")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 19
Quantitative Assessment Characteristics of Small Pulmonary Vessel Remodelling in Populations at High Risk for COPD and Smokers Using Low-Dose CT
Authors Pu Y, Zhou X, Zhang D, Guan Y , Xia Y, Liu S , Fan L
Received 11 September 2023
Accepted for publication 15 December 2023
Published 6 January 2024 Volume 2024:19 Pages 51—62
DOI https://doi.org/10.2147/COPD.S436242
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Russell
Yu Pu,* Xiuxiu Zhou,* Di Zhang, Yu Guan, Yi Xia, Shiyuan Liu, Li Fan
Department of Radiology, Second Affiliated Hospital of PLA Naval Medical University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shiyuan Liu; Li Fan, Department of Radiology, Second Affiliated Hospital of Naval Medical University, No. 415 Fengyang Road, Shanghai, 200003, People’s Republic of China, Tel +86 21 81886012 ; +86 21 81886011, Fax +86 21 63587668, Email [email protected]; [email protected]
Purpose: To explore the morphological alterations in small pulmonary vessels in populations at high risk for chronic obstructive pulmonary disease (COPD) and smokers based on multiple computed tomography (CT) quantitative parameters.
Patients and Methods: A total of 1969 Three Major Chest Diseases Screening Study participants with available demographic data and smoking history who underwent low-dose chest CT from 2018 to 2020 were included. All subjects were divided into normal, high risk for COPD, and COPD groups according to their pulmonary function test (PFT) results. Furthermore, the three groups were further subdivided into never-smokers, current smokers, and former smokers subgroups according to their smoking history. Quantitative parameters, such as the number, area at 6 mm~24 mm subpleura and volume of small pulmonary vessels, were extracted by computer software. Differences in small pulmonary vessel parameters among the groups were compared using two-way ANOVA.
Results: The number, area at 6 mm~24 mm subpleura and volume of small pulmonary vessels in the group at high risk for COPD were lower than those in the normal group (P< 0.05). The number, area at 6 mm~24 mm subpleura and volume of small pulmonary vessels in the COPD group were higher than those in the normal group (P< 0.05). The number, area of small pulmonary vessels at 6 mm~12 mm subpleura in current smokers with high risk for COPD were higher than those in former smokers with high risk for COPD (P< 0.05).
Conclusion: The number, area, and volume of small pulmonary vessels in populations at high risk for COPD were decreased. Smoking cessation may impede structural changes in small pulmonary vessels in populations at high risk for COPD.
Keywords: chronic obstructive pulmonary disease, computed tomography, pulmonary vascular structure, quantitative analysis, smoking
Introduction
Populations at high risk for COPD and their diagnostic criteria have recently garnered widespread attention,1 given that early diagnosis, intervention, and treatment of COPD patients could reverse the clinical course of COPD.2,3 Although PFT was the gold standard for the diagnosis of COPD, it is not sensitive in diagnosing populations at high risk for COPD. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2020 Report proposed redefining the diagnosis of COPD based on environmental exposure, clinical symptoms, CT imaging, and spirometric criteria.4 Lancet Commission recommended a redefinition for COPD in 2019, which highlighted the importance of functional imaging as a quantitative structure for the early screening and diagnosis of COPD.5 Moreover, the latest GOLD COPD 2023 Report states that CT imaging is necessitated for the diagnosis and assessment of COPD.6 Based on quantitative CT and lung function parameters, our previous study corroborated that FEV1/FVC≥ 0.7 and FEV1% predicted value (FEV1% pre)< 72% are optimal classification criteria for high risk for COPD.7 The definition of populations at high risk for COPD is a premise for comprehending pulmonary micro-structural changes in these populations. Pathological manifestations of pulmonary vessels in early COPD and smokers include endothelial dysfunction, vasoconstriction, thick-walled vessels with a narrow lumen, and loss of micro-vasculature.8–10 In animal models, tobacco exposure induced early structural remodeling, which preceded emphysematous changes.11 In smokers at risk for COPD and mild COPD patients, perfusion deficits in peripheral small pulmonary vessels were observed on MRI images.12,13 However, the degree of damage to the pulmonary micro-vasculature in populations at high risk for COPD and smokers is unknown.
As is well documented, imaging findings can reflect pathologic changes in organs. In order to conduct a clinical intervention, it is necessary to identify pathological manifestations in populations at high risk for COPD. Small pulmonary vessels can be quantified non-invasively via computer-based image analysis of CT scans.14,15 Vessel pruning predominantly occurs in small pulmonary vessels below the pleura and is associated with low pulmonary perfusion.16 According to Cho YH et al, CT quantitative parameters of small pulmonary vessels below the pleura comprise the number of vessels, number of vessels with a cross-sectional area below 5 mm2, area of pulmonary vessels, and total surface area of pulmonary vessels at 6 mm~24 mm subpleura.17 In addition to the number and area of small pulmonary vessels, blood vessel volume in vessels with a cross-sectional area less than 5mm2 (BV5) represents the distribution of peripheral vessel volume. Furthermore, additional small pulmonary vessel quantitative parameters below the pleura were collected, and more information on adjustments in small pulmonary vessel structure was obtained.
According to the Three Major Chest Diseases Screening Study, low-dose chest CT scans were performed on urban community residents. Not only data on the number and area of small pulmonary vessels at 6 mm~24 mm depth from the pleural surface were retrieved, but also data on total blood volume (TBV) and peripheral pulmonary vascular volume were gathered from the CT quantitative analysis. We hypothesized that small pulmonary vessels are damaged in populations at high risk for COPD. Therefore, this study aimed to evaluate differences in the small pulmonary vessels of populations at high risk for COPD and smokers using multiple pulmonary vessels CT quantitative parameters.
Materials and Methods
Participants
A total of 1969 consecutive community residents were screened from August 2018 to December 2020 in our hospital. The subjects were all over 40 years of age. The inclusion criteria were as follows: 1) subjects with complete information regarding questionnaire survey results, PFT, and inspiratory phase CT scan; 2) All small pulmonary vessel parameters were collected by CT analysis. Exclusion criteria were: 1) subjects with incomplete clinical information; 2) subjects were unable to undergo PFT; 3) marked respiratory motion or metal artifact on CT images; 4) underlying lung diseases such as lung cancer, severe pulmonary interstitial fibrosis, and massive pulmonary infection, which may cause CT image not being analysed by software; 5) subjects who had a previous history of asthma. The study was approved by the institutional review board of Second Affiliated Hospital of Naval Medical University, Shanghai, China, and the study was registered in the Chinese Clinical Trials Registry (http://www.chictr.org.cn/index.aspx; ChiCTR2000035283). The study was conducted in accordance with the Declaration of Helsinki. All the subjects signed written informed consent for participating in this study.
Study Design
Questionnaire Survey
The questionnaire included subjects’ baseline information, including age, sex, weight, height, and history of smoking.
Pulmonary Function Test
All patients underwent PFT using a Multi-Functional Spirometer (HI-801 Chestgraph, CHEST M.I., Inc., Tokyo, Japan). Among 15 PFT parameters, FEV1/FVC and FEV1% predicted values were selected for this study. According to the GOLD guidelines and classification criteria for high risk for COPD populations in our previous study,7 all subjects were divided into three groups, namely the normal group with FEV1/FVC≥ 0.70 and FEV1% predicted value≥ 72%, group at high risk for COPD with FEV1/FVC≥ 0.70 and FEV1% predicted value< 72%, and COPD group with FEV1/FVC< 0.70.
CT Scanning
All patients underwent breath-hold training before the CT scan and were subsequently placed in the supine position with arms above the head. Non-contrast-enhanced volumetric chest CT scanning was performed at peak inspiration using a 256-slice CT scanner (Brilliance iCT, Philips Medical Systems, Netherlands) from the thoracic inlet to the diaphragm, respectively. The following CT scanning parameters were used: collimation 128×0.625 mm, tube energy 120 kV, Z-axial and 3D automatic tube current modulation, Doseright® collimator (Philips Healthcare), reduced dose level 3 (inspiratory /expiratory scanning), pitch 0.915, slice thickness 1 mm, slice increment 1 mm, Field of View (FOV) 350 mm*350 mm, matrix 512*512, and high and standard resolution algorithms.
Image Analysis
Image analysis was carried out by a thoracic radiologist with 2 decades of experience who was blinded to the patients’ clinical information and PFT results. The parameters of pulmonary small vessels were analyzed using commercial software (A-VIEW, Suhai Alderi Information Technology Ltd., Suzhou, China). Pulmonary vessels were automatically segmented, and parameters of pulmonary vessels were obtained on the inspiratory image, as illustrated in Figure 1. At 6 mm, 9 mm, 12 mm, 15 mm, 18 mm, 21 mm, and 24 mm depth from the pleural surface, parameters of pulmonary vessels consisted of the number of small pulmonary vessels (No. Vessels), number of pulmonary vessels with a cross-sectional area less than 5 mm2 (No. Vessels CSA< 5 mm2), surface area of low-attenuating-areas below −950 HU (Surface area of LAA), area of small pulmonary vessels (Vessel Area) and total surface area of small pulmonary vessels (Total Vessel Surface Area). Figure 2 displays the difference between the area and total surface area of small pulmonary vessels. The following parameters were also included: lung volume (LV), total blood volume (TBV), blood vessel volume in vessels with a cross-sectional area less than 1mm2 (BV1), blood vessel volume in vessels with a cross-sectional area less than 5mm2 (BV5), the ratio of BV1 to TBV (BV1/TBV), and the ratio of BV5 to TBV (BV5/TBV). Parameters were obtained at the levels of the whole lung.
 |
Figure 1 Extraction of pulmonary vessels based on low-dose CT images. (a) showed tracing pulmonary vessels from low-dose chest CT images. (b) showed extraction of pulmonary vessels. |
 |
Figure 2 Diagram of area and surface area of small pulmonary vessel. (A) represented the vascular surface area within the solid line. (B) represented the vascular area within the dashed line. |
Statistical Analysis
Statistical analyses were performed using SPSS 26.0 software (IBM SPSS Statistics, Armonk, NY, USA). Data were expressed as mean±standard deviation. Parameters among groups were compared using two-way ANOVA. Comparisons of categorical parameters between groups were evaluated using the chi-square test or rank sum test. A two-sided p-value< 0.05 was considered statistically significant.
Results
Differences in Demographic and Clinical Characteristics, PFT Parameters, and Cigarette Smoke Exposure Between the Normal, High Risk for COPD and COPD Groups
Among the 2333 community residents recruited, 364 subjects were excluded. 1968 subjects with available demographic and clinical characteristics, smoking history, PFT results, and pulmonary small vessel parameters were eligible for further analysis. Table 1 details the baseline characteristics of all included subjects. The proportion of males in the high risk for COPD and normal groups was significantly lower than those in the COPD group (P<0.001). On the other hand, the proportion of never-smokers in the high risk for COPD and normal groups were significantly higher than that in the COPD group (P<0.05). Besides, subjects in the group at high risk for COPD were significantly older than those in the normal and COPD groups (P<0.05). Nonetheless, BMI was comparable among the three groups (P=0.37).
 |
Table 1 Demographic and Clinical Characteristics and PFT Among Normal, High Risk for COPD and COPD Groups |
Differences in Parameters of Pulmonary Small Vessels at the Whole Lung Level Between the Normal, High Risk for COPD, and COPD Groups
The results revealed that No. Vessels, No. Vessels CSA< 5 mm2 and Total Vessel Surface Area at 6~12 mm subpleura, as well as LV, TBV, BV1, BV5, BV1/TBV and BV5/TBV, were significantly lower in subjects in the group at high risk for COPD than those in the normal group (P<0.05) (Table 2). Contrastingly, the surface area of LAA was comparable between the group at high risk for COPD and normal group (P>0.05) (Table 2). At 6 mm subpleura, No. Vessels and No. Vessels CSA< 5 mm2 were significantly lower in the COPD group compared with those in the normal group (P<0.05), but these parameters were significantly greater at 9 and 12 mm below pleura in patients in the COPD group compared with those in the normal group (P<0.05) (Table 2). Additionally, Total Vessel Surface Area at 6, 9, and 12 mm subpleura and LV, TBV, BV1 and BV5 were significantly higher in the COPD group than that in the normal group (P<0.05) (Table 2). Likewise, the Surface area of LAA at 6, 9, and 12 mm subpleura was significantly higher in the COPD group than that in the normal group (P<0.001) (Table 2). Differences in parameters of small pulmonary vessels at 15~24 mm among three groups are summarized in Supplementary Table 1. Figure 3 depicts the differences in small pulmonary vessel parameters between the normal, high risk for COPD, and COPD groups.
 |
Table 2 Differences in Parameters of Pulmonary Vessels Among Normal, High Risk for COPD and COPD Groups |
 |
Figure 3 Difference in small pulmonary vessel parameters among normal, high risk for COPD and COPD groups. No. Vessels and total vessel surface area at 6mm below pleura and BV5 (blood vessel volume in vessels with a cross-sectional area less than 5mm2) in high risk for COPD subjects were less than that in normal subjects (P<0.05). No. Vessels at 6mm below pleura in COPD subjects was less than that in normal subjects, but No. Vessels at 9mm below pleura in COPD subjects was more than that in normal subjects (P<0.05). Total vessel surface area at 6mm below pleura and BV5 (blood vessel volume in vessels with a cross-sectional area less than 5mm2) in COPD subjects were also more than that in normal subjects (P<0.05). |
Differences in Pulmonary Small Vessel Parameters Among Never-Smokers, Current Smokers, and Former Smokers in the Group at High Risk for COPD
No. Vessels, No. Vessels CSA< 5 mm2, Total Vessel Surface Area, Surface Area of LAA at 6~12 mm subpleura, LV, TBV, BV1 and BV5 in current smokers with high risk for COPD were significantly higher than those in never smokers with high risk for COPD (P<0.05) (Table 3). Similarly, No. Vessels, No. Vessels CSA< 5 mm2, Total Vessel Surface Area, Surface Area of LAA at 6~12 mm subpleura, LV, TBV, BV1, BV5, BV1/TBV and BV5/TBV were significantly higher in current smokers than those in never-smokers in the normal group (P<0.05) (Supplementary Table 2). It is worthwhile emphasizing that No. Vessels CSA< 5 mm2, Total Vessel Surface Area at 6~12 mm subpleura, and LV were significantly lower in former smokers with high risk for COPD than those in current smokers with high risk for COPD (P<0.05) (Table 3). Interestingly, the surface area of LAA was similar between the two groups (P>0.05) (Table 3). Lastly, there were no significant differences in any of the small pulmonary vessel parameters between current smokers with COPD and former smokers with COPD (P>0.05) (Supplementary Table 3). Figure 4 delineates the differences in TBV between never-smokers, current smokers, and former smokers.
 |
Table 3 Differences in Pulmonary Vessel Parameters Among Never-Smokers, Current-Smokers and Former-Smokers in Group at High Risk for COPD |
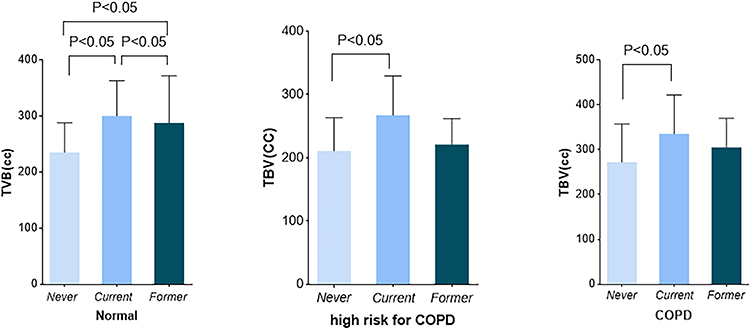 |
Figure 4 Total blood volume among subjects with different pulmonary function compared with smoking status. TBV (total blood volume) in never-smoker with high risk for COPD was less than that in current-smoker with high risk for COPD (P<0.05). This difference can also be seen in the normal and COPD subjects. Moreover, TBV in never-smokers with normal PFT (pulmonary function test) was less than that in current-smokers with normal PFT (P<0.05). |
Discussion
CT imaging can reflect aberrant lung micro-structural alterations and provide additional information on morphological changes. In this study, a reduction in the number, area, and volume of small pulmonary small vessels was noted in populations at high risk for COPD. The number, area, and volume of current smokers with high risk for COPD were higher than that of never smokers with high risk for COPD. And also, clinical intervention and proper treatment of populations at high risk for COPD may alleviate the damage in pulmonary vessels.
The prevalence of COPD increases with age. Indeed, there is a five-fold increased risk of COPD in patients aged over 65 years compared with patients under 40 years.18 Herein, all participants were community residents over 40 years old. The current study found that populations in the group at high risk for COPD were typically older than those in the normal and COPD groups. According to previous studies, the prevalence of COPD is higher in males, which is consistent with our findings. More importantly, the risk of developing COPD has been rapidly increasing among women, possibly because women appear to be more susceptible to the toxic effects of tobacco smoke than men. Tobacco smoking is an established risk factor for COPD. An earlier study concluded that approximately 50% of smokers eventually develop COPD.19 In addition, genetics, air pollutants, second-hand smoking, and environmental tobacco smoke are also risk factors for COPD.20 In our study, the proportion of smokers in the COPD group was higher than that in the normal group and the group at high risk for COPD. Furthermore, our study found that the proportion of non-smokers in the populations at high risk for COPD was 73.3%. This signified that smoking is not a determinant risk of COPD. Besides, some studies shown that BMI was closely associated with the incidence of COPD, low BMI was an important risk factor for the development of COPD, and a predictor for COPD severity.21–23 Being underweight might be related to malnutrition and/or low socioeconomic status, which are considered as environmental risk factors for COPD. BMI of COPD patients was significantly lower than that of non-COPD subjects.24 In this study, we found that no significant difference in BMI between the normal, high risk for COPD, and COPD groups. The following factors may contribute to this finding. All subjects in this study who were community residents came from economically-advanced city, good education, wealthy, great nutritional status and socioeconomic status and cognizance of exercise may contribute to the subgroups without BMI difference.
Occlusion and loss of pulmonary small vessels, thickening of pulmonary vascular walls and lumen narrowing, and reduced lung perfusion are the primary manifestations of pulmonary vascular remodeling.25–28 Muscularization in arterioles, smooth muscle cell proliferation, as well as elastin and collagen deposition promote the thickening of the vessel walls and is characterized by increased cross-sectional area and volume of small pulmonary vessels. Quantitative parameters of the vascular area and volume were higher in COPD patients than in healthy populations, as determined in this study. Although pulmonary vascular volumes were increased, the pulmonary blood flow may not have increased, as portrayed in functional MRI images, which exhibited distal lung perfusion defects in COPD patients.9 Emphysema and increased residual volume in COPD patients contributed to the increase in lung volume compared to the healthy population, which was in agreement with the observation of earlier studies. Previous studies also reported that the histologic evidence of small vascular loss was consistent with the pruning of distal pulmonary small vessels on CT images.13,29 The current study identified that COPD patients possessed a lower number of small vessels at 6 mm below the pleura and a higher number at 9 mm and above compared to the healthy population. Occlusion and absence of terminal pulmonary vessels resulted in increased blood flow in the proximal pulmonary vessels. With congestion and dilatation of vessels on the proximal side, more pulmonary vessels were captured on the CT scan, and more vessels were visualized on the images. Humbert M et al described that micro-vasculature pruning may suggest loss, narrowing, or reduced filling of smaller vessels or even proximal vessel dilation.30 Moreover, the pruning of vessels was associated with severity of pulmonary hypertension and an increase in right ventricular volume.31,32
CT imaging and post-processing techniques uncovered that morphological changes in small pulmonary vessels in populations at high risk for COPD were characterized by a decrease in the number, area, and volume of vessels compared to normal populations. To our knowledge, studies on pulmonary vascular changes in populations at high risk for COPD using multiple quantitative parameters are scarce. We speculated that the change in pulmonary small vessels in the populations at high risk for COPD might be associated with pulmonary vasoconstriction. For example, endothelial dysfunction leads to the generation of vasoconstricting and vasoproliferative agents and interferes with the effects of vasodilators.33 The effect of increased residual volume and emphysema on pulmonary vascular changes also needs to be considered. Increased emphysema can result in an increase in residual volume. Previous studies found that the percentage of cross-sectional area of vessels <5mm2 (%CSA <5) and BV5 was negatively correlated with LAA%-950 in COPD patients.14,34 It suggested that small peripheral pulmonary vessels were susceptible to emphysema leading to loss, narrowing, or decreased filling. The effects of asthma on the pulmonary vasculature cannot be ignored. In our study, the subjects at high risk for COPD may contain undiagnosed asthma populations. The changes of pulmonary vasculature are manifested by an increase in the number of small peripheral blood vessels and an increase in blood flow in asthma.35,36 Nevertheless, Small pulmonary vessel changes in COPD combined with asthma require more researches. Unexpectedly, the number, area, and volume of pulmonary vessels in the populations at high risk for COPD were not only lower than those in the normal populations but also lower than those in COPD patients. This observation signals that pulmonary vessel remodeling may not be as severe in populations at high risk for COPD as in COPD patients. Thus, adequate intervention and treatment may be more effective in promoting pulmonary vessel remodeling in populations at high risk for COPD relative to COPD patients. Park SW et al reported that the number of small pulmonary vessels was decreased during GOLD stage progression.37 Unlike their study, our study did not collect follow-up data on the subjects. What’s more, the paucity of animal models or vivo tissue tests for high risk for COPD impedes a comprehensive understanding of the pathological mechanisms underlying the decline in vessel number, area, and volume.
Quantitative parameters such as the number, area, and volume of small pulmonary vessels in current smokers with high risk for COPD were higher than those in never-smokers with high risk for COPD. The same results were observed in the normal population. Synn AJ et al demonstrated that current smokers had a higher pulmonary vascular volume compared with never-smokers.38 Interestingly, Aaron CP et al found that total pulmonary vascular volume was higher in former non-COPD smokers than that in non-COPD never smokers,39 in line with our results. There are several possible explanations for our findings with regard to the higher number, area, and volume in participants exposed to tobacco. To begin, carbon monoxide (a byproduct of tobacco combustion) facilitates vasodilation via nitric oxide-mediated mechanisms, which was validated in mouse models.40,41 Secondly, pulmonary surfactant is decreased during smoking, leading to increased surface tension, alveolar collapse, ventilation perfusion mismatches and hypoxemia. Increased vessel calibre as a result of negative pressure surrounding pulmonary capillaries and engorgement of blood capillaries. Thirdly, interstitial fibrosis, inflammation adjacent to pulmonary vessels or fluid filtration may be misclassified as being part of the vessel by the algorithm, a concern that was raised by Jacob J et al.42 Fourthly, as previously mentioned, the increase in volume and area of small pulmonary vessels may be attributed to vascular wall thickening, while blood flow was not increased. In our study, the number and area of small pulmonary vessels in current smokers with high risk for COPD were higher than in former smokers with high risk for COPD. We theorize that clinical management of populations at high risk for COPD may delay pulmonary vascular change. Takayanagi S et al claimed that management has a superior effect on pulmonary vasculature in early-stage COPD.3 In populations at high risk for COPD, remodeling of peripheral pulmonary vessels, including their distensibility in some degree, may be opposite to the impact of cumulative smoking burden on vessels. More studies of populations at high risk for COPD are necessary to confirm this hypothesis. And studies regarding the follow-up of populations at high risk for COPD and smokers are also essential. Follow-up of populations at high risk for COPD and smokers could help us to comprehend the dynamics change of pulmonary vessels and the impact of smoking cessation on change of pulmonary vessels.
There were several limitations to this study that cannot be overlooked. Firstly, this study was conducted at a single center using retrospective data, which may limit the generalization and applicability of our observations to other populations or regions. In addition, radiographic assessment of the small pulmonary vessel structure did not distinguish venous from arterial vessels. Pulmonary vein remodeling is observable in COPD patients, as evidenced by arterialization of the pulmonary vein wall and intimal fibrosis, and is positively correlated with pulmonary artery remodeling.43 It is reasonable to speculate that pulmonary venous remodeling also occurs in populations at high risk for COPD. Artificial intelligence techniques are paving the way for future studies to investigate differences in pulmonary arteriovenous remodeling in populations at high risk for COPD.44 All subjects in our study were from urban communities, and the majority of subjects were normal populations and populations at high risk for COPD. Given that this was a real-world study, the imbalance in the number of non-COPD and COPD subjects may have affected the accuracy of our results. Populations with previous history of asthma were excluded from this study, which may included people with undiagnosed asthma. More researches are needed about pulmonary vascular changes in populations with asthma-COPD overlap. In addition, further studies on longitudinal pulmonary vascular changes in populations at high risk for COPD and smokers are warranted.
Conclusion
Based on quantitative CT parameters, the number, area, and volume of small pulmonary vessels were decreased in the populations at high risk for COPD. The number, area, and volume of current smokers with high risk for COPD were higher than that of never smokers with high risk for COPD. And also, clinical management of populations at high risk for COPD, such as smoking cessation, may be effectively improve pulmonary vascular change in populations at high risk for COPD.
Abbreviations
COPD, chronic obstructive pulmonary disease; CT, computed tomography; PFT, pulmonary function test; GOLD, Global Initiative for Chronic Obstructive Lung Disease; FEV1% pre, FEV1% predicted value; No. Vessels, number of small pulmonary vessels; No. Vessels CSA< 5mm2, numbers of pulmonary vessels with a cross-sectional area less than 5 mm2; Surface Area of LAA, surface area of low-attenuating-areas below −950 HU; Vessel Area, area of small pulmonary vessels; Total Vessel Surface Area, total surface area of small pulmonary vessels; LV, lung volume; TBV, total blood volume; BV1, blood vessel volume in vessels with a cross-sectional area less than 1mm2; BV5, blood vessel volume in vessels with a cross-sectional area less than 5mm2.
Data Sharing Statement
The data will be available from the corresponding author on reasonable request.
Consent for Publication
The authors confirm that all the contents in this review can be published.
Acknowledgments
We greatly appreciate Ms. Qian He (Department of Statistics, Naval Medical University, Shanghai, China) for her assistance in statistical analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (grant numbers: 82171926, 81930049); National Key R&D Program of China (grant number: 2022YFC2010000, 2022YFC2010002, 2022YFC2010005); the program of Science and Technology Commission of Shanghai Municipality (grant number 21DZ2202600); the construction of CT standardized database for chronic obstructive pulmonary disease (grant number: YXFSC2022JJSJ002); Clinical Innovation Project of Shanghai Changzheng Hospital (grant number: 2020YLCYJ-Y24).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Soriano JB, Polverino F, Cosio BG. What is early COPD and why is it important? Eur Respir J. 2018;52(6):1801448. doi:10.1183/13993003.01448-2018
2. Jobst BJ, Weinheimer O, Buschulte T, et al. Longitudinal airway remodeling in active and past smokers in a lung cancer screening population. Eur Radiol. 2019;29(6):2968–2980. doi:10.1007/s00330-018-5890-4
3. Takayanagi S, Kawata N, Tada Y, et al. Longitudinal changes in structural abnormalities using MDCT in COPD: do the CT measurements of airway wall thickness and small pulmonary vessels change in parallel with emphysematous progression? Int J Chronic Obstr. 2017;12:551–560. doi:10.2147/COPD.S121405
4. Balkissoon R. Journal Club-COPD2020 Update. Global Initiative for Chronic Obstructive Lung Disease 2020 Report and the Journal of the COPD Foundation Special Edition, Moving to a New Definition for COPD: ”COPDGene® 2019”. Chronic Obstr Pulm Dis. 2019;6(4):64–72. doi:10.15326/jcopdf.7.1.2020.0133
5. Dransfield M, Stolz D, Kleinert S. Lancet COPD COMMISSIONERSTOWARDS eradication of chronic obstructive pulmonary disease: a lancet commission published correction appears in lancet. Lancet. 2019;393(10183):1786–1788. doi:10.1016/S0140-6736(19)30950-X
6. Venkatesan P. GOLD COPD report: 2023 update. Lancet Respir Med. 2023;11(1):18. doi:10.1016/S2213-2600(22)00494-5
7. Pu Y, Zhou X, Zhang D, et al. Re-defining high risk COPD with parameter response mapping based on machine learning models. Int J Chron Obstruct Pulmon Dis. 2022;17:2471–2483. doi:10.2147/COPD.S369904
8. Synn AJ, Li W, San José Estépar R, et al. Radiographic pulmonary vessel volume, lung function and airways disease in the Framingham Heart Study. Eur Respir J. 2019;54(3):1900408. doi:10.1183/13993003.00408-2019
9. Hueper K, Vogel-Claussen J, Parikh MA, et al. Pulmonary microvascular blood flow in mild chronic obstructive pulmonary disease and emphysema. the mesa COPD study. Am J Respir Crit Care Med. 2015;192(5):570–580. doi:10.1164/rccm.201411-2120OC
10. Santos S, Peinado VI, Ramírez J, et al. Characterization of pulmonary vascular remodelling in smokers and patients with mild COPD. Eur Respir J. 2002;19(4):632–638. doi:10.1183/09031936.02.00245902
11. Ferrer E, Peinado VI, Díez M, et al. Effects of cigarette smoke on endothelial function of pulmonary arteries in the Guinea pig. Respir Res. 2009;10(1):76. doi:10.1186/1465-9921-10-76
12. Fan L, Xia Y, Guan Y, et al. Capability of differentiating smokers with normal pulmonary function from COPD patients: a comparison of CT pulmonary volume analysis and MR perfusion imaging. Eur Radiol. 2013;23(5):1234–1241. doi:10.1007/s00330-012-2729-2
13. Xia Y, Guan Y, Fan L, et al. Dynamic contrast enhanced magnetic resonance perfusion imaging in high risk smokers and smoking-related COPD: correlations with pulmonary function tests and quantitative computed tomography. COPD. 2014;11(5):510–520. doi:10.3109/15412555.2014.948990
14. Estépar RS, Kinney GL, Black-Shinn JL, et al. Computed tomographic measures of pulmonary vascular morphology in smokers and their clinical implications. Am J Respir Crit Care Med. 2013;188(2):231–239. doi:10.1164/rccm.201301-0162OC
15. Jimborean G, Ianoși ES, Postolache P, et al. The role of quantitative computed tomography in the diagnosis of chronic obstructive pulmonary disease. Pneumologia. 2016;65(4):184–188.
16. Matsuoka S, Yamashiro T, Matsushita S, et al. Relationship between quantitative CT of pulmonary small vessels and pulmonary perfusion. AJR Am J Roentgenol. 2014;202(4):719–724. doi:10.2214/AJR.13.11027
17. Cho YH, Lee SM, Seo JB, et al. Quantitative assessment of pulmonary vascular alterations in chronic obstructive lung disease: associations with pulmonary function test and survival in the KOLD cohort. Eur J Radiol. 2018;108:276–282. doi:10.1016/j.ejrad.2018.09.013
18. Raherison C, Girodet PO. Epidemiology of COPD. Eur Respir Rev. 2009;18(114):213–221. doi:10.1183/09059180.00003609
19. Phillips AM. The influence of environmental factors in chronic bronchitis. J Occup Med. 1963;5:468–475.
20. Salvi S. Tobacco smoking and environmental risk factors for chronic obstructive pulmonary disease. Clin Chest Med. 2014;35(1):17–27. doi:10.1016/j.ccm.2013.09.011
21. Zhou Y, Wang D, Liu S, et al. The association between BMI and COPD: the results of two population-based studies in Guangzhou, China. COPD. 2013;10(5):567–572. doi:10.3109/15412555.2013.781579
22. Xiao YL, Li HY, Lin Y, et al. Prevalence of chronic obstructive pulmonary disease and associated risk factors. Chin J Behav Med Sci. 2005;14(9):786–787.
23. Jiang RG, Luo DS, Huang CP, Li WM. The prevalence of chronic obstructive pulmonary disease and correlated risk factors in the rural areas in Hubei province. Chin J Epidemiol. 2007;28(10):976–979.
24. Ran PX, Wang C, Yao WZ, et al. A study on the correlation of body mass index with chronic obstructive pulmonary disease and quality of life. Zhonghua Jie He He Hu Xi Za Zhi. 2007;30(1):18–22.
25. Berg K, Wright JL. The pathology of chronic obstructive pulmonary disease: progress in the 20th and 21st centuries. Arch Pathol Lab Med. 2016;140(12):1423–1428. doi:10.5858/arpa.2015-0455-RS
26. Tuder RM, Cool CD. Pulmonary arteries and microcirculation in COPD with pulmonary hypertension: bystander or culprit? Chest. 2019;156(1):4–6. doi:10.1016/j.chest.2019.04.100
27. Scarrow GD. The pulmonary angiogram in chronic bronchitis and emphysema. Proc R Soc Med. 1965;58(9):684–687. doi:10.1177/003591576505800907
28. Jacobson G, Turner AF, Balchum OJ, et al. Vascular changes in pulmonary emphysema. The radiologic evaluation by selective and peripheral pulmonary wedge angiography. Am J Roentgenol Radium Ther Nucl Med. 1967;100(2):374–396. doi:10.2214/ajr.100.2.374
29. Ohno Y, Yui M, Yoshikawa T, et al. 3D Oxygen-Enhanced MRI at 3T MR system: comparison with thin-section CT of quantitative capability for pulmonary functional loss assessment and clinical stage classification of COPD in smokers. J Magn Reson Imaging. 2021;53(4):1042–1051. doi:10.1002/jmri.27441
30. Humbert M, Guignabert C, Bonnet S, et al. Pathology and pathobiology of pulmonary hypertension: state of the art and research perspectives. Eur Respir J. 2019;53(1):1801887. doi:10.1183/13993003.01887-2018
31. Sakao S, Voelkel NF, Tatsumi K. The vascular bed in COPD: pulmonary hypertension and pulmonary vascular alterations. Eur Respir Rev. 2014;23(133):350–355. doi:10.1183/09059180.00007913
32. Washko GR, Nardelli P, Ash SY, et al. Arterial vascular pruning, right ventricular size, and clinical outcomes in chronic obstructive pulmonary disease. A longitudinal observational study. Am J Respir Crit Care Med. 2019;200(4):454–461. doi:10.1164/rccm.201811-2063OC
33. Wright JL, Levy RD, Churg A. Pulmonary hypertension in chronic obstructive pulmonary disease: current theories of pathogenesis and their implications for treatment. Thorax. 2005;60(7):605–609. doi:10.1136/thx.2005.042994
34. Mashimo S, Chubachi S, Tsutsumi A, et al. Relationship between diminution of small pulmonary vessels and emphysema in chronic obstructive pulmonary disease. Clin Imaging. 2017;46:85–90. doi:10.1016/j.clinimag.2017.07.008
35. Mandlik DS, Mandlik SK. New perspectives in bronchial asthma: pathological, immunological alterations, biological targets, and pharmacotherapy. Immunopharmacol Immunotoxicol. 2020;42(6):521–544. doi:10.1080/08923973.2020.1824238
36. Harkness LM, Kanabar V, Sharma HS, Westergren-Thorsson G, Larsson-Callerfelt AK. Pulmonary vascular changes in asthma and COPD. Pulm Pharmacol Ther. 2014;29(2):144–155. doi:10.1016/j.pupt.2014.09.003
37. Park SW, Lim MN, Kim WJ, et al. Quantitative assessment the longitudinal changes of pulmonary vascular counts in chronic obstructive pulmonary disease. Respir Res. 2022;23(1):29. doi:10.1186/s12931-022-01953-7
38. Synn AJ, Zhang C, Washko GR, et al. Cigarette smoke exposure and radiographic pulmonary vascular morphology in the Framingham Heart Study. Ann Am Thorac Soc. 2019;16(6):698–706. doi:10.1513/AnnalsATS.201811-795OC
39. Aaron CP, Hoffman EA, Lima JAC, et al. Pulmonary vascular volume, impaired left ventricular filling and dyspnea: the mesa lung study. PLoS One. 2017;12(4):e0176180. doi:10.1371/journal.pone.0176180
40. Seimetz M, Parajuli N, Pichl A, et al. Inducible NOS inhibition reverses tobacco-smoke-induced emphysema and pulmonary hypertension in mice. Cell. 2011;147(2):293–305. doi:10.1016/j.cell.2011.08.035
41. Thorup C, Jones CL, Gross SS, et al. Carbon monoxide induces vasodilation and nitric oxide release but suppresses endothelial NOS. Am J Physiol. 1999;277(6):F882–F889. doi:10.1152/ajprenal.1999.277.6.F882
42. Jacob J, Bartholmai BJ, Rajagopalan S, et al. Mortality prediction in idiopathic pulmonary fibrosis: evaluation of computer-based CT analysis with conventional severity measures. Eur Respir J. 2017;49(1):1601011. doi:10.1183/13993003.01011-2016
43. Andersen KH, Andersen CB, Gustafsson F, et al. Pulmonary venous remodeling in COPD-pulmonary hypertension and idiopathic pulmonary arterial hypertension. Pulm Circ. 2017;7(2):514–521. doi:10.1177/2045893217709762
44. Nardelli P, Jimenez-Carretero D, Bermejo-Pelaez D, et al. Pulmonary artery-vein classification in ct images using deep learning. IEEE Trans Med Imaging. 2018;37(11):2428–2440. doi:10.1109/TMI.2018.2833385
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.