")
Back to Journals » Infection and Drug Resistance » Volume 17
Ceftazidime-Avibactam Combination Therapy versus Monotherapy for the Treatment Carbapenem-Resistant Gram-Negative Bacterial Infections: A Retrospective Observational Study
Authors Li K, Li D, Dong H, Ren D, Gong D, Wang S, Li Y, Wu Y, Yang J, Yan W, Li Y
Received 14 December 2023
Accepted for publication 26 March 2024
Published 29 March 2024 Volume 2024:17 Pages 1281—1289
DOI https://doi.org/10.2147/IDR.S452805
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Keyang Li,1,* Debao Li,2,* Hongliang Dong,1 Dongmei Ren,2 Dandan Gong,1 Shubo Wang,1 Yang Li,1 Yuanyuan Wu,1 Jikang Yang,3 Wenjuan Yan,4 Yi Li4
1Department of Clinical Pharmacy, Jiaozuo People’s Hospital, Jiaozuo, Henan, People’s Republic of China; 2Department of Clinical Laboratory, Jiaozuo People’s Hospital, Jiaozuo, Henan, People’s Republic of China; 3Infectious Diseases Department, Jiaozuo People’s Hospital, Jiaozuo, Henan, People’s Republic of China; 4Department of Clinical Laboratory, Henan Provincial People’s Hospital, Zhengzhou, Henan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenjuan Yan; Yi Li, Department of Clinical Laboratory, Henan Provincial People’s Hospital, Weiwu Road 7#, Jinshui District, Zhengzhou, Henan, 450003, People’s Republic of China, Tel +86 15225061830 ; +86 15939039006, Email [email protected]; [email protected]
Purpose: Since the introduction of ceftazidime–avibactam (CZA) in the Chinese market, accumulating clinical evidence has substantiated its efficacy in the treatment of infections caused by carbapenem-resistant gram-negative bacteria (CR-GNB). Nevertheless, an ongoing debate persists concerning the choice between monotherapy and combination therapy when devising clinical anti-infection protocols.
Patients and Methods: This retrospective, single-center observational study enrolled patients with CR-GNB infections who received CZA treatment between December 2019 and August 2023. The primary outcome assessed was 30-day mortality, and the secondary outcome measured was 14-day bacterial clearance. A multivariate Cox regression model was used to identify variables that were independently associated with 30-day mortality rate.
Results: Eighty-three patients were enrolled in the study; of which, 45 received CZA monotherapy, whereas 38 received combination therapy. The overall 30-day mortality rate was 31.3%, and no significant difference was observed in the 30-day mortality rates between the CZA combination therapy and monotherapy groups (31.6% vs 31.1%, p=0.963). After adjustment by propensity score matching, the 30-day mortality rate was not significantly different between the two groups (28.6% vs 31.4%, p=0.794). Multivariate COX analysis revealed that age and SOFA score were independent predictors of 30-day mortality.
Conclusion: Combination therapy with CZA and other antimicrobials was not found to have an advantage over monotherapy in reducing the 30-day mortality rate.
Keywords: ceftazidime-avibactam, carbapenem-resistant gram-negative bacteria, combination therapy K. pneumoniae carbapenemase
Introduction
Multidrug-resistant gram-negative bacterial infections have persistently been among the most urgent challenges in the field of infectious diseases.1 Owing to limited antibiotic options and high mortality rates, infections caused by multidrug- and extensively drug-resistant gram-negative bacteria have become a major challenge for global health organizations.2,3 For decades, carbapenems have been the preferred choice for treating infections caused by these pathogens.4–7 However, the emergence and spread of carbapenemases threatens their efficacy as the last line of defense against multidrug-resistant bacteria.8,9 For domestic use, the most prevalent carbapenemases are Klebsiella pneumoniae carbapenemases (KPC),10 which belong to the Ambler class A enzymes and can hydrolyze all available traditional β-lactam antibiotics.
Ceftazidime-avibactam (CZA) is a novel combination of the cephalosporin antibiotic ceftazidime and non-β-lactam β-lactamase inhibitor avibactam. CZA exhibits broad activity against Ambler class A, C, and certain class D enzymes.11 It has been approved for treating complicated urinary tract and complicated intra-abdominal infections, including hospital-acquired and ventilator-associated pneumonia, as well as for gram-negative bacterial infections in adult patients with limited treatment options.12,13
Although there have been published reports of the clinical use of CZA in practical settings.14–19 The Infectious Diseases Society of America (IDSA) expert consensus released in 2023 recommends monotherapy for treating gram-negative bacteria that do not produce metalloenzymes,20 controversy exists regarding whether CZA should be used as a monotherapy or in combination with other antimicrobial agents in patients with carbapenem-resistant gram-negative bacterial (CR-GNB) infections in China.21 Therefore, we conducted a single-center retrospective analysis to investigate whether CZA combination therapy is more effective than CZA monotherapy for patients with CR-GNB and to evaluate the risk factors associated with mortality outcomes.
Materials and Methods
Study Design and Population
This was a single-center, retrospective, and observational study conducted at the People’s Hospital of Jiaozuo City, an 1800-bed tertiary care hospital in Jiaozuo, Henan, China, from December 1, 2019, to August 31, 2023. The included patients met the following criteria: 1) age ≥18 years at admission and 2) received CZA for > 72 h. The following patients were excluded from the analysis: (1) who received previous CZA treatment before the current study began, (2) who received empirical treatment with CZA, and (3) who had missing follow-up data. This study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of Jiaozuo People’s Hospital. The Ethics Committee waived the need for informed consent from patients because of the retrospective and anonymous nature of the study.
Data Collection and Definitions
For eligible patients, the baseline data comprised the following variables: demographic data; underlying diseases, including Charlson comorbidity index;22 clinical characteristics, including type of infection (according to CDC criteria),23 sepsis,24 and severity of illness at infection onset (SOFA,25 APACHE II);26 renal replacement therapy; source control; and the standard dose of 2.5 g CZA, administered intravenously every 8 h, with dose adjustments based on the recommended renal function in the product’s instructions. Each dose was administered for 2 h. The CZA treatment regimen, classified as a combination therapy, included at least one other antimicrobial agent administered for ≥ 72 h. The primary outcome was all-cause mortality within 30 days of treatment onset. The secondary outcome was the bacterial clearance within 14 days. Bacterial clearance was defined as the absence of target bacteria in subsequent cultures. All data were extracted from the electronic medical record information system. All data were anonymized.
Microbiological Methods
All pathogen isolations and antimicrobial susceptibility tests (excluding CZA) were conducted using a Vitek 2 Compact System (bioMérieux, Inc.). The susceptibility to CZA was determined using the disk diffusion (Kirby–Bauer) method. A diameter of inhibition zone ≥21 mm indicated susceptibility, whereas that ≤20 mm indicated resistance. The interpretation of all antibiotic susceptibility test results was based on the evaluation standards and breakpoints defined by the Clinical and Laboratory Standards Institute (CLSI) in 2019.27 For Enterobacterales, confirmatory MIC testing is indicated for isolates with zones of 20–22 mm to avoid reporting false-susceptible or false-resistant results. The MIC of CZA was determined using concentration gradient agar diffusion drug susceptibility strips (Etest, bioMérieux, France). Quality control strains ATCC 25922, ATCC 27853, ATCC BAA-1705, and ATCC BAA-2146 were purchased from the National Culture Collection Center, Rapid Detection of Carbapenemase Genotype. A colloidal gold enzyme immunochromatography (NG-Test CARBA 5) kit was purchased from Shanghai FosunPharma Co., Ltd.
Statistical Analysis
Statistical analyses were performed using the R software package (http://www.R-project.org, The R Foundation) and Empower-Stats (http://www.empowerstats.com, X&Y Solutions, Inc., Boston, MA, USA). Continuous variables were described using the median and interquartile range (IQR). Student’s t- or Mann–Whitney U-test was used to compare normally and non-normally distributed continuous variables. The chi-squared or Fisher’s exact test was used to compare categorical variables. Univariate logistic regression analysis was employed to evaluate the association between exposure variables, after which significant variables (p<0.05) were entered into the multivariate regression model to identify independent risk factors for mortality. Propensity score matching was performed to control for confounding variables, and the propensity score was estimated using a logistic regression model. In this study, a one-to-one nearest neighbor matching algorithm was adopted with a caliper width of 0.05. Variables adjusted for propensity score matching included age, APACHE II score, SOFA score, sepsis, pulmonary infection, and ICU stay before initiating CZA. A two-sided P value of <0.05 was considered statistically significant.
Results
Characteristics of Baseline and Microbiology
During the study, 121 patients prescribed CZA were assessed, and 83 patients were ultimately included in the analysis. The remaining 38 cases were excluded from the analysis due to the following reasons: CZA treatment duration ≤72 h (n=24), negative culture results (n=10), age <18 years (n=2), and loss to follow-up (n=2), as depicted in Figure 1.
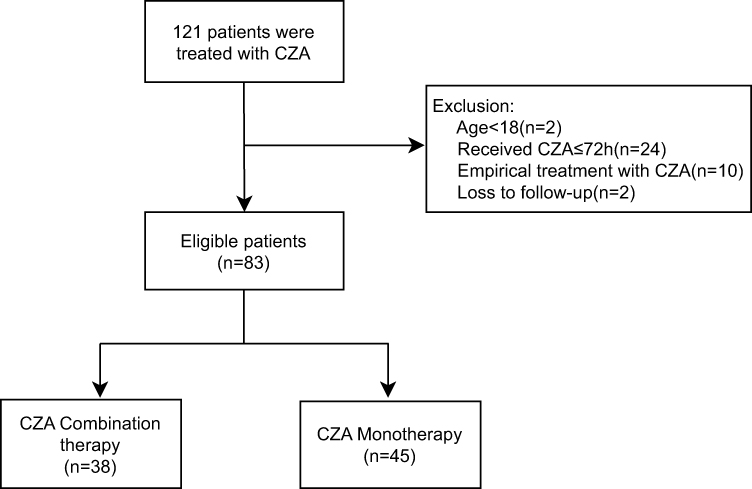 |
Figure 1 Study flow chart. Abbreviation: CZA, ceftazidime/avibactam. |
The patient characteristics following CZA treatment are compared in Table 1. There were 62 males (74.7%) and the mean ± standard deviation age was 64.2 ± 15.1 years, with no significant difference between the two groups. Most patients presented with comorbidities at admission, with hypertension and cerebrovascular disease being the most common. The median Charlson comorbidity index scores for the monotherapy and combination therapy groups were 3 (1–4) and 3 (1–4), respectively, with no differences between the two groups. The APACHE II scores were 20 (16–23) and 18.5 (15.25–23) for the two groups, whereas the SOFA scores were 5 (4–6) and 4 (3–7.5), with no significant differences between the groups. The incidence of sepsis (44.4% vs 57.9%, p=0.222) was lower in the CZA monotherapy group; however, the difference was not statistically significant.
 |
Table 1 Baseline Clinical Characteristics of Patients Treated with CZA |
In the overall study cohort, there were 54 cases of pulmonary infection (65.1%) and 20 cases of bloodstream infections (24.1%). Other infections included urinary tract, abdominal cavity, and catheter-related infections. The distribution of each type of infection was similar between the CZA combination and monotherapy groups.
The infecting microorganisms included K. pneumoniae, Pseudomonas aeruginosa, and Escherichia coli, none of which produce metallo-beta-lactamases. These cells were sensitive to CZA. A total of six cases of infection involving multiple gram-negative bacteria were observed, among which five were simultaneously infected with K. pneumoniae and P. aeruginosa and one was simultaneously infected with K. pneumoniae and E. coli. Additionally, there were 77 cases of infection involving a single gram-negative bacterium, with 75 cases infected with K. pneumoniae, 1 infected with P. aeruginosa, and 1 infected with E. coli (Table S1).
Treatment Regimens and Outcomes
In this cohort of 83 patients, 45 received CZA monotherapy and 38 received combination therapy. The median duration of CZA therapy was 7 days (6–10). The duration of treatment in the combination therapy group was 8.5 days (6–11.75), whereas that in the monotherapy group was 7 days (5–9). The duration of combination therapy was slightly longer than that of monotherapy; however, the difference was not statistically significant.
Regarding the primary outcome, there was no significant difference in the 30-day mortality rates between the CZA combination therapy and monotherapy groups (31.6% vs 31.1%, p=0.963). In addition, after adjusting for some variables using the propensity score matching between the two groups, we compared the outcome variables of the monotherapy group with those of the combination therapy group (Table 2) and found that the 30-day mortality rate of CZA treatment was not significantly different (31.4% vs 28.6%, p=0.794), and there was no statistical difference in the 14-day bacterial clearance rate (42.9% vs 42.9%, p=1.00).
 |
Table 2 Baseline Clinical Characteristics of Patients Treated with CZA After Adjustment |
Independent Predictors of Mortality
In the univariate analysis (Table 3), the following variables demonstrated significant associations with the 30-day mortality rate: the APACHE II score (p=<0.0001), age (p=0.007), sepsis (p<0.001), pulmonary infection (p=0.005), ICU stay before initiating CZA (p=0.024), duration of therapy (p=0.030), SOFA score (p<0.0001), CCI (p=0.007), vasoactive drug use (p<0.001), ICU stay positive (p=0.002), surgery history (p=0.048). In the multivariate COX regression analysis (Table 3), the SOFA score was identified as an independent predictor of 30-day mortality. The duration of therapy was an independent predictor of 30-day survival. After adjusting for propensity score matching, adjusted multivariate COX analysis showed that age and SOFA score were independent predictors of 30-day mortality (Table 4).
 |
Table 3 Univariate and Multivariate COX Regression Analysis Associated with 30-Day Mortality |
 |
Table 4 Univariate and Multivariate COX Regression Analysis Associated with 30-Day Mortality After Adjustment |
Discussion
Since its introduction into the Chinese market in 2019, CZA has been widely used for the clinical treatment of infections caused by CR-GNB. However, traditional viewpoints have led to the belief that combination therapy with two or more antibiotics is superior to monotherapy for the treatment of CR-GNBinfections.28–30 Consequently, the formulation of CZA-based treatment regimens is controversial in clinical practice. Therefore, this study aimed to compare the efficacy of CZA combination therapy with that of CZA monotherapy in patients with CR-GNB infections.
Our study found that CZA combination therapy is not superior to CZA monotherapy in reducing the 30-day mortality rate of patients. Considering the individual differences in illness severity between the CZA monotherapy and combination therapy groups, propensity score matching was conducted for indicators of illness severity and age. However, the results remain unchanged. This finding is consistent with those of previous studies. A meta-analysis of seven randomized controlled trials and six retrospective studies involving 503 patients found no difference in the mortality rates between patients receiving CZA monotherapy and those receiving combination therapy for CRE infections.31 In a recent large multicenter retrospective study involving 577 patients,14 the overall mortality rate did not decrease with combination therapy using active agents compared with monotherapy, even in severe cases associated with septic shock or a high mortality score. However, other studies reached conflicting conclusions. In a retrospective study by Zheng G et al,21 this study involving 62 critically ill patients, CZA combined with other in vitro non-susceptible antimicrobials, especially carbapenems, fosfomycin, and tigecycline, could significantly lower the mortality risk in critically ill patients with CRKP infection.
The mortality rate of patients with CR-GNB infections treated with CZA in this study cohort was 31.3%, which is similar to the previously reported results of CZA studies.32 Adjusted multivariate Cox regression survival analysis suggested that age and SOFA score were independent risk factors for 30-day mortality in patients with CR-GNB infections. This finding is consistent with those of previous studies.33,34 Some studies have shown that the duration of antimicrobial drug use may be a protective factor.35 In our study, this may be due to the small sample size, but it also reflects the fact that clinical symptoms improve during treatment, allowing for the continued use of antimicrobial drugs until the infection is under control.
This study has several limitations. First, this was a single-center study, and the sample size was insufficient. It is worth mentioning that this study included the largest number of patients compared to previous studies from China. Moreover, this was a retrospective cohort study that may have been subject to incomplete data and inclusion bias. Well-designed prospective studies or randomized controlled trials with larger sample sizes should be conducted. Furthermore, all infected patients underwent CZA susceptibility testing, and the clinical application of antibiotics may have been delayed by explicit antimicrobial susceptibility testing. Nevertheless, this is the most common route of administration in clinical practice.
Conclusion
In conclusion, our study showed that combination therapy with CZA and other antimicrobials was not associated with a better clinical or microbiological response. Given the potential toxicity associated with certain multi-drug regimens and the adverse effects resulting from the unnecessary use of antibiotics, the efficacy of CZA as monotherapy should not be overlooked.
Abbreviations
CR-GNB, carbapenem-resistant gram-negative bacteria; CRE, carbapenem-resistant Enterobacteriaceae; CRKP, carbapenem-resistant Klebsiella pneumoniae; CZA, ceftazidime–avibactam; APACHE, Apache Acute Physiology and Chronic Health Evaluation; SOFA, Sequential Organ Failure Assessment; HAP, hospital-acquired pneumonia; KPC, Klebsiella pneumoniae carbapenemase.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Review Board of Jiaozuo People’s Hospital (Number: 2023-007-K07).
Acknowledgments
We thank the hospital for its assistance with this study. We would like to thank Editage for English language editing.
Author Contributions
All the authors have read and approved the final version of the manuscript. All authors made a significant contribution to the work reported, whether that is in the study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; approved the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This work was supported by the Science and Technology Research Project of the Henan Province (LHGJ20230021). The funder had no role in the study design, data collection and interpretation, or decision to submit the work for publication.
Disclosure
The authors report no conflicts of interest related to this work.
References
1. Jean SS, Harnod D, Hsueh PR. Global threat of carbapenem-resistant gram-negative bacteria. Front Cell Infect Microbiol. 2022;12:823684. doi:10.3389/fcimb.2022.823684
2. Babiker A, Clarke LG, Saul M, Gealey JA, Clancy CJ, Nguyen MH. Changing epidemiology and decreased mortality associated with carbapenem-resistant gram-negative bacteria, 2000–2017. Clin Infect Dis. 2021;73(11):e4521–e4530. doi:10.1093/cid/ciaa1464
3. Tangden T, Ramos MV, Felton TW, et al. The role of infection models and PK/PD modelling for optimising care of critically ill patients with severe infections. Intensive Care Med. 2017;43(7):1021–1032. doi:10.1007/s00134-017-4780-6
4. Doi Y, Bonomo RA, Hooper DC, et al. Gram-negative bacterial infections: research priorities, accomplishments, and future directions of the antibacterial resistance leadership group. Clin Infect Dis. 2017;64(suppl_1):S30–S35. doi:10.1093/cid/ciw829
5. Shein AMS, Hongsing P, Abe S, et al. Will there ever be cure for chronic, life-changing colistin-resistant Klebsiella pneumoniae in urinary tract infection? Front Med. 2021;8:806849. doi:10.3389/fmed.2021.806849
6. Shein AMS, Wannigama DL, Higgins PG, et al. High prevalence of mgrB-mediated colistin resistance among carbapenem-resistant Klebsiella pneumoniae is associated with biofilm formation, and can be overcome by colistin-EDTA combination therapy. Sci Rep. 2022;12(1):12939. doi:10.1038/s41598-022-17083-5
7. Shein AMS, Wannigama DL, Higgins PG, et al. Novel colistin-EDTA combination for successful eradication of colistin-resistant Klebsiella pneumoniae catheter-related biofilm infections. Sci Rep. 2021;11(1):21676. doi:10.1038/s41598-021-01052-5
8. Chen J, Liang Q, Ding S, et al. Ceftazidime-avibactam for the treatment of carbapenem-resistant pseudomonas aeruginosa infection in lung transplant recipients. Infect Drug Resist. 2023;16:2237–2246. doi:10.2147/IDR.S407515
9. Durante-Mangoni E, Andini R, Zampino R. Management of carbapenem-resistant Enterobacteriaceae infections. Clin Microbiol Infect. 2019;25(8):943–950. doi:10.1016/j.cmi.2019.04.013
10. Zhang Y, Wang Q, Yin Y, et al. Epidemiology of carbapenem-resistant enterobacteriaceae infections: report from the China CRE network. Antimicrob Agents Chemother. 2018;62(2):2. doi:10.1128/AAC.01882-17
11. Shirley M. Ceftazidime-avibactam: a review in the treatment of serious gram-negative bacterial infections. Drugs. 2018;78(6):675–692. doi:10.1007/s40265-018-0902-x
12. Mazuski JE, Gasink LB, Armstrong J, et al. Efficacy and safety of ceftazidime-avibactam plus metronidazole versus meropenem in the treatment of complicated intra-abdominal infection: results from a randomized, controlled, double-blind, Phase 3 program. Clin Infect Dis. 2016;62(11):1380–1389. doi:10.1093/cid/ciw133
13. Torres A, Zhong N, Pachl J, et al. Ceftazidime-avibactam versus meropenem in nosocomial pneumonia, including ventilator-associated pneumonia (REPROVE): a randomized, double-blind, phase 3 non-inferiority trial. Lancet Infect Dis. 2018;18(3):285–295. doi:10.1016/S1473-3099(17)30747-8
14. Tumbarello M, Raffaelli F, Giannella M, et al. Ceftazidime-Avibactam use for klebsiella pneumoniae carbapenemase-producing K. Pneumoniae infections: a retrospective observational multicenter study. Clin Infect Dis. 2021;73(9):1664–1676. doi:10.1093/cid/ciab176
15. Zhu X, Wang H, Guo K, et al. Chinese journal of integrated traditional and western medicine in intensive and critical care. Chin J TCM WM Crit Care. 2022;29(3):284–287.
16. Zhen S, Wang H, Feng S. Update of clinical application in ceftazidime-avibactam for multidrug-resistant Gram-negative bacteria infections. Infection. 2022;50(6):1409–1423. doi:10.1007/s15010-022-01876-x
17. Vena A, Giacobbe DR, Castaldo N, et al. Clinical experience with ceftazidime-avibactam for the treatment of infections due to multidrug-resistant gram-negative bacteria other than carbapenem-resistant enterobacterales. Antibiotics. 2020;9(2):71. doi:10.3390/antibiotics9020071
18. Shein AMS, Wannigama DL, Hurst C, et al. Novel intranasal phage-CaEDTA-ceftazidime/avibactam triple combination therapy demonstrates remarkable efficacy in treating Pseudomonas aeruginosa lung infection. Biomed. Pharmacother. 2023;168:115793. doi:10.1016/j.biopha.2023.115793
19. Wannigama DL, Sithu Shein AM, Hurst C, et al. Ca-EDTA restores the activity of ceftazidime-avibactam or aztreonam against carbapenemase-producing Klebsiella pneumoniae infections. iScience. 2023;26(7):107215. doi:10.1016/j.isci.2023.107215
20. Tamma PD, Aitken SL, Bonomo RA, et al. Infectious Diseases Society of America 2022 Guidance on the Treatment of Extended-Spectrum β-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clin Infect Dis. 2022;75(2):187–212. doi:10.1093/cid/ciac268
21. Zheng G, Zhang J, Wang B, et al. Ceftazidime-avibactam in combination with in vitro non-susceptible antimicrobials versus ceftazidime-avibactam in monotherapy in critically ill patients with carbapenem-resistant klebsiella pneumoniae infection: a retrospective cohort study. Infect Dis Ther. 2021;10(3):1699–1713. doi:10.1007/s40121-021-00479-7
22. Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
23. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of healthcare-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36(5):309–332. doi:10.1016/j.ajic.2008.03.002
24. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
25. Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22(7):707–710. doi:10.1007/BF01709751
26. Knaus WA, Draper EA, Wagner DP, et al. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–829. doi:10.1097/00003246-198510000-00009
27. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial- susceptibility testing; 2019, M100–M129.
28. Alexander EL, Loutit J, Tumbarello M, et al. Carbapenem-resistant Enterobacteriaceae infections: results from a retrospective series and implications for the design of prospective clinical trials. Open Forum Infect Dis. 2017;4:ofx063.
29. Daikos GL, Tsaousi S, Tzouvelekis LS, et al. Carbapenemase-producing Klebsiella pneumoniae bloodstream infections: lowering mortality by antibiotic combination schemes and the role of carbapenems. Antimicrob Agents Chemother. 2014;58(4):2322–2328. doi:10.1128/AAC.02166-13
30. Tzouvelekis LS, Markogiannakis A, Piperaki E, et al. Treating infections caused by carbapenemase-producing Enterobacteriaceae. Clin Microbiol Infect. 2014;20(9):862–872. doi:10.1111/1469-0691.12697
31. Fiore M, Alfieri A, Di Franco S, et al. Ceftazidime-avibactam combination therapy compared to ceftazidime-avibactam monotherapy for the treatment of severe infections due to carbapenem-resistant pathogens: a systematic review and network meta-analysis. Antibiotics. 2020;9(7):388. doi:10.3390/antibiotics9070388
32. Balandin B, Ballesteros D, Pintado V, et al. Multicentre study of ceftazidime/avibactam for Gram-negative bacteria infections in critically ill patients. Int J Antimicrob Agents. 2022;59(3):106536. doi:10.1016/j.ijantimicag.2022.106536
33. Tumbarello M, Trecarichi EM, Corona A, et al. Efficacy of ceftazidime-avibactam salvage therapy in patients with infections caused by klebsiella pneumoniae carbapenemase-producing K. pneumoniae. Clin Infect Dis. 2019;68(3):355–364. doi:10.1093/cid/ciy492
34. Blot S, Antonelli M, Arvaniti K, et al.; Abdominal Sepsis Study (AbSeS) group on behalf of the Trials Group of the European Society of Intensive Care Medicine. Epidemiology of intra-abdominal infection and sepsis in critically ill patients: ”AbSeS”, a multinational observational cohort study and ESICM Trials Group Project. Intensive Care Med. 2019;45(12):1703–1717. doi:10.1007/s00134-019-05819-3
35. Chen J, Liang Q, Chen X, et al. Ceftazidime-avibactam versus polymyxin b in the challenge of carbapenem-resistant pseudomonas aeruginosa infection. Infect Drug Resist. 2022;15:655–667. doi:10.2147/IDR.S350976
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.