Back to Journals » Clinical Ophthalmology » Volume 9
Visual recovery following open globe injury with initial no light perception
Authors Han Y, Kavoussi S, Adelman R ![]()
Received 3 May 2015
Accepted for publication 10 June 2015
Published 11 August 2015 Volume 2015:9 Pages 1443—1448
DOI https://doi.org/10.2147/OPTH.S87852
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yong S Han, Shaheen C Kavoussi, Ron A Adelman
Department of Ophthalmology and Visual Science, Yale University School of Medicine, New Haven, CT, USA
Background: The purpose of this study was to analyze eyes presenting with no light perception (NLP) after open globe injury (OGI) to determine visual outcomes and prognostic indicators for visual recovery.
Methods: The records of consecutive patients with at least 6 months of follow-up presenting with OGI and NLP to a single institution between January 1, 2003 and December 31, 2013 were reviewed for demographics, ophthalmic history, context and characteristics of injury, ocular examination findings, surgical interventions, and follow-up visual acuity. Unpaired t-tests and Fisher’s Exact tests were used for statistical analysis.
Results: Twenty-five patients met our inclusion criteria. The mean age was 50.4±25.5 (range 8–91) years. Four patients (16%) regained vision (hand motion in three patients and light perception in one patient) while 21 patients (84%) remained with NLP or had a prosthesis at final follow-up. Fourteen eyes (56%) were enucleated; nine (36%) were secondary enucleations. Although the sample sizes were small, neither ocular trauma score nor wound size was found to predict visual recovery.
Conclusion: Four patients regained some vision after presenting with NLP due to OGI. These findings suggest that, in select cases, physicians should discuss the possibility of regaining some vision.
Keywords: no light perception, open globe injury, visual recovery, vitreoretinal surgery
Introduction
Open globe injuries (OGIs), defined as full-thickness wounds of the eye wall,1 are estimated to occur at a rate of 3.5 per 100,000 persons per year worldwide.2 Similar estimates are found in the USA.3–5 Patients who initially present with no light perception (NLP) vision are at risk for poor visual outcomes,6–10 and primary enucleation of these eyes is considered to mitigate the risk of sympathetic ophthalmia and to reduce pain.10–13
Arguing against primary enucleation of OGIs with initial NLP, however, are reports demonstrating improved vision following primary closure and possible subsequent vitreoretinal surgery.6,14–20 To date, few studies have attempted to identify prognostic indicators for visual outcomes in patients with OGI presenting with NLP. These factors include age,21 mechanism and type of injury,22–24 presence of a relative afferent pupillary defect (RAPD),14,25 size and location of the wound,14,16,23 retinal detachment (RD),14,15,23 ciliary body or choroidal damage,15 vitreous hemorrhage (VH),23,24,26 and time to intervention.6,22
The recovery of visual perception in traumatized eyes with NLP can have profound functional and psychological implications for patients. Given the controversy concerning the management of eyes presenting with NLP after OGI, we present a study of 25 consecutive patients with initial NLP, four of whom regained vision following primary repair and subsequent vitreoretinal surgery. We describe the characteristics of injury, visual and anatomic outcomes, and attempt to identify predictors for visual improvement.
Methods
The study protocol was approved by the human investigations committee of the Yale University School of Medicine. A retrospective review of medical records was performed on patients with OGI and initial NLP vision who presented to Yale-New Haven Hospital between January 1, 2003 and December 31, 2013. Demographics, ophthalmic history, context and characteristics of injury, best-corrected visual acuity, and ocular examination findings at time of injury and after surgical intervention(s) were recorded for each patient. Unpaired two-tailed t-tests were utilized to determine whether ocular trauma score (OTS) and wound size were associated with visual recovery. Other possible predictor variables for prognosis included age, mechanism, and type of injury, RAPD, size and location of the wound, RD, choroidal damage, VH, and subsequent vitreoretinal surgical intervention. Outcomes included follow-up best-corrected visual acuity at 6 months, 1 year, and final follow-up.
Results
The inclusion criteria were met by 25 patients. The mean age (± standard deviation) was 50.4±25.5 (range 8–91) years, and eight patients (32%) were women. The left eye was involved in 17 of the cases (68%). Four patients (16%) were pseudophakic.
The subjects experienced ocular trauma in both the indoor (48%) and outdoor (52%) settings (Table 1). Materials of impact included shoes (n=3), bullets (n=3), windshields (n=2), bottles (n=2), and knives (n=2), among others. Approximately half of the patients suffered globe rupture, and the remainder experienced either perforation (20%) or penetration (28%). Only one patient had an intraocular foreign body, which was metallic and resulted in NLP.
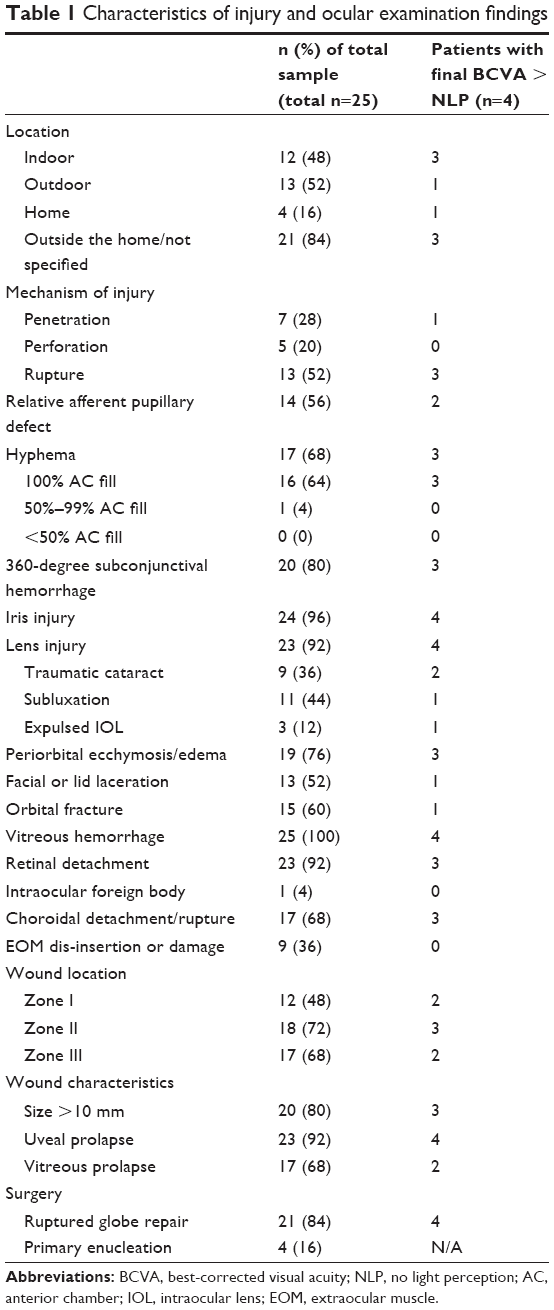 | Table 1 Characteristics of injury and ocular examination findings |
Twenty-one patients (84%) remained with NLP or had a prosthesis at final follow-up, while four patients improved to light perception or hand motion (HM, Table 2). Mean final follow-up for all patients was 25.48±18.2 (range 6–66) months. For the group that had light perception or better at final follow-up, the mean follow-up duration was 39±28.8 months, while the mean for those who remained with NLP was 22.90±15.2 months. There was no significant difference in follow-up duration between the two groups (P=0.35). The four patients with visual recovery after initial NLP are described thus:
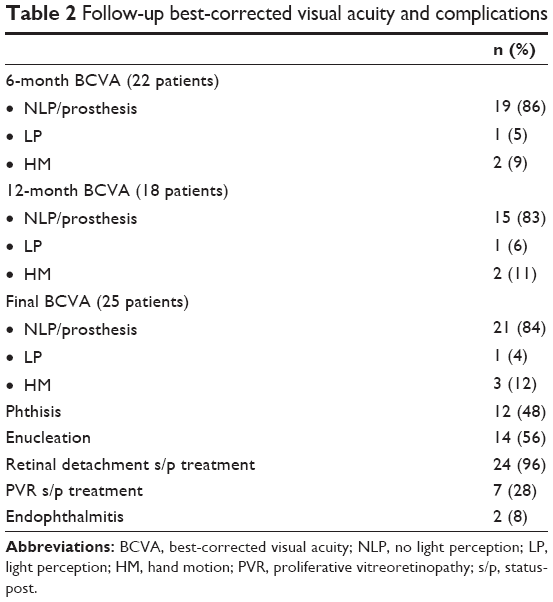 | Table 2 Follow-up best-corrected visual acuity and complications |
Patient 1
A 72-year-old Caucasian female with a history of Fuchs’ dystrophy and prior penetrating keratoplasty suffered a dehisced penetrating keratoplasty with an 8 mm wound (zone I) after blunt trauma from a plastic whiffle-ball during outdoor play with a grandchild. She presented with a traumatic cataract, VH, and choroidal detachment. The wound was associated with uveal and vitreous prolapse. OTS was 26. The patient underwent globe repair with reapproximation of the corneal graft within 24 hours. Her postoperative course was complicated by failed corneal transplant, RD, and proliferative vitreoretinopathy (PVR). She underwent two subsequent vitrectomies and a repeat corneal transplant. Visual acuity at one year is HM.
Patient 2
A 58-year-old male patient with no significant ocular history suffered a ruptured globe with a 15 mm corneoscleral wound after blunt trauma from a punch during an assault. He presented with an RAPD in the affected eye, total hyphema, 360-degree subconjunctival hemorrhage, and subluxation of the natural lens. Posterior examination revealed VH, RD, and choroidal rupture. The wound extended to zone III (>5 mm from the limbus) with uveal prolapse. OTS was 16. The patient was taken for ruptured globe repair within 24 hours of injury. His postoperative course was complicated by a funnel RD and PVR, for which he underwent pars plana vitrectomy (PPV) with membrane peel and silicone oil. Visual acuity at 2 years is HM.
Patient 3
An 8-year-old Hispanic female with no significant ocular history suffered an open globe injury with a 25 mm corneoscleral wound (zone III) from a collision with a glass door at home. She presented with total hyphema, uveal prolapse, 360-degree subconjunctival hemorrhage, traumatic cataract, periorbital swelling and ecchymosis, and adnexal injuries, including lid laceration and orbital fracture. Posterior examination revealed VH and RD. OTS was 26. She underwent ruptured globe repair within 24 hours, and her postoperative course was complicated by PVR, aphakia, corneal scar, and retinal incarceration. She underwent a combined scleral buckle and vitrectomy with pars plana lensectomy and silicone oil. Subsequently she received repeat vitrectomy with temporary keratoprosthesis, silicone oil, and penetrating keratoplasty. Her visual acuity at 5 years is light perception.
Patient 4
A 61-year-old female with no significant ocular history suffered an OGI with a 10 mm corneoscleral wound (zone II) with uveal and vitreous prolapse after blunt trauma from a fall while shopping. She presented with RAPD, total hyphema, 360-degree subconjunctival hemorrhage, expulsed natural lens, VH, and RD. OTS was 16. The patient was taken for open globe repair within 24 hours. Her postoperative course was complicated by hyphema rebleed, total RD, retinal incarceration, and PVR. She underwent anterior chamber washout with vitrectomy and silicone oil. Visual acuity at 5 years was HM.
Outcomes and characteristics
All four patients who regained vision required vitreoretinal surgery after primary closure. Patients who underwent PPV were more likely to regain vision than patients who did not undergo vitreoretinal surgery (odds ratio 123.5, 95% confidence interval 4.3–333.3, P=0.0004).
Five patients (20%) underwent primary enucleation for what were deemed unsalvageable injuries, three of whom had presented more than 24 hours from injury. All five patients who had primary enucleations had zone III injuries. Enucleation in the follow-up period was performed on an additional nine eyes for a total of 14 eyes (56%, Table 2). The most common indication for secondary enucleation was phthisis (Table 2). There were no cases of sympathetic ophthalmia. Two patients developed endophthalmitis, and all patients had received intravenous antibiotics at the time of primary intervention.
Ocular examination findings, including RAPD, hyphema, 360-degree subconjunctival hemorrhage, lens injury, and adnexal injury were not possible to establish as prognostic indicators due to the small sample sizes and heterogeneous types and causes of injury. Twenty-three of the 25 patients (92%) had a form of lens injury. Subluxation was most common (44%), followed by traumatic cataract (36%) and expulsed intraocular lens (12%). VH was present in all 25 patients, and RD occurred in 84%. Choroidal detachment or rupture was observed in 17 patients (68%).
Twenty patients (80%) had wounds greater than 10 mm in size. The mean wound size for all patients was 16.52±7.6 mm (Table 3). Mean OTS for all patients was 16.68±9.3. Neither wound size nor OTS was found to predict visual recovery (P=0.58 and P=0.20, respectively), although the sample sizes were small for this comparison.
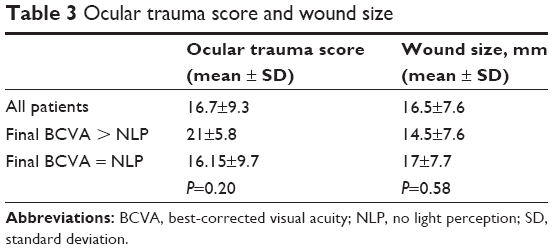 | Table 3 Ocular trauma score and wound size |
Discussion
Our study highlights four patients (16%) with OGI presenting with initial NLP who eventually improved to light perception (n=1) or HM (n=3) by final follow-up. No cases of sympathetic ophthalmia occurred in our study, with previous estimations ranging from 0.28% to 1.9% in OGIs.12,15,27,28
In the previous reports of visual recovery following OGI and initial NLP,6,14–18,20,23 the proportion of patients with visual recovery compared with those remaining with NLP has varied widely. In a retrospective review, Salehi-Had et al reported 12 of 57 eyes with visual recovery.6 Soni et al reported 17 of 73 (23%) with improvement to light perception or better, with HM being the most common visual outcome, as was the case in our study.16 One eye had improved to 20/100. Feng et al in an interventional case series involving 33 eyes found that 18 eyes (55%) recovered light perception or better, with five eyes having better than 20/200 vision.23 Two additional case series have reported rates of 67% and 33%, with four eyes (14.8%) in the latter study regaining 20/50–20/200 vision.14,15 Vitreoretinal surgery has an established role in the subsequent care of penetrating ocular trauma involving the posterior segment and is utilized within 3–14 days of initial injury to prevent PVR.29–33 In our study, a total of five patients (20%) underwent PPV, four of whom recovered to light perception or better. Vitreoretinal surgery was significantly associated with improved vision at final follow-up (P=0.0004). All four patients who had improved visual outcomes had undergone vitrectomy, while 20 of the remaining 21 patients had no subsequent vitreoretinal intervention. It is important to note, however, that only eyes that spontaneously recovered some vision underwent PPV. Thus, our findings cannot support a causal relationship between the intervention and visual outcome.
Similar results were reported in both studies by Feng et al: all patients received PPV, with visual recovery rates of 54.5% and 66.7%.15,23 Likewise, all 18 patients in a prospective interventional case series underwent vitrectomy, 16 of whom improved to at least light perception.18 Six eyes (33%) in that study achieved 20/200 or better final VA. Soni et al observed that 14 of 15 receiving PPV after primary open globe repair recovered to light perception or better.16 Similar to our study, eyes that underwent PPV compared with eyes without vitreoretinal intervention were significantly more likely to achieve visual recovery (odds ratio 256.7; 95% confidence interval 24.8–2,659.3).16 Salehi-Had et al reported that all eyes without vitreoretinal intervention remained NLP or experienced phthisis within 7 months, whereas five of the eight patients (62.5%) who had vitreoretinal surgery experienced improved vision ranging from HM to 20/70.6 However, the argument can be made that vitreoretinal surgery following primary open globe repair is reserved only for eyes clinically deemed to have visual potential, while eyes with anticipated final NLP are observed or undergo secondary enucleation. For this reason, each case must be handled with clinical judgment, with an alertness to the evidence for visual recovery following vitreoretinal intervention in appropriate candidates. To identify these candidates, we initially sought to perform Fisher’s Exact tests on initial examination findings and t-tests (unpaired and two-tailed t-tests) on wound size and OTS, but the small sample sizes and the heterogeneity of the types and causes of injuries precluded meaningful statistical comparisons. However, larger samples in the literature identify age, mechanism and type of injury, RAPD, size and location of the wound, RD, ciliary body or choroidal damage, VH, and time to intervention as having significant associations with visual outcomes.6,14–16,21–26
An additional limitation to retrospective studies of OGI with NLP is visual acuity testing, which by its nature requires subjective input and effort both from patients and examiners, and thus can be unreliable in the setting of severe significant media opacity or altered mental status.34
Nevertheless, our findings support the limited but existing evidence for visual recovery following cases of OGI with initial NLP. Several studies have also variously described the toll of enucleation, which can have profound psychological as well as physical consequences.35–37 Reports in the literature show that a significant proportion of anophthalmic patients can experience depression, anxiety, or stress compared with the normal population, and may also report lower health-related quality of life.38–40 Moreover, chronic pain due to diverse causes ranging from dryness to infection and inflammation, such as in giant papillary conjunctivitis, has been associated with prosthetic eyes.41–44 Phantom eye pain, estimated to occur in up to as many as 28% of anophthalmic patients, is a particularly challenging form of chronic pain, and permanent pain relief is often reported to occur in less than 10% of all patients.36,45,46
In conclusion, in the absence of an obviously unsalvageable case such as optic nerve avulsion, primary open globe repair with possible subsequent vitreoretinal intervention in appropriate cases is recommended to offer the best possible visual outcome for the patient, with the resultant psychological and functional benefits of even minimal visual restoration.
Disclosure
The authors report no conflicts of interest in this work.
References
Kuhn F, Morris R, Witherspoon CD. Birmingham Eye Trauma Terminology (BETT): terminology and classification of mechanical eye injuries. Ophthalmol Clin North Am. 2002;15:139–143. | ||
Negrel AD, Thylefors B. The global impact of eye injuries. Ophthalmic Epidemiol. 1998;5:143–169. | ||
Tielsch JM, Parver L, Shankar B. Time trends in the incidence of hospitalized ocular trauma. Arch Ophthalmol. 1989;107:519–523. | ||
Karlson TA, Klein BE. The incidence of acute hospital-treated eye injuries. Arch Ophthalmol. 1986;104:1473–1476. | ||
Landen D, Baker D, LaPorte R, Thoft RA. Perforating eye injury in Allegheny County, Pennsylvania. Am J Public Health. 1990;80: 1120–1122. | ||
Salehi-Had H, Andreoli CM, Andreoli MT, Kloek CE, Mukai S. Visual outcomes of vitreoretinal surgery in eyes with severe open-globe injury presenting with no-light-perception vision. Graefes Arch Clin Exp Ophthalmol. 2009;247:477–483. | ||
Schmidt GW, Broman AT, Hindman HB, Grant MP. Vision survival after open globe injury predicted by classification and regression tree analysis. Ophthalmology. 2008;115:202–209. | ||
Gilbert CM, Soong HK, Hirst LW. A two-year prospective study of penetrating ocular trauma at the Wilmer Ophthalmological Institute. Ann Ophthalmol. 1987;19:104–106. | ||
Esmaeli B, Elner SG, Schork MA, Elner VM. Visual outcome and ocular survival after penetrating trauma. A clinicopathologic study. Ophthalmology. 1995;102:393–400. | ||
Moshfeghi DM, Moshfeghi AA, Finger PT. Enucleation. Surv Ophthalmol. 2000;44:277–301. | ||
Morris R, Kuhn F, Witherspoon CD. Management of the opaque media eye with no light perception. In: Alfaro DV, III, Liggett PE. Vitreoretinal Surgery of the Injured Eye. Philadelphia, PA, USA: Lippincott-Raven; 1999:113–124. | ||
du Toit N, Motala MI, Richards J, Murray AD, Maitra S. The risk of sympathetic ophthalmia following evisceration for penetrating eye injuries at Groote Schuur Hospital. Br J Ophthalmol. 2008;92:61–63. | ||
Matthews GP, Das A, Brown S. Visual outcome and ocular survival in patients with retinal detachments secondary to open- or closed-globe injuries. Ophthalmic Surg Lasers. 1998;29:48–54. | ||
Agrawal R, Wei HS, Teoh S. Predictive factors for final outcome of severely traumatized eyes with no light perception. BMC Ophthalmol. 2012;12:16. | ||
Feng K, Shen L, Pang X, et al. Case-control study of risk factors for no light perception after open-globe injury: eye injury vitrectomy study. Retina. 2011;31:1988–1996. | ||
Soni NG, Bauza AM, Son JH, Langer PD, Zarbin MA, Bhagat N. Open globe ocular trauma: functional outcome of eyes with no light perception at initial presentation. Retina. 2013;33:380–386. | ||
Yang S, Jiang T. Vitrectomy combined with silicone oil tamponade in the treatment of severely traumatized eyes with the visual acuity of no light perception. Int J Ophthalmol. 2013;6:198–203. | ||
Heidari E, Taheri N. Surgical treatment of severely traumatized eyes with no light perception. Retina. 2010;30:294–299. | ||
Savar A, Andreoli MT, Kloek CE, Andreoli CM. Enucleation for open globe injury. Am J Ophthalmol. 2009;147:595–600. | ||
Sheng I, Bauza A, Langer P, Zarbin M, Bhagat N. A 10-year review of open-globe trauma in elderly patients at an urban hospital. Retina. 2015;35:105–110. | ||
Chiquet C, Zech JC, Gain P, Adeleine P, Trepsat C. Visual outcome and prognostic factors after magnetic extraction of posterior segment foreign bodies in 40 cases. Br J Ophthalmol. 1998;82:801–806. | ||
Lee SH, Ahn JK. Emergent risk factors associated with eyeball loss and ambulatory vision loss after globe injuries. J Trauma. 2010;69:195–198. | ||
Feng K, Yun TH, Ma Z. Prognostic indicators for no light perception after open-globe injury: Eye Injury Vitrectomy Study. Am J Ophthalmol. 2011;152:654–662. | ||
Pieramici DJ, MacCumber MW, Humayun MU, Marsh MJ, de Juan E, Jr. Open-globe injury: update on types of injuries and visual results. Ophthalmology. 1996;103:1798–1803. | ||
Rahman I, Maino A, Devadason D, Leatherbarrow B. Open globe injuries: factors predictive of poor outcome. Eye. 2006;20:1336–1341. | ||
Groessl S, Nanda SK, Mieler WF. Assault-related penetrating ocular injury. Am J Ophthalmol. 1993;116:26–33. | ||
Albert DM, Diaz-Rohena R. A historical review of sympathetic ophthalmia and its epidemiology. Surv Ophthalmol. 1989;34:1–14. | ||
Gürdal C, Erdener U, Irkeç M, Orhan M. Incidence of sympathetic ophthalmia after penetrating eye injury and choice of treatment. Ocul Immunol Inflamm. 2002;10:223–227. | ||
Sobaci G, Mutlu FM, Bayer A, Karagül S, Yildirim E. Deadly weapon-related open-globe injuries: outcome assessment by the ocular trauma classification system. Am J Ophthalmol. 2000;129:47–53. | ||
Hui Y, Wang L, Shan W. [Exploratory vitrectomy for traumatized eyes with no light perception and dense vitreous hemorrhage]. Zhonghua Yan Ke Za Zhi. 1996;32:450–452. Chinese. | ||
Coleman DJ. Early vitrectomy in the management of the severely traumatized eye. Am J Ophthalmol. 1982;93:543–551. | ||
Mieler WF, Mittra RA. The role and timing of pars plana vitrectomy in penetrating ocular trauma. Arch Ophthalmol. 1997;115: 1191–1192. | ||
de Bustros S, Michels RG, Glaser BM. Evolving concepts in the management of posterior segment penetrating ocular injuries. Retina. 1990;10:S72–S75. | ||
Abrams GW, Kington RW. Falsely extinguished bright light flash electroretinogram. Its association with dense vitreous hemorrhage. Arch Ophthalmol. 1984;100:1427–1429. | ||
Aggarwal H, Singh SV, Kumar P, Kumar Singh A. Prosthetic rehabilitation following socket reconstruction with Blair-Brown graft and conformer therapy for management of severe post-enucleation socket syndrome – a clinical report. J Prosthodont. Epub ahead of print, September 17, 2014. | ||
Bohman E, Roed Rassmusen ML, Kopp ED. Pain and discomfort in the anophthalmic socket. Curr Opin Ophthalmol. 2014;5:455–460. | ||
Hegarty D, Coakley D, Dooley I. Psychological reactions and persistent facial pain following enucleation. Pain Res Treat. 2014;2014:232989. | ||
Ahn JM, Lee SY, Yoon JS. Health-related quality of life and emotional status of anophthalmic patients in Korea. Am J Ophthalmol. 2010;149:1005–1011. | ||
Masdottir S, Sahlin S. Patient satisfaction and results after evisceration with a split-sclera technique. Orbit. 2007;26:241–247. | ||
Rasmussen ML, Ekholm O, Prause JU, Toft PB. Quality of life of eye amputated patients. Acta Ophthalmol. 2012;90:435–440. | ||
Jang SY, Lee SY, Yoon JS. Meibomian gland dysfunction in longstanding prosthetic eye wearers. Br J Ophthalmol. 2013;97:398–402. | ||
Vardizer Y, Lang Y, Mourits MP, Briscoe MD. Favorable effects of lacrimal plugs in patients with an anophthalmic socket. Orbit. 2007;26:263–266. | ||
Bozkurt B, Akyurek N, Irkec M, Erdener U, Memis L. Immunohistochemical findings in prosthesis-associated giant papillary conjunctivitis. Clin Experiment Ophthalmol. 2007;35:535–540. | ||
Samimi DB, Bielory BP, Miller D, Johnson TE. Microbiologic trends and biofilm growth on explanted periorbital biomaterials: a 30-year review. Ophthalm Plast Reconstr Surg. 2013;29:376–381. | ||
Soros P, Vo O, Husstedt IW, Evers S, Gerding H. Phantom eye syndrome: its prevalence, phenomenology, and putative mechanisms. Neurology. 2003;60:1542–1543. | ||
Roed Rasmussen ML, Prause JU, Johnson M, Toft PB. Phantom eye syndrome: types of visual hallucinations and related phenomena. Ophthal Plast Reconstr Surg. 2009;25:390–393. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.