")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 19
Real-World Effectiveness Study of Nirmatrelvir-Ritonavir or Molnupiravir in Hospitalized Unvaccinated Patients with Chronic Respiratory Diseases and Moderate COVID-19 at Presentation
Authors Kwok WC , Tam TCC, Ho JCM, Lam DCL, Ip MSM, Ho PL
Received 16 October 2023
Accepted for publication 26 December 2023
Published 9 January 2024 Volume 2024:19 Pages 77—86
DOI https://doi.org/10.2147/COPD.S440895
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Wang Chun Kwok,1 Terence Chi Chun Tam,1 James Chung Man Ho,1 David Chi Leung Lam,1 Mary Sau-Man Ip,1 Pak Leung Ho2
1Department of Medicine, Queen Mary Hospital, The University of Hong Kong, Pokfulam, Hong Kong Special Administrative Region, People’s Republic of China; 2Department of Microbiology and Carol Yu Centre for Infection, Queen Mary Hospital, The University of Hong Kong, Pokfulam, Hong Kong Special Administrative Region, People’s Republic of China
Correspondence: Pak Leung Ho, Department of Microbiology and Carol Yu Centre for Infection, The University of Hong Kong, Queen Mary Hospital, 102 Pokfulam Road, Pokfulam, Hong Kong Special Administrative Region, People’s Republic of China, Tel +852-2255-2584, Fax +852 2855 1241, Email [email protected]
Introduction: Nirmatrelvir-ritonavir (NMV-r) and molnupiravir (MOL) were developed as out-patient anti-viral for mild COVID-19. There was limited data on their role in treating COVID-19 for hospitalized patients, especially among adult patients who are unvaccinated and had chronic respiratory diseases.
Methods: A territory-wide retrospective study was conducted in Hong Kong to compare the efficacy of NMV-r and MOL against COVID-19 in unvaccinated adult patients with asthma, chronic obstructive pulmonary disease, bronchiectasis and interstitial lung diseases presenting with moderate COVID-19 from 16th February 2022 to 15th March 2023.
Results: A total of 1354 patients were included, 738 received NMV-r and 616 received MOL. NMV-r was more effective in reducing 90-day mortality with adjusted hazard ratios (aHR) of 0.508 (95% confidence interval [CI] = 0.314– 0.822, p = 0.006). Patients who received NMV-r also had significantly shorter length of stay (LOS) than those receiving MOL, with median LOS of 4 (Interquartile range [IQR] = 2– 7) for NMV-r and 6 (IQR = 3– 10) for MOL (p-value < 0.001). There was no statistically significant difference in the development of respiratory failure and severe respiratory failure in the two groups.
Discussion: NMV-r was more effective than MOL among unvaccinated adults with chronic respiratory diseases who were hospitalized for moderate COVID-19 without hypoxaemia on admission.
Keywords: asthma, COPD, bronchiectasis, interstitial lung disease, molnupiravir, nirmatrelvir-ritonavir, COVID-19
Introduction
The introduction of oral antivirals nirmatrelvir-ritonavir (NMV-r) and molnupiravir (MOL) against COVID-19 allows successful outpatient management of COVID-19.1–3 NMV-r is a combination of oral protease inhibitors, with nirmatrelvir blocking the activity of the SARS-CoV-2-3CL protease and coadministration with ritonavir slows the metabolism of nirmatrelvir so it remains active in the body for longer and at higher concentrations. MOL is a nucleoside analog that inhibits SARS-CoV-2 replication by inducing lethal mutations in the viral RNA. NMV-r and MOL have been demonstrated to reduce hospitalization and mortality in clinical trials.4–6 The benefits were also demonstrated in real-world studies.7–9 However, for patients with co-morbidities, including patients with chronic respiratory diseases (including asthma, bronchiectasis, chronic obstructive pulmonary disease (COPD) and interstitial lung disease) who have compromised pulmonary function, they may still develop moderate-to-severe diseases that require hospitalization.10–13 NMV-r and MOL have been suggested to be effective among adult patients with chronic respiratory diseases who were unvaccinated, when managed in outpatients in preventing respiratory failure (NMV-r), severe respiratory failure (NMV-r and MOL) and in-hospital mortality (MOL).14 Among patients hospitalized for COVID-19, remdesivir has been approved to be used in the treatment of hospitalized children ≥12 years and adults with COVID-19, regardless of the severity of disease.15 But remdesivir requires three intravenous doses over 3 days, which is less convenient than oral anti-virals and early discharge is not possible before the 3-day course is finished, unlike for oral anti-virals. Given the effectiveness of MOL and NMV-r against COVID-19 in prior studies, there have been studies on whether they can also be used among hospitalized patients. A target trial emulation study suggested that both MOL and NMV-r could reduce all-cause mortality in hospitalized patients regardless of the vaccination status. However, intensive care unit admission or the need for ventilatory support was not reduced.16 Another study suggested that using NMV-r and MOL in hospitalized patients who do not require supplementary oxygen at the time of admission is associated with clinical benefits in terms of all-cause mortality, composite disease progression outcome, need for oxygen therapy and time to achieving a low viral burden.17 To date, both MOL and NMV-r have only been approved to be used as out-patient anti-viral agents in patients who are at high risk for progression to severe COVID-19, including hospitalization or death by The US Food and Drug Administration (FDA)18,19 and European Medicines Agency (EMA).20,21
While NMV-r and MOL were proven to be effective as oral agents in out-patient setting, NMV-r was a more preferred option given its superior clinical benefits over MOL.22 There was even less evidence on the use of NMV-r and MOL in selected subgroup, such as those having chronic respiratory diseases,14 especially for head-to-head comparison. It is worthwhile to know the effectiveness of NMV-r and MOL among these patients who are at risk of severe COVID-19.
Materials and Methods
We conducted a retrospective territory-wide cohort study in Hong Kong to investigate the efficacy of NMV-r and MOL among adult patients who had chronic respiratory diseases (COPD, asthma, bronchiectasis and interstitial lung diseases (ILD)), who were unvaccinated and hospitalized for COVID-19 with moderate severity at presentation that did not require supplemental oxygen on admission. Eligible patients were identified from the Clinical Data Analysis and Reporting System (CDARS) of Hospital Authority (HA), which is an electronic database containing all the patient information within HA. HA operates all public hospitals and clinics and is responsible for the vast majority of healthcare services in Hong Kong. It also managed the majority of patients with COVID-19 in Hong Kong. Patients that were clinically stable would be managed in designated outpatient clinics. Patients with moderate-to-severe COVID-19 or had multiple co-morbidities would be admitted to designated isolation facilities.23 Early COVID-19 treatment regimens would be offered to inpatients who were at high risk of severe disease. MOL was first available in Hong Kong on 26th February 2022, while NMV-r from 16th March 2022. Patients were considered to have a high risk of severe disease if they had the following conditions: diabetes mellitus, obesity (body mass index >30 kg/m2), age >60, immunocompromised, chronic diseases and COVID-19 vaccination incomplete. For patients with mild symptoms but at high risk of disease progression and within 5 days of disease onset, NMV-r or MOL will be started. NMV-r is the preferred agent unless contraindicated.
Patients with confirmed COVID-19 were identified by the International Classification of Diseases, Ninth Revision (ICD-9) diagnostic code of 519.8 from 26th February 2022 to 15th March 2023. According to the National Institutes of Health (NIH) Coronavirus Disease 2019 (COVID-19) Treatment Guidelines, moderate COVID-19 was defined as COVID-19 among patients who had lower respiratory disease on clinical assessment or imaging and had an oxygen saturation ≥94% on room air at sea level.24 Patients with underlying COPD, asthma, bronchiectasis and ILD were identified using the following ICD-9 diagnostic codes of 493.x, 496.x, 494.x and 516.3/517.2/517.8/714.81/495, respectively.25–27 Patients who had a previous history of COVID-19, who received MOL or NMV-r in an outpatient setting before hospitalization, who received remdesivir treatment, received both MOL and NMV-r in the same index admission (simultaneous or sequential) and those requiring supplementary oxygen upon admission were excluded. The cohort was followed-up until 30th June 2023. There is no overlap between the current inpatient cohort and the outpatient cohort in our previous work as all the patients who had outpatient management were excluded in this study.14 Unvaccinated patients were referred to as patients who did not complete two doses of COVID-19 within 14 days at the time of COVID-19.
The exposure of interest was NMV-r and MOL prescriptions in hospitalized patients who had chronic respiratory diseases and were unvaccinated and who do not need supplemental oxygen on admission. The standard treatment course of NMV-r and MOL was 5 days.28
The study was approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (UW 23-450).
Outcomes
The primary outcome of interest was COVID-19 related mortality within 90 days of the onset of infection. The secondary outcomes include COVID-19 related respiratory failure, COVID-19 related severe respiratory failure, in-hospital mortality, and length of stay. COVID-19 related respiratory failure was defined as desaturation with oxygen saturation <90% within 14 days of confirmed COVID-19. COVID-19 related severe respiratory failure was defined as the need for high flow nasal cannula (HFNC), non-invasive ventilation (NIV), or invasive mechanical ventilation (IMV) within 14 days of confirmed COVID-19.29
Statistical Analysis
Clinical and demographic data were described in frequency, mean (± standard deviation [SD]) or median (interquartile range [IQR]). Categorical variables were expressed as frequency and percentage and compared with Chi-square tests or Fisher’s exact tests where appropriate. Continuous variables were expressed as mean (± SD) and compared with Student’s t-tests or Mann–Whitney U-tests where appropriate. MOL was chosen to be the reference group for comparison with the NMV-r group. To identify whether NMV-r or MOL use was associated with protection from the primary and secondary outcomes, univariate logistic regression analyses were performed. The length of stay in both groups was compared by linear regression. Multiple logistic regression was adopted to account for potential confounders including age (<70 or ≥70), sex, Charlson comorbidity index (CCI) (<5 or ≥5), time from admission to initiation of antiviral (≤3 or >3 days), degree of renal impairment, concomitant Group 1 to 3 medication and underlying respiratory diagnosis, all as categorical variables by a multivariate analysis model. Cox regression analysis was used to assess survival. Kaplan–Meier analysis was used to estimate the cumulative death rates and the stratified log-rank statistics to assess the effects of anti-viral treatment in the follow-up period with respect to the composite end point of death in 90 days. Statistical significance was determined at the level of p value below 0.05. Odds ratios (OR), hazard ratios (HR) and 95% confidence intervals (CI) for the outcomes in the NMV-r and MOL groups were calculated using logistic regression and Cox regression, respectively. Statistical analyses were performed using the 28th version of SPSS statistical package. Sensitivity analysis was performed, analyzing patients who received early treatment for NMV-r and MOL, as defined by within 5 days of admission. The same co-primary outcomes were analyzed in sensitivity analysis with logistic regression and Cox regression as in primary analysis.
Results
A total of 3856 adult unvaccinated patients who had chronic respiratory diseases were identified from CDARS. A total of 2502 patients were excluded and 1354 were included in the final analysis. The patient selection is illustrated in Figure 1. Among the 1354 patients in the cohort, 738 received NMV-r and 616 patients received MOL (Table 1). Patients who received NMV-r were younger than those who received MOL (Median 78.5 vs 82 years old, p < 0.001), had lower CCI (median 5 vs 6, p < 0.001), less likely to be on concomitant Group 1 to 3 medication (Table S1) that would interact with NMV-r (57.2 vs 83.4%, p < 0.001) and had anti-viral within 3 days of admission (94.4% vs 91.5%, p = 0.037).
 |
Table 1 Demographic and Clinical Characteristics of Included Patients |
 |
Figure 1 Flow diaphragm on patient selection. |
COVID-19-Related Respiratory Failure
Among the patients included in the study, 9.0% (122/1354) developed COVID-19 related respiratory failure (Table 2). Patients who received MOL (10.7%) were more likely to develop COVID-19 related respiratory failure than those who received NMV-r (7.6%). The unadjusted OR was 0.684 (95% CI = 0.471–0.994, p = 0.046) for NMV-r. The adjusted OR (aOR) was 0.841 (95% CI = 0.530–1.332, p = 0.460) for NMV-r.
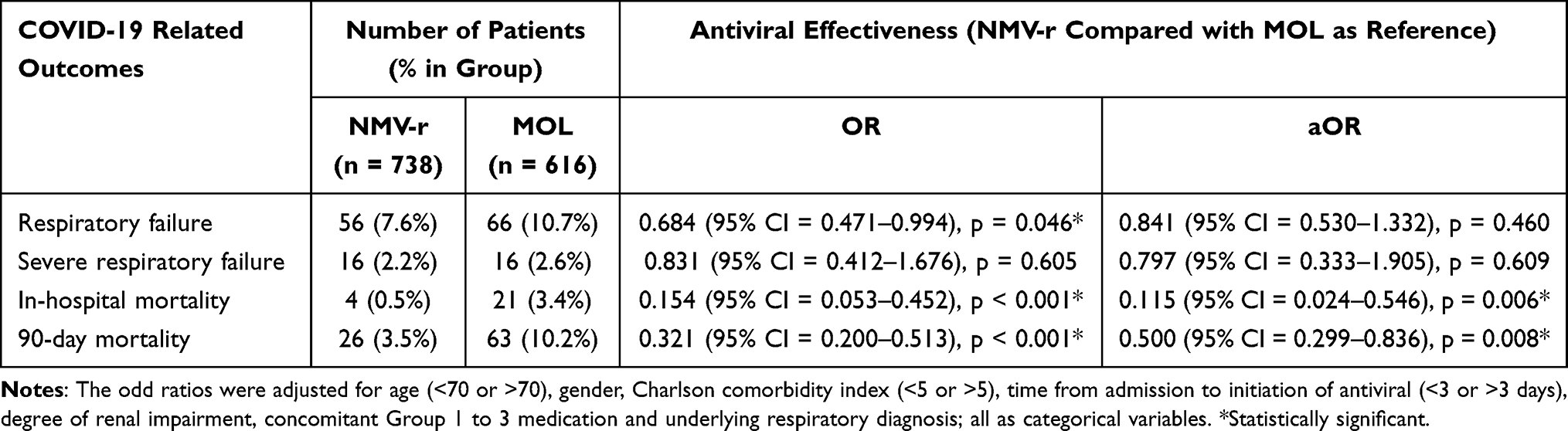 |
Table 2 Effectiveness of Nirmatrelvir-Ritonavir (NMV-r) and Molnupiravir (MOL) in Preventing COVID-19 Related Respiratory Failure, Severe Respiratory Failure and Mortality |
COVID-19-Related Severe Respiratory Failure
COVID-19 related severe respiratory failure developed in 2.4% (32/1354) of the included patients (Table 2). There were 16 (2.6%) patients who received MOL and 16 (2.2%) patients who received NMV-r developed COVID-19 related severe respiratory failure. The unadjusted OR was 0.831 (95% CI = 0.412–1.676, p = 0.605) for NMV-r. The aOR was 0.797 (95% CI = 00.333–1.905, p = 0.609) for NMV-r.
Mortality
Overall, 1.8% (25/1354) died within the index hospitalization (Table 2). Patients who received MOL (3.4%) were significantly more likely to die within the index hospitalization than patients who received NMV-r (0.5%). The unadjusted OR was 0.154 (95% CI = 0.053–0.452, p < 0.001) for NMV-r. The aOR was 0.115 (95% CI = 0.024–0.546, p = 0.006) for NMV-r. This suggests that patients who received NMV-r had a lower risk of in-hospital mortality even after adjusting for confounders.
Overall, 6.6% (89/1354) died within 90 days from the day of admission (Table 2). Patients who received MOL (5.7%) were more likely to die within 90 days from day of admission than patients who received NMV-r (1.6%). The unadjusted OR was 0.321 (95% CI = 0.200–0.513, p < 0.001) for NMV-r. The aOR was 0.500 (95% CI = 0.299–0.836, p = 0.008) for NMV-r.
Survival analysis with the outcome of 90-day mortality was performed with Cox-regression. The HR was 0.333 (95% CI = 0.211–0.526, p < 0.001) and aHR was 0.508 (95% CI = 0.314–0.822, p = 0.006) for patients receiving NMV-r, suggesting that patients who received NMV-r had lower risks of 90 days mortality (Figure 2).
 |
Figure 2 Survival analysis for whole cohort. |
Length of Stay (LOS)
The median LOS was 4 (IQR = 2–7) for patients receiving NMV-r and 6 (IQR = 3–10) for patients receiving MOL. The p-value was <0.001 in both univariate and multivariate analysis. This suggests that patients who received NMV-r had significantly shorter LOS.
Sensitivity Analysis
Subgroup analysis was performed on patients who received early treatment for NMV-r and MOL, as defined by within 5 days of admission. There were 1278 patients, 704 received NMV-r and 574 received MOL. The results from the sensitivity analysis were consistent with those from the primary analysis and the results were summarized in Tables S2 and S3 and Figure S1.
Discussion
To the best of our knowledge, this study is the first real-world study to suggest the superiority of NMV-r over MOL as an in-patient anti-viral agent among adult patients who had underlying COPD, asthma, bronchiectasis and ILD, who were unvaccinated and hospitalized for moderate COVID-19 at presentation. Our findings concur with previous report on the efficacy of NMV-r use among patients hospitalized for COVID-19, as well as other literature to suggest the superiority of NMV-r over MOL in other settings.17,22 This mainly lies on the mortality reduction with aOR of 0.321 and aHR of 0.503 for 90-day mortality. There were also benefits in terms of shorter LOS. The results suggested the use of NMV-r over MOL in adult unvaccinated patients who had chronic respiratory diseases hospitalized for moderate COVID-19.
In previous studies, while there may be trends to suggest NMV-r being superior to MOV as in-patient anti-viral, a definite conclusion was not reached.16,17 Furthermore, they included all in-patients, regardless of the COVID-vaccination status and the co-morbidities. Whether these results are applicable to patients at increased risk of severe COVID-19, such as unvaccinated patients with chronic respiratory diseases, is uncertain. We try to provide possible answers to the above questions with the current study. Our study included a more well-defined cohort of adult unvaccinated patients who had chronic respiratory diseases only. They were all not requiring supplementary oxygen at the time of admission, which suggested that they had moderate but not severe COVID-19. From the results of this well-defined cohort, it further enriches the prior reports on potential success with early initiation of NMV-r among selected hospitalized patients with COVID-19 in particular the subgroup with underlying chronic respiratory diseases, who had a high risk of severe COVID-19. Early treatment with NMV-r for these patients could prevent mortality, as well as hastening the recovery with shorter LOS, as shown by our study, as in other patient groups as demonstrated by prior studies.16,17 The findings can allow for the potential use of NMV-r as an initial oral anti-viral for adult unvaccinated patients who had chronic respiratory diseases admitted for COVID-19, who do not require supplementary oxygen at the time of admission.
While remdesivir was the only approved anti-viral agent to be used for patients hospitalized for COVID-19, there has been concern about its effectiveness30 and a prospective observational study suggested NMV-r to be more effective than remdesivir in out-patient management.31 Based on the results from our study, as well as previous reports, NMV-r may have an emerging role as a potential anti-viral option among patients hospitalized with COVID-19 who had moderate disease, at least as an alternative to remdesivir, with mortality reduction and hastening the recovery with shorter length of stay. Another benefit of NMV-r over remdesivir is on the ease of administration as an oral anti-viral, as remdesivir needs to be given by intravenous route. On the other hand, the prescription of MOL among hospitalized patients might not be most appropriate as it is less effective than NMV-r. The role of MOL in hospitalized patients with chronic respiratory diseases who did not have COVID-19 vaccination should be properly assessed in future studies.
Patients with underlying medical co-morbidities and unvaccinated are considered to have increased risks for COVID-19 complications according to local clinical management guideline issued by HA. They warrant early treatment to prevent disease progression according to local practice guideline.23 While there have been studies to suggest the NMV-r to be superior to MOL among mild-to-moderate COVID-19, MOL are considered among patients who are contraindicated to NMV-r, in particular patients with major renal impairment and on drugs that have potential interaction with NMV-r. In our study, more patients were treated with NMV-r than MOL. The main reason for prescribing MOL is the use of concomitant medication that are reported to have clinically relevant drug–drug interactions, with 94.0% on Group 1 to 3 medication in the MOL group. From our study findings, the careful consideration of NMV-r with appropriate dose adjustment or suspension of concomitant medication if clinically feasible should be seriously considered, as MOL was shown to be less effective in terms of mortality reduction and length of stay.
In this study, patients prescribed with NMV-r were older and more likely to be on Group 1 to 3 medications. This could reflect the clinicians’ preference on anti-viral among elderly patients with co-morbidities, due to potential concerns of drug interaction and renal function impairment among elderly patients. Patients prescribed with NMV-r were also initiated with anti-virals earlier. But more than 90% of the patients were prescribed with NMV-r or MOL within 5 days of hospital admission, which is the recommended time frame for anti-viral prescription.
Despite demonstrating the survival benefits from NMV-r, there was no statistical significance regarding the other outcomes including respiratory failure and severe respiratory failure in the two groups. This could be explained by the fact that the development of respiratory failure and severe respiratory failure could be affected by the severity of the underlying respiratory diseases. Patients with more advanced underlying respiratory diseases might be more prone to developing respiratory failure and severe respiratory failure upon having COVID-19 and any other respiratory viral infections. To properly assess the benefits of anti-virals in terms of respiratory failure, a prospective study with proper measurement of other respiratory related parameters such as the ratio of partial pressure of oxygen in arterial blood (PaO2) to the fraction of inspiratory oxygen concentration (FiO2), time to wean off from supplementary oxygen and the duration of mechanical ventilation would be helpful.
The strength of this study is that a highly specialized population was selected, who are at increased risk of severe COVID-19. Moreover, the efficacy of NMV-r and MOL was compared at the time of the fifth wave of outbreak in Hong Kong, with Omicron variants being the dominant strain. The results from this study were also consistent with previous reports on the use NMV-r and MOL for Omicron variants. Our study is also the first head-to-head comparison of NMV-r and MOL as in-patient anti-viral for adult unvaccinated patients who had underlying chronic respiratory diseases.
In our study, public electronic medical record was used which encompass the vast majority of COVID-19 cases in the study period. Together with the introduction of NMV-r and MOL in the public health-care system during the fifth wave of COVID-19, the effectiveness in adult unvaccinated patients who had underlying chronic respiratory diseases is assessed in real-world settings. There are few limitations in our study. First, in the prescription of antivirals, indication bias could be present, as reflected by the differences in age and co-morbidities among the NMV-r and MOL groups. Potential residual confounding due to indication and contraindications could be present when deciding on the prescription MOL over NMV-r. Nonetheless, potential confounders including CCI, baseline eGFR, prescription record of group 1 to 3 medication and other important confounders were adjusted in multivariate analysis with consistent results. As a retrospective study, the medication prescription and the follow-up management are not exactly protocol based. The date of symptom onset was not available, and the date of hospital admission was used as a surrogate. Nonetheless, the management of COVID-19 for patients in this cohort is largely following the standard treatment guidelines as required by HA. Following a local guideline for the management of COVID-19 in the public hospitals can help to minimize the heterogeneity in patient management. The relatively small sample size is also a potential limitation in our study. The inclusion of only patients with chronic respiratory diseases may limit the generalizability of the results, though similar findings have been demonstrated in other studies. Another limitation is that the exact symptom onset date was not available, and we used the time from hospital admission to the time of anti-viral initiation to define whether the patients had early anti-viral treatment.
Conclusion
Among unvaccinated adults having chronic respiratory disease hospitalized for moderate COVID-19, NMV-r was more effective than MOL with benefits in terms of mortality reduction and shorter LOS compared.
Data Sharing Statement
The data presented in this study are available in the manuscript and Supplementary Materials.
Informed Consent Statement
Informed consent was waived by the Institutional Review Board of the University of Hong Kong and Hospital Authority Hong Kong West Cluster, as it was a retrospective study without active patient recruitment and the data were already deidentified.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the University of Hong Kong and Hospital Authority Hong Kong West Cluster (UW23-450).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by internal funding from the Department of Microbiology, The University of Hong Kong.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Wang Z, Yang L, Song X-Q. Oral GS-441524 derivatives: next-generation inhibitors of SARS-CoV-2 RNA-dependent RNA polymerase. Front Immunol. 2022;13:1015355. doi:10.3389/fimmu.2022.1015355
2. Sasaki M, Tabata K, Kishimoto M, et al. S-217622, a SARS-CoV-2 main protease inhibitor, decreases viral load and ameliorates COVID-19 severity in hamsters. Sci Trans Med. 2022;15(679):eabq4064. doi:10.1126/scitranslmed.abq4064
3. Yang L, Wang Z. Bench-to-bedside: innovation of small molecule anti-SARS-CoV-2 drugs in China. Eur J Med Chem. 2023;257:115503. doi:10.1016/j.ejmech.2023.115503
4. Jayk Bernal A, Gomes da Silva MM, Musungaie DB, et al. Molnupiravir for oral treatment of Covid-19 in nonhospitalized patients. N Engl J Med. 2022;386(6):509–520. doi:10.1056/NEJMoa2116044
5. Singh AK, Singh A, Singh R, Misra A. Molnupiravir in COVID-19: a systematic review of literature. Diabetes Metab Syndr. 2021;15(6):102329. doi:10.1016/j.dsx.2021.102329
6. Hammond J, Leister-Tebbe H, Gardner A, et al. Oral nirmatrelvir for high-risk, nonhospitalized adults with Covid-19. N Engl J Med. 2022;386(15):1397–1408. doi:10.1056/NEJMoa2118542
7. Evans A, Qi C, Adebayo JO, et al. Real-world effectiveness of molnupiravir, nirmatrelvir-ritonavir, and sotrovimab on preventing hospital admission among higher-risk patients with COVID-19 in Wales: a retrospective cohort study. J Infect. 2023;86(4):352–360. doi:10.1016/j.jinf.2023.02.012
8. Mutoh Y, Umemura T, Nishikawa T, et al. Real-world experience of the comparative effectiveness and safety of molnupiravir and nirmatrelvir/ritonavir in high-risk patients with COVID-19 in a community setting. Viruses. 2023;15(3):811. doi:10.3390/v15030811
9. Wong CKH, Au ICH, Lau KTK, Lau EHY, Cowling BJ, Leung GM. Real-world effectiveness of molnupiravir and nirmatrelvir plus ritonavir against mortality, hospitalisation, and in-hospital outcomes among community-dwelling, ambulatory patients with confirmed SARS-CoV-2 infection during the omicron wave in Hong Kong: an observational study. Lancet. 2022;400(10359):1213–1222. doi:10.1016/S0140-6736(22)01586-0
10. Kwok WC, Tam AR, Ho JCM, et al. Asthma, from mild to severe, is an independent prognostic factor for mild to severe Coronavirus disease 2019 (COVID-19). Clin Respir J. 2022;16(4):293–300. doi:10.1111/crj.13480
11. Gomez Antunez M, Muino Miguez A, Bendala Estrada AD, et al. Clinical characteristics and prognosis of COPD patients hospitalized with SARS-CoV-2. Int J Chron Obstruct Pulmon Dis. 2020;15:3433–3445. doi:10.2147/COPD.S276692
12. Choi H, Lee H, Lee SK, et al. Impact of bronchiectasis on susceptibility to and severity of COVID-19: a nationwide cohort study. Ther Adv Respir Dis. 2021;15:1753466621995043. doi:10.1177/1753466621995043
13. Cilli A, Hanta I, Uzer F, et al. Characteristics and outcomes of COVID-19 patients with IPF: a multi-center retrospective study. Respir Med Res. 2022;81:100900. doi:10.1016/j.resmer.2022.100900
14. Kwok WC, Tsoi MF, Leung SHI, et al. Real-world study on effectiveness of molnupiravir and nirmatrelvir-ritonavir in unvaccinated patients with chronic respiratory diseases with confirmed SARS-CoV-2 infection managed in out-patient setting. Viruses. 2023;15(3). doi:10.3390/v15030610
15. Foster City CBGS, Inc. Veklury. US FDA approved product information; 2020. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/214787Orig1s000lbl.pdf.
16. Wan EYF, Yan VKC, Mok AHY, et al. Effectiveness of molnupiravir and nirmatrelvir-ritonavir in hospitalized patients with COVID-19: a target trial emulation study. Ann Intern Med. 2023;176(4):505–514. doi:10.7326/M22-3057
17. Wong CKH, Au ICH, Lau KTK, Lau EHY, Cowling BJ, Leung GM. Real-world effectiveness of early molnupiravir or nirmatrelvir-ritonavir in hospitalised patients with COVID-19 without supplemental oxygen requirement on admission during Hong Kong’s omicron BA.2 wave: a retrospective cohort study. Lancet Infect Dis. 2022;22(12):1681–1693. doi:10.1016/S1473-3099(22)00507-2
18. FDA. Fact Sheet for Healthcare Providers: Emergency Use Authorization for Paxlovid™. FDA, editor. The United States Food and Drug Administration (FDA); 2022.
19. FDA. Fact Sheet for Healthcare Providers: Emergency Use Authorization for Lagevrio™ (Molnupiravir) Capsules. FDA, editor. The United States Food and Drug Administration (FDA); 2021.
20. EMA. Summary of Product Characteristics - Nirmatrelvir-Ritonavir. EMA, editor. European Medicines Agency (EMA); 2022.
21. EMA. Conditions of Use, Conditions for Distribution and Patients Targeted and Conditions for Safety Monitoring Addressed to Member States for Unauthorised Product Lagevrio (Molnupiravir) Available for Use. EMA, editor. European Medicines Agency (EMA); 2022.
22. Amani B, Akbarzadeh A, Amani B, et al. Comparative efficacy and safety of nirmatrelvir/ritonavir and molnupiravir for COVID-19: a systematic review and meta-analysis. J Med Virol. 2023;95(6):e28889. doi:10.1002/jmv.28889
23. HA CCIDER. Interim Recommendation on Clinical Management of Adult Cases with Coronavirus Disease 2019 (COVID-19). Hospital Authority Central Committee on Infectious Disease and Emergency Responses (HA CCIDER); 2023.
24. NIH. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health (NIH); 2023.
25. Ye Y, Hubbard R, Li GH, et al. Validation of diagnostic coding for interstitial lung diseases in an electronic health record system in Hong Kong. Pharmacoepidemiol Drug Saf. 2022;31(5):519–523. doi:10.1002/pds.5421
26. Kwok WC, Tam TCC, Sing CW, Chan EWY, Cheung CL. Validation of diagnostic coding for bronchiectasis in an electronic health record system in Hong Kong. Pharmacoepidemiol Drug Saf. 2023;32(10):1077–1082. doi:10.1002/pds.5638
27. Kwok WC, Tam TCC, Sing CW, Chan EWY, Cheung CL. Validation of diagnostic coding for asthma in an electronic health record system in Hong Kong. J Asthma Allergy. 2023;16:315–321. doi:10.2147/JAA.S405297
28. HA CCIDER. Interim Recommendation on Clinical Management of Adult Cases with Coronavirus Disease 2019 (COVID-19). Hospital Authority Central Committee on Infectious Disease and Emergency Responses (HA CCIDER); 2022.
29. WHO. COVID-19 Clinical Management Living Guidance. Vol. 3.
30. Del Borgo C, Garattini S, Bortignon C, et al. Effectiveness, tolerability and prescribing choice of antiviral molecules molnupiravir, remdesivir and nirmatrelvir/r: a real-world comparison in the first ten months of use. Viruses. 2023;15(4):1025. doi:10.3390/v15041025
31. Tiseo G, Barbieri C, Galfo V, et al. Efficacy and safety of nirmatrelvir/ritonavir, molnupiravir, and remdesivir in a real-world cohort of outpatients with COVID-19 at high risk of progression: the PISA outpatient clinic experience. Infect Dis Ther. 2023;12(1):257–271. doi:10.1007/s40121-022-00729-2
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.