Back to Journals » Clinical Ophthalmology » Volume 14
XEN® Gel Stent: A Comprehensive Review on Its Use as a Treatment Option for Refractory Glaucoma
Authors Fea AM ![]() , Durr GM
, Durr GM ![]() , Marolo P
, Marolo P ![]() , Malinverni L, Economou MA
, Malinverni L, Economou MA ![]() , Ahmed I
, Ahmed I
Received 29 March 2020
Accepted for publication 22 May 2020
Published 30 June 2020 Volume 2020:14 Pages 1805—1832
DOI https://doi.org/10.2147/OPTH.S178348
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Antonio M Fea,1 Georges M Durr,2,3 Paola Marolo,1 Lorenza Malinverni,1 Mario A Economou,4 Ike Ahmed5
1Struttura Complessa Oculistica, Città Della Salute e Della Scienza di Torino, Dipartimento di Scienze Chirurgiche - Università Degli Studi di Torino, Torino, Italy; 2Department of Ophthalmology, Université de Montréal, Montréal, Québec, Canada; 3Department of Ophthalmology, Centre Hospitalier Universitaire de Montréal (CHUM), Montréal, Québec, Canada; 4Karolinska Institute, Stockholm, Sweden; 5Department of Ophthalmology and Vision Sciences, University of Toronto, Toronto, Ontario, Canada
Correspondence: Antonio M Fea Email [email protected]
Abstract: The XEN Gel Microstent is a subconjunctival microinvasive glaucoma surgical device developed with the aim of improving the predictability and safety profile of bleb-forming glaucoma surgical procedures. The stent is a hydrophilic tube composed of a porcine gel cross-linked with glutaraldehyde with good stability and biocompatibility with minimal tissue reaction. This device has demonstrated promising outcomes with fewer risks compared to traditional surgeries. The aim of the review is to present early studies on different designs of the XEN Gel Stent, to summarize different surgical techniques of implantation and to analyze more comprehensively the results, complications and rates of needling of the commercially available device (Xen 45). The review will address separately special cases (PXG, UVG, ICE, congenital glaucoma) and describe small series and case reports.
Keywords: XEN Gel Stent, glaucoma surgery, review, efficacy, safety, needling
Background
Primary open angle glaucoma (POAG) is one of the leading causes of irreversible blindness.1 The pathogenesis of POAG is not yet fully understood, but elevated intraocular pressure (IOP) is considered the only modifiable risk factor. The mainstay of glaucoma treatment is IOP reduction, which can be achieved with topical or oral drugs, laser treatments and surgery. First-line treatment typically involves hypotensive drops, which are effective, but cause local side effects such as ocular surface irritation or allergy.2,3 Laser treatments have been proven to significantly reduce IOP, but the effect may be short-lived or in some cases altogether ineffective.4,5 Traditional surgeries such as trabeculectomy have a long track-record of IOP reduction, yet carry significant long-term risks of hypotony and infection.6,7 Recently, minimally invasive glaucoma surgeries (MIGS) have made their way into our treatment armamentarium. The aim of MIGS is to decrease IOP while reducing significant risks of intra and postoperative complications as well as rapid recovery. There are three main MIGS subtypes: 1) trabecular8 2) suprachoroidal9 3) subconjunctival.10 Trabecular bypass MIGS generally provide an excellent safety profile with modest IOP lowering more often combined with cataract surgery.11 There are currently no available suprachoroidal shunts on the market although there are ongoing trials (MINIject and iStent Supra). The subconjunctival route has become increasingly popular due to encouraging early results. The XEN Gel Stent has been widely available since its approval by the FDA in 2016 with a growing number of publications. The aim of this article is to review the available literature on this device. The review addresses the implantation procedures, the ex-vivo studies, the pre-marketing studies involving devices with different lumens. Studies with the currently available 45-micron inner diameter will be discussed and they will be divided into: solo and combined with cataract surgery studies, addressing glaucoma subtypes and compared to trabeculectomy. Needling and complications will be addressed separately. A subsection will be addressing small series and case reports. Different criteria have been used to define success and they will be summarized in Table 1 to ease the reading of the paper. At the end of each section a short summary of the main findings will also be provided.
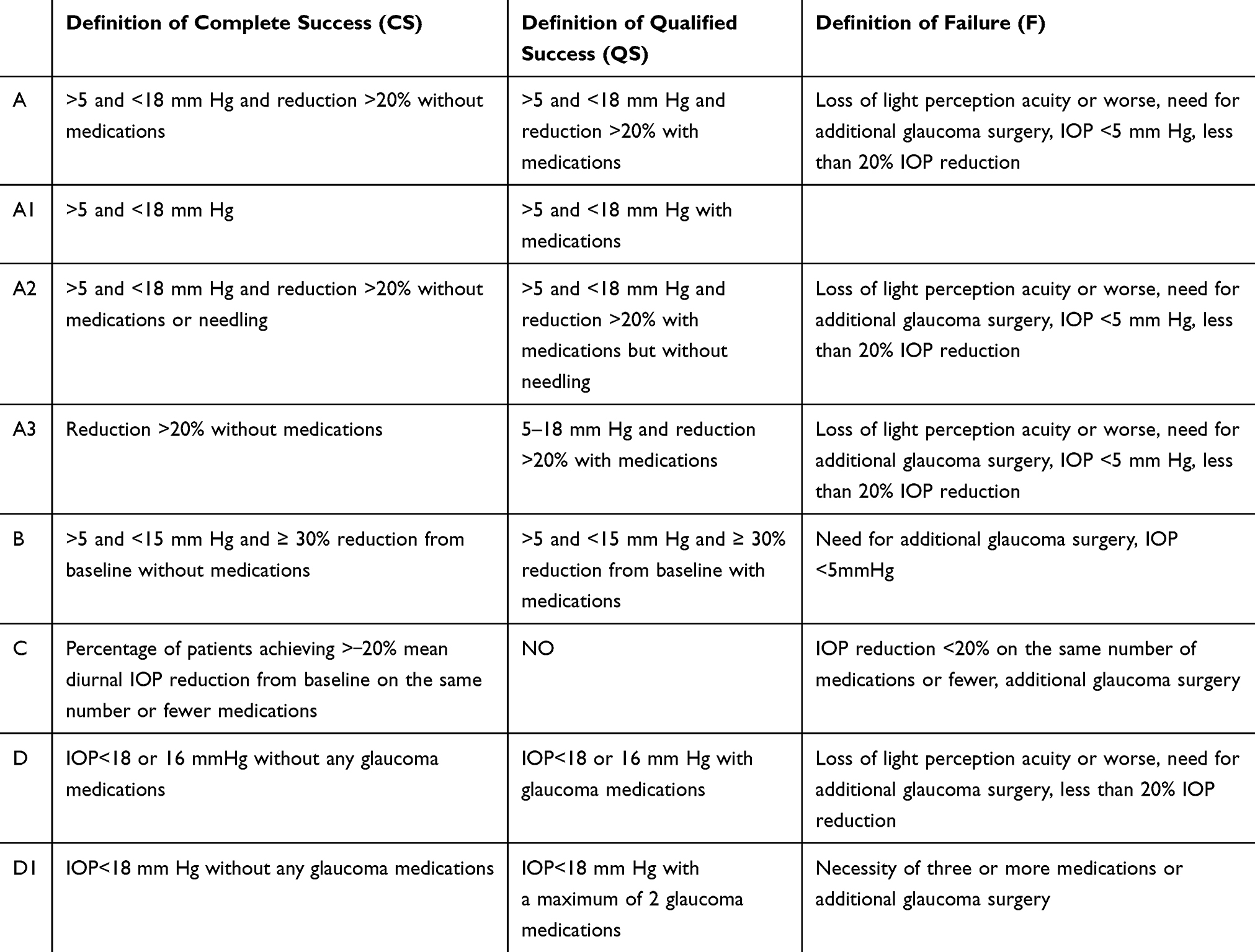 |
Table 1 Definitions of Success |
Device and Procedure
The XEN® Gel Stent (Allergan INC, Dublin, Ireland) is a flexible and permanent ab interno collagen implant draining aqueous fluid from the anterior chamber to the subconjunctival space through a scleral channel. Originally three designs were created: Xen 140, Xen 63 and Xen 45. They are all 6.0 mm long but differ in the inner diameter of their lumen (140 μm, 63 μm and 45 μm, respectively). The commercially available version of the implant is currently the Xen 45. According to the Hagen–Poiseuille equation, the stent is designed to create resistance to outflow of around 6 to 8 mmHg under conditions of physiologically normal aqueous production (2 to 2.5 mL/min) without the need for a valve.12 The stent is a hydrophilic tube composed of a porcine gel cross-linked with glutaraldehyde. Animal studies have shown the material’s stability and biocompatibility with minimal tissue reaction.13, A, B The XEN® Gel Stent is firm when dry, but it becomes soft and flexible when hydrated, conforming to the surrounding tissues. The device passes through the scleral channel with a typical “S” curve and creates a natural bend of approximately 35 degrees under the conjunctiva and Tenon. Its high flexibility reduces the upward force onto the conjunctiva during implantation which reduces the risk of erosion. The inserter has a 27G needle preloaded with the implant and sterilized via gamma irradiation. The injector is designed to place the gelatin stent in the intended position, and deployment is achieved by a linear movement of the slider at the center of the injector body.
The XEN® Gel Stent is indicated for the treatment of primary open angle glaucoma (POAG) where previous medical treatment failed and for patients with pseudoexfoliative glaucoma (PXG) or pigmentary glaucoma (PDG) that cannot be controlled with maximum tolerated medical therapy. It can be used also for juvenile (JVG)14–16 and uveitic glaucoma (UVG).17,18 The device is CE marked in the European Union and it has been approved by the US Food and Drug Administration. It is also licensed for use in Canada, Switzerland and Turkey.
The XEN® Gel Stent is usually implanted through an ab interno approach without conjunctival dissection either as a standalone procedure (Xen solo) or in combination with cataract surgery (Xen combo). Some surgeons have preferred an ab externo delivery of the device with or without conjunctival dissection. The surgery can be performed under peribulbar or topical anesthesia.
The ab interno steps are the following. The superior nasal conjunctiva is marked 2.5 mm from the limbus. Intraoperative mitomycin C (MMC) is injected subconjunctivally in order to reduce postoperative scar tissue formation. Clear corneal incisions (main and side-port) are created and the anterior chamber is filled with a cohesive viscoelastic. The needle is inserted through the main corneal incision and directed across the anterior chamber (AC) towards the superonasal quadrant. A goniolens can be used to assess positioning in the angle, ideally entering just above trabecular meshwork to avoid bleeding and to stay clear of iris and endothelium. The needle is advanced through the sclera into the subconjunctival space, while the eye is stabilized using a second instrument in the side-port incision. Once the bevel is clearly visualized exiting sclera into the subconjunctival space, the gelatin stent is released and the injector removed from the eye. Approximately, 1 mm of the implant remains in the AC, 3 mm pass through the scleral and 2 mm emerge under the conjunctiva. The viscoelastic is then washed out of the anterior chamber creating an early bleb and confirming patency of the device.
The ab-externo placement can be performed with or without conjunctival dissection. In the first case, the conjunctiva is displaced anteriorly, and the needle pierces the sclera at 2.5 mm from the limbus, entering the AC where the stent is then released. MMC is injected subconjunctivally before or after implantation. If conjunctiva is opened, the stent is deployed 2.5 mm from the limbus and MMC soaked sponges or injections are used. The conjunctiva and Tenon’s layer are then closed. Ab-externo placement avoids viscoelastic injection and allows for more precise positioning of the device.
Ex vivo Studies
Lewis10 reviewed critical choices in the design of Xen Gel Stent. Lumen size, length, flexibility, stability and biocompatibility of the device were discussed as crucial characteristics in order to optimize subconjunctival drainage. The material also plays a key role in the biocompatibility of the device. The Xen is formed of porcine gelatin cross-linked with glutaraldehyde exhibiting excellent hydrolytic stability and biocompatibility without any foreign-body reactions in dogs at 12 months and in nonhuman primates at 6 years.13, A, B Histology studies showed that reduced drainage occurred due to fibrosis surrounding the device rather than lumen obstruction. As for flexibility, it was measured assuming the natural bend of 10 and 35 degrees that the device takes while passing through the sclera. Measurements were performed using a microforce gauge with sensitivity in the micrometer range. At the bending angle of 10 degrees, the flexibility was 50–60 μN for Xen 140, 25 μN for Xen 63 and 15 μN for Xen 45, comparing to the 2000 μN of silicone tube shunts. At the bending angle of 35 degrees, it was 280 μN for Xen 140, 100 μN for Xen 63, 70 μN for Xen 45. This was unmeasurable in tube shunts as it was too high. Compared to Xen 140, Xen 45 was 4 times more flexible and Xen 63 was 2 to 3 times more flexible with minimal force to the overlying conjunctiva (2.2 N at a 3.0 mm exit point). This property should theoretically minimize conjunctival erosion. Another feature is the outflow resistance of the stent. According to the Hagen-Poiseuille equation, its inner diameter and length create a passive resistance to fluid. Considering a maximum flow rate with normal aqueous production (approximately 2 μL/min or 3 mL/day), an inner diameter of 45 μm and a length of 6 mm, the Xen 45 gives a flow of 0.02 μL/sec or 1.2 μL/min with a resultant IOP of 6–8 mmHg.
Sheybani et al12 compared fluid dynamics of Xen with an Ex-Press shunt (Alcon, Fort Worth, TX) and a 10 mm silicone tube derived from a Baerveldt implant (Johnson & Johnson Vision, Santa Ana, CA). Using a syringe pump and a pressure transducer at multiple flow rates, they obtained results comparable to the ones previously described by Lewis. In order to prevent hypotony, the difference of pressure between the two ends of a tube (steady-state pressure), should be approximately 5 mmHg with an aqueous humor production rate of 2–3 μL/min. The flow rate through Xen 45 at 5 mmHg was of 1.2 μL/min, which is less than aqueous production. Considering the Hagen-Poiseuille equation and the principles of Newtonian fluidics, at a flow rate of 2.5 μL/min the Xen 45 achieved a steady-state pressure at 7.56 mmHg, while the Ex-Press shunt and Baerveldt tube reached steady-state pressures at 0.09 and 0.01 mmHg, respectively.
Xen 63 and Xen 140 Clinical Studies
Sheybani et al19 first performed a pilot study on phacoemulsification combined with Xen 63 or Xen 140 to treat open-angle glaucoma (27 eyes, 79.4%), PXG (9 eyes, 26.4%) and PDG (1 eye, 2.9%). Three eyes (8.8%) previously underwent cyclophotocoagulation and 11 eyes (32.3%) had previous ALT or SLT. In a nonrandomized prospective interventional case series, 34 out of 37 eyes (3 patients were lost to follow-up) were followed 1 year after surgery. Mitomycin C was not used during the surgical procedure and postoperative medications (and needling) were added as needed. The definition of success/failure was A. IOP decreased from 22.4±4.2 mmHg at baseline to 15.4±3.0 mmHg at 12 months (−31.3%) (p<0.0001). Complete success was obtained in 47.1% of cases and qualified in 85.3%. Glaucoma medications (meds) were reduced from 2.5±1.4 to 0.9±1.0. There was no difference in outcomes and complications between Xen 140 and Xen 63. Early hypotony was common (13 patients had IOP<5mmHg in the first day; 4 at 1 week) but self-limited (no patient at one month). Needling rates were 32% at 1-year.
In a subsequent prospective, multicentric, nonrandomized, cohort study, Sheybani et al reviewed the 1-year results after solo Xen 140 implantation in 49 eyes (17 pseudophakic).14 Glaucoma types varied with 38 POAG (77.5%), 6 PXG (12.2%), 2 PDG (4%) and 3 JOAG (6.1%). One patient was lost to follow-up and 3 failed. Mean IOP decreased from 23.1±4.1mmHg with 3.0±1.1 meds at baseline to 14.7±3.7mmHg (36.4% percent IOP reduction) with 1.3 meds at 12 months. Eighteen patients (40%) achieved complete success and 40 (89%) qualified success (definition A). Needling was required in 47% of the eyes, with a reduction of mean IOP from 24.6±7.2 mmHg before needling to 13.2±4.8 mmHg after needling (p<0.001). As in the previous study, high needling rates may be due to no MMC at the time of surgery. Comparing eyes with previous glaucoma surgery (22 eyes; 21 trabeculectomy and 2 tube shunt) and eyes without (37), no significant difference in final IOP or medication use, although needling rate were higher in patients with previous surgery (54.6 vs 33%). Three eyes required further glaucoma surgery.
Lenzhofer et al20 published a prospective multicenter study reporting the results of Xen 63 implantation with 4-year follow-up. Sixty-four eyes with POAG (34, 52%), PXG (26, 41%) and PDG (7, 7%) with uncontrolled IOP or intolerance to drops were enrolled: 35 with Xen 63 solo and 29 with Xen 63 combo. At 4-years 34 eyes (53%) were analyzed: 11 eyes (17%) were lost to follow-up and 19 (29.7%) were classified as complete surgical failure. MMC was not used. IOP decreased at 4 years from 22.5±4.2mmHg with 2.4±1.3 meds to 13.4±3.1mmHg with 1.2±1.3 meds (40% IOP decrease p< 0.001). There was no difference in mean IOP and mean medications at 4 years between solo and combo groups (IOP 13.2±2.7 vs 13.7±3.7mmHg (p=0.65); medication 1.1±1.3 vs 1.4±1.4 (p= 0.40), respectively). Twelve out of 53 (25%) patients achieved complete surgical success and 28 eyes (53%) qualified success after 4 years (definition A). Needling was required in 53.1% of cases, with an average of 1.3 needling after a mean of 3.9 years. Further glaucoma surgeries were required in 19/53 eyes (36%) with a mean surgical failure per year of 10%. Visual acuity and visual fields remained stable at 4 years postoperatively. Low complication rates were reported: 3/36 patients presented early clinically hypotony, which resolved by year 4, 1/36 patients had an exposure requiring additional glaucoma surgery and 2/36 patients had lumen obstruction resolved with Nd:YAG laser..
Summary of the ex vivo and Pre-Marketing Studies
The XEN presents excellent biocompatibility and the ex vivo studies, later confirmed by clinical studies, proved that the fluidics provided by this implant allow for a significant decrease of IOP with minimal risk of hypotony.
Xen 45 Clinical Studies
Efficacy
Xen 45 Solo
Tan et al21 presented a retrospective consecutive nonrandomized interventional case series, of 39 eyes some of which with previous surgery (30.8% cataract surgery, 7.7% trabeculectomy, 5.13% iStent [iStent trabecular micro-bypass; Glaukos Corporation, Laguna Hill, CA, USA]) (Table 2). In all eyes, a single surgeon implanted Xen 45 using MMC (0.2 mg/mL). The majority of patients had POAG (30, 71.7%), followed by PXG (5, 5.1%), uveitic glaucoma (4, 10.3%), PDG (1, 2.5%), NVG (1, 2.5%) and steroid induced (1, 2.5%). The pre-operative IOP was 24.9±7.8mmHg and decreased to 14.5±3.4mmHg at 12month (p<0.005); meds decreased from 3 pre-surgery to 0.7 at 12 month (p<0.005). The percentage of complete success was 87% (definition A) and 62% (definition B) while qualified success was 92% and 64% respectively (Table 1).
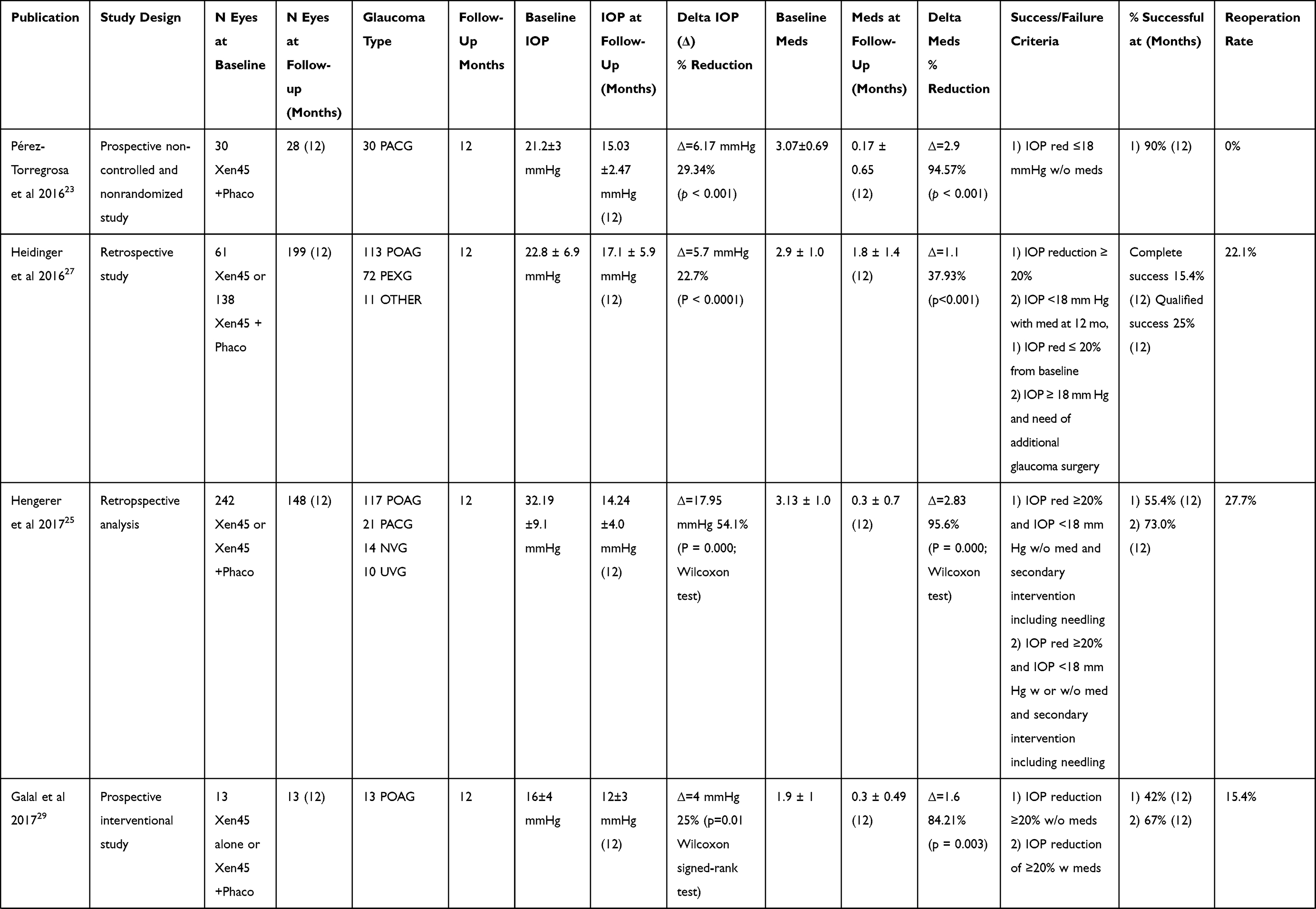 |  |  |  |
Table 2 Efficacy Results of Xen Studies |
Grover et al22 in their prospective, single-arm, open-label, multicenter study, reviewed solo Xen 45 implantation in 52 out of 65 eyes with refractory glaucoma at 12 months. Seven (10.7%) required explantation, 2 (3%) were lost to follow-up, 2 (3%) died and 2 (3%) were not included in the analysis. Refractory glaucoma was defined as a previously failed filtering surgery or cycloablative procedures (84.6%) and/or uncontrolled IOP on maximally tolerated medical therapy. Glaucoma types were POAG in 57 eyes (57.6%), 6 PXG (9.2%), 1 PDG (1.5%) and 1 combined mechanism glaucoma (CMG) (1.5%). At 12 months, 75.4% were successful (Criterion C) with a mean diurnal IOP reduction of 6.2 mmHg and meds decreased from 3.5±1 (baseline) to 1.7±1.5 (12 months) with no change when stratifying by age (<60, 60 to <70, 70 to <80, and ≥80 years), baseline IOP (20 to 25, >25 to 30, and >30 mmHg), baseline medication count (1, 2, 3, 4, and 5), sex, or ethnicity (Asian, African American, Hispanic, and Caucasian). In a subgroup analysis, excluding 4 patients with missing data and 9 patients who required further surgical intervention, mean diurnal IOP was 15.9±5.2 and mean IOP change from baseline was >27% at all postoperative visits, reaching −9.1mmHg at 12 months. IOP decrease of at least 20% was achieved in 88.5% of the eyes in this subgroup and 20 patients (38.5%) did not require meds. Compared with baseline, 36 (69.2%) patients required fewer topical medications, 16 (30.8%) required the same number, and none required more. Complete success was achieved in 75% of cases at 1 year (definition C).
Xen 45 Combo
Pérez-Torregrosa et al23 published a prospective nonrandomized, uncontrolled study with 1-year follow-up on 28 POAG eyes with implant and combined cataract surgery with Xen45 combo. All eyes had 0.1 mL of 0.1 mg/mL MMC injected subconjunctivally. IOP and medications significatively decreased from 21.2±3.4 mmHg with 3.1±0.7 meds to 15.03±2.5 mmHg with 0.2±0.7 meds (reduction of 29.3%, p<0.001 and 94.6%, p<0.001 respectively). Complete success was achieved in 90% of the cases (definition A). Three patients still required medications at 1 year. No significant reduction in VA was reported (Table 2).
De Gregorio et al24 published a nonrandomized prospective clinical study on 41 eyes of 33 patients. Glaucoma types were POAG in 35 (85.3%) and 6 (14.6%) had PXG. MMC dose was 0.1mL of 0.1mg/mL. Complete success was achieved in 33 eyes (80.4%) and qualified success in 40 eyes (97.5%) (definition A1). IOP and meds decreased from 22.5±3.7 mmHg with 2.5±0.9 meds at baseline to 13.1±2.4 mmHg with 0.4±0.8 meds at 1 year (IOP reduction 41.82%, p<0.05).
Xen 45 Solo vs Xen 45 Combo
Hengerer et al25 compared Xen 45 solo (n=200) with Xen 45 combo (n=39) in a retrospective single center, single surgeon analysis including 117 patients with POAG (48.3%), 62 with PXG (25.6%), 21 with primary angle closure glaucoma (PACG) (8.7%), 14 with NVG (5.8%) and 10 with uveitic glaucoma (4.2%) with a 12 months follow-up. One-year data was available for 148 eyes. MMC dose was 0.1 mL of 0.1 mg/mL. One hundred seventy eyes (70.2%) had undergone prior interventions, with 53 eyes (21.9%) having a trabecular micro-bypass stent and 52 eyes (21.5%) having undergone prior trabeculectomy. Almost all eyes (n=239; 98.8%) were on at least one anti-glaucoma medication, 40 eyes (16.5%) were on two medications, 175 eyes (72.3%) were on 3 or 4 medications, and 11 eyes (4.5%) were on 5 medications with 87 eyes (36%) requiring systemic acetazolamide. The mean medicated baseline IOP in the Xen solo group was 31.5±8.4 mmHg on 3.1±1.0 meds decreasing to 14.3±4.2 mmHg on 0.3±0.7 meds and in the Xen combo group was 35.7±12.0 on 3.3±1.0 meds decreasing to 13.9±2.5 mmHg on 0.4±0.7 meds at post-operative month 12. Complete success was achieved in 55.4% of the eyes and qualified success in 73% with no significant difference between the two groups (definition A2).
Ozal et al26 compared Xen 45 solo (n=9) and Xen 45 combo (n=6) in a retrospective consecutive case series study including patients with POAG (66.6%), PXG (26.6%), PDG (6.6%) and previous filtering surgeries (20%) with 1 year follow-up. No MMC was injected. Nine eyes (60%) were on 4 meds, 6 eyes (40%) were on 3 meds. The mean medicated baseline IOP was 36.1 mmHg decreasing to 16.7 mmHg (p<0.001) and the number of meds decreased from 3.6±0.5 to 0.3±0.9 (p<0.001). Success criteria was not defined. At 12 months two patients (13.3%) required glaucoma treatment.
Widder et al16 in a retrospective single center study comparing Xen 45 solo (139 pseudophakic and 45 phakic eyes) and Xen 45 combo (49 eyes) including POAG (180, 77.2%), PXG (44, 18.8%), PDG (2, 0.8%), JOAG (1, 0.4%) and secondary unspecified glaucoma (6, 2.5%) with an average follow-up of 8.5 months (range: 1–23 months). MMC dose was 0.1 mL of 0.1 mg/mL. Patients included had prior history of laser therapy (ALT/SLT, 39) and glaucoma surgeries such as trabeculectomy (17), deep sclerectomy (6), trabectome (31) and vitrectomy (6). All patients with insufficient IOP reduction underwent a surgical revision as the primary treatment. The baseline IOP was 24.3±6.6 mmHg with 2.6±1.1 meds and significantly decreased to 16.8±7.7 mmHg (p<0.001) with 0.2±0.7 meds (p<0.001) at last follow-up. The authors used multiple definitions of success: Score A indicated the number of eyes that achieved target pressure without additional surgery: Score B was defined as IOP reduction >20% and IOP<18mmHg; score C as IOP<21 mmHg and reduction>20%; Score D as IOP lower than 15 mmHg and IOP reduction ≥40%. The percentage of primary success (Score A: no revision) was 66% and the overall success rate was 90% (1 revision). Pseudophakic eyes had higher success rates compared to phakic eyes and Xen combo (primary success was 73%, 53%, 55% respectively).
Heidinger et al27 in a single-center, retrospective study compared Xen 45 solo (n=61) and Xen 45 combo (n=138) in patients with POAG (113, 56.8%), PXG (72, 36.2%), and other glaucoma types (11, 5.5%) with up to 18 months follow-up. Only, 89/199 completed 12-month follow-up and 42/199 completed 18-month. MMC dose was 0.1 mL of 0.1 mg/mL. Baseline IOP and meds was 22.8±6.9mmHg on 2.9±1.0 meds decreasing to 17.1±5.9mmHg on 1.8±1.4 meds (P < 0.0001) at 12 months, and to 16.4±3.8 mmHg and 1.8±1.4 at 18 months. Complete success was achieved in 15.4% of cases, whereas qualified success in 25.0% (definition A). Stratification by age (categories: <60, 60 to 79, >79y), sex, type of glaucoma, type of operation (solo vs combo) and previous surgeries showed similar results in terms of IOP reduction and meds.
Karimi et al28 in a retrospective case series evaluated Xen 45 solo (n=187) and Xen 45 combo (n=72) without any previous surgery. Only 89 eyes were evaluated at 12 months. Patients had POAG (208, 80.3%), NPG (17, 6.6%), PXG (13, 5%), PDG (6, 2.3%), traumatic glaucoma (6, 2.3%), NVG (5, 1.9%), iatrogenic glaucoma (1, 0.4%) and other types of glaucoma (3, 1.3%). Exclusion criteria were not mentioned. Baseline IOP and meds decreased from 19.3±0.7 mmHg on 2.6±0.1 meds to 14.2±0.9 on 0.8±0.2 meds (P<0.0001). At 12 months, complete success was achieved in 37.4% and qualified success in 24.2% (definition A). There was no difference in outcomes between the two groups and they had similar needling rates and complications. Patients with previous glaucoma surgery also showed similar IOP reduction (19.8±6.9 mmHg to 13.9±4.0 mmHg) to patients without any previous surgery (19.4±13.3 mmHg to 13.5±6.3 mmHg). Similarly, no difference was found in terms of meds used, bleb needlings or adverse events in either subgroups.
Galal et al29 reviewed a prospective interventional case series of Xen 45 solo (n=3) and Xen 45 combo (n=10) with 12-month follow-up. MMC dose was 0.1 mL of 0.1 mg/mL. The results were not separated between solo and combo cases. Overall, baseline IOP decreased from 16±4 mmHg to 12±3 mmHg (−31.6%, p=0.01) and meds decreased from 1.9±1 to 0.3±0.49 (−82.9%, p=0.003). Complete success was achieved in 42%, while qualified success in 67% (definition A3).
Mansouri et al30 (2018), in a prospective interventional case series compared Xen 45 solo (n=40, 26.8%) and Xen 45 combo (n=109, 73.2%) with 12-month follow-up. MMC dose was 0.1 mL of 0.2 mg/mL. Glaucoma types were POAG (46, 54%), PXG (32, 37.2%) and other types (6, 7.1%). Only 87 eyes achieved 12-month follow-up. Mean IOP decreased from 20.0±7.1 with 1.9±1.3 medications to 13.9±4.3 mmHg (p<0.01) with 0.5±0.8 medications (p<0.001). The median IOP reduction was 40% in the Xen 45 solo group and 22.9% in the Xen 45 combo group. The primary endpoint, a 20% or more decrease from medicated baseline IOP at 1 year, was achieved in a total of 54 (62.1%) eyes; 17 (81.0%) in Xen 45 solo and 37 (56.1%) in Xen 45 combo (P = 0.04). At 1-year, complete success was achieved in 57.5% of the Xen 45 solo group and 64.2% of the Xen 45 combo group (definition C). There were no factors associated with increased failure. At 1 year, 28.7% of eyes required antiglaucoma medications for IOP reduction and 37% required a needling. Adverse effects included bleb revision (5), choroidal detachment (2), and secondary glaucoma surgery (9).
Hohberger et al31 conducted a single center prospective interventional study with a 6 months follow-up, comparing Xen 45 solo (n=81) and Xen 45 combo (n=30) in patients with POAG (72, 64.8%), PXG (31, 27.9%) and other types (8, 7.2%). Fifty-two eyes were pseudophakic in the Xen 45 solo group (64%). MMC dose was 0.1 mL of 0.3 mg/mL. The authors do not report mean IOP results. Complete success was achieved in 46.9% of Xen solo group and qualified success was 2.5% compared to 53.3% in the Xen combo group and qualified success of 3.3% (definition D1). No complications or needlings were reported.
A prospective multicenter nonrandomized trial by Reitsamer et al32 compared results of Xen 45 solo (n=120) and Xen 45 combo (n=98) with 2-year follow-up in uncontrolled moderate POAG. Two-hundred and forty eyes of 218 patients were enrolled (19 patients underwent Xen 45 implant in both eyes, at least one month apart). Overall, 197/218 (90.4%) eyes completed the 12-month visit; 174/218 (79.8%) completed the 24-month visit, while 44/218 (20.2%) discontinued the study. No case was withdrawn due to complications. Similar populations were available, in a modified intent-to-treat (mITT) model, with 182/202 (90.1%) and 161/202 (79.7%) eyes completing the 12- and 24-month visits, respectively, and 41/202 (20.3%) discontinuing the study. Adjunctive subconjunctival antifibrotic agents were used in all eyes; 99% received MMC, while the remaining 1% received 5- fluorouracil (5-FU). The absolute dose and time of injection of MMC was variable between sites raging from 10 to 500 µg administered either the day before surgery, right before or after implantation. No sub-analysis compared MMC dose. Mean medicated baseline IOP was reduced from 21.4±3.6 to 14.9±4.5 mmHg at 12 months and 15.2±4.2 mmHg at 24 months, with similar results in both treatment groups. Changes in mean IOP and medication count from baseline were −6.5±5.3mmHg and −1.7±1.3 meds at 12 months and −6.2±4.9mmHg and −1.5±1.4 meds at 24 months, respectively (all p < 0.001). Overall, 51.1% (12 months) and 44.7% (24 months) of eyes were medication-free. Results were similar in both treatment arms. The mean changes in IOP from baseline were −6.6±5.6 and −6.4±5.0mmHg at month 12 and −6.4±5.2 and −5.9±4.6 mmHg at month 24 in the Xen solo and Xen combo groups, respectively. The mean changes in meds were −1.8±1.3 and −1.6±1.2 at month 12 and −1.5±1.5 and −1.5±1.2 at month 24, respectively. The mean percentage changes in IOP from baseline were −29.6% (month 12) and −28.2% (month 24) in the former group and −29.1% (month 12) and −27.2% (month 24) in the latter. At 24 months, outcomes were also similar in pseudophakic eyes that received the implant alone (IOP reduction, −8.4 mmHg; reduction in medication number, −1.5; n = 15 in the mITT population) versus the overall Xen alone group and the Xen combo group. The outcomes also appeared similar between phakic (n = 80) and pseudophakic (n = 25) eyes, although no statistical comparisons were made between these groups. Complete success was achieved in 65.8% of cases at 2-years (definition C). Several other cutoffs were used at 2 years: a reduction in IOP ≥30% in 48.4%, IOP ≤18 mmHg in 85.1%, IOP ≤15mmHg in 62.7% and IOP ≤12 mmHg in 24.2%. Overall, 51.1% (12 months) and 44.7% (24 months) of eyes were medication-free.
In a prospective multicenter open-label study, Fea et al33 compared 298 patients with Xen 45 solo (n=115) and Xen 45 combo (n=56) at 1-year results with 171 patients undergoing more than 9 months follow-up. At the 12-month visit, data were available for 87.1% of patients (149/171). In the Xen 45 solo, 72 were pseudophakic. Glaucoma subtypes included POAG (134, 45.0%), PXG (27, 9.0%), JOAG (2, 0.7%), NPG (7, 2.3%), uveitic (3, 1.0%), CMG (2, 0.7%) and ocular hypertension (1, 0.3%). Overall, mean IOP and meds decreased significantly at 12-months from 23.9±7 mmHg on 3.0±1.1 to 15.5±3.9 mmHg on 0.5±1.0. No patient was on oral CAIs (28 at baseline). Compared with baseline, IOP decreased in both the combo and solo groups at the final visit from 21.4 mmHg to 15.8 mmHg and from 25.0 to 15.4 mmHg, respectively. At 1 week postoperatively, IOP was significantly lower in the solo group compared with the combo group (p=0.04), but no significant differences were detected at the following visits. Mean meds remained the same between groups at all follow-ups. No significant differences in IOP or the number of medications were detected between phakic and pseudophakic patients. IOP and the number of medications were reduced at the final visit by 38.6% and 83.7% in the solo group and by 26.2% and 80.1% in the combo group, respectively. Phakic patients achieved the highest percentage reduction for both parameters, although none of these differences were statistically significant Similarly, no significant differences were found for either qualified or complete success, with IOP cutoffs of ≤18 and 16 mmHg with or without medications. However, with a stricter cutoff of ≤14 mmHg, the solo group achieved higher success rates compared to the combo group (41.6% vs 22.9%; p=0.03)
Summary of Xen Solo and Combo
The studies reported in this section are very heterogeneous in terms of design, inclusion and exclusion criteria, pre-operative pressure and type of analysis. Xen 45 significantly reduced IOP (pre-operative range: 16–36.1 to postoperative range: 12–17.1) and medication use (pre-operative range: 1.9–3.6 to postoperative range: 0.2–1.8) both as a solo or as a combined procedure. The Authors disagree on the issue of better XEN efficacy as a solo or as a combined procedure. Some of the differences may be due to the way data have been analyzed, and it seems realistic that lower pressures may be reached, as in trabeculectomy, when the Xen is used as a solo procedure.
Safety
Complications
Xen 45 safety was evaluated by analyzing complication rates intra and postoperatively, needling rates and the need for a secondary surgical procedure. Timing of needlings varied widely due to surgical technique, surgeon preference and study population. Failure criteria was also variable with multiple definitions used if reported at all. Intraoperative complications include bleeding, subconjunctival and anterior chamber bleeding, dislocation and reimplantation of the device. Postoperative complications include hyphema and corneal pathologies. A significant postoperative complication is hypotony. Early numerical hypotony is usually transient and self-limited in the first month.21 Persistent clinical hypotony is defined as IOP <6mmHg with corneal folds, maculopathy, chorioretinal folds, choroidal detachments or reduced vision. Many options are available to address hypotony, including conservative management, air or viscoelastic injection, revisional surgery and conjunctival compression sutures.17 Early IOP spikes may also occur and are typically transient. Chronic IOP rise can be due to a variety of causes including device obstruction, malposition, iris incarceration or fibrosis of the filtering bleb. Steroid response, although uncommon, can also occur. Understanding the underlying cause to IOP elevation allows to better tailor our treatment.
Finally, severe complications rates are fortunately low. Endophthalmitis and blebitis, as well as avascular filtering bleb secondary to MMC have all been documented in case reports. Anterior chamber reaction, uveitis, cystoid macular edema and fibrin formation can all occur postoperatively and are typically self-limited. Malignant glaucoma, erosions and leaks have also been reported in a small number of cases.
We will analyze individually each study, maintaining the division between studies analyzing Xen 45 solo, Xen 45 combo and Xen 45 solo vs Xen 45 combo (Tables 3 and 4).
 |  |  |
Table 3 Needling Results of Xen Studies |
 |  |  |
Table 4 Needling Results of Xen Studies |
Xen 45 Solo
In the study of Tan et al21 numerical hypotony at day 1 was observed in 8 patients (20.5%) but resolved by four weeks without intervention except for one eye, which required AC reformation. Hyphema requiring AC wash-out occurred in one case (2.8%). Bleb intervention (median 2) occurred in 20 patients (51.3%). No patient required further glaucoma surgery. Subgroup analysis was performed between groups receiving a bleb intervention and a group which did not. Phakic patients were more frequent in the intervention group and had significantly higher IOP at 12-months (p=0.03).
Grover et al22 did not report any intraoperative complication. Sixteen (24.6%) patients experienced transient numerical hypotony (defined as IOP <6 mmHg) with 87.5% of cases had resolving by day 27. Overall, visual recovery following implantation of the gelatin stent was rapid and most patient experienced no change of VA by one year (94.6%). Of the four cases with reduced VA at one year, all were attributed to some retinal morbidity unrelated to the implant and in one case VA improved after cataract extraction. Needling was performed in 21 (32.3%) patients; 6 (9.2%) had 2 needlings and 1 (1.5%) had 3 needlings. One case of stent exposure occurred following implant repositioning. A secondary surgical intervention was required for 9 patients (13.8%). Those procedures occurred within 90 (1), 180 (4), 240 (7) and 300 days (9).
Xen 45 Combo
Pérez-Torregrosa et al,23 reported no hypotony or other severe complications. They reported intraoperative complications such as subconjunctival bleeding after MMC injection (11, 36.6%), slight intra-cameral hemorrhage (26, 86.6%) and bleeding at the scleral exit point (27, 90%). In 6 eyes (20%), the device was re-implanted due to short subconjunctival pathway and in one eye (3.3%) the device was re-implanted as it was too long into the AC.
De Gregorio et al24 had one case of possible obstruction of the device occurring one month after surgery and requiring a trabeculectomy. Few complications was noted with only one patient with hypotony and choroidal detachment which resolved spontaneously in one week, one needling and one device migration requiring explantation.
Xen 45 Solo vs Xen 45 Combo
Hengerer et al25 reported transient intraoperative hyphema in 4 eyes (1.7%) and conjunctival bleeding in 12 eyes (5.0%). Hypotony was observed in 9 eyes (3.7%) at one month and two eyes (0.8%) required an AC viscoelastic injection. Needling was required in 27.7% of all eyes and were performed between Week 1 and Months 3. Secondary surgical interventions were performed in 14/242 eyes (5.8%) and 12 eyes (5%) were successful with a second XEN 45 implant.
Ozal et al26 did not report needling rates. Bleeding at the time of implantation occurred in one case (6.6%), in another case the stent was removed because it prolapsed in the anterior chamber.
Widder16 reported intra-operative hyphema (22, 9.4%) with resultant post-operative hyphema which spontaneously resolved in 13 eyes (5.6%). Choroidal detachment occurred in 8 eyes (3.4%), IOP spikes (≥30mmHg) in 6 eyes (2.6%); macular edema in 4 eyes (1.7%) and fibrin reaction in 2 eyes (0.9%). A shallow anterior chamber was found in 3 eyes with one requiring AC viscoelastic injection. Two stents eroded the conjunctiva and were removed with one requiring a secondary stent, while the other developed a spontaneous bleb without any implant. One patient had a stent completely in the subconjunctival space and another one was damaged. The rate of surgical revision was 34% (80 eyes), and the rate of more than one surgical revision or with secondary filtering surgery was 10% (23 eyes). The mean time interval between stent implantation and revisional surgery was 5.0±4.2 months, and the mean time interval between revisional surgery and last follow-up was 5.2±4.8 months.
Heidinger et al27 reported no significant intraoperative complications. In 16 cases (8.0%) hypotony (≤6mmHg) occurred at day 1 with only one case requiring AC viscoelastic injection. Early hyphema (7, 3.5%) resolved within 1 week. Malignant glaucoma developed in one patient at day 5 requiring vitrectomy and there was one case of late-onset endophthalmitis at four months postoperatively treated with intravitreal antibiotics. Needlings/revisions were performed in 44 eyes (22.1%) with some cases requiring multiple needling revisions. In total 65 needlings were performed: 44 (67.7%) with 5-FU, 12 (18.5%) with dexamethasone and 2 (1.5%) without medications. Time to first needling ranged between 6 and 582 days with a median of 59.5 days. Three revisions (1.5%) were required due to stent exposure. In 28 cases (14.1%) a secondary filtering surgery was performed: 15 trabeculectomies (53.6%), 8 second Xen implant (28.6%), 4 transscleral cyclophotocoagulations (14.3%). Time to reoperation ranged between 8 and 916 days with a median of 196 days.
The most common complication in the Karimi study28 was numerical hypotony (90, 34.7%) with 72% resolving within 1 week. Hypotony maculopathy occurred in 5 eyes (1.9%), three resolved spontaneously (2 in one week and 1 in 1 month) and two required surgery (one re-suturing because of a bleb leak and one cryotherapy). IOP spikes (≥30mmHg) occurred in 33 eyes (12.7%). Secondary filtration surgery or ECP was needed in 29 cases (11.1%). Transient occlusion of the implant was present in 10 (3.9%) cases, 9 of which due to iris blocking the inlet of the device. One of these eyes (0.4%) required iris manipulation and another case (0.4%) medications were added. Persistent BCVA loss of ≥2 lines or ≥10 ETDRS letters lasting >1 month occurred in 9 (3.5%) eyes. Large dysesthetic blebs developed in 6 cases (3.9%). Six cases (2.3%) had stent erosion/exposure. One case (0.4%) of endophthalmitis was present at 18 months. Central retinal vein occlusion developed in one (0.5%) case and a cyclodialysis cleft secondary to implant insertion in one (0.5%) case. Sixteen cases (6.2%) required bleb or implant revision or repositioning. Apart from ECP, 2 further cases (0.7%) underwent other laser procedures to reduce IOP.
Galal et al29 counted 4 eyes (30.7%) requiring needling and 2 (15.4%) requiring trabeculectomy as a second intervention. No severe complications were reported, and minor complications were transient choroidal detachment in 2 eyes and implant extrusion in 1 eye that required repositioning and conjunctival suture.
Mansouri et al30 demonstrated a good safety profile with a low number of eyes experiencing adverse events. The total rate of adverse events was 14.7% with 22 eyes experiencing one or more adverse events. Three eyes (2%) had a loss in BCVA ≥2lines. Visual acuity loss was permanent in 2 eyes, one due to retinal detachment and one secondary to hypotony maculopathy. Needling rates at 1 year in combo eyes were 37% and a higher in solo eyes (45%) on average 4.5 months after surgery. Additional glaucoma surgery was needed in 9 eyes (10%), with 7 (4.7%) undergoing deep sclerectomy, 2 (1.4%) implanted with a second glaucoma drainage device, 1 (0.7%) with a second Xen, while 1 (0.7%) needed Xen repositioning.
Reitsamer32 reported intraoperative complications in 10 eyes (4.6%), the most common being AC bleeding in 6 eyes (2.8%). Postoperative complications occurred in 65 out of 218 eyes (29.8%); persistent uncontrolled IOP (6.4%) and hyphema in 10 eyes (4.6%) being the most common. Numerical hypotony occurred in 44/218 eyes (20.2%) and resolved spontaneously within the first 2 postoperative weeks. No hypotony complications were reported. Three of the study eyes experienced serious adverse events: central retinal vein occlusion at 12 months, conjunctival erosion with implant exposure, endophthalmitis (15 months postoperatively) and high IOP with SSI (cyclodestructive surgery) in the untreated fellow eye. The overall needling rate at 2 years was 41.1%, without significant differences between Xen solo (43.9%) and Xen combo (37.5%). Mean and median numbers of needling per eye were 1.6±1.1 and 1.0 (range of 1 to 6) in the overall population at 24 months. The majority of needled eyes (56 out of 83; 67.5%) had 1 needling, the mean time to the 1st needling was 152±160 days (median, 90 days). Secondary surgical intervention was needed in 14 eyes (6.4%).
Intra-operative complications were not reported in the study by Fea et al.33 Post-operative complications included: hyphema (33), shallow anterior chamber (7), choroidal detachment (16), migration in the anterior chamber (3), fibrin reaction (1), perforation after needling (1) and exposure (1). Stent repositioning was necessary in 3 cases. A single case of malignant glaucoma which needed vitrectomy was reported. The visual acuity was reduced to 1/10 at the final follow-up visit. Overall, 147 needlings were performed in 79 patients (46.2%), most patients required only 1 needling (41), others required 2 (21), 3 (10), 4 (3), 5 (2), and 6 (2) needlings. The needling rate was significantly higher in patients in the combo group compared with the solo group (48.21% vs 45.22%, P <.01) and in pseudophakic vs phakic patients (45.83% vs 44.19%, p=0.002). Additional surgery was performed in 12 (7%) patients (8 in the solo group and 4 in the combo group) including trabeculectomy (8), Ahmed valve implant (1), Baerveldt glaucoma implant (1), vitrectomy for malignant glaucoma (1), and bleb revision for exposure (1). Four of the additional procedures were performed on patients who had undergone previous glaucoma surgery.
Xen 45 in Glaucoma Different from POAG
PXG
Some studies included PXG patients but did not perform any analysis to further characterize their outcomes and will not be included in this section.
Ibáñez-Muñoz et al34 compared 21 eyes in a retrospective 12 months chart review analysis (13 Xen 45 alone and 8 Xen 45 combo) of patients with pseudoexfoliative glaucoma (PXG). Two experienced surgeons performed all cases using 0.1mL of MMC 0.1mg/mL. The baseline IOP was 21.1±3.8mmHg with 3.0±0.1 meds and the post-operative IOP was 15.2 ±3.9 mmHg with 1.23±1.22 meds (p<0.001) with no differences between the two groups. Total success rate was 85.7% (18) with 28.6% (6) achieving complete success and 57.1% (12) qualified success (definition A3). Needling was performed in 5 (23.8%) of the cases and one (4.8%) went on to trabeculectomy. Adverse events were transient including hypotony (4.8%), hyphema (4.8%), choroidal detachment (4.8%), uveitis (9.5%) and cystoid macular edema (4.8%).
Subgroup analysis were performed for POAG and PXG in the Hohberger et al (2018), described above. Xen 45 complete success was higher in the Xen 45 combo group in eyes affected by PXG (57.1%) compared to POAG (46.7%), but lower in the Xen 45 solo group (POAG 57.4% vs PXG 20%).
Mansouri et al35 conducted a prospective study including 57 eyes with POAG and 53 eyes with PXG with 1-year follow-up. Xen 45 solo was performed in 41 cases (72%) and Xen 45 combo in 40 cases (75%) by 2 surgeons. MMC dose was 0.1 mL of 0.2 mg/mL. IOP decreased at 1 year from 19.8±5.8 to 13.9±4.6 (−30%, p<0.01) in POAG and from 19.7±8.2 to 13.6±4.3 (−31%, p<0.01) in PXG. Medications decreased from 1.9±1.1 to 0.4±0.8 (p<0.001) in POAG and from 2.0±1.3 to 0.5±0.8 (p<0.001) in PXG. Complete success (IOP ≤16 mmHg without meds) was obtained in 38% of POAG and 57% of PXG (p=0.086), while qualified success (IOP ≤16 mmHg with meds) in 33% and 81%, respectively. PXG (HR, 0.36; P=0.043), lower baseline IOP (HR, 1.16; P < 0.005), and higher baseline meds (HR, 0.62; P = 0.043) were risk factors for success. Overall, there were a total of 27 ocular adverse events during the follow-up period. The most frequent were bleb revisions (3.4%), decrease in BCVA of > 2 lines (2%), and damaged XEN implant during needling (2%). One eye (0.9%) developed clinical hypotony with hypotony maculopathy. Nine (8.2%) eyes required a second glaucoma surgery.
Two years after implantation, Gillmann et al36 compared Xen 45 solo (24%) and Xen 45 combo (76%) in patients with POAG (57 eyes) and PXG (53 eyes). Patient characteristics were similar between the 2 groups except for older age for the patients with PXG. Mean medicated IOP were 19.8±5.8 mmHg on 1.9±1.6 meds (POAG) versus 19.8±8.2 mmHg on 2.0±1.3 meds (PXG) at baseline which decreased to 14.5±3.6 mmHg (−27%) on 0.6±0.9 meds versus 14.2±3.8 mmHg (−28%) on 0.4±0.7 meds, respectively, at 2 years. Using an IOP cutoff of 16 mmHg, 51.4% (POAG) versus 57.1% (PXG) eyes achieved complete success at 2 years. By 24 months, needling was performed in 42.8% (POAG) and 43.2% (PXG), with an average time to needling of 163 and 135 days, respectively. The rates of adverse effects were 30.6% (POAG) and 36.4% (PXG). Secondary glaucoma surgeries were required in 14.3% of POAG versus 15.9% PXG eyes. Three incisional bleb revision were performed in the PXG group compared to 1 in the in the POAG group. Overall, a total of 28 ocular adverse events were recorded during the follow-up period, excluding second surgical interventions. The most frequent early (<1 month) adverse events were hyphema (total 8.2%; 7.0% POAG; 9.4% PXG) and transient hypotony (total 3.6%; 5.3% POAG; 0% PXG). The most frequent late (>6 months) adverse event was surgical revision (total 3.6%; 1.8% POAG; 5.7% PXG).
UVG
Qureshi et al37 retrospectively, reviewed 37 eyes with medically uncontrolled uveitic glaucoma treated with Xen 45 solo with 12 months follow-up. Preoperatively all patients were on more than 3 ocular hypotensive medications and 75.7% were on oral acetazolamide. Systemic immunosuppression was used in 62.2% and all were on topical steroids. Baseline IOP was 36.1±9.6 mmHg on 3.7±0.5 meds and decreased to 12.6±4.1 mmHg (−65%) on 0.6±1.1 meds (−83%) at 1 year. Bleb needling with 5-fluorouracil was performed on 5 eyes (13.5%). Clinical hypotony occurred in 7 eyes requiring AC reformation (4) and compression sutures (2). Five eyes (13.5%) required secondary glaucoma surgery. Complete (no meds) success at 1 year was 89.2% for an IOP ≤ 21 mmHg and ≥ 20% reduction from baseline and for an IOP ≤ 15 mmHg and ≥ 30% reduction from baseline. Qualified (with meds) success was 91.9% for both IOP cutoffs.
Sng et al18 published a prospective case series on 24 (17 phakic, 7 pseudophakic) uveitic glaucomas implanted with Xen 45 solo with 12-month follow-up. MMC dose was 0.1 mL of 0.2 mg/mL. IOP decreased from 30.5±9.8 mmHg on 3.3±0.8 meds at baseline to 12.2±3.1 mmHg (−60%) with 0.4±0.9 meds at 1 year with 62.5% being medication-free. Needling was performed in 10 eyes (41.7%), bleb revision in 5 eyes (21%), anterior chamber reformation with viscoelastic in 5 eyes (20.8%). Further glaucoma surgery was needed in 4 eyes (16.7%): 1 eye trabeculectomy and 3 tube shunts. The most common postoperative complication was transient postoperative IOP elevation in 15 eyes (62.5%). Hypotony was noted in nine eyes (37.5%) resolving within 2 weeks in eight eyes. One patient (4.2%) had persistent hypotony and a choroidal effusion 2 months after XEN-45 implantation and required bleb revision with choroidal drainage. Erosion of the Xen occurred in two eyes (at postoperative month 3 and postoperative month 4, respectively) requiring surgical revision. Three eyes (12.5%) lost ≥2 lines of BCVA due to cataract progression after implantation. One eye developed blebitis (4.2%) 9 months after implantation due to an avascular bleb and resolved with topical antibiotics.
ICE
Lin et al38 presented 4 cases of eyes with ICE syndrome. Baseline IOP was 28.5 mmHg on 3.8 meds and decreased to 10.5 mmHg on 1.0 med. No additional surgery was required during the 6.9 months of follow-up. Two patients had transient hypotony, one that resolved with conservative treatment and another with concomitant choroidal effusions required AC viscoelastic injection with eventual resolution of the choroidal at 6.9 months. No implants were occluded by membranes or peripheral anterior synechiae.
Hohberger et al39 described a case report of a 53-year-old woman with ICE syndrome with corectopia who underwent previous DMEK surgery and CPC. Baseline IOP was 24 mmHg on maximal therapy. Subconjunctival anti-VEGF and 5-FU were used pre and postoperatively. At final follow-up (6 months), IOP was 12 mmHg on 1 med.
After Dexamethasone Implants
Rezkallah et al40 reported on five eyes of four consecutive cases of steroid induced glaucoma who underwent Xen 45 solo (3) or Xen combined (2) surgery and subsequent DEX-implants with no further increase in IOP increase with a mean follow-up of 5 months.
In Pediatric Glaucoma
Smith41 reports four cases of pediatric glaucoma treated with 3 ab interno and 1 ab externo Xen. One patient previously underwent cataract surgery and another had previous ab externo trabeculotomy. The patient with previous ab externo trabeculotomy failed the first Xen after 5 weeks and a second Xen was implanted through an ab externo route. The third case presented with a closed angle and underwent a Xen 45 combo. MMC concentration varied from 01 to 0.2 mL of 0.2 to 0.4 mg/mL. The length of follow-up ranged from 6 months to two years. In this small series no complications were reported.
Efficacy and Safety of Needling Revision
The needling rate reported in the different studies has been examined in the safety section for each individual study and only studies specifically addressing needlings revision are reported in this section.
Ferreira et al42 reported the first case where Xen early failure (IOP 26mmHg with a thickened non-diffuse bleb despite medical treatment) which was needled with trypan blue injected in the AC prior to the intervention. This case report highlights the advantages of injecting Trypan blue at the time of needling as it helps better assess when the flow is re-established. IOP was well controlled after needling with a diffuse bleb after 2 months.
Olivari et al43 described 3 cases of unintentional Xen amputation at the time of needling, resulting in a mean distal segment length of the truncated Xen of 0.83 (range: 0.7 to 1) mm. The mean IOP decreased from 25.0mmHg (range 21–30) before needling to 12.0mmHg (range 10 −14) after needling, with a mean follow-up of 15.3 (range: 11 to 18) months and no vision-threatening complications. These were encouraging as shortening of the device should theoretically decrease resistance and increase flow rate, according to the Poiseuille’s equation. Bustros et al44 illustrated a similar case in which the view was obstructed at the time of needling due to subconjunctival heme. At the end of the procedure a fragment of Xen (1.1 mm in length) was found under the conjunctiva. The Authors report a formed bleb up to one month after needling.
Midha et al45 performed a recent prospective interventional study about the efficacy of needling revision as a procedure of choice in the management of fibrotic blebs. Needling was performed with a 27G needle and MMC with 10% of concentration was injected subconjunctivally. One limitation of this study was that decision to needle was dependent upon the surgeon’s discretion. Fifty-one eyes (13 Xen 45 solo and 38 Xen 45 combo) with raised IOP associated with either a fibrotic or a shallow bleb or increased vascularity were enrolled in the study, while other causes of filtration failure (stent malposition, obstruction) were excluded. Glaucoma types were mainly POAG (n=21), and PXG (n=18). Comparing the solo and combo groups, no difference was found in the number of needlings (P=0.96), the time between surgery and needling (P = 0.23), or the time between the first and the second needling (P = 0.98). Overall 20 of 51 eyes (39.2%) required >1 needling revision, and 14 eyes (24.5%) required further surgery. Mean preoperative IOP was 22.3±8.2mmHg and decreased to 14.3±8.0mmHg at day 1 after surgery (−36.8%). Mean pre-needling IOP was 23.6±8.9mmHg, and it reduced to 12.1±4.2mmHg (−48.7%) at the first post-revision appointment. The primary outcome was the IOP percent reduction after needling at the last follow-up visit (on average 17.0±7.0 months after the first needling). A significant IOP reduction of 39.4% from prerevision baselines and of 35.9% from preoperative values was found, with a mean IOP of 14.3±4.1mmHg. Partial amputation of the Xen during needling occurred in 2 cases (3.9%). Hypotony with choroidal detachment occurred in 1 case (2%), and further 14 cases (27.5%) required further glaucoma surgery.
Trabeculectomy and Xen
Schlenker et al15 performed an international, multicenter, retrospective, interventional, cohort study. The Xen 45 solo group included 185 eyes and the trabeculectomy group169 eyes with a variety of glaucoma types including POAG (202, 57.1%), PXG (80, 22.6%), PACG (4, 1.1%) PDG (20, 5.6%), JOAG (12, 3.4%) and CMG (20, 5.6%) and NPG (8, 2.3%). Baseline characteristics were similar between groups except for more males (56% vs 43%), younger patients, better preoperative visual acuity, and more trabeculoplasty (52% vs 30%) in the Xen group. Before surgery 0.05 to 0.2 mL MMC of 0.2 mg/mL) was injected subconjunctivally (MMC soaked sponges were used for some of the trabeculectomy patients). The median preoperative IOP in the Xen group was 24.0 (19.0–30.0) mmHg and 24 (19.0 −32.0) mmHg in the trabeculectomy group which improved to 13.0 (11.0–16.0) mmHg in both groups at 12 months. The median number of baseline meds was 3.0 (3.0–4.0) for both groups and decreased to 0.0 (IQR, 0.0–0.0) meds in both groups. Complete success was defined IOP between 6 to 17 mm Hg without medications or with medication (qualified success) and with different IOP cutoffs of 6 to 21 mmHg. Postoperative intervention rates were 43% needling in the Xen group and 31% needling in the trabeculectomy group as well as 50% laser suture lysis. Reoperation rates were 10% (19) in the Xen group and 5% (9) in the trabeculectomy group (p=0.11). Complications were as follow in the Xen vs trabeculectomy group: hyphema 1.1% vs 1.2%; hypotony 1.1% vs 0.6%, choroidal detachment 0.5% vs 1.2%. Four microstent eyes and 2 trabeculectomy eyes developed malignant glaucoma. One trabeculectomy eye had blebitis that resolved with conservative treatment. The most common reoperation was repeat microstent insertion, followed by a Baerveldt tube shunt. Eyes with preoperative IOP of more than 21 mmHg, non-Caucasians and with BCVA of 0.4 logMAR or better appeared to perform better with the Xen and when preoperative IOP was 21 mmHg or less, Caucasians and with BCVA of 0.4 logMAR or worse appeared to perform better with the trabeculectomy.
XEN Post-Trabeculectomy
Karimi et al46 performed a 12 months multicenter retrospective case review of 17 eyes (3 Xen 45 solo and 14 Xen 45 combo) with prior failed trabeculectomy. The patients enrolled had POAG (13, 76.4%), secondary OAG (3, 17.6%) and other type of glaucoma (1, 5.8%). Pre-operative IOP was 21.5± 2.4 mmHg on 2.8±0.6 meds decreasing to 13.6±3.4 mmHg on to 1.0±1.3 meds. Complications included: numerical hypotony (4, 23.5%) that all resolved spontaneously, IOP spike of ≥ 30 mmHg (2, 11.8%) and transient occlusion of the implant by iris (1, 5.9%). Secondary filtration surgery (Baerveldt tube implantation) was required in 2 (11.8%) cases. Postoperative bleb intervention was required in 9 cases (52.9%), usually in the first month after surgery.
Trabeculectomy Post-Xen
Gizzi et al47 in a retrospective case series of 8 eyes (7 solo, 1 combo) described outcomes of trabeculectomy with MMC (0.2–0.4mg/mL) performed by 3 surgeons following a failed Xen (MMC 0.1–0.2mL of 0.1–0.4 mg/mL) with at least 6 months follow-up (median 10.5 (6–26) months). Glaucoma types were POAG (5, 62.5%), PXG (2, 25%) and uveitic (1, 12.5%). Median IOP was 29.0 (12–45) mmHg on 2.5 (0–5) meds decreasing to 7.5 (2–12) mmHg on 0 medications. At the time of Xen implantation, there were 2 intraoperative complications: one patient required a second Xen due to stent malposition and one patient required conjunctival opening to free the Xen under tissue. After Xen implantation, 4 cases had postoperative complications: 1 bleb leak, which resolved with a bandage contact lens, 1 AC shallowing needing viscoelastic injection and 2 IOP spikes (one treated medically and one requiring urgent trabeculectomy). Six patients required one or multiple needlings for suboptimal IOP. Reasons for trabeculectomy were inadequate IOP (7) and drop intolerance (1). At the time of trabeculectomy 1 patient had the Xen implant removed and 2 patients received an injection of bevacizumab in the AC. After trabeculectomy, 3 patients experienced transient bleb leaks. One patient required a trabeculectomy revision at 4 weeks for poorly controlled IOP.
Bleb Imaging
Fea et al48 performed a prospective 12-month study on patients with POAG, either alone or combined with cataract surgery. The primary aim was to examine bleb morphology using a variety of imaging techniques such as biomicroscopy, to measure bleb area, borders and vascularization; IVCM (HRT II/Rostock Cornea Module, RCM; Heidelberg Engineering, Inc, Franklin MA, USA) to measure the bleb area, density of intraepithelial microcysts and reflectivity of subepithelial connective tissue; AS-OCT (RTVue-100 Optovue, Inc, Fremont, CA, USA) to analyze macroscopically the morphology of the bleb. A postoperative IOP≤18mmHg without or on medications was respectively defined as complete and qualified success while an IOP>18mmHg was defined as failure. Twelve eyes of 11 patients were evaluated. At one year, 5 out of 10 patients available achieved a complete success while five were qualified success. AS-OCT showed that bleb wall reflectivity was significantly higher in the failure group; IVCM revealed that stromal density was significantly lower in the success group.
AS-OCT was also used by Lenzhofer et al49 to evaluate Xen bleb morphology in a prospective, single-center, single-armed cohort study over 12 months. The Authors classified bleb appearance using their own method into four different entities: uniform, subconjunctival separation, microcystic uniform and microcystic multiform. Uniform blebs in AS-OCTs showed higher IOPs at all examinations between week 1 (17.7±4.8 mmHg versus 11.3±7.1mmHg, p=0.001) and month 3 (16.4±6.1 versus 13.4±6.1, p=0.04). Subconjunctival tissue separation bleb morphology was associated with lower mean IOPs during the course of 12 months (r = 0.75, p = 0.031). Predictors for surgical failure at month 12 were microcystic multiform bleb morphology in AS-OCT at month 3 (60% versus 15%, relative risk 4.0, p = 0.043) and uniform bleb morphology at month 9 (33% versus 23%, relative risk 1.4, p = 0.015).
Predictors/Risk Factors
Identifying risk factors can help guide anti-fibrotic use, the number and timing of post-operative visit or eventually the exclusion of subtypes of patients. Better understanding of these factors can allow us to tailor our treatments.
In the study of Midha50 mean IOP at day 1 was significantly lower in Xen 45 solo group compared to the Xen 45 combo group, but this difference did not persist at 1 week. In the Xen 45 solo group, higher postoperative day 1 IOP lead to higher rate of needlings (OR: 1.14; 1.02–1.28) and total number of needlings (OR: 1.15; 1.06–1.26). In the solo group, an IOP >20 mmHg on day 1 increases the probability of needling to 80%. The probability of needling and the number of needlings was not influenced by age, type, severity of glaucoma and number of glaucoma medications. Success rates at 1 year were better in the Xen 45 solo group with 81% eyes achieving complete success versus 56.1% in Xen 45 combo group (p = 0.04) when lower IOP were measured at day one.
One study found female gender to have higher qualified success rates (female 68% vs male 39%).20 Although there was no difference in complete success rates (28% female vs 18% male).
Mansouri35 showed higher success in patients with PXG (HR 0.36; P = 0.043), lower baseline IOP (HR 1.16; P < 0.005) and more baseline medications (HR 0.62; P = 0.043). All other factors analyzed (age, sex, type of surgery, baseline MD) were not predictive of success.
Week 1 and month 1 IOP were associated with better success rates in a multicenter study by Fea.33 Patients with a week one IOP lower than 6, 8 or 10 mmHg had a significantly higher probability of success defined as an IOP ≤14, ≤16, or ≤18 mmHg at the final follow-up visit. In addition, patients with an IOP change of <6 mmHg between week 1 and month 1 had a higher chance of achieving an IOP ≤16 or ≤18 mmHg at the final follow-up. Number of needlings were significantly correlated with day 1 (r = 0.24, P =.006), week 1 (r = 0.27, P <.001), and month 1 (r = 0.32, P <.0001) postoperative IOP. Patients who did not undergo needling had a chance of achieving complete success with IOP ≤14 mmHg (68.8% vs 46.7%), ≤16 mmHg (66.7% vs 41.9%) and ≤18 mmHg (66.7% vs 39.3%).
Endothelial Cell Loss
Fea et al48 prospectively evaluated 12 eyes of 11 patients over one year. Ten eyes underwent a solo procedure. At the end of the study there were no differences in terms of endothelial cell count, although cell hexagonality increased significantly.
Gillmann et al51 in a retrospective study compared the effect on ECD of Xen 45 combo (n=17) with that of a standard phacoemulsification (phacoemulsification) (n=15) over 24 months. ECDs at baseline were 2568±491 cells/mm2 in the Xen 45 combo group and 2379±335 in the phacoemulsification group and decreased by 14.5% in the Xen combo group and 14.3% in the phaco group at 24 months. There was no change in ECD in patients receiving needlings. A risk factor for ECD loss in both groups was the presence of a shallow anterior chamber preoperatively (VH grade ≤ 3) with a mean ECD loss in shallow anterior chambers of 37.9±11.5% vs 10.1±9.2%.
Case Report/Small Case Series
Dislocation
Dervenis et al52 presented a case of Xen dislocation into the anterior chamber in a 45-year-old female with asthma, eczema and multiple allergies. Six months post-surgery she developed episcleritis and one month later the device was noted in the anterior chamber angle.
Gillman reported a case a Xen dislocation due to probable eye rubbing. ECC measurements taken monthly showed a more important drop the month of the dislocation (2.1%) before the device was replaced.
Dysesthetic Bleb
Yavuzer et al53 reported a case of a 75-year-old male patient with PXG who underwent a Xen 45 combo with 0.1 mL 0.2 mg/mL of MMC. Three months postoperatively, unmedicated IOP varied between 9 and 13 mmHg. However, the bleb extended in the nasal quadrant causing mechanical ectropion of the lower eyelid. Compression sutures were required to limit the extent of the bleb.
Refractory Patients After Previously Failed Glaucoma Surgeries
Sandhu et al54 presented a case report with a 44-year-old man with juvenile chronic open-angle glaucoma previously unsuccessfully treated with selective laser trabeculoplasty, trabeculectomy, an infero-nasally placed Ahmed and a revision of the Ahmed valve, who finally reached a medicated pressure of 17 mmHg one year post-surgery.
A case report of Tailor et al55 was about a 72-year-old man with neovascular glaucoma who was successfully treated with XEN 45 and after CPC and bevacizumab injection. His pressure was 13 mmHg without meds at 24 months.
Endophthalmitis
Karri et al56 presented a case of endophthalmitis 4 months after surgery with an exposed Xen. The stent was removed and a pars plana vitrectomy with intravitreal antibiotics were performed.
Two cases of endophthalmitis were reported by Olgun et al.57 A 68-year-old women with blepharitis, underwent a Xen implant and developed endophthalmitis at 5 month postoperatively. Her bleb was of moderate height, spanning over 1 to 2 clock hours with an avascular zone (no obvious purulent material) and IOP of 42 mmHg. She was initially treated with medical therapy and eventually required vitrectomy with ceftazidime injection and silicone oil tamponade. The XEN was retained. Three months later, the device was correctly positioned and the IOP was 15 mmHg. A 80-year-old male underwent Xen implant and developed endophthalmitis and a Xen erosion at 4 month postoperatively. He required vitrectomy with silicone oil and Xen removal. At last follow-up, his IOP was 20 mmHg without medication.
Intraluminal Obstruction
Rigo58 reported the OCT findings of 46 eyes (39 patients) retrospectively evaluated 6 months or more after an uneventful Xen. Possible intraluminal obstructions evidenced by hyper-reflective material on OCT were identified in 16 eyes (15 POAG eyes and 1 PXG) with unremarkable slit-lamp exams in. In two cases the material was either in the internal lumen or near the subconjunctival portion of the implant suggesting that the obstruction may be originating from the anterior chamber. Despite these obstructions, IOPs were controlled and no further intervention was warranted.
Suprachoroidal Hemorrhage
Prokosch-Willing et al59 reported a case of an 84-year old female patient with PXG on maximal therapy who underwent XEN implant with MMC 0.1 mL of 0.2 mg/mL. On postoperative day 1, IOP was 4 mmHg with a deep anterior chamber and a small shallow bleb. On day 2, patient presented with sudden pain and IOP increased to 54 mmHg with a flat anterior chamber and a suprachoroidal hemorrhage. The patient was observed and treated topically with a resolution of the bleed after 6 weeks. Vision decreased from 20/200 preoperatively to hand motion.
Hyphema
Rezkallah et al60 reported a case of 72-year-old male who presented with a total hyphema two days after uneventful Xen implant. The patient was on anticoagulants with an international normalized ratio between 2 and 3. The patient was on fluid restriction (1.5L/day) and told to lie with an elevated head. The hyphema resolved after 1 month spontaneously with IOP of 11mmHg and 20/20 vision.
Degradation
Widder et al61 presented a 63-year-old woman with Xen implant requiring revision 3 years after surgery after having had two failed previous revision. At the time of revision, the conjunctiva was opened and the implant was stripped of the adhesive scar tissues. No flow was seen through the stent and thus, removed. The intrascleral and intracameral portions had degraded with an irregular surface and the lumen in the middle of the stent was obstructed.
Conjunctival Erosion
Lapira et al62 reported a case of a Xen 45 solo in a pseudophakic 87-year-old man with PXG and a previous failed trabeculectomy. Three and a half months postoperatively, he presented with a 24-hour history of pain and reduced vision in his left eye after an episode of eye rubbing. The Xen was eroded through conjunctiva and broken. It was removed and treated with antibiotics and vitrectomy for endophthalmitis. After treatment, IOP was 20 mmHg with topical therapy.
Arnould et al63 reported a case of recurrent conjunctival erosion and Xen exposure treated with a conjunctival autograft. The patient had 0.1 mL of 0.2 mg/mL of MMC at time of surgery and underwent one needling 0.1 mL of 0.1 mg/mL MMC at month 1. After two months a surgical revision was performed, and the Xen remained exposed with a bleb leak. A free conjunctival autograft covered with an amniotic membrane graft was then performed and one month later IOP was 13 on 2 medications with a diffuse bleb.
Fea et al64 reported a case of Xen implant in a patient with a previously failed trabeculectomy and a scarred superior bleb. The stent was placed nasal to the previous bleb. Despite adequate IOP control, the stent exposed due to the thin conjunctiva and nasal bleb. An amniotic membrane was used to cover the defect with a conjunctiva autograft. At six months postoperatively, the unmedicated IOP was 14 mmHg with stable vision.
Salinas et al65 described a case of a PXG patient who underwent bilateral combined cataract and Xen implantation. One month postoperatively, the patient presented with a flat bleb and an extruded Xen in one eye, which was successfully treated with medical therapy (vitamin A ointment). The fellow eye Xen extruded two weeks later and the medical therapy proved ineffective. After a subconjunctival injection of 1 mL of MMC 0.02% a second Xen was implanted ab interno and the first Xen was removed, with dissection of scar tissue, and suturing of the conjunctiva. One month later, IOP was 15 mmHg without any medications and with a diffuse bleb over the second implant with no leakage.
Olate-Perez6 described a case of erosion 18 months after surgery in a 78-year-old woman. During revision, the Xen was amputated flush with the sclera and the conjunctiva was closed. IOP was eventually controlled on meds after revision.
Acknowledgments
Editorial assistance was provided to the authors by Melanie Gatt (PhD), an independent medical writer, on behalf of Health Publishing & Services Srl and funded by Allergan plc, Dublin, Ireland, at the request of the investigator.
Disclosure
Dr Antonio M Fea reports Consultant fees from Glaukos, Ivantis, ELTSight, iSTAR, and EyeD, travel fess from Johnson and Johnson, Allergan, and Sooft, outside the submitted work. Dr Georges M Durr report personal fees from Alcon, Allergan, Bausch & Lomb, Glaukos, Novartis, MST, Santen, and Sight Sciences, outside the submitted work. Dr Ike Ahmed reports the following, C- Consultant/Consulting Fees S- Speakers Honoraria R- Research Grant/Support; Aequus: C, Aerie Pharmaceuticals: C, R, Akorn: C, Alcon: C,S,R, Allergan: C,S,R, ArcScan: C, Bausch Health: C, Beaver Visitec: C, Beyeonics: C, Camras Vision: C, R, Carl Zeiss Meditec: C,S, CorNeat Vision: C, Ellex: C, ELT Sight: C, ElutiMed: C, Equinox: C, Genentech: C, Glaukos: C, R, Gore: C, InjectSense: C, Iridex: C, iStar: C, Ivantis: C, R, Johnson & Johnson Vision: C, S, R, KeLoTec: C, LayerBio: C, Leica Microsystems: C, MicroOptx: C, MST Surgical: C, S, Mundipharma: S, Mynosys: C, New World Medical: C, R, Ocular Instruments: C, Ocular Therapeutix: C, Omega Ophthalmics: C, PolyActiva: C, Sanoculis: C, Santen: C, R, Science Based Health: C, Sight Sciences: C, Stroma: C, Thea Pharma: C, ViaLase: C, Vizzario: C. The authors report no other conflicts of interest in this work.
References
1. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
2. Leung EW, Medeiros FA, Weinreb RN. Prevalence of ocular surface disease in glaucoma patients. J Glaucoma. 2008;17(5):350–355. doi:10.1097/IJG.0b013e31815c5f4f
3. Fechtner RD, Godfrey DG, Budenz D, Stewart JA, Stewart WC, Jasek MC. Prevalence of ocular surface complaints in patients with glaucoma using topical intraocular pressure-lowering medications. Cornea. 2010;29(6):618–621. doi:10.1097/ICO.0b013e3181c325b2
4. Harasymowycz PJ, Papamatheakis DG, Latina M, De Leon M, Lesk MR, Damji KF. Selective laser trabeculoplasty (SLT) complicated by intraocular pressure elevation in eyes with heavily pigmented trabecular meshworks. Am J Ophthalmol. 2005;139(6):1110–1113. doi:10.1016/j.ajo.2004.11.038
5. Bettis DI, Whitehead JJ, Farhi P, Zabriskie NA. Intraocular pressure spike and corneal decompensation following selective laser trabeculoplasty in patients with exfoliation glaucoma. J Glaucoma. 2016;25(4):e433–437. doi:10.1097/IJG.0000000000000340
6. Kotecha A, Feuer WJ, Barton K, Gedde SJ. Quality of life in the tube versus trabeculectomy study. Am J Ophthalmol. 2017;176:228–235. doi:10.1016/j.ajo.2017.01.019
7. Gedde SJ, Singh K, Schiffman JC, Feuer WJ. The tube versus trabeculectomy study: interpretation of results and application to clinical practice. Curr Opin Ophthalmol. 2012;23(2):118–126. doi:10.1097/ICU.0b013e32834ff2d1
8. Pfeiffer N, Garcia-Feijoo J, Martinez-de-la-Casa JM, et al. A randomized trial of a schlemm’s canal microstent with phacoemulsification for reducing intraocular pressure in open-angle glaucoma. Ophthalmology. 2015;122(7):1283–1293. doi:10.1016/j.ophtha.2015.03.031
9. Hoeh H, Vold SD, Ahmed IK, et al. Initial clinical experience with the CyPass micro-stent: safety and surgical outcomes of a novel supraciliary microstent. J Glaucoma. 2016;25(1):106–112. doi:10.1097/IJG.0000000000000134
10. Lewis RA. Ab interno approach to the subconjunctival space using a collagen glaucoma stent. J Cataract Refract Surg. 2014;40(8):1301–1306. doi:10.1016/j.jcrs.2014.01.032
11. Fea AM, Ahmed II, Lavia C, et al. Hydrus microstent compared to selective laser trabeculoplasty in primary open angle glaucoma: one year results. Clin Exp Ophthalmol. 2017;45(2):120–127. doi:10.1111/ceo.12805
12. Sheybani A, Reitsamer H, Ahmed II. Fluid dynamics of a novel micro-fistula implant for the surgical treatment of glaucoma. Invest Ophthalmol Vis Sci. 2015;56(8):4789–4795. doi:10.1167/iovs.15-16625
13. Yu D-Y, Morgan WH, Sun X, et al. The critical role of the conjunctiva in glaucoma filtration surgery. Prog Retin Eye Res. 2009;28(5):303–328. doi:10.1016/j.preteyeres.2009.06.004
14. Sheybani A, Dick HB, Ahmed II. Early clinical results of a novel ab interno gel stent for the surgical treatment of open-angle glaucoma. J Glaucoma. 2016;25(7):e691–696. doi:10.1097/IJG.0000000000000352
15. Schlenker MB, Gulamhusein H, Conrad-Hengerer I, et al. Efficacy, safety, and risk factors for failure of standalone ab interno gelatin microstent implantation versus standalone trabeculectomy. Ophthalmology. 2017;124(11):1579–1588. doi:10.1016/j.ophtha.2017.05.004
16. Widder RA, Dietlein TS, Dinslage S, Kuhnrich P, Rennings C, Rossler G. The XEN45 Gel Stent as a minimally invasive procedure in glaucoma surgery: success rates, risk profile, and rates of re-surgery after 261 surgeries. Graefes Arch Clin Exp Ophthalmol. 2018;256(4):765–771. doi:10.1007/s00417-018-3899-7
17. Yu JTS, Au L. Conjunctival bleb compression as a treatment for hypotony post XEN45 implant in uveitic glaucoma. Eur J Ophthalmol. 2019;1120672119836339.
18. Sng CC, Wang J, Hau S, Htoon HM, Barton K. XEN-45 collagen implant for the treatment of uveitic glaucoma. Clin Exp Ophthalmol. 2018;46(4):339–345. doi:10.1111/ceo.13087
19. Sheybani A, Lenzhofer M, Hohensinn M, Reitsamer H, Ahmed IIK. Phacoemulsification combined with a new ab interno gel stent to treat open-angle glaucoma: pilot study. J Cataract Refract Surg. 2015;41(9):1905–1909. doi:10.1016/j.jcrs.2015.01.019
20. Lenzhofer M, Kersten-Gomez I, Sheybani A, et al. Four-year results of a minimally invasive transscleral glaucoma gel stent implantation in a prospective multi-centre study. Clin Exp Ophthalmol. 2019;47(5):581–587. doi:10.1111/ceo.13463
21. Tan SZ, Walkden A, Au L. One-year result of XEN45 implant for glaucoma: efficacy, safety, and postoperative management. Eye (Lond). 2018;32(2):324–332. doi:10.1038/eye.2017.162
22. Grover DS, Flynn WJ, Bashford KP, et al. Performance and safety of a new Ab interno gelatin stent in refractory glaucoma at 12 months. Am J Ophthalmol. 2017;183:25–36. doi:10.1016/j.ajo.2017.07.023
23. Perez-Torregrosa VT, Olate-Perez A, Cerda-Ibanez M, et al. Combined phacoemulsification and XEN45 surgery from a temporal approach and 2 incisions. Arch Soc Esp Oftalmol. 2016;91(9):415–421. doi:10.1016/j.oftal.2016.02.006
24. De Gregorio A, Pedrotti E, Russo L, Morselli S. Minimally invasive combined glaucoma and cataract surgery: clinical results of the smallest ab interno gel stent. Int Ophthalmol. 2018;38(3):1129–1134. doi:10.1007/s10792-017-0571-x
25. Hengerer FH, Kohnen T, Mueller M, Ab Interno C-HI. Gel implant for the treatment of glaucoma patients with or without prior glaucoma surgery: 1-year results. J Glaucoma. 2017;26(12):1130–1136. doi:10.1097/IJG.0000000000000803
26. Ozal SA, Kaplaner O, Basar BB, Guclu H, Ozal E. An innovation in glaucoma surgery: XEN45 gel stent implantation. Arq Bras Oftalmol. 2017;80(6):382–385. doi:10.5935/0004-2749.20170093
27. Heidinger A, Schwab C, Lindner E, Riedl R, Mossbock G, Retrospective A. Study of 199 Xen45 stent implantations from 2014 to 2016. J Glaucoma. 2019;28(1):75–79. doi:10.1097/IJG.0000000000001122
28. Karimi A, Lindfield D, Turnbull A, et al. A multi-centre interventional case series of 259 ab-interno Xen gel implants for glaucoma, with and without combined cataract surgery. Eye (Lond). 2019;33(3):469–477. doi:10.1038/s41433-018-0243-8
29. Galal A, Bilgic A, Eltanamly R, Osman A. XEN glaucoma implant with mitomycin C 1-year follow-up: result and complications. J Ophthalmol. 2017;2017:5457246. doi:10.1155/2017/5457246
30. Mansouri K, Guidotti J, Rao HL, et al. Prospective evaluation of standalone XEN gel implant and combined phacoemulsification-XEN gel implant surgery: 1-year results. J Glaucoma. 2018;27(2):140–147. doi:10.1097/IJG.0000000000000858
31. Hohberger B, Welge-Lussen UC, Lammer R. MIGS: therapeutic success of combined Xen Gel Stent implantation with cataract surgery. Graefes Arch Clin Exp Ophthalmol. 2018;256(3):621–625. doi:10.1007/s00417-017-3895-3
32. Reitsamer H, Sng C, Vera V, Lenzhofer M, Barton K, Stalmans I. Two-year results of a multicenter study of the ab interno gelatin implant in medically uncontrolled primary open-angle glaucoma. Graefes Arch Clin Exp Ophthalmol. 2019;257(5):983–996. doi:10.1007/s00417-019-04251-z
33. Fea AM, Bron AM, Economou MA, et al. A real-life prospective study on the efficacy of the XEN 45 stent: a European study. J Cataract Refract Surg. 2020.
34. Ibanez-Munoz A, Soto-Biforcos VS, Chacon-Gonzalez M, et al. One-year follow-up of the XEN(R) implant with mitomycin-C in pseudoexfoliative glaucoma patients. Eur J Ophthalmol. 2019;29(3):309–314. doi:10.1177/1120672118795063
35. Mansouri K, Gillmann K, Rao HL, Guidotti J, Mermoud A. Prospective evaluation of XEN gel implant in eyes with pseudoexfoliative glaucoma. J Glaucoma. 2018;27(10):869–873. doi:10.1097/IJG.0000000000001045
36. Gillmann K, Bravetti GE, Mermoud A, Rao HL, Mansouri K. XEN gel stent in pseudoexfoliative glaucoma: 2-year results of a prospective evaluation. J Glaucoma. 2019;28(8):676–684. doi:10.1097/IJG.0000000000001295
37. Qureshi A, Jones NP, Au L. Urgent management of secondary glaucoma in uveitis using the Xen-45 gel stent. J Glaucoma. 2019;28(12):1061–1066. doi:10.1097/IJG.0000000000001389
38. Lin MM, Morgan WH, Kolomeyer NN, et al. XEN gel stent to treat ICE syndrome: 4 cases. J Glaucoma. 2019;28(12):1090–1094. doi:10.1097/IJG.0000000000001341
39. Hohberger B, Welge-Luen UC, Lammer R. ICE-syndrome: a case report of implantation of a microbypass xen gel stent after DMEK transplantation. J Glaucoma. 2017;26(2):e103–e104. doi:10.1097/IJG.0000000000000584
40. Rezkallah A, Mathis T, Denis P, Kodjikian L. XEN gel stent to treat intraocular hypertension after dexamethasone-implant intravitreal injections: 5 cases. J Glaucoma. 2019;28(1):e5–e9. doi:10.1097/IJG.0000000000001092
41. Smith OU, Grover DS, Emanuel ME, Godfrey DG, Fellman RL. XEN gel stent in pediatric glaucoma. J Glaucoma. 2020;29(4):e19–e22. doi:10.1097/IJG.0000000000001453
42. Ferreira NP, Pinto JM, Teixeira F, Pinto LA, Gel Stent XEN. Early failure-dye-enhanced Ab-externo revision. J Curr Glaucoma Pract. 2018;12(3):139–141. doi:10.5005/jp-journals-10078-1237
43. Olivari S, Cutolo CA, Negri L, et al. XEN implant fracture during needling procedure. J Glaucoma. 2019;28(12):1086–1089. doi:10.1097/IJG.0000000000001360
44. Bustros Y, Chaudhary A, Salinas L, Mansouri K. Cutting the subconjunctival fragment of the XEN gel implant during needling procedure. Eur J Ophthalmol. 2020;30(1):Np11–np15. doi:10.1177/1120672118805876
45. Midha N, Gillmann K, Chaudhary A, Mermoud A, Mansouri K. Efficacy of needling revision after XEN gel stent implantation: a prospective study. J Glaucoma. 2020;29(1):11–14. doi:10.1097/IJG.0000000000001394
46. Karimi A, Hopes M, Martin KR, Lindfield D. Efficacy and safety of the Ab-interno Xen gel stent after failed trabeculectomy. J Glaucoma. 2018;27(10):864–868. doi:10.1097/IJG.0000000000001044
47. Gizzi C, Mohamed-Noriega J, Elkarmouty A, Scott A. Trabeculectomy following failed Ab interno gelatin microstent: case series. J Glaucoma. 2018;27(10):e168–e173. doi:10.1097/IJG.0000000000001000
48. Fea AM, Spinetta R, Cannizzo PML, et al. Evaluation of Bleb morphology and reduction in IOP and glaucoma medication following implantation of a novel gel stent. J Ophthalmol. 2017;2017:9364910. doi:10.1155/2017/9364910
49. Lenzhofer M, Strohmaier C, Hohensinn M, et al. Longitudinal bleb morphology in anterior segment OCT after minimally invasive transscleral ab interno Glaucoma Gel Microstent implantation. Acta Ophthalmol. 2019;97(2):e231–e237. doi:10.1111/aos.14167
50. Midha N, Rao HL, Mermoud A, Mansouri K. Identifying the predictors of needling after XEN gel implant. Eye (Lond). 2019;33(3):353–357. doi:10.1038/s41433-018-0206-0
51. Gillmann K, Bravetti GE, Rao HL, Mermoud A, Mansouri K. Impact of combined XEN gel stent implantation on corneal endothelial cell density: 2-year results. J Glaucoma. 2019;28(6):e93–e95. doi:10.1097/IJG.0000000000001200
52. Dervenis N, Mikropoulou AM, Dervenis P, Lewis A. Dislocation of a previously successful XEN glaucoma implant into the anterior chamber: a case report. BMC Ophthalmol. 2017;17(1):148. doi:10.1186/s12886-017-0540-1
53. Yavuzer K, Mesen A. The treatment of a hypertrophic bleb after XEN gel implantation with the “Drainage channel with sutures” method: a case report. BMC Ophthalmol. 2019;19(1):245. doi:10.1186/s12886-019-1249-0
54. Sandhu S, Dorey MW. Case report: xen Ab interno gel stent use in a refractory glaucoma patient with previous filtration surgeries. J Glaucoma. 2018;27(3):e59–e60. doi:10.1097/IJG.0000000000000864
55. Tailor R, Lalias TA. Case of refractory neovascular glaucoma treated with a XEN 45 implant. J Glaucoma. 2018;27(10):929–930. doi:10.1097/IJG.0000000000001033
56. Karri B, Gupta C, Mathews D. Endophthalmitis Following XEN Stent Exposure. J Glaucoma. 2018;27(10):931–933. doi:10.1097/IJG.0000000000001012
57. Olgun A, Imamoglu S, Karapapak M, Duzgun E, Kacar H. Endophthalmitis after XEN gel stent implantation: 2 cases. J Glaucoma. 2018;27(12):e191–e194. doi:10.1097/IJG.0000000000001076
58. Rigo J, Castany M, Banderas S, Pujol O, Amilburu M, Dou A. Possible intraluminal obstruction of the XEN45 gel stent observed with anterior segment optical coherence tomography. J Glaucoma. 2019;28(12):1095–1101. doi:10.1097/IJG.0000000000001351
59. Prokosch-Willing V, Vossmerbaeumer U, Hoffmann E, Pfeiffer N. Suprachoroidal bleeding after XEN gel implantation. J Glaucoma. 2017;26(12):e261–e263. doi:10.1097/IJG.0000000000000795
60. Rezkallah A, Mathis T, Denis P, Kodjikian L. XEN gel stent: a total delayed-onset postoperative hyphema. Int J Ophthalmol. 2019;12(7):1224–1226. doi:10.18240/ijo.2019.07.27
61. Widder RA, Kuhnrich P, Hild M, Rennings C, Szumniak A, Rossler GF. Intraocular degradation of XEN45 gel stent 3 years after its implantation. J Glaucoma. 2019;28(12):e171–e173. doi:10.1097/IJG.0000000000001364
62. Lapira M, Cronbach N, Shaikh A. Extrusion and breakage of XEN gel stent resulting in endophthalmitis. J Glaucoma. 2018;27(10):934–935. doi:10.1097/IJG.0000000000001058
63. Arnould L, Theillac V, Moran S, Gatinel D, Grise-Dulac G-DA. Recurrent exposure of XEN gel stent implant and conjunctival erosion. J Glaucoma. 2019;28(3):e37–e40. doi:10.1097/IJG.0000000000001146
64. Fea A, Cannizzo PM, Consolandi G, Lavia CA, Pignata G, Grignolo FM. Managing drawbacks in unconventional successful glaucoma surgery: a case report of stent exposure. Case Rep Ophthalmol Med. 2015;2015:847439.
65. Salinas L, Chaudhary A, Guidotti J, Mermoud A, Mansouri K. Revision of a leaking bleb with XEN gel stent replacement. J Glaucoma. 2018;27(1):e11–e13. doi:10.1097/IJG.0000000000000811
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.