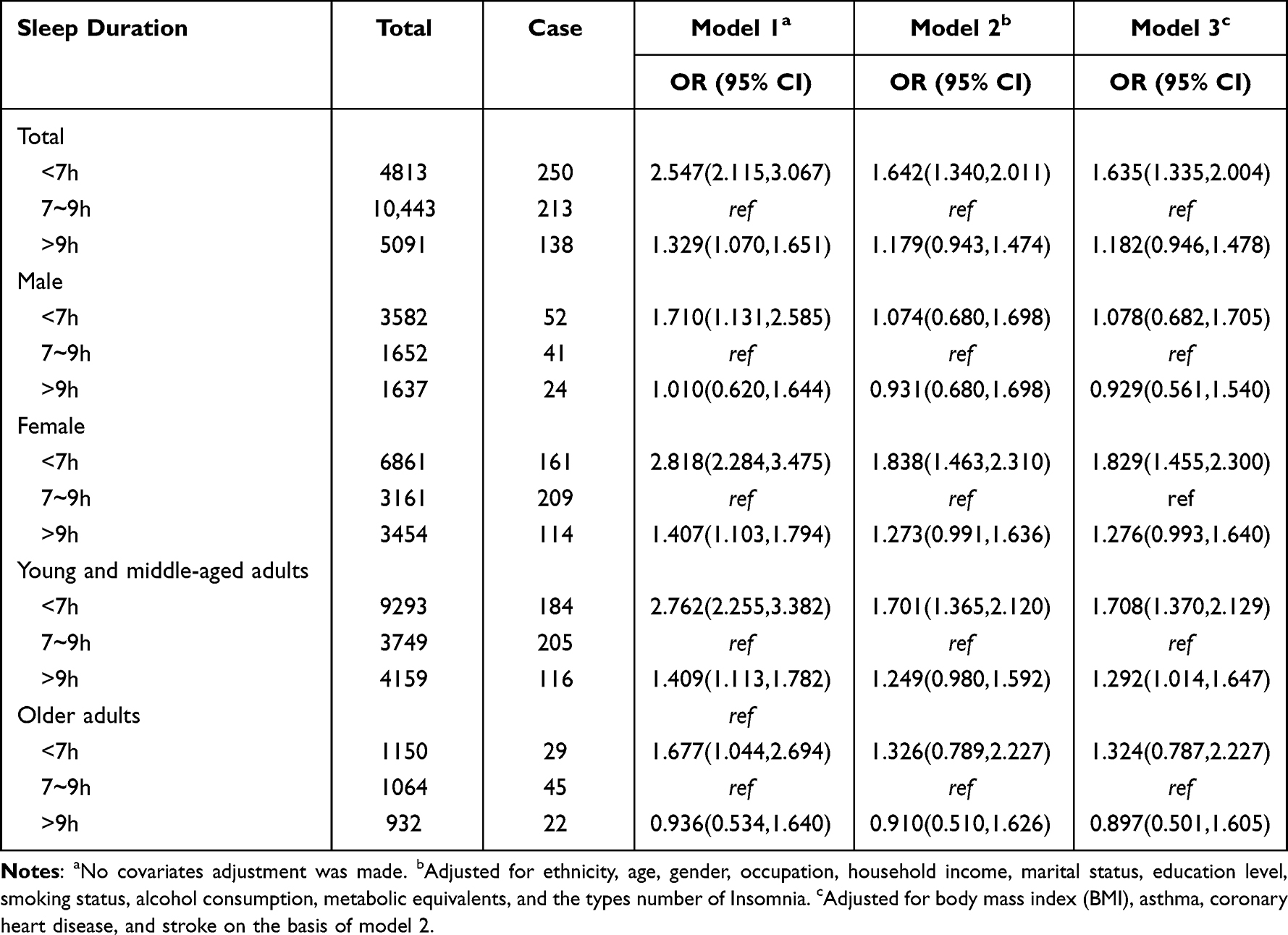 |
Table 3 Association Between Sleep Duration and Comorbid Depressive and Anxiety Symptoms (No-Stratified Analyses and Stratified Analyses) |
 |
Figure 2 The association between sleep duration, insomnia and CDAS after adjusting for covariates in Model 3. Model 3: Adjusted for ethnicity, age, gender, body mass index (BMI), previous occupation, household income, marital status, education level, smoking status, alcohol consumption, metabolic equivalents, asthma, coronary heart disease, stroke and Sleep duration/ The number of Insomnia types. |
A significant non-linear ”U” shaped relationship between sleep duration and CDAS could be observed in Figure 3 (p for nonlinearity <0.001) either with or without adjustment of covariates. A negative correlation between sleep duration and the likelihood of CADS was observed when sleep duration was <5.96 (hr/d). After stratifying analysis for different genders, the results of RCS with adjustment of covariates showed that there was the “U” shaped relationship between sleep duration and CDAS in female (p for nonlinearity <0.001), but not in male (p for nonlinearity=0.46), with a different inflection point (8.03 hr) (Figure S1). “U” shaped relationship between sleep duration and CDAS was observed among young and middle-aged adults (p for nonlinearity <0.001), but not in older adults (p for nonlinearity=0.11), by the RCS stratified by different ages, with a different inflection point (7.98 hr) (Figure S2).
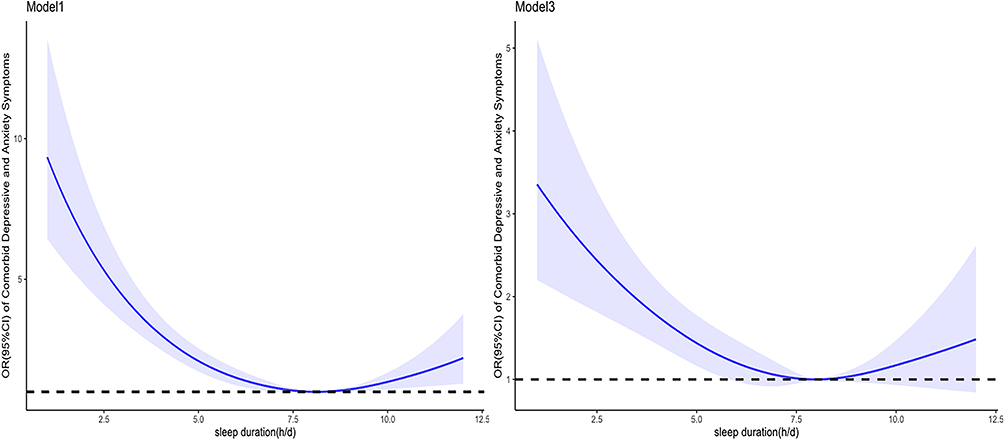 |
Figure 3 Dose-response relationship between sleep duration and CDAS (Model 1 and Model 3). Model 1: no adjustment. Model 3: Adjusted for ethnicity, age, gender, body mass index (BMI), previous occupation, household income, marital status, education level, smoking status, alcohol consumption, metabolic equivalents, asthma, coronary heart disease, stroke and the number of Insomnia types. The OR is shown with the blue solid line, and 95% CIs are shown with the shaded area. The black horizontal short dashed line represents the reference line y=1. |
The relationship between insomnia and CDAS is shown in Table 4. In the fully adjusted model 3, compared to participants without insomnia, participants with a higher number of insomnia types were more strongly associated with CDAS with ORs of 1.834 (95% CI: 1.381 ~2.437), 3.024 (95% CI: 2.405 ~ 3.801) and 5.113 (95% CI: 4.058 to 6.442). The association with developing CDAS increased with the number of insomnia types with multifactorial adjustment (p<0.001 for trend test). The visual presentation by model 3 is shown in Figure 2.
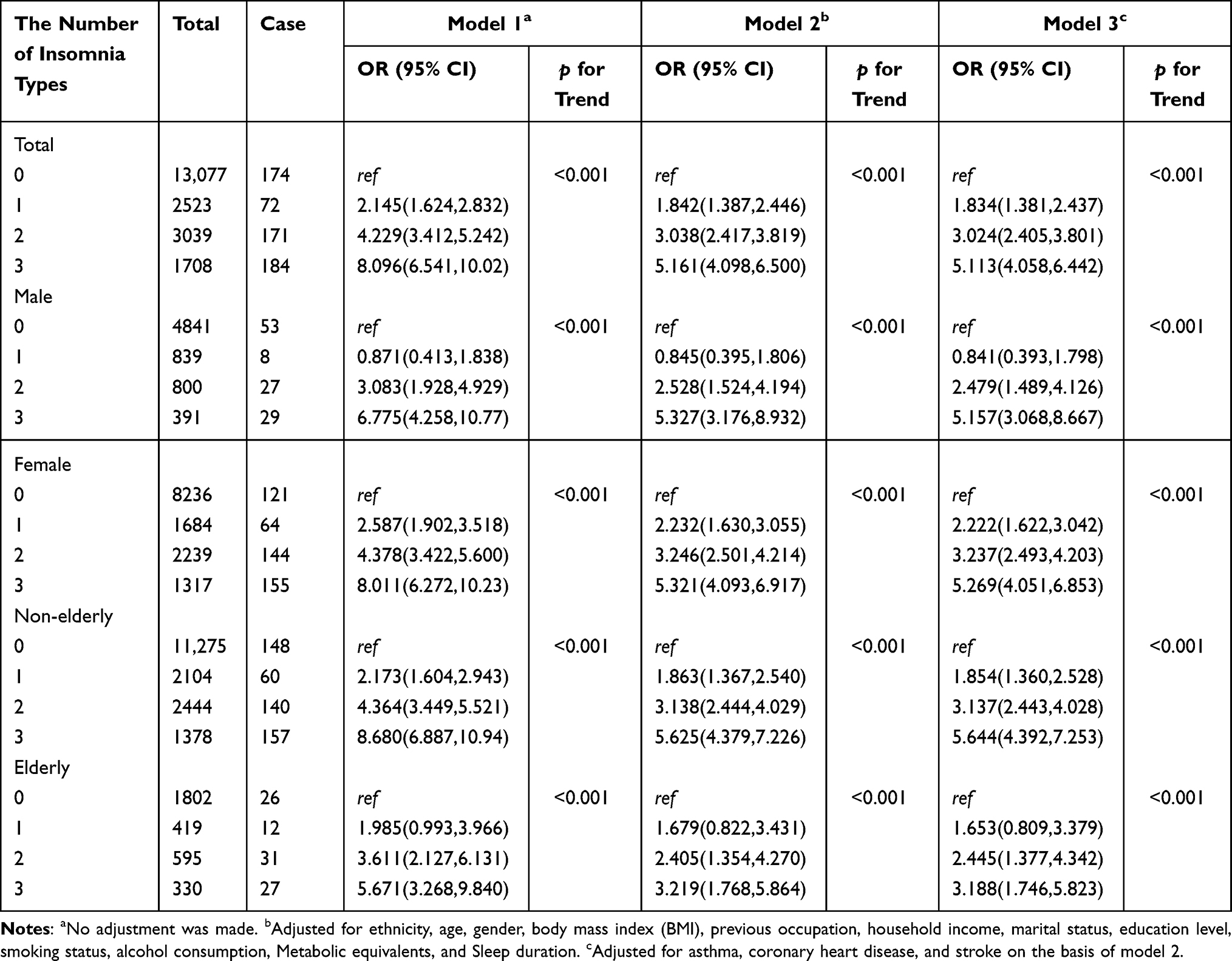 |
Table 4 Association Between Insomnia and Comorbid Depressive and Anxiety Symptoms |
After stratifying analyses for different genders and different ages, we found that this positive trend association between insomnia and CDAS both appeared in women and men, as well as in older adults and young and middle-aged adults (see Table 4 for details).
In a sensitivity analysis, after excluding those participants with a history of sleeping pills use, it was found that the association with CDAS was 1.596 times (OR=1.596, 95% CI=1.289, 1.975) and 1.171 times (OR=1.171, 95% CI=0.929, 1.476) greater for those who slept <7 hr and >9 hr, respectively, compared to those who slept 7~9 hr. In addition, compared to those without insomnia, participants with different numbers of insomnia types had 1.865, 2.397 and 4.898 times greater association with developing CDAS, respectively. The association with developing CDAS as a degree of insomnia increased (all p < 0.01). And these results were consistent with those of the main analyses, and the details can be seen (Table S3 and Table S4). After excluding those participants with a history of sleeping pills use, the results of RCS adjusted covariates still showed a “U” shaped relationship between sleep duration and CDAS with an inflection point at 7.97 hr of sleep duration (p for nonlinearity <0.001), as detailed (Figure S3).
Discussion
Our study found that insomnia was independently and significantly associated with the prevalence of CDAS. This association was observed consistently across gender and age groups. Sleep duration exhibited a nonlinear relationship with the risk of CDAS. However, when stratified by gender and age, this association was only observed in women and young and middle-aged adults, not in men and older adults.
In this study, we found that the prevalence of CDAS was 2.8% (95% CI 2.6%~3.0%) individuals had CDAS. In addition, the prevalence of CDAS in men was lower than that in women in rural communities, which may be the reason why many previous studies only focused on females.8,9 No significant statistical differences were found between different age groups and CDAS. Considering that the reason for this situation in this study may be that the study area is a relatively underdeveloped and remote area, where there is often a lack of education related to mental health and intentional failure to report due to feeling ashamed in older people.14,25,26
First, in multivariate logistic analysis, when normal sleep duration (7–9 hr) was used as the reference group, only short sleep duration (<7 hr) was associated with CDAS and not found in the participants who have long sleep duration (>9 hr). The RCS showed a “U” curve relationship. In sleep duration less than 5.69 hr, the shorter the sleep duration, the more likely to have CDAS. The results of this study are still similar to some articles.27,28 Compared to grouping sleep duration, RCS analysis can utilize continuous data, bridge breakpoints and discontinuities in the data and provide smooth curve fitting. The results of RCS analysis precisely confirm this. A possible reason for the nonlinear relationship between sleep time and CDAS is that circadian rhythm disorder caused by insufficient sleep in the human body may lead to changes in hormone levels, which may contribute to the development of CDAS.
Because previous studies mostly focus on the elderly and women, even though this study did not find significant differences in the prevalence rate of CDAS among different age groups in the univariate analysis, this study still stratified the age and gender and explored again. The results of the stratified analysis by gender and age group showed no association between sleep duration and CDAS in men. Similarly, no association was found in the >65 years age group. This suggests that the association between sleep duration and CDAS may differ by gender and age. This finding is similar to that of another study of Chinese community residents.29 This may be caused by different sleep conditions, work schedule and hormonal secretion at different ages, and different social pressures and physiological structures at different genders.
This study also found an association between insomnia and CDAS and that insomnia may be a risk factor for CDAS. And as people who have more types of insomnia, the association with a higher likelihood of CDAS. Likewise, after stratified analysis by age and gender, a significant association was found between insomnia and CDAS, either by gender or by age group, and this finding was again consistent with the main analysis. The association between insomnia and CDAS may be linked to inflammation. Some researchers believe that sleep disorders may directly enhance emotional sensitivity to cytokines or increase levels of inflammatory cytokines such as C-reactive protein and interleukin-6 in the body. These inflammatory factors also enhance neural sensitivity, ultimately increasing the occurrence of depression or anxiety.30,31 Good sleep can help improve levels of melatonin, a multifunctional regulatory molecule that can alleviate anxiety symptoms.32
Considering that some participants with a history of taking sleeping pills may have influenced the results of this study, sensitivity analyses after excluding participants with a history of sleeping pills were conducted, and the results were found to be consistent with the main analysis and have good robustness.
This study showed that sleep has a correlation with CDAS. Furthermore, both experiencing insomnia symptoms and having insufficient sleep duration can have unfavorable effects on individuals’ psychological well-being. Therefore, interventions targeting the population’s sleep conditions may contribute to maintaining their mental health.
The strengths of this study were the large sample of community adults and the data was obtained from the CMEC, which was a multi-ethnic cohort design and had good representativeness and strict quality control. Exploration of the more damaging CDAS, rather than focusing on a single anxiety or depression. The statistical methodology is richer, with varying degrees of adjustment for confounding factors. Stratified analysis was conducted for different ages and genders. Sensitivity analyses were also conducted using participants excluding a history of sleeping pills to verify the stability of the results, and dose–response relationships were conducted using restricted cubic splines. On the other hand, there are also some shortcomings in our study. Firstly, due to the specific nature of the PHQ-2 and GAD-2, they cannot be used to diagnose anxiety and depression, but only to screen anxiety and depression symptoms. Secondly, there may also be confounding factors that were not accounted for in this study, such as: the dietary habits of certain refreshing drinks such as coffee, cola, sleep latency and other important sleep-related information. They might have some impact on the outcome. Thirdly, this study is a cross-sectional study, which cannot establish causal relationships but can only provide etiological clues. Finally, sleep duration is only self-reported by participants, but self-reported sleep duration has been shown to be a reliable predictor of mortality and other health outcomes.29 In the future, we will further refine the aforementioned shortcomings and aim to validate them through cohort studies that can provide stronger evidence of causality. Additionally, there is a need for further research into the underlying biological mechanisms linking sleep and anxiety and depressive symptoms.
Conclusion
The prevalence of CDAS was higher in women than in men. After adjusting for covariates, there is a nonlinear relationship between sleep duration and CDAS. When the sleep duration was less than 5.96 (hr/d), a negative correlation between sleep duration and the likelihood of CADS was observed. As more types of insomnia increased, the association with a higher prevalence of CDAS in the population increased. A significant correlation between sleep duration and CDAS appeared in women and young and middle-aged adults, but not in men and older adults.
Data Sharing Statement
Some or all datasets generated during and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This research received ethical approval from Kunming Medical University Medical Ethical Review Board (KMMU2020MEC078). All of the participants signed an informed consent prior to participating.
Acknowledgments
We gratefully acknowledge the staff of various health institutions in Yunnan Province and the undergraduates of Kunming Medical University, who conducted the site survey. We are grateful to all survey respondents for their participation in this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the National Natural Science Foundation of China (No. 81960617) and Yunnan Applied Basic Research Projects-Kunming Medical University Union Foundation (No. 202001AY070001-182). The study funder had no influence on the study design, collection, management, analysis, and interpretation of data, writing of the report, or decision to submit the report for publication.
Disclosure
The authors declare no conflict of interest in this work.
References
1. Dinges DF, Douglas SD, Hamarman S, Zaugg L, Kapoor S. Sleep deprivation and human immune function. Adv Neuroimmunol. 1995;5(2):97–110. doi:10.1016/0960-5428(95)00002-j
2. Wu W, Wang W, Gu Y, et al. Sleep quality, sleep duration, and their association with hypertension prevalence among low-income oldest-old in a rural area of China: a population-based study. J Psychosom Res. 2019;127:109848. doi:10.1016/j.jpsychores.2019.109848
3. Kojima M, Wakai K, Kawamura T, et al. Sleep patterns and total mortality: a 12-year follow-up study in Japan. J Epidemiol. 2000;10(2):87–93. doi:10.2188/jea.10.87
4. Hublin C, Partinen M, Koskenvuo M, Kaprio J. Sleep and mortality: a population-based 22-year follow-up study. Sleep. 2007;30(10):1245–1253. doi:10.1093/sleep/30.10.1245
5. Gottlieb DJ, Punjabi NM, Newman AB, et al. Association of sleep time with diabetes mellitus and impaired glucose tolerance. Arch Intern Med. 2005;165(8):863–867. doi:10.1001/archinte.165.8.863
6. Sun Y, Shi L, Bao Y, Sun Y, Shi J, Lu L. The bidirectional relationship between sleep duration and depression in community-dwelling middle-aged and elderly individuals: evidence from a longitudinal study. Sleep Med. 2018;52:221–229. doi:10.1016/j.sleep.2018.03.011
7. Yokoyama E, Kaneita Y, Saito Y, et al. Association between depression and insomnia subtypes: a longitudinal study on the elderly in Japan. Sleep. 2010;33(12):1693–1702. doi:10.1093/sleep/33.12.1693
8. Paudel M, Taylor BC, Ancoli-Israel S, et al. Sleep disturbances and risk of depression in older men. Sleep. 2013;36(7):1033–1040. doi:10.5665/sleep.2804
9. Maglione JE, Ancoli-Israel S, Peters KW, et al. Subjective and objective sleep disturbance and longitudinal risk of depression in a cohort of older women. Sleep. 2014;37(7):1179–1187. doi:10.5665/sleep.3834
10. Krystal AD. Depression and insomnia in women. Clin Cornerstone. 2004;6(Suppl 1B):S19–S28. doi:10.1016/s1098-3597(04)80022-x
11. Szklo-Coxe M, Young T, Peppard PE, Finn LA, Benca RM. Prospective associations of insomnia markers and symptoms with depression. Am J Epidemiol. 2010;171(6):709–720. doi:10.1093/aje/kwp454
12. Anderson KN, Bradley AJ. Sleep disturbance in mental health problems and neurodegenerative disease. Nat Sci Sleep. 2013;5:61–75. doi:10.2147/nss.S34842
13. Almeida OP, Alfonso H, Yeap BB, Hankey G, Flicker L. Complaints of difficulty to fall asleep increase the risk of depression in later life: the health in men study. J Affect Disord. 2011;134(1–3):208–216. doi:10.1016/j.jad.2011.05.045
14. Liu Q, Wangqing P, Baima Y, et al. Comorbid depressive and anxiety symptoms and their correlates among 93,078 multiethnic adults in Southwest China. Front Public Health. 2021;9:783687. doi:10.3389/fpubh.2021.783687
15. Zhao X, Hong F, Yin J, et al. Cohort Profile: the China Multi-Ethnic Cohort (CMEC) study. Int J Epidemiol. 2021;50(3):721–721l. doi:10.1093/ije/dyaa185
16. Belzer K, Schneier FR. Comorbidity of anxiety and depressive disorders: issues in conceptualization, assessment, and treatment. J Psychiatr Pract. 2004;10(5):296–306. doi:10.1097/00131746-200409000-00003
17. XiaoY H. Study on the Prevalence Nd Influencing Factors of Hyperlipidemia Among Han People in Yongsheng County, Yunnan Province. master. kunming medical university; 2021.
18. Luo Z, Li Y, Hou Y, et al. Gender-specific prevalence and associated factors of major depressive disorder and generalized anxiety disorder in a Chinese rural population: the Henan rural cohort study. BMC Public Health. 2019;19(1):1744. doi:10.1186/s12889-019-8086-1
19. Luo Z, Li Y, Hou Y, et al. Adaptation of the two-item generalized anxiety disorder scale (GAD-2) to Chinese rural population: a validation study and meta-analysis. Gen Hosp Psychiatry. 2019;60:50–56. doi:10.1016/j.genhosppsych.2019.07.008
20. Cable N, Chandola T, Aida J, Sekine M, Netuveli G. Can sleep disturbance influence changes in mental health status? Longitudinal research evidence from ageing studies in England and Japan. Sleep Med. 2017;30:216–221. doi:10.1016/j.sleep.2016.11.017
21. Grandner MA, Hale L, Moore M, Patel NP. Mortality associated with short sleep duration: the evidence, the possible mechanisms, and the future. Sleep Med Rev. 2010;14(3):191–203. doi:10.1016/j.smrv.2009.07.006
22. Sun X, Zheng B, Lv J, et al. Sleep behavior and depression: findings from the China Kadoorie Biobank of 0.5 million Chinese adults. J Affect Disord. 2018;229:120–124. doi:10.1016/j.jad.2017.12.058
23. Ciren W, Yu W, Nima Q, et al. Social capital and sleep disorders in Tibet, China. BMC Public Health. 2021;21(1):591. doi:10.1186/s12889-021-10626-x
24. Zhang WZ. Intensified, optimized and standardized management of Chinese patients with hypertension: comments on ”2018 Chinese guidelines for prevention and treatment of hypertension”. J Geriatr Cardiol. 2019;16(3):178–181. doi:10.11909/j.issn.1671-5411.2019.03.013
25. Moffitt TE, Harrington H, Caspi A, et al. Depression and generalized anxiety disorder: cumulative and sequential comorbidity in a birth cohort followed prospectively to age 32 years. Arch. Gen. Psychiatry. 2007;64(6):651–660. doi:10.1001/archpsyc.64.6.651
26. Blay SL, Fillenbaum GG, Mello MF, et al. 12-month prevalence and concomitants of DSM-IV depression and anxiety disorders in two violence-prone cities in Brazil. J Affect Disord. 2018;232:204–211. doi:10.1016/j.jad.2018.02.023
27. Zhang J, He M, Wang X, Jiang H, Huang J, Liang S. Association of sleep duration and risk of mental disorder: a systematic review and meta-analysis. Sleep Breath. 2023;29. doi:10.1007/s11325-023-02905-1
28. Li Y, Wu Y, Zhai L, Wang T, Sun Y, Zhang D. Longitudinal association of sleep duration with depressive symptoms among middle-aged and older Chinese. Sci Rep. 2017;7(1):11794. doi:10.1038/s41598-017-12182-0
29. Zhang XF, Liu F, Liu WP, Ye XM, Cui BY, Wang HJ. 中国四省中老年人睡眠时长与抑郁症状的关联性研究 [Relationship between sleep duration and depressive symptoms in middle-aged and elderly people in four provinces of China]. Zhonghua Liu Xing Bing Xue Za Zhi. 2021;42(11):1955–1961. Chinese. doi:10.3760/cma.j.cn112338-20200930-01210
30. Irwin MR, Opp MR. Sleep health: reciprocal regulation of sleep and innate immunity. Neuropsychopharmacology. 2017;42(1):129–155. doi:10.1038/npp.2016.148
31. Cho HJ, Eisenberger NI, Olmstead R, Breen EC, Irwin MR. Preexisting mild sleep disturbance as a vulnerability factor for inflammation-induced depressed mood: a human experimental study. Transl Psychiatry. 2016;6(3):e750. doi:10.1038/tp.2016.23
32. Ding L, Zhang L, Cui Y, et al. The association of sleep duration and quality with depressive symptoms in older Chinese women. PLoS One. 2022;17(3):e0262331. doi:10.1371/journal.pone.0262331
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.