Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 12
Vitiligo – New Treatment Approach
Authors Konstantinova VA, Olisova OY, Gladko VV ![]() , Burova EP
, Burova EP ![]()
Received 31 August 2019
Accepted for publication 15 November 2019
Published 18 December 2019 Volume 2019:12 Pages 911—917
DOI https://doi.org/10.2147/CCID.S229175
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Video abstract presented by Veronika Konstantinova.
Views: 343258
Veronika A Konstantinova,1 Olga Yu Olisova,2 Victor V Gladko,3 Ekaterina P Burova2–4
1Dermatology and Cosmetology Department Dao Clinic, Leninskiy Prospekt, Moscow 119119, Russia; 2Rakhmanov Department of Dermatology and Venereal Diseases, I.M.Sechenov First Moscow State Medical University of the Russian Federation, Moscow 119435, Russia; 3Department of Dermatology, Venereology and Cosmetology Medical Institute of Continuing Medical Education, Moscow State University of Food Production, Moscow 125080, Russia; 4Dermatology Department Bedford Hospital NHS Trust, South Wing, Bedford MK42 9DJ, UK
Correspondence: Ekaterina P Burova
Dermatology Department Bedford Hospital NHS Trust, South Wing, 27 Rothsay Road, Bedford MK40 3PT, UK
Tel +447771857936
Email [email protected]
Introduction: Vitiligo is one of the most common hypomelanoses. Current treatments include ultraviolet, topical corticosteroids, calcineurin inhibitors. Orally administered vitamins, acting as anti-oxidants and in combination with ultraviolet light have also demonstrated skin re-pigmentation. In our pilot study of seven patients, we injected skin affected with vitiligo intra-dermally with a complex of vitamins and minerals and assessed the outcome.
Aim: The aim of this study was to evaluate a novel treatment modality for vitiligo.
Methods: We present a pilot study of seven patients; each having been diagnosed with generalized progressive vitiligo. In all cases, multiple therapies had been previously attempted. All patients were subjected to intradermal injections of biorevitalizant NCTF 135 (3 mls) in the hypo-pigmented areas of skin, once a week for 5 weeks. A 30Gx13 mm needle was used for the 0.025 mls intradermal injections to create micro-papules with a 1 cm distance between the injection sites. The results were assessed at 2 weeks and 5 weeks and were considered successful if partial or complete repigmentation was achieved.
Results: Partial or complete skin re-pigmentation post-treatment was observed in vitiligo macules of all patients (100%). No significant side effects, or exacerbation of vitiligo were observed during or after treatment with NCTF 135 in the following 6 months (five patients) and 12 months (two patients).
Discussion: Increasing the armamentarium of new treatments of vitiligo is important. Previous studies showed the effectiveness of oral and intramuscularly injected multivitamins in the treatment of vitiligo, explaining the results by the antioxidative qualities of the above. Our study demonstrated that intradermal mesotherapy injections of NCTF135, rich with vitamins and other antioxidants are well tolerated and effective in achieving significant re-pigmentation of de-pigmented skin in all patients studied, including five who had been resistant to previous standard therapies.
Keywords: antioxidants, vitamins and minerals, mesotherapy
Introduction
Vitiligo is one of the most common hypomelanoses with an incidence of 0.5–2% in the general population.1 The common age of onset of this condition is below 20, although it may occur at any stage of life. The dyschromia presents with depigmented macules, due to loss of melanocytes from the cutaneous epidermis or loss of the ability to secrete melanin.2 This occurs secondary to the deficit of tyrosinase enzyme in melanocytes, which stimulates the process of pigment formation. The psychological and emotional impact on the patients affected by this condition can be overwhelming, and requires development of new, more effective, treatment options.
The absence of a unified approach to the causes of vitiligo makes it challenging to choose the best treatment modality and to predict its effectiveness. There are multiple theories of the pathogenesis of vitiligo. They include genetic, neurogenic, autoimmune, oxidative stress and other theories.3 A number of factors, such as ultraviolet (UV) radiation, psychological and emotional stress, changes in the functional state of the peripheral nervous system are implicated as triggers of the condition.
One of the most recent theories is the oxidative stress theory. It stipulates that oxygen radicals (not oxygen itself) are the main cause of apoptosis of melanocytes. Normally the formation and decomposition of active forms of oxygen are balanced up and do not accumulate in cells. The levels of free radicals may rise due to the increase in the rate of their production or cells’ reduced ability to neutralize them.4 The combination of these processes creates the conditions for oxidative stress.
One of the triggering mechanisms for the formation of reactive oxygen species (ROS) in the body is ultraviolet radiation. In reasonable doses, it stimulates melanogenesis, but when the potency and duration of the radiation increases, melanocytes can get damaged. The quantum of light that has been absorbed by the tissues destabilizes the molecules and leads to the formation of endogenous toxic agents - ROS. They reduce the functional activity of melanocytes and cause their apoptosis.6,7
The incidental observation of the response to mesotherapy with NCTF135 (Laboratoires Filorga) in the areas affected with vitiligo and a subsequent analysis of the product’s composition, prompted the idea of using it as an antioxidant in the treatment of vitiligo. NCTF135 is a complex of 55 active ingredients (13 vitamins, 23 amino acids, 6 minerals, 6 nucleotides, co-enzymes, glutathione and 0.025 mg/mL hyaluronic acid).
The antioxidant system of the human body is a complex mechanism which provides extracellular and intracellular protection. It is represented by non-enzyme substances (natural antioxidants): tocopherols, carotenoids, ascorbic acid, uric acid, glutathione, and by active enzymes: superoxide dismutase, catalase, transferase, etc.8,9 NCTF135 includes such antioxidants as glutathione, hyaluronic and ascorbic acid, tocopherol (vitamin E). All of them are the most important elements in the cellular protection from ROS. The increase of the intracellular concentration of glutathione stimulates antioxidant cells’ protection and improves cellular metabolism. Hyaluronic acid activates neo-angiogenesis and improves skin microcirculation in the areas of injections. This improves absorption of vitamins and microelements when they are injected. Cell proliferation is activated and the main metabolic processes in the cells become more intense. It has been shown that the vitiligo macules are not completely devoid of melanocytes, and that their activity can be restored following the effects of some stimuli.10 We hypothesized that NCTF135 is effective, because during its manufacture all components are stored in the active form through using double extraction purification. NCTF135 does not contain stabilizers, preservatives, dyes or fragrances, and this reduces the risks of allergic reactions. NCTF135 is licensed for skin rejuvenation, treatment of acne and alopecia.
There are no reports in the literature of the use of mesotherapy injections in the foci of vitiligo. The search criteria included PubMed search for “vitiligo treatment”, “vitiligo and mesotherapy”, “vitiligo and hyaluronic acid”. Vitiligo is not listed amongst the indications for the use of the preparation NCTF135.
Patients and Methods
We observed a group of seven females, aged from 25 to 54 years, with a diagnosis of generalized vitiligo, who attended the clinic for the purpose of skin rejuvenation using mesotherapy. All our patients presented with multiple white macules of different shapes and sizes on the face, neck, body, arms and legs. Six of them had onset of vitiligo in childhood, and one patient developed it during pregnancy. At the time of initiation of therapy, the disease was progressive in all patients. None of them had a family history of vitiligo.
All patients were examined for any other comorbidities. Full blood count, liver function test, urea and electrolytes, blood glucose, thyroid function and antibody profiles, including thyroid antibodies, and thyroid ultrasound were performed. Two patients had raised antithyroid peroxidase and thyroglobulin (threefold raised in one and 50-fold raised in the other patient) antibodies. They were consulted by an endocrinologist and diagnosed with an autoimmune thyroiditis. The thyroid function was normal in both cases and did not require treatment.
Five patients tried other treatments for vitiligo before the course of mesotherapy. The nature of treatments, their effectiveness and free treatment time before mesotherapy are listed in Table 1.
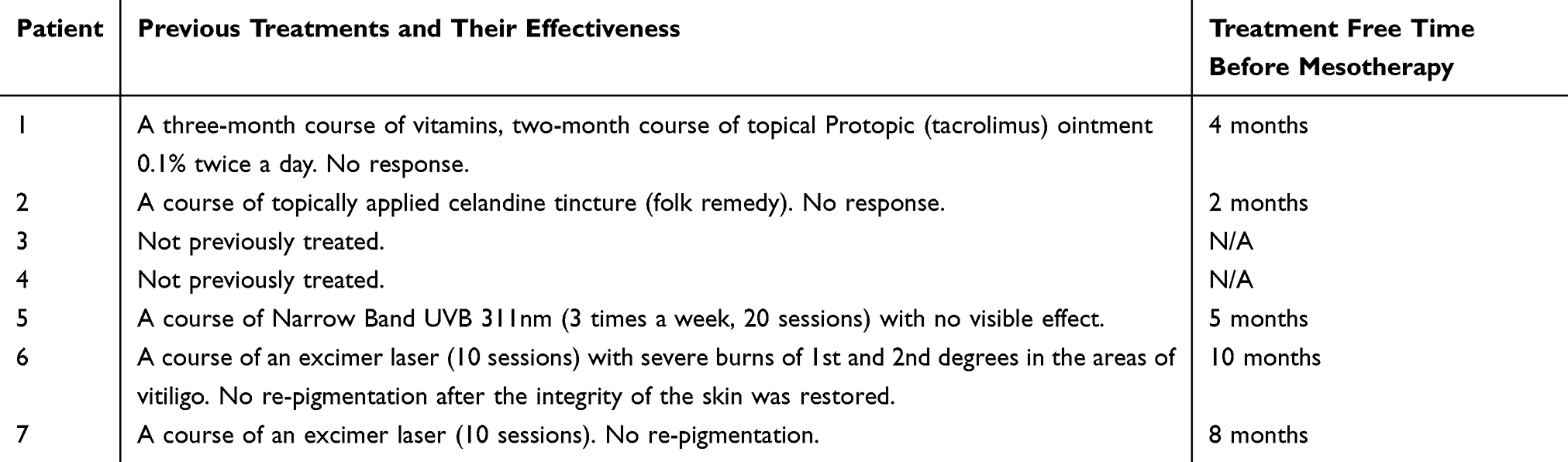 |
Table 1 Treatments Prior to Mesotherapy |
Despite, or due to, the lack of clinical improvement after previous therapies, all patients were very keen to explore other treatments.
At initial presentation, depigmented white macules were localized on the skin of the periorbital and perioral areas, neck and upper chest, hands, axillae and medial surfaces of the thighs (Figure 1A, 2А, 3А, 4А and B). Photographs of the lesions were taken before and 2 weeks after treatment.
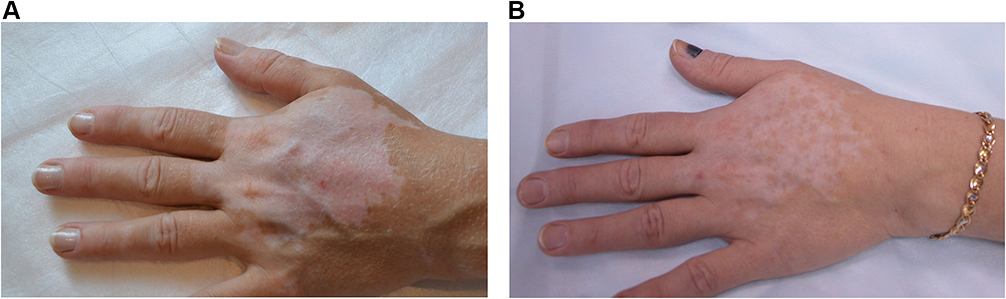 |
Figure 1 Patient A, area of vitiligo on the hands (A) before and (B) 2 weeks after treatment with NCTF135. |
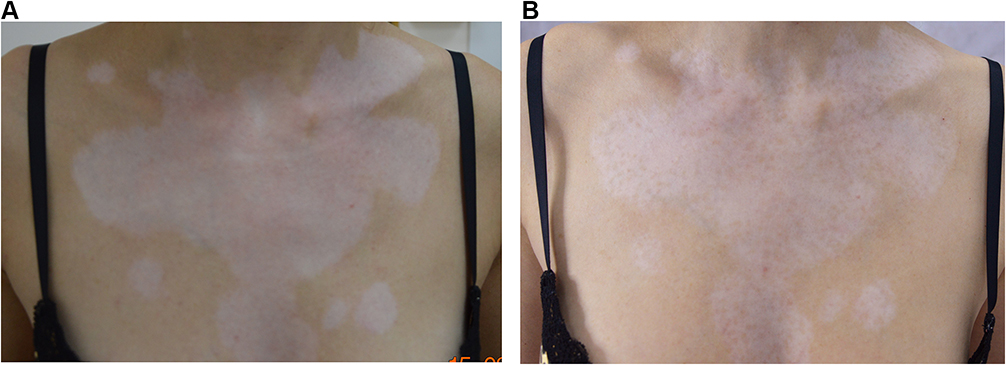 |
Figure 2 Patient A, areas of vitiligo on the chest (A) before and (B) 2 weeks after treatment with NCTF135. |
 |
Figure 3 Patient B, areas of vitiligo on the upper chest (A) before and (B) 2 weeks after treatment with NCTF135. |
 |
Figure 4 Patient L, areas of vitiligo on the face (A) and the neck (B) before the treatment with NCTF135. |
Protocol of Procedure
Written informed consent was provided by the participants prior to receiving the treatment with NCTF135 (Laboratoires Filorga), including consent to the publication of any identifiable images.
NTCF 135 is a pink fluid, supplied in 3mls vials, with 30Gх13мм needles and 3 mL syringes provided by the manufacturer.
All participants received 3.0 mls of intradermal injections of NCTF135 (Figure 5) in depigmented areas once a week for 5 weeks. The manufacturer advises the use of a maximum of 3 mls (1 vial) per session of mesotherapy and we followed the advice. Opened vials were discarded after being used and not kept for further procedures, as per the manufacturer’s advice.
 |
Figure 5 Biorevitalizant NCTF135. |
Application technique: intradermal injections of 0.025 mls of NTCF 135 with 30Gх13мм needle, creating micro papules with a 1 cm distance between the injection sites (Figure 6A and B). Each session lasts 15–20 mins.
 |
Figure 6 Patient L. intradermal injections in the macules on the face (A) and the neck (B). |
All procedures performed in the study were in accordance with the ethical standards of the institutional research and ethics committee of the I. M. Sechenov First Moscow Medical University, Ministry of Health of the Russian Federation and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Results
All seven patients visually recorded “mosaic” re-pigmentation in all treated areas as early as within the first 2 weeks of injections (Figure 1B, 2B and 3B) which expanded by the end of the 5 weeks course. In addition, the sharp border between the affected and the healthy skin disappeared. Patient L achieved full re-pigmentation of the macule next to the right corner of the mouth, and the affected area on the left side of the neck decreased in size, partially re-pigmented and divided into two parts by a band of healthy skin. (Figure 7A and B).
 |
Figure 7 Patient L, the macules of vitiligo on the face (A) and the neck (B) 2 weeks after the treatment with NCTF135. |
The treated areas, which did not achieve full re-pigmentation gained “café-au-lait” color. The patients noticed a change in the sensitivity to UV radiation of the treated but not fully pigmented macules of vitiligo. Short-term exposure to UV light no longer caused severe long-term erythema, as it was the case before the treatment. There were no cases of allergic response. None of the patients had side effects or exacerbation of vitiligo during or after treatment with NCTF 135. All the patients were advised to use SPF50+ sunscreens.
All the patients fully retained the pigment in the treated areas, which accounted for about 30% of the affected skin, 6 months after completion of the course of mesotherapy. Two out of seven patients received a second course of mesotherapy with NCTF135 within the following 6 months, which resulted in further re-pigmentation of 15–20% of remaining vitiligo. Five other patients could not proceed with further treatments due to financial difficulties.
Discussion
In many countries, including Russia, topical steroids are often used as a monotherapy or in combination with ultraviolet radiation. These treatment modalities achieve statistically good outcomes and result in persistent re-pigmentation of the areas affected by vitiligo. However, they have many disadvantages.
A long-term application of topical steroids often causes skin atrophy and, in some cases, tachyphylaxis. There is also a risk of a secondary infection.
Topical calcineurin inhibitors (tacrolimus and pimecrolimus) are not always well-tolerated and effective in the treatment of vitiligo.
A 2-year study of 100 patients with vitiligo, who were treated with oral folic acid (5 mg) and VitB12 (1 mg) in combination with sunlight exposure and UVB radiation, showed re-pigmentation in 52 participants with stable and progressive vitiligo. The authors hypothesized that Vit B12 has an important role in the metabolism of homocysteine, increased levels of which are responsible for the loss of pigment due to deficient methionine synthesis. The formation of methionine depends on joint metabolism of B12 and folate in human plasma.11
We described a new approach in the treatment of vitiligo by employing intradermal injections of vitamin and mineral complexes as antioxidants into affected areas. We found that this treatment has little or no side effects, provided standard contraindications for mesotherapy are addressed, and the patient has no allergic reactions to any component (esp. vitamins, hyaluronic acid) of the biorevitalizant NCTF135.
More well designed, controlled studies are needed in the future to increase the armamentarium of effective treatments of vitiligo. One of the questions to be answered is the effects of oral B12 and folic acid in combination with UVB versus intradermal injections of NCTF135 and UVB.
Our results demonstrated the efficacy of biorevitalizant NCTF135 (Laboratoires Filorga) in vitiligo as a monotherapy. The persistent effect on re-pigmentation of vitiligo after the injections of antioxidants and the increasing effect with a repeated course, support the theory of involvement of oxidative stress in the pathogenesis of vitiligo.
Further studies of the effects of NCTF135 and similar preparations in the treatment of vitiligo will be important in our understanding of this cosmetically and psychologically debilitating disease.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Krüger C, Schallreuter KU. A review of the worldwide prevalence of vitiligo in children/adolescents and adults. Int J Dermatol. 2012;51(10):1206–1212. doi:10.1111/j.1365-4632.2011.05377.x
2. Ezzedine K, Eleftheriadou V, Whitton M, van Geel N. Vitiligo. Lancet. 2015;386(9988):74–84. doi:10.1016/S0140-6736(14)60763-7
3. Alkhateeb A, Fain PR, Thody A, Bennet DC, Spritz RA. Epidemiology of vitiligo and associated autoimmune diseases in Caucasian probands and their relatives. Pigment Cell Res. 2003;16(3):208–214. doi:10.1034/j.1600-0749.2003.00032.x
4. Boldyrev AA. Oxidative stress and the brain. Soros Educ J. 2001;7(4):21–28.
5. Boldyrev AA. Introduction to Biomembranology.Textbook. Moscow State University; 1990. (in Russian).
6. Vladimirov YA. Free radical oxidation of lipids and physical properties of the lipid layer of biological membranes. Biophysics. 1987;32(5):830–844.
7. Xie H, Zhou F, Liu L, et al. Vitiligo: how do oxidative stress-induced autoantigens trigger autoimmunity? J Dermatol Sci. 2016;81(1):3–9. doi:10.1016/j.jdermsci.2015.09.003
8. Gereykhanova LG, Lomonosov KM, Bashlakova KA. Oxidative stress in the pathogenesis of vitiligo and methods for its correction. Russ J Skin Venereal Dis. 2016;19(1):45–48.
9. Seiberg M. Age-induced hair greying – the multiple effects of oxidative stress. Int J Cosm Sci. 2013;35(6):532–538. doi:10.1111/ics.12090
10. Schallreuter KU, Krüger C, Würfel BA, Panske A, Wood JM. From basic research to the bedside: efficacy of topical treatment with pseudo-catalase PC-KUS in 71 children with vitiligo. Int J Dermatol. 2008;47(7):743–753. doi:10.1111/j.1365-4632.2008.03660.x
11. Juhlin L, Olsson MJ. Improvement of vitiligo after oral treatment with vitamin B12 and folic acid and the importance of sun exposure. Acta Derm Venereol. 1997;77(6):460–462. doi:10.2340/000155555577460462
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.