")
Back to Journals » Nature and Science of Sleep » Volume 16
Associations Between Repetitive Negative Thinking and Objective and Subjective Sleep Health in Cognitively Healthy Older Adults
Authors Munns LB , Demnitz-King H , André C , Rehel S, Ourry V, de La Sayette V, Vivien D, Chételat G, Rauchs G , Marchant NL
Received 18 October 2023
Accepted for publication 10 January 2024
Published 5 March 2024 Volume 2024:16 Pages 233—245
DOI https://doi.org/10.2147/NSS.S441509
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Lydia B Munns,1,2,* Harriet Demnitz-King,1,* Claire André,3 Stéphane Rehel,3 Valentin Ourry,3 Vincent de La Sayette,4 Denis Vivien,3,5 Gaël Chételat,3 Géraldine Rauchs,3,* Natalie L Marchant1,* On behalf of the Medit-Ageing Research Group
1Division of Psychiatry, University College London, London, UK; 2Department of Psychology, York University, York, UK; 3Normandie Univ, UNICAEN, INSERM, U1237, Physiopathology and Imaging of Neurological Disorders (PhIND), Neuropresage Team, GIP Cyceron, Caen, France; 4Service de Neurologie, CHU de Caen-Normandie, Caen, France; 5Département de Recherche Clinique, CHU Caen-Normandie, Caen, France
*These authors contributed equally to this work
Correspondence: Natalie L Marchant, Division of Psychiatry, University College London, London, UK, Email [email protected] Lydia B Munns, Department of Psychology, York University, York, United Kingdom, Email [email protected]
Objective: Poor sleep and high levels of repetitive negative thinking (RNT), including future-directed (ie, worry) and past-directed (ie, brooding) negative thoughts, have been associated with markers of dementia risk. The relationship between RNT and sleep health in older adults is unknown. This study aimed to investigate this association and its specificities including multiple dimensions of objective and subjective sleep.
Methods: This study used a cross sectional quantitative design with baseline data from 127 cognitively healthy older adults (mean age 69.4 ± 3.8 years; 63% female) who took part in the Age-Well clinical trial, France. RNT (ie, worry and brooding) levels were measured using the Penn State Worry Questionnaire and the Rumination Response Scale (brooding subscale). Polysomnography was used to assess sleep objectively, and the Pittsburgh Sleep Quality Index and the St. Mary’s Hospital Sleep Questionnaire were used to measure sleep subjectively. In primary analyses the associations between RNT and sleep (ie, objective sleep duration, fragmentation and efficiency and subjective sleep disturbance) were assessed via adjusted regressions.
Results: Higher levels of RNT were associated with poorer objective sleep efficiency (worry: β=− 0.32, p< 0.001; brooding: β=− 0.26, p=0.002), but not objective sleep duration, fragmentation, or subjective sleep disturbance. Additional analyses, however, revealed differences in levels of worry between those with short, compared with typical and long objective sleep durations (p < 0.05).
Conclusion: In cognitively healthy older adults, RNT was associated with sleep characteristics that have been implicated in increased dementia risk. It will take additional research to ascertain the causal link between RNT and sleep characteristics and how they ultimately relate to the risk of developing dementia.
Keywords: perseverative cognition, rumination, sleep, anxiety, ageing
Introduction
Sleep health among older adults has been widely implicated in the maintenance of physical and mental health, while poor sleep health has emerged as a significant contributor to depression, cognitive impairment and Alzheimer’s disease pathology, the primary cause of dementia.1–3 Therefore, improved understanding of factors that may contribute to sleep health in older adults is important for healthy ageing/preventative approaches.
In assessing the various facets of sleep health, polysomnography emerges as the gold standard for objectively evaluating sleep patterns.4 Sleep regularity, levels of alertness and sleepiness, sleep efficiency, duration and timing have been identified as domains that represent habitual sleep health characteristics.5,6 This multifaceted view of sleep health suggests that multiple sleep characteristics can be present concurrently, irrespective of the presence of sleep disorders.6 Spira and colleagues suggest that poor sleep may be a prodromal feature of cognitive decline and dementia, whilst healthy sleep helps to maintain brain integrity.7 As well as being an early symptom of dementia,8 poor sleep, particularly short sleep duration, has been highlighted as a risk factor for pathological brain changes.9 In addition to sleep duration, other sleep characteristics most strongly associated with dementia risk include objectively measured sleep fragmentation (awakenings during sleep), sleep efficiency (ratio between time spent asleep and time in bed), sleep latency (reflecting easiness or difficulties falling asleep), and subjectively assessed sleep quality.7,10–14 Sleep efficiency in particular is an important sleep characteristic to consider, as this incorporates multiple sleep metrics, including sleep latency, the length of sleep awakenings and sleep duration, and therefore provides a more holistic way of quantifying sleep health. Particular sleep stages, such as slow wave sleep (SWS) and rapid eye movement (REM) sleep, as well as sleep disorders such as sleep-disordered breathing (or sleep apnoea), have also been implicated in poorer cognitive performance and increased dementia risk due to their associations with dementia biomarkers.15–17 Further to associations with dementia, poor levels of subjective sleep quality and objective sleep fragmentation, as well as alterations in REM sleep stages have been implicated in psychiatric disorders among older adults, including depression.3,18
Another risk factor implicated in a variety of neurodegenerative and psychiatric disorders includes repetitive negative thinking (RNT), a recurrent negatively focused thinking process that is perceived as difficult to control.19 RNT is a cognitive process that encompasses both past-directed negative thoughts (ie, brooding, a maladaptive form of rumination) and future-directed negative thoughts (ie, worry), which relates to negative affect20 and has been implicated in the development and maintenance of depression and anxiety disorders, respectively.21
RNT has also been associated with objective and subjective cognitive performance and decline, amyloid and tau deposition, and accelerated brain ageing in older adults.22–26 While there is substantiating evidence supporting the correlation between RNT and biomarkers associated with Alzheimer’s disease, the specific interplay between its two components—namely, worry and rumination (brooding) — remains less evident. This is due to previous literature assessing RNT more broadly via the Perseverative Thinking Questionnaire (PTQ), or exclusively investigating either worry or rumination. Therefore, exploring the individual contributions of worry and rumination on other risk factors for dementia and psychological disorders, such as sleep, would be valuable.
Prior studies involving elderly individuals have frequently employed a comprehensive RNT metric, such as the Reflective Thinking Scale (RTS), or have concentrated solely on either apprehension or reflective thought. To attain a more thorough comprehension of the association between RNT and the risk of cognitive decline, undertaking inquiries that concurrently scrutinize both constituents within the same participant pool would be advantageous. Such an approach would facilitate a more intricate examination of the unique contributions of apprehension and reflective thought to outcomes related to Alzheimer’s disease.
Both sleep and RNT have been independently associated with a range of mental, physical and neurological disorders, and they are also associated with each other.14 A large meta-analysis of studies that assessed the relationship between RNT and sleep characteristics found small to medium associations between high levels of RNT and poorer sleep quality, shorter sleep duration and longer sleep onset latency.14 The majority of studies within this meta-analysis however, included young and middle-aged samples, and few included both objective and subjective sleep measurements. Indeed, despite both objective and subjective sleep measures being associated with disorders such as depression and dementia risk, the coherence between the two is often low when assessed in older adults.27 It remains unknown why coherence is low, but one explanation may be that they often assess different time periods. Further, one might anticipate that RNT could also help explain these inconsistencies, as RNT may have different strengths of association with subjective and objective sleep individually. Alternatively, it has been suggested that objective and subjective sleep are arguably two different outcomes and therefore it is important to consider both when exploring the relationship between sleep and RNT.14 Considering this, alongside the importance of sleep health for the physical and mental health of older adults,1–3 there is an important gap in the literature surrounding perseverative cognition and the levels of both objective and subjective sleep among older adults.
The current study addressed this gap in the research by investigating the cross-sectional association between RNT (ie, worry and brooding) and a range of objective and subjective sleep health measures in community-dwelling cognitively healthy older adults. Specifically, higher worry and brooding levels were hypothesised to be associated with poorer objective sleep efficiency, increased sleep fragmentation, reduced sleep duration, and worse subjective sleep quality – all of which have been associated with RNT in younger-aged cohorts, as well as depression, Alzheimer’s disease biomarkers and dementia risk.3,14,28–30 No specific hypotheses were made in relation to other measures of sleep health and were thus considered exploratory analyses. Further, we also assessed the coherence between objective and subjective sleep measurements collected over the same one-night period and examined whether RNT influenced the coherence. Gaining a better understanding of the relationship between RNT and sleep among older adults will allow us to have a better idea of how these factors work together to contribute to the development and progression of mental and neurological disorders in this population and can help us identify potential therapeutic interventions to improve overall mental and neurological health outcomes for older adults.
Methods
Participants
Baseline data from 135 cognitively healthy older adults enrolled in the Age-Well randomised clinical trial were eligible for inclusion. The Age-Well trial aimed to evaluate a meditation-based intervention designed to enhance mental health and well-being in elderly individuals. Age-Well was designed with the capability to identify, when comparing the meditation vs passive control arms of the trial, an effect size of 0.75 concerning the volume and perfusion of the anterior cingulate cortex and insula. The study was powered with 80% statistical power and a two-sided type I error of 1.25%. Consequently, the minimum required sample size was determined to be 126 participants, which has been exceeded with 135 participants. In adherence to guidance,31 we did not conduct post-hoc power analyses for this secondary outcome study. All participants were recruited from the general population, at least 65 years old, native French speakers, retired for at least 1 year, received a minimum of 7 years of education, and performed within the normal range for age and educational levels on standardised cognitive tests of a neuropsychological diagnostic battery, including measures of global cognitive functioning, executive functions, and verbal episodic memory. Participants underwent a medical interview with a physician and completed a diagnostic test battery to verify criteria. Detailed eligibility criteria have previously been described.32
The Age-Well clinical trial was approved by local ethics committees (CPP Nord-Ouest III, Caen; trial registration number: EudraCT:2016–002441-36; IDRCB:2016-A01767-44), in full compliance with the principles of the Declaration of Helsinki and was registered on ClinicalTrials.gov (NCT02977819). All participants provided written informed consent prior to participation.
Repetitive Negative Thinking
The Penn State Worry Questionnaire
Worry was assessed via the 16-item Penn State Worry Questionnaire (PSWQ).33 Participants were asked to indicate how typical statements are for them on a 5-point Likert scale ranging from 1 (not at all typical of me) to 5 (very typical of me). A total score is calculated by summing the first 11 items and the reverse-scores of the latter five items, with global scores ranging from 16 to 80 (higher scores representing greater worry). The psychometric properties of the PSWQ have been examined in older adults, where it has demonstrated excellent internal consistency and adequate convergent validity in individuals with Generalised Anxiety Disorder and those without psychiatric diagnoses.34 Additionally, the PSWQ has demonstrated clear divergent validity with measures of anxiety and depression, suggesting that these measure different concepts.35
Rumination Response Scale - Brooding Sub-Scale
Participants completed the full 22-item Rumination Response Scale (RRS), with scores from the 5-item brooding subscale used to assess brooding levels.36 Participants were asked to respond to items assessing the frequency of thoughts on a scale ranging from 1 (almost never) to 4 (almost always). Scores can range from 5 to 20, with higher scores representing a greater degree of brooding. The brooding subscale of the RRS has been found to have strong convergent and predictive validity and good internal consistency in older adults.37
Sleep
Polysomnography
All participants underwent a polysomnography (PSG) at home using a portable device (Siesta®, Compumedics, Australia) as previously described.38 The PSG involved using multiple measurement instruments, as described in previous research.39 This included an electroencephalogram (EEG), an electrooculogram (EOG) an electromyogram (EMG) and an oximeter to measure oxygen saturation. Recordings from the EEG were visually scored by experts in 30-second epochs according to the scoring rules of the American Academy of Sleep Medicine.40 Standard sleep parameters were computed, including sleep duration, sleep fragmentation (the number of awakenings), sleep efficiency, sleep latency and the proportion of time spent in each sleep stage (relative to total sleep time) were computed, as well as respiratory parameters such as the apnoea-hypopnea index (AHI), an index used to indicate the severity of sleep apnoea. Eighty-seven individuals (69%) underwent 2 polysomnography recordings, including a habituation night. Data from the second night was used.
Pittsburgh Sleep Quality Index
The Pittsburgh Sleep Quality Index (PSQI)41 is a 19-item questionnaire that assesses subjective sleep quality and disturbances over the previous 4 weeks. It assesses 7 different components of sleep (ie, subjective sleep disturbance, sleep latency, sleep duration, sleep efficiency, sleep fragmentation, use of sleeping medication, and daytime dysfunction) which are coded categorically from 0 to 3. A global score, with a range from 0 to 21, is created by summing each of the 7 sub-components. Higher scores on each of the sub-components and global score are indicative of worse sleep. Continuous data are also gathered for sleep duration, sleep efficiency, and sleep latency, and in this study were used as continuous variables instead of their categorical equivalents.
St Mary’s Hospital Sleep Questionnaire
The St Mary’s Hospital Sleep Questionnaire is a 14-item self-report questionnaire that records information about sleep latency, duration, and efficiency from the previous night’s sleep.42 This questionnaire was administered the morning after the polysomnography night.
Statistical Analyses
To determine associations between RNT and objective and subjective sleep measures, we performed a series of regression models, with worry and brooding as independent predictors and each sleep measure as a dependent variable. Linear regressions were conducted for continuous outcomes (ie, objective sleep measures: duration, efficiency, fragmentation, latency, % REM sleep, % Slow Wave Sleep (SWS) and subjective sleep measures from the PSQI: duration, efficiency, latency and total PSQI score). Categorical variables (ie, subjective sleep measures from the PSQI: disturbance, fragmentation, and daytime dysfunction) were first converted to binary outcomes by merging bins with the lowest count with their nearest neighbour, and then analysed using logistic regressions). Subjective sleep measures using the PSQI were used as they gathered information on sleep over the past 4 weeks making it more comparable to the Penn State Worry Questionnaire and the Rumination Response scale compared to the St Mary’s Hospital Sleep Questionnaire which only measures sleep over the past 24 hours. All analyses adjusted for age, sex, and AHI. The covariates age and AHI were included as continuous variables, and sex as a categorical variable. Primary analyses (ie, objective sleep fragmentation, efficiency, and duration, and subjective sleep disturbance) were controlled for multiple comparisons using a Bonferroni correction (ie, 0.05/4 = 0.0125).
Due to literature suggesting an inverted U-shaped (ie, non-linear) association between sleep duration and cognitive decline2 additional analyses were conducted to investigate whether levels of RNT differed between individuals with short, typical, and long sleep durations. A tertial split was used to classify participants into different sleep duration categories based on their objective polysomnography-derived sleep measurements, with participants in the highest tertile classified as long sleepers, participants in the lowest tertile short sleepers, and the middle tertile as typical sleepers. ANCOVA’s, adjusted for age, sex, and AHI, were conducted to investigate differences between RNT levels and sleep duration. Games-Howell post-hoc tests were used due to heterogeneity of variance between tertile groups.
Linear regressions were conducted to examine the association between objective (assessed via polysomnography) and subjective sleep (assessed via the St Mary’s Hospital Sleep questionnaire), as both measured the same night’s sleep, along with the difference statistics to ascertain whether participants were more prone to over or under-estimate their sleep behaviours. Only continuous variables of sleep measured in both objective and subjective assessments were analysable (ie, sleep latency, sleep duration and sleep efficiency). The difference score was calculated by subtracting the subjective score from the objective score for each of these outcomes. Linear regressions were then used to investigate whether levels of RNT predicted any discrepancy between objective and subjective sleep.
Stata (version 17.0) and JupyterLab (version 3.5.0) were used to analyse data and standardised betas (βs) are reported throughout. Figures were created in Python (version 3.8.15).
Results
Participant Characteristics
Demographic characteristics are provided in Table 1. Of the 135 participants, 8 were missing AHI data, thus the current study reports results from a maximum of 127 participants across primary and exploratory analyses.
 |
Table 1 Demographic and Clinical Baseline Data (N=127) |
Being female was associated with lower levels of objective sleep fragmentation (p<0.001) and higher levels of SWS (p=0.018), REM sleep (p=0.048), objective sleep efficiency (p=0.014), objective sleep duration (p=0.002) and subjective sleep disturbance (p=0.034). AHI was positively associated with objective sleep fragmentation (p=0.003), and negatively associated with objective sleep measures including proportion of REM sleep (p=0.001) and SWS (p=0.001), and total sleep duration (p=0.03). Age was not associated with any objective or subjective sleep characteristic. Neither worry nor brooding were associated with any covariate (ie, age, sex or AHI).
Associations Between RNT and Sleep Measure Variables
Results from primary analyses assessing the relationship between RNT and objective (sleep duration, efficiency, and fragmentation) and subjective (sleep disturbance) sleep measures are described below and presented in Table 2.
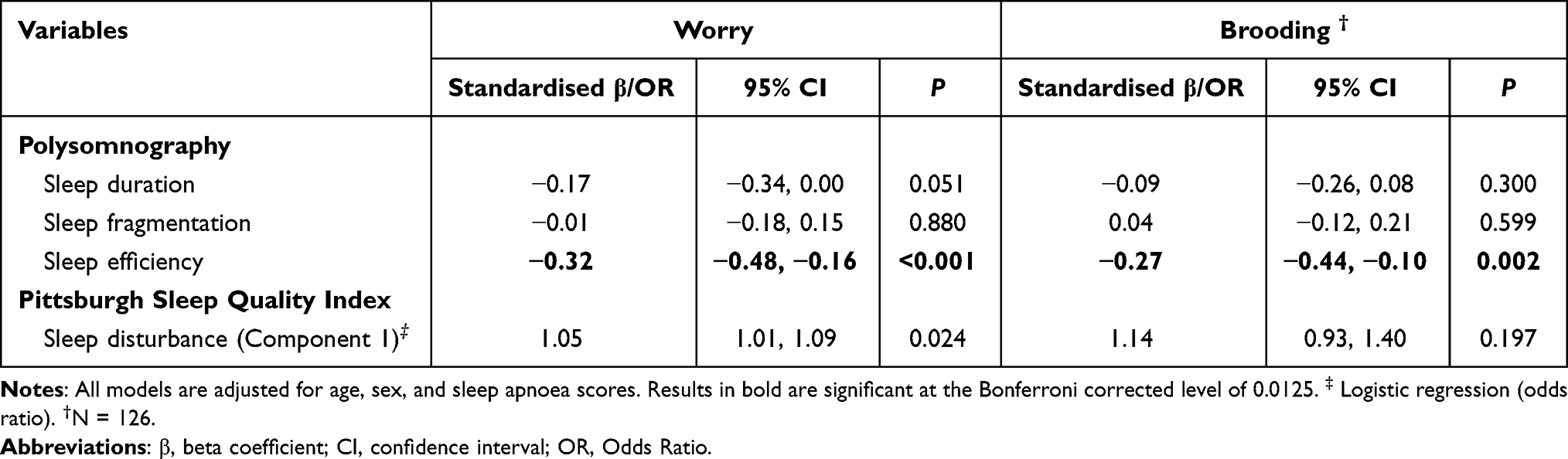 |
Table 2 Primary Analysis Results Examining the Relationship Between Worry and Brooding and Sleep Health (N=127) |
Higher levels of RNT were associated with worse objective sleep efficiency (worry: β=−0.32, 95% CI: −0.48 to −0.16, p<0.001; brooding: β=−0.27, 95% CI: −0.44 to −0.10, p=0.002), but there was no evidence of an association between RNT and objective sleep fragmentation (worry: p=0.880; brooding: p=0.598), or objective sleep duration (worry: p=0.050; brooding: p=0.300). Associations with subjective sleep disturbance did not survive corrections for multiple comparisons (worry: p=0.025; brooding: p=0.058). However, in analyses assessing the association between RNT and different sleep duration categories (ie, short, typical, or long) associations emerged with worry (F[2, 124]=7.03, p=0.001) and not brooding (F[2, 123]=2.68, p=0.073). Post-hoc analyses were then run for both worry and brooding. Worry levels in the short sleep duration group (M = 47.0, SD = 12.3) were significantly higher than in the typical (M = 38.6, SD = 9.1) and long (M = 39.8, SD = 11.4) sleep duration groups (p=0.002, p=0.018 respectively). Worry levels did not differ between typical and long sleep duration groups. No significant differences in levels of brooding were found between sleep duration groups. Figure 1 shows the associations between RNT and categorical sleep durations and Supplementary Table 1 contains means and standard deviations of RNT scores by sleep duration.
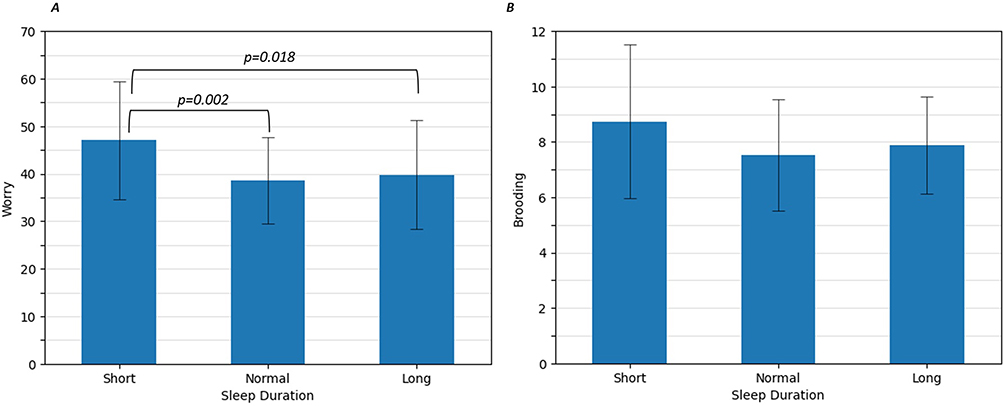 |
Figure 1 Associations between RNT and categorical sleep duration: short, typical, and long. (A) Worry and sleep duration, and (B) brooding and sleep duration. Mean and standard deviations shown. |
Exploratory Analyses
Positive associations were observed between RNT and the global PSQI score (worry: β=0.23, 95% CI: 0.07 to 0.40, p=0.007; brooding: β=0.21, 95% CI: 0.04 to 0.38, p=0.018). Further, positive associations were observed between brooding and subjective daytime dysfunction (β=1.30, 95% CI: 1.09 to 1.54; p=0.003) and subjective sleep latency (β=0.18, 95% CI: 0.00 to 0.35, p=0.049). No other associations were observed (Table 3).
 |
Table 3 Exploratory Analysis Results Examining the Relationship Between Worry and Brooding and Sleep Health (N=127) |
Coherence Between Subjective and Objective Sleep Measures
Positive associations were observed between subjective and objective measures of sleep efficiency (r(108)=0.22, p<0.001), duration (r(108)=0.23, p<0.001), and latency (r(112)=0.07, p=0.019).
Sleep Duration
The mean difference between objectively and subjectively assessed sleep duration was 36.5 minutes (SD=119.2). On average participants perceived that they had 36.5 minutes less sleep than that was recorded via polysomnography. This discrepancy was not predicted by RNT (worry: p=0.412; brooding: p=0.822).
Sleep Efficiency
The mean difference between objectively and subjectively assessed sleep efficiency was 9.5% (SD=19.8), suggesting that on average participants believed that their sleep was less efficient than objective measures had recorded. This discrepancy was not predicted by RNT (worry: p=0.944; brooding: p=0.558).
Sleep Latency
The mean difference between objectively and subjectively assessed sleep latency was −23.3 minutes (SD=43.7), suggesting that on average participants estimated that they took more time to fall asleep than objective measures had recorded. The discrepancy was not predicted by RNT (worry: p=0.877; brooding: p=0.319).
Discussion
The current study sought to better understand the association between RNT (ie, worry and brooding) and components of sleep health known to be associated with increased dementia risk in cognitively healthy older adults. Higher levels of RNT (ie, both worry and brooding) were associated with lower objective sleep efficiency. Although there was no evidence of a linear relationship between RNT and sleep duration, participants with shorter sleep durations had significantly higher levels of worry compared to those with typical or long sleep durations. These findings partially align with the cognitive debt hypothesis by showing that RNT is associated with some sleep characteristics that have previously been associated with dementia risk.43
The associations found between RNT and sleep health could be potentially explained by biological mechanisms. Chronic worry, for example, can dysregulate the hypothalamus-pituitary adrenal (HPA) axis, which can impact the secretion of cortisol and other stress related hormones.44 The presence of increased stress hormones has been associated with disruptions in the sleep cycle and overall sleep quality in older adults.45
Sleep efficiency is one metric by which sleep health can be assessed. Since both worry and brooding were exclusively linked to sleep efficiency, our findings may imply that sleep efficiency is the most important metric of sleep health in relation to cognitive debt. This could be attributed to the fact that sleep efficiency encompasses various sleep metrics, making it a potentially more sensitive indicator of overall sleep health. Sleep regularity, levels of alertness and sleepiness, sleep efficiency, duration and timing have been identified as domains that represent habitual sleep health characteristics.5,6 This multifaceted view of sleep health suggests that multiple sleep characteristics can be present concurrently, irrespective of the presence of sleep disorders.6
A nonlinear relationship between RNT and sleep duration may exist - RNT, particularly worry, was associated with short sleep duration when assessed categorically, rather than continuously. While both categorically-defined short and long sleep durations have been associated with cognitive decline,2 here we observed that worry was only associated with one segment of that inverted-u shaped curve. It may be that the causes of short and long sleep duration are different; worry being one mechanism to explain short sleep duration, with other factor(s) driving longer sleep duration (comorbidities, for example). Interestingly, levels of brooding were not found to differ significantly depending on sleep duration. This could be explained methodologically by the rather more limited range of responses on the brooding subscale, or that worry has been found to be more predictive of both depression and anxiety than rumination,46 which have both been consistently associated with poorer sleep health47 and with dementia risk.48,49
Due to the cross-sectional design of the current study the direction of the association between RNT and sleep health, however, remains unclear. For instance, RNT could negatively impact sleep health, poor sleep health could cause increased levels of RNT, a third factor could influence both (ie, prodromal dementia) or indeed as recent evidence suggests, there could be bidirectional feedback loop.50 Looking further into potential explanations for associations between sleep and RNT more generally, executive function (ie, the ability to plan, focus attention and concentrate)51 and emotional regulation (ie, the ability to appropriately respond to a range of emotions)52 may play important roles. Cox and colleagues investigated these potential mechanisms and reported that insomnia levels in community-dwelling adults influenced change in RNT over a three-month period via an indirect effect of executive functioning on emotional regulation.53 Further, another study found that sleep disturbance was not associated with levels of rumination in older adults with higher inhibitory control, suggesting that inhibitory control, a component of executive function, may play a mediating role between sleep and RNT.54 Based on our and others’ findings, interventions such as meditation, that target cognitive control and/or emotion regulation may be particularly suited to improve sleep health and reduce RNT. Future research could investigate the benefits of such nonpharmacological interventions to reduce RNT and improve sleep outcomes among older adults. The use of nonpharmacological interventions is particularly important among older adults, who are often on multiple medications, in order to avoid side effects and negative drug-interactions.
The coherence between subjective and objective sleep measures was examined by utilising polysomnography metrics and data from a sleep questionnaire collected the following morning. Small but significant associations were observed, unlike previous research,27 which may be due to our method of assessment (using subjective and objective data collected in close temporal proximity). This may explain why previous research that assessed objective and subjective sleep over different time periods has often failed to observe associations between the two.27 We hypothesised that RNT might have impacted the results as previous research suggests that worry and brooding are more closely associated with subjective measures of sleep disturbance than objective measures.14 However, we did not observe stronger RNT associations with subjective sleep measures, and discrepancies between objective and subjective measures were not affected by levels of RNT. This suggests that worry and brooding did not influence a person’s ability to accurately assess their sleep.
Other factors may therefore explain the disparity between subjective and objective sleep measures. Factors such as age, sleep apnoea, physical health, and cognitive performance have been found to influence time perception and assessment of sleep duration.55–57 This could explain why the current results contradict previous research among younger adults, where worry was found to impact the association between objective and subjective sleep.58 These factors, alongside individual differences in levels of self-awareness and understanding of sleep,59 are likely to influence subjective sleep scores.
Strengths and Limitations
The current study has several strengths. It fills in an important gap in the research by investigating the association between RNT and sleep health in a well-characterised sample of older adults. Further, the combination of both subjective and objective sleep measurements meant in-depth data could be gathered on both physiological characteristics and individual’s perception of sleep, including a questionnaire which allowed subjective and objective sleep to be assessed over the same period. Similarly, including assessments of two forms of RNT (ie, worry and brooding), allowed us to determine their distinct and overlapping relationships with markers of sleep, to the best of our knowledge, for the first time in older adults. The fact that their associations were largely consistent across all outcomes supports the shift towards a transdiagnostic approach to the assessment of negative thinking styles.46 Finally, due to the comprehensive data collected, covariates including age, sex and sleep apnoea were able to be considered, which ensures any associations found were not influenced by these factors which have previously been associated with sleep, Alzheimer’s disease biomarkers and/or dementia risk.17,60,61
However, the cross-sectional data used in this research precludes the determination of causality between RNT and sleep health, or their influence on cognitive trajectory and dementia incidence. Secondly, the current study only examined a single night of polysomnography and not all participants benefited from a habituation night, therefore outcomes may not reflect habitual sleep in every participant given that some people may find it difficult to sleep while wearing the polysomnography device. Further to this, measuring the consistency between subjective and objective sleep data was only assessed over one night. To address these limitations, future research could employ longitudinal designs to better understand the temporal dynamics and potential causal links between RNT, sleep health, and cognitive outcomes. Incorporating multiple nights of polysomnography or with validated wearable devices would also ensure a more comprehensive assessment of habitual sleep patterns which could allow for a more robust investigation into the consistency between subjective and objective sleep measurements.
Implications and Conclusions
Findings from this study show an association between sleep and RNT, clustering two emerging psychological risk factors for dementia, which is important given that prevention is an important channel for dementia management.62 Further research is needed to determine the causal relationship between these variables to identify which could be a promising risk factor to target for dementia prevention strategies.
The identification of factors that delay the onset of dementia may help combat the large and rapidly increasing public health challenge that this syndrome presents. Although it is not known whether RNT and sleep health are causal pathways to dementia risk, or whether they are prodromal symptoms, these results suggest that they are avenues worth exploring in future research, especially since both RNT and sleep are modifiable via nonpharmacological interventions.63,64 The clinical implications of this research extend beyond the mere observation of associations, urging a proactive and multi-faceted approach toward dementia prevention. By identifying and addressing modifiable risk factors, clinicians, researchers and policymakers can contribute to the collective effort to delay the onset of dementia and mitigate its impact on public health.
Data Sharing Statement
Data is available on request following a formal data sharing agreement and approval by the consortium and executive committee. The data sharing request form can be downloaded at https://silversantestudy.eu/2020/09/25/data-sharing/.
Ethics Approval
The Age-Well clinical trial was approved by local ethics committees (CPP Nord-Ouest III, Caen; trial registration number: EudraCT: 2016-002441-36; IDRCB: 2016-A01767-44). The Age-Well clinical trial was conducted in full compliance with the principles of the Declaration of Helsinki.
Clinical Trial Registration
Age-Well was registered on ClinicalTrials.gov (NCT02977819).
Sponsor and Grant Number
The Age-Well randomised controlled trial was sponsored by the Institut National de la Santé et de la Recherche Médicale (Inserm), and is part of the Medit-Ageing project funded through the European Union in Horizon 2020 program related to the call PHC22 Promoting Mental Well-Being in the Ageing Population and under grant agreement No. 667696.
Medit-Ageing Research Group
Florence Allais, Sebastian Baez Lugo, Alexandre Bejanin, Pierre Champetier, Léa Chauveau, Anne Chocat, Fabienne Collette, Sebastian Czajko, Sophie Dautricourt, Robin De Flores, Marion Delarue, Séverine Fauvel, Francesca Felisatti, Eglantine Ferrand Devouge, Antoine Garnier-Crussard, Julie Gonneaud, Sacha Haudry, Oriane Hébert, Frank Jessen, Olga Klimecki, Pierre Krolak-Salmon, Elizabeth Kuhn, Brigitte Landeau, Antoine Lutz, Valérie Lefranc, Sara Martinez, Florence Mezenge, Laurence Michel, José Luis Molinuevo, Inès Moulinet, Cassandre Palix, Géraldine Poisnel, Stefano Poletti, Anne Quillard, Florence Requier, Eric Salmon, Corinne Schimmer, Marco Schlosser, Clémence Tomadesso, Edelweiss Touron, Anne-Laure Turpin, Patrik Vuilleumier, Tim Whitfield and Miranka Wirth.
This research was orally presented in June 2022 at the Alzheimer’s Disease International Conference, London, to conference attendees.
Acknowledgments
Lydia B Munns and Harriet Demnitz-King are co-first authors for this study. Géraldine Rauchs and Natalie L Marchant are co-senior authors for this study. We are also grateful to all the participants of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
N.L. Marchant and G. Chételat report a grant from European Union’s Horizon 2020 research and innovation programme (grant 667696). N.L. Marchant was supported by a Senior Fellowship from the Alzheimer’s Society (AS-SF-15b-002). The authors report no other conflicts of interest in this work.
References
1. Kent BA, Feldman HH, Nygaard HB. Sleep and its regulation: an emerging pathogenic and treatment frontier in Alzheimer’s disease. Prog Neurobiol. 2021;197:101902. doi:10.1016/j.pneurobio.2020.101902
2. Yaffe K, Falvey CM, Hoang T. Connections between sleep and cognition in older adults. Lancet Neurol. 2014;13(10):1017–1028. doi:10.1016/S1474-4422(14)70172-3
3. Maglione JE, Ancoli-Israel S, Peters KW, et al. Depressive Symptoms and Subjective and Objective Sleep in Community-Dwelling Older Women. J Am Geriatr Soc. 2012;60(4):635–643. doi:10.1111/j.1532-5415.2012.03908.x
4. Kline CE. Polysomnography. In: Gellman MD editor. Encyclopedia of Behavioral Medicine. Springer International Publishing; 2020:1700–1704. doi:10.1007/978-3-030-39903-0_825
5. Wallace ML, Yu L, Buysse DJ, et al. Multidimensional sleep health domains in older men and women: an actigraphy factor analysis. Sleep. 2021;44(2):zsaa181. doi:10.1093/sleep/zsaa181
6. Buysse DJ. Sleep Health: can We Define It? Does It Matter? Sleep. 2014;37(1):9–17. doi:10.5665/sleep.3298
7. Spira AP, Chen-Edinboro LP, Wu MN, Yaffe K. Impact of Sleep on the Risk of Cognitive Decline and Dementia. Curr Opin Psychiatry. 2014;27(6):478–483. doi:10.1097/YCO.0000000000000106
8. Mander BA. Local Sleep and Alzheimer’s Disease Pathophysiology. Front Neurosci. 2020;14. doi:10.3389/fnins.2020.525970
9. Sabia S, Fayosse A, Dumurgier J, et al. Association of sleep duration in middle and old age with incidence of dementia. Nat Commun. 2021;12(1):2289. doi:10.1038/s41467-021-22354-2
10. Lim ASP, Kowgier M, Yu L, Buchman AS, Bennett DA. Sleep Fragmentation and the Risk of Incident Alzheimer’s Disease and Cognitive Decline in Older Persons. Sleep. 2013;36(7):1027–1032. doi:10.5665/sleep.2802
11. Jee HJ, Shin W, Jung HJ, Kim B, Lee BK, Jung YS. Impact of Sleep Disorder as a Risk Factor for Dementia in Men and Women. Biomol Ther. 2020;28(1):58–73. doi:10.4062/biomolther.2019.192
12. Branger P, Arenaza-Urquijo EM, Tomadesso C, et al. Relationships between sleep quality and brain volume, metabolism, and amyloid deposition in late adulthood. Neurobiol Aging. 2016;41:107–114. doi:10.1016/j.neurobiolaging.2016.02.009
13. Brown BM, Rainey-Smith SR, Villemagne VL, et al. The Relationship between Sleep Quality and Brain Amyloid Burden. Sleep. 2016;39(5):1063–1068. doi:10.5665/sleep.5756
14. Clancy F, Prestwich A, Caperon L, Tsipa A, O’Connor DB. The association between worry and rumination with sleep in non-clinical populations: a systematic review and meta-analysis. Health Psychol Rev. 2020;14(4):427–448. doi:10.1080/17437199.2019.1700819
15. Lee YF, Gerashchenko D, Timofeev I, Bacskai BJ, Kastanenka KV. Slow Wave Sleep Is a Promising Intervention Target for Alzheimer’s Disease. Front Neurosci. 2020;14. doi:10.3389/fnins.2020.00705
16. Azami H, Moguilner S, Penagos H, et al. EEG Entropy in REM Sleep as a Physiologic Biomarker in Early Clinical Stages of Alzheimer’s Disease. J Alzheimer's Dis. 2023;91(4):1557–1572. doi:10.3233/JAD-221152
17. Liguori C, Maestri M, Spanetta M, et al. Sleep-disordered breathing and the risk of Alzheimer’s disease. Sleep Med Rev. 2021;55:101375. doi:10.1016/j.smrv.2020.101375
18. Hoyos CM, Gordon C, Terpening Z, et al. Circadian rhythm and sleep alterations in older people with lifetime depression: a case-control study. BMC Psychiatry. 2020;20(1):192. doi:10.1186/s12888-020-02606-z
19. Ehring T, Zetsche U, Weidacker K, Wahl K, Schönfeld S, Ehlers A. The Perseverative Thinking Questionnaire (PTQ): validation of a content-independent measure of repetitive negative thinking. J Behav Ther Exp Psychiatry. 2011;42(2):225–232. doi:10.1016/j.jbtep.2010.12.003
20. Trick L, Watkins E, Dickens C. The association between perseverative negative cognitive processes and negative affect in people with long term conditions: a protocol for systematic review and meta-analysis. Syst Rev. 2014;3(1):5. doi:10.1186/2046-4053-3-5
21. Espinosa F, Martin-Romero N, Sanchez-Lopez A. Repetitive Negative Thinking Processes Account for Gender Differences in Depression and Anxiety During Adolescence. Int J Cogn Ther. 2022;15(2):115–133. doi:10.1007/s41811-022-00133-1
22. Schlosser M, Demnitz-King H, Whitfield T, Wirth M, Marchant NL. Repetitive negative thinking is associated with subjective cognitive decline in older adults: a cross-sectional study. BMC Psychiatry. 2020;20(1):500. doi:10.1186/s12888-020-02884-7
23. de Vito A, Calamia M, Greening S, Roye S. The association of anxiety, depression, and worry symptoms on cognitive performance in older adults. Aging Neuropsychol Cogn. 2019;26(2):161–173. doi:10.1080/13825585.2017.1416057
24. Marchant NL, Lovland LR, Jones R, et al. Repetitive negative thinking is associated with amyloid, tau, and cognitive decline. Alzheimer's Dement. 2020;16(7):1054–1064. doi:10.1002/alz.12116
25. Schwarz C, Lange C, Benson GS, et al. Severity of Subjective Cognitive Complaints and Worries in Older Adults Are Associated With Cerebral Amyloid-β Load. Front Aging Neurosci. 2021:13. doi:10.3389/fnagi.2021.675583
26. Karim HT, Ly M, Yu G, et al. Aging faster: worry and rumination in late life are associated with greater brain age. Neurobiol Aging. 2021;101:13–21. doi:10.1016/j.neurobiolaging.2021.01.009
27. Landry G, Best J, Liu-Ambrose T. Measuring sleep quality in older adults: a comparison using subjective and objective methods. Front Aging Neurosci. 2015;7. doi:10.3389/fnagi.2015.00166
28. Shi L, Chen SJ, Ma MY, et al. Sleep disturbances increase the risk of dementia: a systematic review and meta-analysis. Sleep Med Rev. 2018;40:4–16. doi:10.1016/j.smrv.2017.06.010
29. Min ZD, Zhang C, Yang Y, et al. The relationship between sleep efficiency and clinical symptoms is mediated by brain function in major depressive disorder. J Affect Disord. 2020;266:327–337. doi:10.1016/j.jad.2020.01.155
30. Ouyang P, Sun W. Depression and sleep duration: findings from middle-aged and elderly people in China. Public Health. 2019;166:148–154. doi:10.1016/j.puhe.2018.10.007
31. Zhang Y, Hedo R, Rivera A, Rull R, Richardson S, Tu X. Post hoc power analysis: is it an informative and meaningful analysis? Gen Psychiatry. 2019;
32. Poisnel G, Arenaza-Urquijo E, Collette F, et al. The Age-Well randomized controlled trial of the Medit-Ageing European project: effect of meditation or foreign language training on brain and mental health in older adults. Alzheimer's Dement Transl Res Clin Interv. 2018;4:714–723. doi:10.1016/j.trci.2018.10.011
33. Meyer TJ, Miller ML, Metzger RL, Borkovec TD. Development and validation of the Penn State Worry Questionnaire. Behav Res Ther. 1990;28(6):487–495. doi:10.1016/0005-7967(90)90135-6
34. Beck JG, Stanley MA, Zebb BJ. Psychometric properties of the Penn State Worry Questionnaire in older adults. J Clin Geropsychol. 1995;1(1):33–42.
35. Wuthrich VM, Johnco C, Knight A. Comparison of the Penn State Worry Questionnaire (PSWQ) and abbreviated version (PSWQ-A) in a clinical and non-clinical population of older adults. J Anxiety Disord. 2014;28(7):657–663. doi:10.1016/j.janxdis.2014.07.005
36. Nolen-Hoeksema S, Morrow J. A prospective study of depression and posttraumatic stress symptoms after a natural disaster: the 1989 Loma Prieta earthquake. J Pers Soc Psychol. 1991;61:115–121. doi:10.1037/0022-3514.61.1.115
37. Townshend K, Hajhashemi K. Ruminative Response Scale (RRS). In: Medvedev ON, Krägeloh CU, Siegert RJ, Singh NN editors. Handbook of Assessment in Mindfulness Research. Springer International Publishing; 2022:1–19. doi:10.1007/978-3-030-77644-2_84-1
38. André C, Rehel S, Kuhn E, et al. Association of Sleep-Disordered Breathing With Alzheimer Disease Biomarkers in Community-Dwelling Older Adults: a Secondary Analysis of a Randomized Clinical Trial. JAMA Neurol. 2020;77(6):716–724. doi:10.1001/jamaneurol.2020.0311
39. Duivon M, Perrier J, Segura-Djezzar C, et al. Sleep-dependent memory consolidation in breast cancer: use of a virtual reality prospective memory task. Front Neurosci. 2022;16:908268. doi:10.3389/fnins.2022.908268
40. Berry RB, Brooks R, Gamaldo C, et al. AASM Scoring Manual Updates for 2017 (Version 2.4). J Clin Sleep Med JCSM off Publ Am Acad Sleep Med. 2017;13(5):665–666. doi:10.5664/jcsm.6576
41. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
42. Ellis BW, Johns MW, Lancaster R, Raptopoulos P, Angelopoulos N, Priest RG. The St. Mary’s Hospital Sleep Questionnaire: a Study of Reliability. Sleep. 1981;4(1):93–97. doi:10.1093/sleep/4.1.93
43. Marchant NL, Howard RJ. Cognitive Debt and Alzheimer’s Disease. J Alzheimer's Dis. 2015;44(3):755–770. doi:10.3233/JAD-141515
44. Hannibal KE, Bishop MD. Chronic Stress, Cortisol Dysfunction, and Pain: a Psychoneuroendocrine Rationale for Stress Management in Pain Rehabilitation. Phys Ther. 2014;94(12):1816–1825. doi:10.2522/ptj.20130597
45. Morgan E, Schumm LP, McClintock M, Waite L, Lauderdale DS. Sleep Characteristics and Daytime Cortisol Levels in Older Adults. Sleep. 2017;40(5):zsx043. doi:10.1093/sleep/zsx043
46. Hoyer J, Gloster AT, Herzberg PY. Is worry different from rumination? Yes, it is more predictive of psychopathology! GMS Psycho-Soc-Med. 2009;
47. Alvaro PK, Roberts RM, Harris JK. A Systematic Review Assessing Bidirectionality between Sleep Disturbances, Anxiety, and Depression. Sleep. 2013;36(7):1059–1068. doi:10.5665/sleep.2810
48. Byers AL, Yaffe K. Depression and risk of developing dementia. Nat Rev Neurol. 2011;7(6):323–331. doi:10.1038/nrneurol.2011.60
49. Gimson A, Schlosser M, Huntley JD, Marchant NL. Support for midlife anxiety diagnosis as an independent risk factor for dementia: a systematic review. BMJ Open. 2018;8(4):e019399. doi:10.1136/bmjopen-2017-019399
50. Nota JA, Coles ME. Duration and Timing of Sleep are Associated with Repetitive Negative Thinking. Cogn Ther Res. 2015;39(2):253–261. doi:10.1007/s10608-014-9651-7
51. Burgess P, Simons J. Theories of frontal lobe executive function: clinical applications. Eff Rehabil Cogn Deficits. 2005;211–231. doi:10.1093/acprof:oso/9780198526544.003.0018
52. Bjureberg J, Ljótsson B, Tull MT, et al. Development and Validation of a Brief Version of the Difficulties in Emotion Regulation Scale: the DERS-16. J Psychopathol Behav Assess. 2016;38(2):284–296. doi:10.1007/s10862-015-9514-x
53. Cox RC, Jessup SC, Olatunji BO. Executive Dysfunction and Emotion Dysregulation Explain the Effects of Insomnia Symptoms on Repetitive Negative Thinking. Cogn Ther Res. 2019;43(6):995–1004. doi:10.1007/s10608-019-10033-y
54. Brush DM, Paulson D, Legon MJH, et al. Sleep disturbance and depressive symptoms in later-life: cross-sectional examination of cognitive mechanisms. Neurol Psychiatry Brain Res. 2020;37:6–14. doi:10.1016/j.npbr.2020.05.001
55. McCall WV, Turpin E, Reboussin D, Edinger JD, Haponik EF. Subjective Estimates of Sleep Differ From Polysomnographic Measurements in Obstructive Sleep Apnea Patients. Sleep. 1995;18(8):646–650. doi:10.1093/sleep/18.8.646
56. Van Den Berg JF, Van Rooij FJ, Vos H, et al. Disagreement between subjective and actigraphic measures of sleep duration in a population-based study of elderly persons*. J Sleep Res. 2008;17(3):295–302. doi:10.1111/j.1365-2869.2008.00638.x
57. Wittmann M, Lehnhoff S. Age Effects in Perception of Time. Psychol Rep. 2005;97(3):921–935. doi:10.2466/pr0.97.3.921-935
58. Omvik S, Pallesen S, Bjorvatn B, Thayer J, Hilde Nordhus I. Night-time thoughts in high and low worriers: reaction to caffeine-induced sleeplessness. Behav Res Ther. 2007;45(4):715–727. doi:10.1016/j.brat.2006.06.006
59. Ramlee F, Sanborn AN, Tang NKY. What Sways People’s Judgment of Sleep Quality? A Quantitative Choice-Making Study With Good and Poor Sleepers. Sleep. 2017;40(7):zsx091. doi:10.1093/sleep/zsx091
60. Chen JH, Lin KP, Chen YC. Risk Factors for Dementia. J Formos Med Assoc. 2009;108(10):754–764. doi:10.1016/S0929-6646(09)60402-2
61. Sharp ES, Gatz M. The Relationship between Education and Dementia An Updated Systematic Review. Alzheimer Dis Assoc Disord. 2011;25(4):289–304. doi:10.1097/WAD.0b013e318211c83c
62. Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet Lond Engl. 2020;396(10248):413–446. doi:10.1016/S0140-6736(20)30367-6
63. McCarrick D, Prestwich A, Prudenzi A, O’Connor DB. Health effects of psychological interventions for worry and rumination: a meta-analysis. Health Psychol. 2021;40:617–630. doi:10.1037/hea0000985
64. Hu RF, Jiang XY, Chen J, et al. Non‐pharmacological interventions for sleep promotion in the intensive care unit. Cochrane Database Syst Rev. 2015. doi:10.1002/14651858.CD008808.pub2
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.