Back to Journals » Therapeutics and Clinical Risk Management » Volume 11
Update on the management of chemotherapy-induced nausea and vomiting – focus on palonosetron
Authors Zhou M, Popovic M, Pasetka M, Pulenzas N, Ahrari S, Chow E, DeAngelis C
Received 31 December 2014
Accepted for publication 5 March 2015
Published 5 May 2015 Volume 2015:11 Pages 713—729
DOI https://doi.org/10.2147/TCRM.S68130
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Michelle Zhou, Marko Popovic, Mark Pasetka, Natalie Pulenzas, Soha Ahrari, Edward Chow, Carlo DeAngelis
Department of Pharmacy, Odette Cancer Center, Sunnybrook Health Sciences Center, University of Toronto, Toronto, ON, Canada
Purpose: Nausea and vomiting are major adverse effects of chemotherapy and can greatly impact patients’ quality of life. Although chemotherapy-induced nausea and vomiting (CINV) prevalence is high, treatment remains difficult. Palonosetron is a 5-hydroxytryptamine receptor antagonist (5-HT3RA) approved for treatment of CINV. The purpose of this review is to discuss existing and emerging therapeutic options, and examine studies focusing on palonosetron with regards to efficacy, pharmacology, tolerability, safety, and patient-derived outcomes.
Methods: A literature search was conducted using Ovid MEDLINE and EMBASE to identify relevant studies using palonosetron alone or in combination with other antiemetics. Studies were extracted if they included complete response (CR), complete control (CC), no nausea, no vomiting, and no rescue medications as an endpoint. Studies were also included if safety endpoints were examined.
Results: Palonosetron alone has been shown to improve CR and CC rates for patients receiving low, moderate, or high emetogenic chemotherapy. Rates were further improved with the addition of dexamethasone, a corticosteroid. Furthermore, the addition of neurokinin-1 receptor antagonists, such as netupitant markedly improved efficacy profiles compared to palonosetron alone. Aprepitant is an antiemetic that has exhibited positive results in combination with palonosetron. Recently, a new drug consisting of netupitant and palonosetron (NEPA) has demonstrated significantly more efficacious prevention of CINV. Regardless of the combination, palonosetron has been well tolerated. The most common adverse events were constipation, headache, fatigue, and dizziness, with the majority of patients describing them as only mild or moderate.
Conclusion: Palonosetron, alone or with other antiemetics, has improved CINV treatment due to its ability to significantly reduce delayed phases of CINV, compared to similar 5-HT3RAs. Palonosetron is both more effective than first generation 5-HT3RAs and safer, as it results in a smaller prolongation of the QTc interval, compared to other 5-HT3RAs.
Keywords: chemotherapy-induced nausea and vomiting, palonosetron, efficacy, safety, pharmacology, patient-reported outcomes
Introduction
Chemotherapy-induced nausea and vomiting (CINV) is considered a major adverse effect of cytotoxic chemotherapy and can greatly impact patients’ quality of life.1–3 As a result, CINV is one of the major reasons for disruption or delay in treatment, which is often due to patient noncompliance.3 The administration of a safe and efficacious prophylactic antiemetic regimen is thus important for current and future patients at risk for CINV.4 In antiemetic clinical trials, there are five common endpoints that are employed for comparison: complete response (CR), defined as no emesis and no use of rescue medication; complete control (CC), defined as CR with the addition of no mild nausea; no emetic episodes; no episodes of nausea; and no use of rescue medication.4
Trials that used first generation 5-hydroxytryptamine receptor antagonists (5-HT3RAs), including ondansetron, granisetron, tropisetron, and dolasetron, concluded that, although they were successful in controlling the rates of vomiting, nausea still remained a concern, especially in the delayed phase.4 The addition of dexamethasone to 5-HT3RAs is highly effective for acute emetic control; however, the effect on delayed emesis is less evident.5 Despite the introduction of more effective antiemetic agents, nausea and vomiting remain a significant complication of chemotherapy.1
Mechanism of CINV
CINV is composed of an acute phase and delayed phase. The acute phase is defined as nausea and vomiting occurring 0–24 hours after administration of chemotherapy, whereas the delayed phase occurs between 24 hours and up to 5 days later.6
Different but overlapping pathological pathways are involved in the pathogenesis of CINV.3 The emetic center is believed to be a loosely organized network of neurons in the medulla oblongata.3 Chemotherapy agents are thought to activate the release of neurotransmitters, in particular, serotonin, which activates vagal afferents leading to stimulation of the area postrema. Sensory inputs in vagal afferents and the area postrema are then consolidated at the emetic center, resulting in efferent signals that lead to contraction of abdominal muscles, the diaphragm, stomach, and esophagus, producing a reflexive emetic response.3 Several neurotransmitters are thought to be involved in this process and include dopamine, serotonin (5-HT), and substance P (SP). As a result, drugs that antagonize the action of these neurotransmitters have been developed as prophylactic therapies for CINV.3
Emerging and existing treatments
Early treatments of CINV involved the use of dopamine D2 receptor antagonists, the most common of which is metoclopramide.1 Some believe that the antiemetic effects of metoclopramide are due to its weak inhibition of 5-HT3 receptors (which is achieved when it is administered at high doses).1
Chemotherapy can also induce the release of SP, which acts on neurokinin-1 (NK-1) receptors located both peripherally and centrally.6,7 NK-1 receptor antagonists (NK-1 RAs) have been developed to prevent both acute and delayed CINV.7 The broad spectrum of antiemetic activity allows these medications to control many forms of induced emesis.8 Aprepitant was the first approved NK-1 RA whereas others, like netupitant, are still undergoing clinical trials.5 Previous guidelines for CINV management have recommended NK-1 RAs for prophylaxis of delayed phases of CINV due to highly (HEC) or moderately emetogenic chemotherapy (MEC).7
Enterochromaffin cells located in the small intestine release serotonin which binds to 5-HT3 receptors on vagal afferents.4 Throughout the 1990s, several 5-HT3RAs including ondansetron, granisetron, tropisetron, and dolasetron were introduced as antiemetic agents.1,4 These agents bind to the same binding site as serotonin on the 5-HT3 receptor, and, as a result, the CINV effects normally produced by the vagal afferents are inhibited.1
Typically, 5-HT3RAs alone are used for the treatment of acute-phase emesis, whereas both acute and delayed phases are treated with NK-1 RAs in conjunction with 5-HT3RAs and dexamethasone. A number of international groups have suggested that prior to chemotherapy, a combination of 5-HT3RA and dexamethasone be used for acute CINV prophylaxis.1 However, postchemotherapy, dexamethasone should be used alone for delayed CINV prophylaxis.1
A new 5-HT3RA known as palonosetron (Aloxi®, Helsinn Healthcare SA, Pazzallo, Switzerland) was developed to improve response rates, and was approved by the US Food and Drug Administration for delayed emesis treatment.9 Palonosetron is a second-generation 5-HT3RA that has a uniquely strong binding affinity for the serotonin receptor.10 Studies have shown that palonosetron can reduce the incidence of delayed CINV through inhibition of SP, which is not evident in certain first generation 5-HT3RAs.11 The purpose of this review is to examine published data on palonosetron with regard to efficacy, pharmacology, tolerability, safety, and patient-derived outcomes.
Methods
A literature search was conducted using Ovid MEDLINE (1946 to August 2014 [Week 32]) and EMBASE (1947 to August 2014 [Week 32]). The following terms were combined in the search: “palonosetron” and “chemotherapy-induced nausea and vomiting”. Studies were screened for at least one of the following common endpoints: CR, CC, no nausea, no emesis, or no rescue medication. Studies were further stratified by inclusion of either acute or delayed phases. Another literature search was conducted using Ovid MEDLINE (2008 to August 2014 [Week 32]) and EMBASE (2008 to August 2014 [Week 32]) using the following search terms: “chemotherapy-induced nausea and vomiting” and “antineoplastic agents” for articles that were relevant to the mechanism of CINV or antiemetic agents.
Results
A total of 818 articles from the literature search were examined for potential inclusion. The literature search as well as additional references from relevant review articles yielded 32 full articles. Of these, six articles discussed the pharmacology of palonosetron (Tables 1 and 2). Articles that included safety and efficacy were as follows: ten discussed palonosetron alone (Tables 3 and 4); ten discussed safety and efficacy of palonosetron in combination with dexamethasone; six discussed safety and efficacy of palonosetron in combination with aprepitant and dexamethasone; and two discussed safety and efficacy of NEPA (Tables 5and 6).
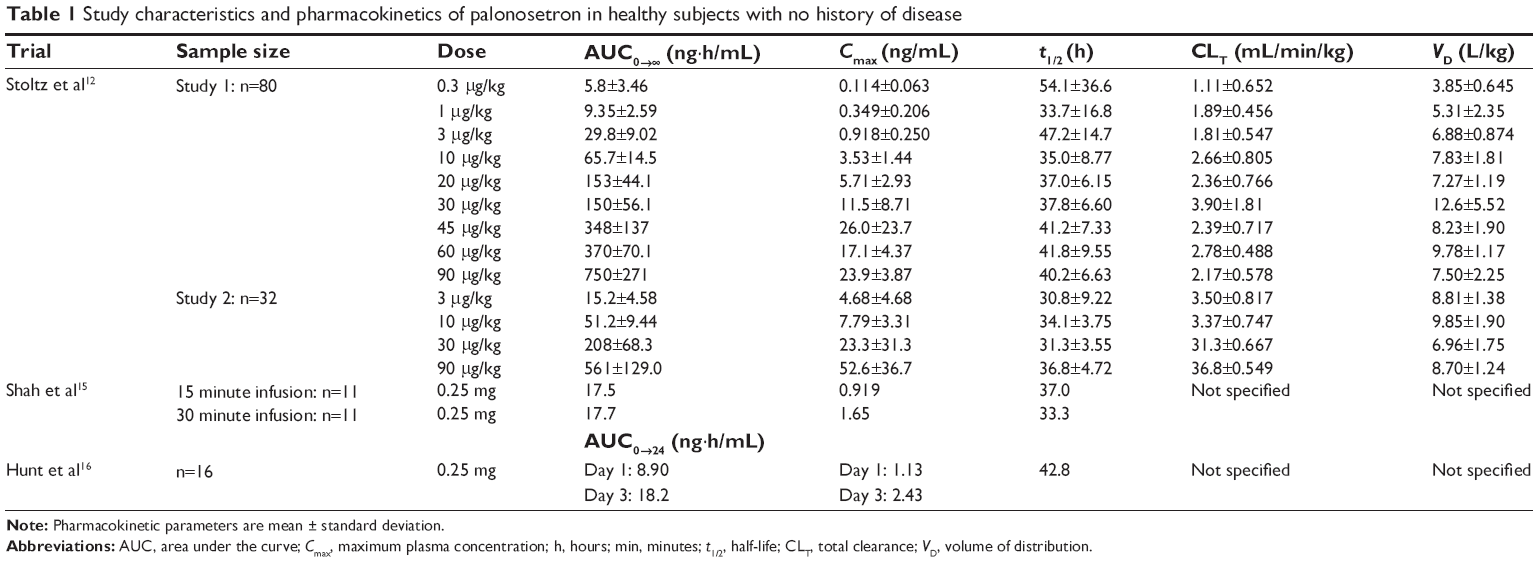 | Table 1 Study characteristics and pharmacokinetics of palonosetron in healthy subjects with no history of disease |
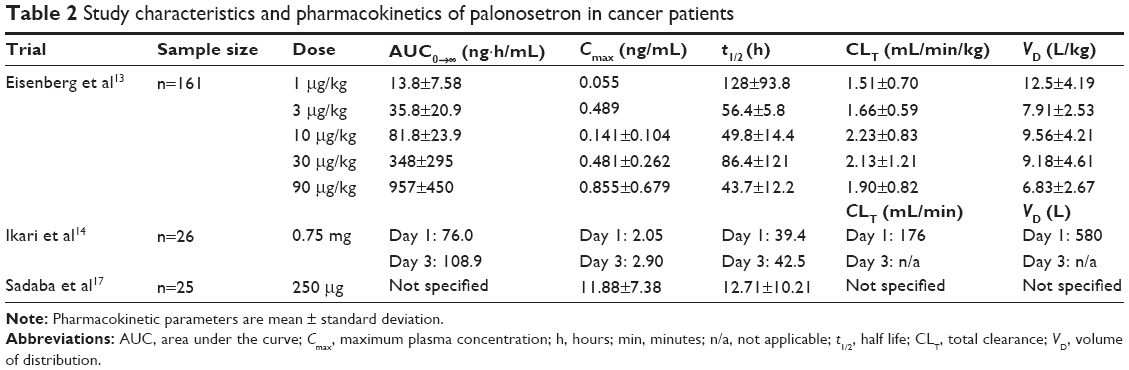 | Table 2 Study characteristics and pharmacokinetics of palonosetron in cancer patients |
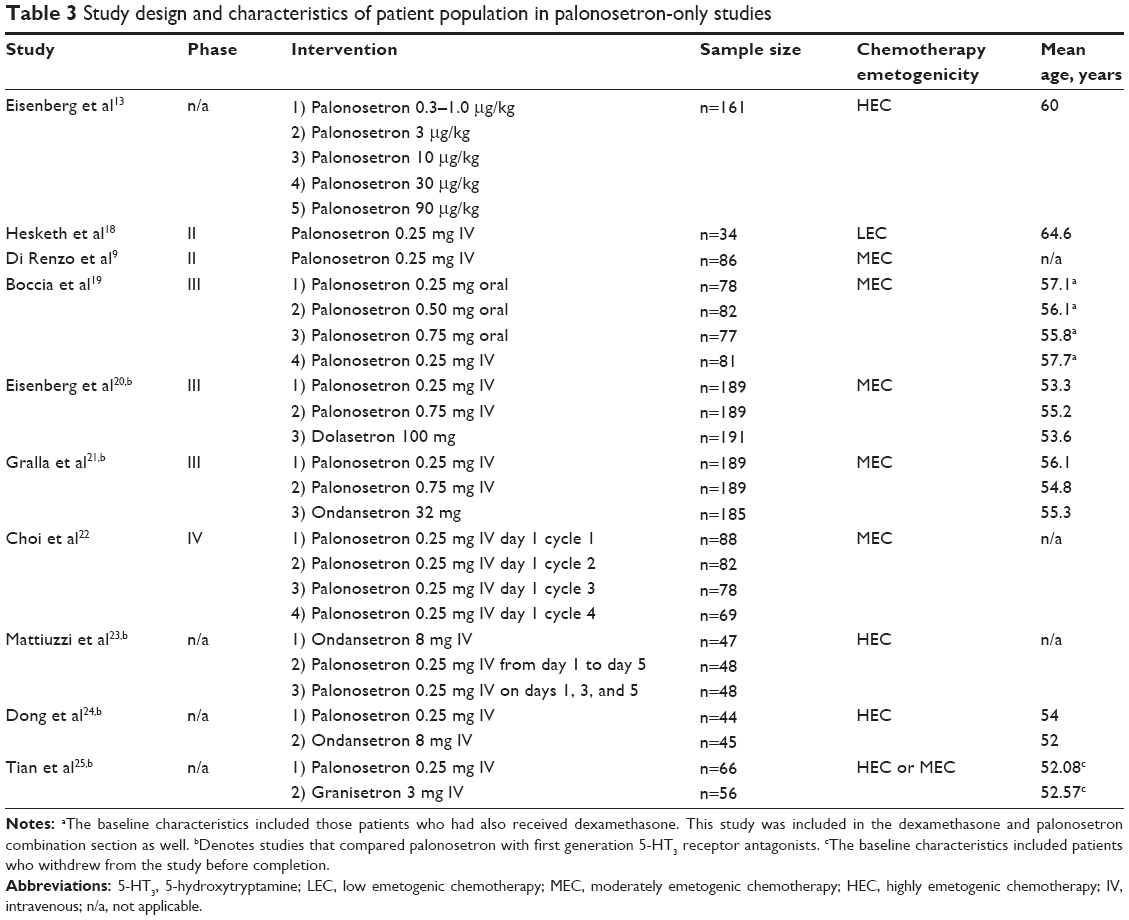 | Table 3 Study design and characteristics of patient population in palonosetron-only studies |
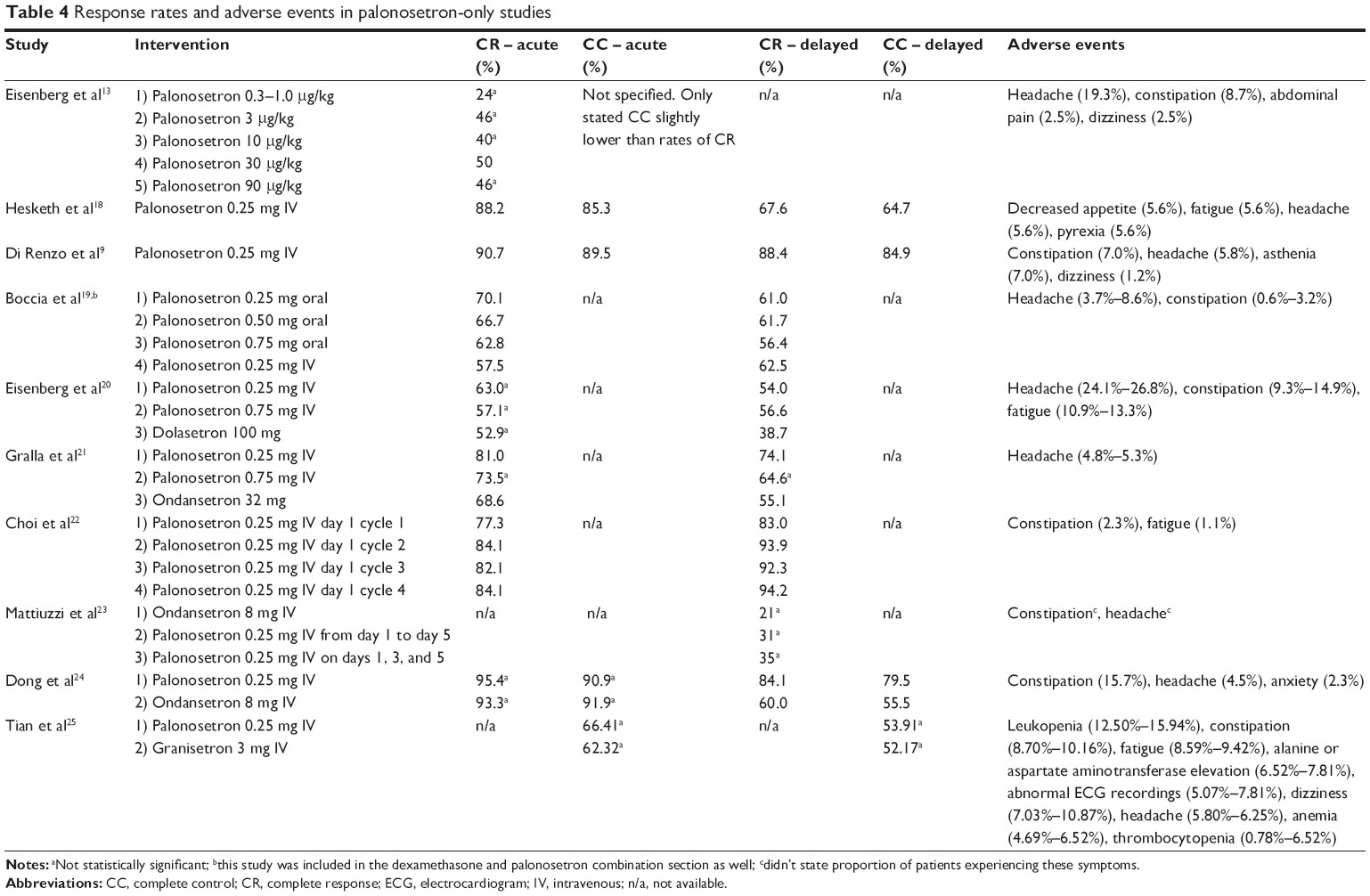 | Table 4 Response rates and adverse events in palonosetron-only studies |
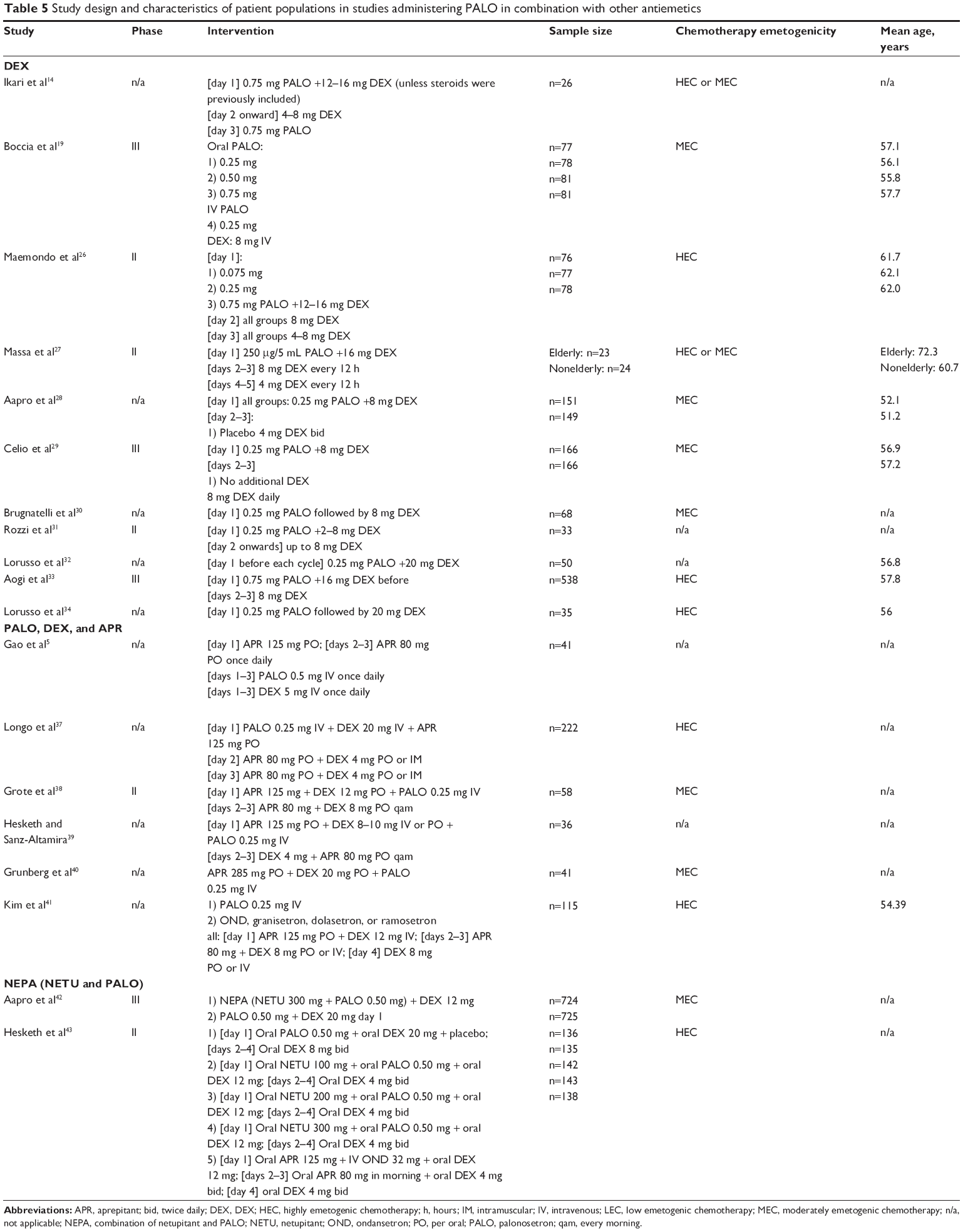 | Table 5 Study design and characteristics of patient populations in studies administering PALO in combination with other antiemetics |
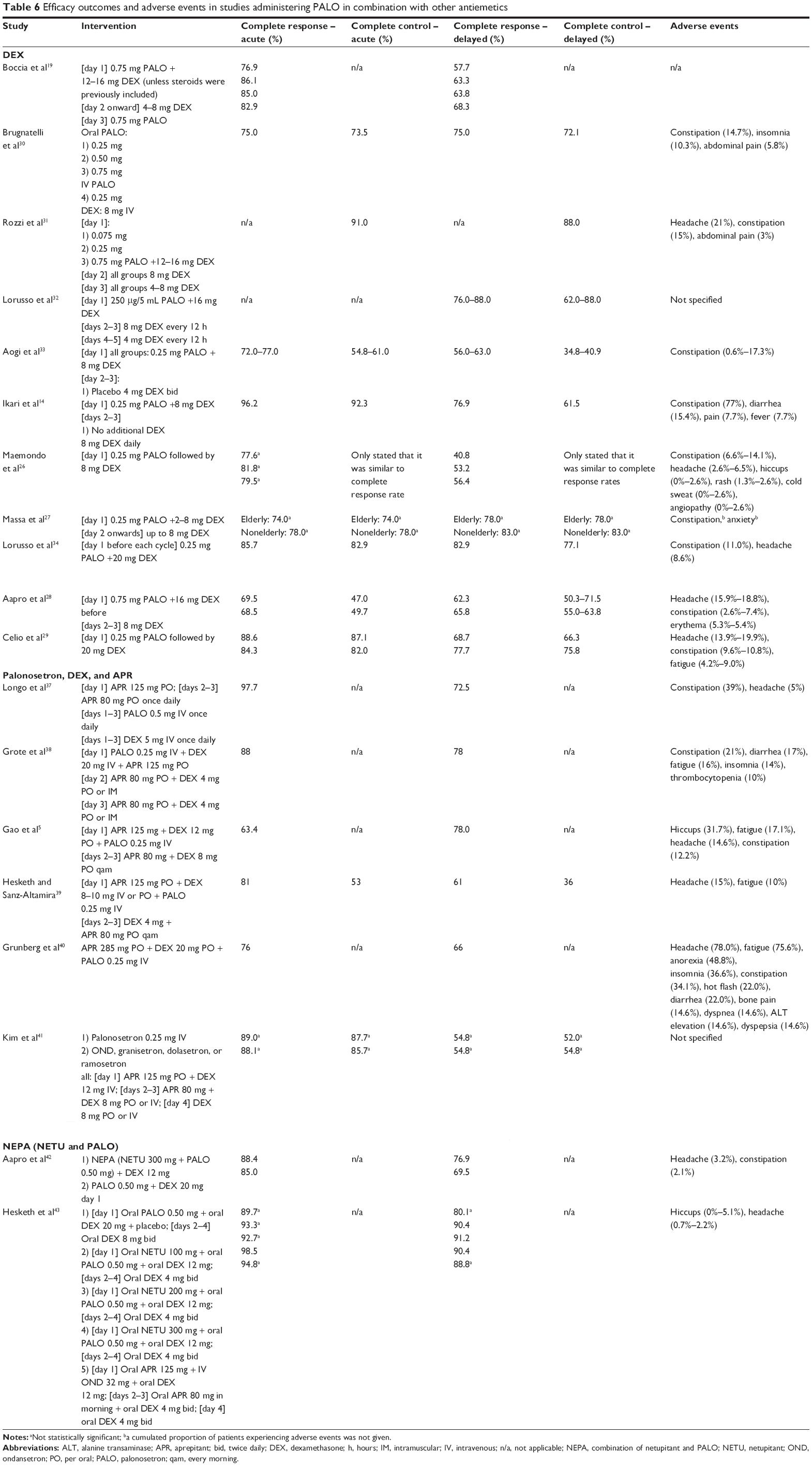 | Table 6 Efficacy outcomes and adverse events in studies administering PALO in combination with other antiemetics |
Pharmacology
The summary of palonosetron pharmacokinetics can be found in Tables 1 and 2. Mean maximum plasma concentrations (Cmax) and area under the concentration-time curve (AUC0–∞) generally increased in a dose-dependent manner.12,13 In 32 healthy American subjects, doses ranged from 0.3 to 90 μg/kg giving rise to increases in both AUC0–∞ and Cmax: 5.8–750 ng·h/mL and 0.114–23.9 ng/mL, respectively.12 Similarly, Eisenberg et al13 reported the same trend in 35 cancer patients, with AUC0–∞ and Cmax ranging from 13.8 to 957 ng·h/mL and 0.89 to 336 ng/mL, respectively, when given doses of 1–90 μg/kg palonosetron.
Three studies involving healthy patients and one involving cancer patients found that total clearance (CLT) for palonosetron was low.12–14 Additionally; volume of distribution (VD) levels for both populations in all studies was found to be elevated, indicating high partitioning into tissue. At comparable doses of intravenous (IV) palonosetron, cancer patients exhibited lower mean CLT and larger mean VD values than their healthy counterparts. At a dose of 1 μg/kg, cancer patients recorded mean CLT and VD levels of 1.51 mL/min/kg and 12.5 L/kg, respectively, whereas healthy patients recorded mean values of CLT =1.89 mL/min/kg and VD =5.31 L/kg.12,13
In both cancer and healthy populations, low CLT and high VD resulted in a longer half-life (t1/2).12–16 The most extreme deviations in half-life from that noted by the manufacturer (ie, t1/2 of approximately 40 hours) were exhibited by cancer patients; the greatest of which was reported to be t1/2 =128 hours, in a study with 161 cancer patients, while the shortest was t1/2 =12.71 hours.15,17
Efficacy
Dose-ranging study
In 2003, Eisenberg et al13 conducted a dose-ranging study in patients receiving HEC to determine the efficacy and safety of palonosetron. A total of 161 patients were enrolled, with doses ranging from 0.3 to 90 μg/kg. Overall, those that received lower doses of palonosetron exhibited a lesser response to therapy than those that received higher doses. Within the first 24 hours, most patients receiving elevated doses (ie, 3, 30, and 90 μg/kg) experienced less nausea, and did not require rescue medication. CRs were exhibited in approximately 50% of the patients for each higher dose test group, whereas only 26% of patients in the low dose test group achieved CR. The authors also noted that the lower dose group exhibited decreased CC compared to the higher dose groups. They concluded that differences between the test groups reached significance at the 30 μg/kg point.15
Phase II studies of palonosetron-only therapy
A number of Phase II studies have examined the use of palonosetron alone for CINV prevention (Tables 3 and 4). Within each study, the use of other antiemetics was prohibited. In an open label, single arm investigation of palonosetron with 34 patients receiving low emetogenic chemotherapy (LEC), 88.2% and 67.6% of patients experienced CR during the acute and delayed phases, respectively. CC was similar at 85.3% and 64.7% for acute and delayed phases. This group suggested that palonosetron was effective in preventing CINV for patients receiving LEC.18
Another study evaluated the efficacy of palonosetron in 74 patients with aggressive non-Hodgkin’s lymphoma who were receiving MEC. Patients received a single dose of 0.25 mg of palonosetron IV. During the acute phase, 90.7% of patients reported a CR while 88.4% of patients reported a CR during the delayed phase. CC was observed in 89.5% of patients during the acute phase and 84.9% during the delayed phase. This study demonstrated the effectiveness and potential role of palonosetron in patients with non-Hodgkin’s lymphoma receiving MEC.9
Phase III studies of palonosetron-only therapy
Several Phase III clinical trials have examined the safety and efficacy of palonosetron in preventing CINV (Tables 3 and 4). One study compared different doses of oral palonosetron with IV palonosetron in 635 patients receiving MEC (Table 3).19 The proportion of CRs observed in the acute phase was higher for all doses administered orally (62.8%–70.1% orally versus 57.5% IV), with the highest resulting from the 0.25 mg dose (70.1%). In the delayed phase however, a greater proportion of CR was observed in patients who received IV palonosetron. Overall, it was found that the oral doses were similar in efficacy when compared to the IV formulation. However, this group also went on to recommend oral palonosetron 0.50 mg as a therapeutic option, citing its numeric superiority in efficacy.19
In another study, the efficacy and safety of palonosetron was evaluated and compared to dolasetron in 569 subjects. The subjects were randomized to receive either IV palonosetron or dolasetron. The primary hypothesis was that at least one dose of palonosetron was noninferior to dolasetron. This hypothesis was supported during the acute phase as the CR rates were 63.0%, 57.1%, and 52.9% of patients for 0.25 mg palonosetron, 0.75 mg palonosetron, and 100 mg dolasetron, respectively. Furthermore, CR rates observed during the delayed phase were significantly higher for both doses of palonosetron compared to dolasetron. This group concluded that a single dose of palonosetron is more effective than a single dose of dolasetron in both acute and delayed CINV prophylaxis in patients receiving MEC.20
Gralla et al21 on the other hand, compared palonosetron with ondansetron. A total of 563 subjects were randomized to receive intravenously, either palonosetron or ondansetron. The CR rates observed in patients who received 0.25 mg of palonosetron were significantly different than those who received ondansetron during the acute (81.0% vs 68.6%) and delayed phases (74.1% vs 55.1%). However, 0.75 mg of palonosetron did not yield any significantly different CR rates in both acute and delayed phases. CC rates for 0.25 mg and 0.75 mg were both significantly higher than ondansetron during the delayed phase. The study group suggested that 0.25 mg of palonosetron was more effective than 32 mg ondansetron in preventing acute and delayed CINV.
Phase IV studies of palonosetron-only therapy
The efficacy of palonosetron in patients with non-Hodgkins’ lymphoma undergoing MEC was assessed in a Phase IV open-labeled, uncontrolled study. Patients received 0.25 mg of palonosetron on day 1 of cycle 1, and at each subsequent cycle. For all cycles, the initial CR rate observed during the acute phase increased as patients entered into the delayed phase. Within the delayed phase, the CR increased from 83.0% to 93.9% from cycle 1 to 2 and remained approximately the same in subsequent cycles. Overall, palonosetron showed control of CINV in both the acute and delayed phases in this patient group.22
Other studies
Mattiuzzi et al23 conducted a comparative randomized controlled trial in 143 patients with acute myelogenous leukemia receiving HEC. Subjects were allotted to receive either ondansetron 8 mg, 0.25 mg IV palonosetron from day 1 to day 5, or palonosetron 0.25 mg IV on days 1, 3, and 5. The CR during the delayed phase were reported to be 21% and 31% for the ondansetron and palonosetron study groups on days 1 to 5, respectively. Palonosetron study groups on days 1, 3, and 5 reported CR rates of 35% in the delayed phase. However, the CR rates were not significantly different across all study arms.
Dong et al24 compared palonosetron to ondansetron in 89 subjects with non-small-cell lung carcinoma (NSCLC) receiving HEC. This group found that the proportion of CR and CC observed during the acute phase were not significantly different between palonosetron and ondansetron groups. Interestingly, the proportions observed during the delayed phases were significantly higher in the palonosetron group with a CR rate of 84.1% and CC rate of 79.5%, compared to 60.0% and 55.5%, respectively in the ondansetron group. This study suggested that palonosetron is more effective in preventing delayed nausea and vomiting than is ondansetron in patients with NSCLC.
Another study compared palonosetron with granisetron in 122 patients.25 The subjects in this study received either HEC or MEC and were randomized to receive either palonosetron intravenously in the first cycle and granisetron intravenously in the second cycle or vice versa. The CR rates of palonosetron for acute and delayed phases were not statistically different than that of granisetron, but were higher than granisetron nonetheless. The CR for palonosetron was 71.09% in the acute phase as opposed to 60.16% in the delayed phase. Overall, palonosetron was effective and noninferior to granisetron in preventing CINV in both acute and delayed phases.
Safety and tolerability of palonosetron-only therapy
The most common adverse events reported by patients among the included studies can be found in Table 4. Palonosetron has been shown to be safe and tolerable as an antiemetic drug. The majority of patients who experienced adverse events reported them as mild or moderate, whereas severe symptoms were determined to be unrelated to the study medication. The most common symptoms across palonosetron-only therapy included studies were: constipation, headache, fatigue, and dizziness.9,15,18–25
Combination studies – dexamethasone
Dexamethasone is a corticosteroid that when administered with 5-HT3RAs increases the antiemetic effect. One explanation of dexamethasone’s mechanism of action is that it increases the low cortisol level that is associated with nausea and vomiting.
Boccia et al19 randomized patients to receive either oral or IV formulations of palonosetron, with or without dexamethasone. This group found that additional dexamethasone was associated with higher CR rates during the acute phase. In oral formulations, the 0.75 mg strength presented with the greatest difference in CR rates: 85.0% with concomitant dexamethasone, compared to 62.8% without. The difference was also substantial in the IV formulation (0.25 mg): 82.9% with concomitant dexamethasone; 57.5% without. There was also a greater CR rate in patients that were administered dexamethasone during the delayed phase, but the difference was much less pronounced. Interestingly, the oral 0.25 mg strength revealed CR rates that were lower with concomitant dexamethasone. This led the group to recommend 0.50 mg of palonosetron as the starting therapeutic option, should dexamethasone also be included in the drug regimen.
In a study by Maemondo et al26 231 subjects were randomized to receive either 0.075, 0.25, or 0.75 mg of palonosetron along with a dose of dexamethasone (12–16 mg) on day 1, followed by dexamethasone doses over the subsequent 2 days. Groups were similar in baseline characteristics, and all individuals were receiving HEC. Across all groups, more than 75% of patients reported CR in the acute phase. Within the delayed phase, only the 0.25 mg and 0.75 mg groups noted that greater than 50% of patients had a CR. CC rates were similar to the CR rates in their respective phases.
A number of trials have demonstrated the utility of combining palonosetron and dexamethasone in specific patient cohorts, including breast and colorectal cancers, as well as glioblastoma; however, the results of these trials were not compared to single agent palonosetron (Tables 5 and 6).16,19,26–34
Massa et al27 examined palonosetron and dexamethasone in elderly and nonelderly individuals receiving either MEC or HEC. Across all groups, more than 75% of patients reported a CR in both the acute and delayed phases. Nonelderly patients reported higher percentages of CR in both phases. Additionally, this study found an increase in the percentage of CR from the acute to the delayed phases for both groups: a 4% increase in elderly individuals, and 5% in nonelderly individuals.
The efficacy of the dexamethasone–palonosetron combination, administered exclusively on day 1 as opposed to subsequent doses of dexamethasone, has also been examined.28,29 Both Aapro et al28 and Celio et al29 conducted their studies using 0.25 mg palonosetron with up to 8 mg of dexamethasone in patients receiving MEC. Patients received either 8 mg of dexamethasone or no dexamethasone, on days 2 and 3. In the acute phase, both studies reported a higher percentage of CR in patients, although the difference was not statistically significant. Both groups also found increased CR rates in the delayed phase. In terms of CC, Celio et al29 uncovered a similar trend (ie, greater percentage of those achieving CC in those without subsequent doses of dexamethasone in the acute phase, followed by a greater percentage in those who received additional doses in the delayed phase), whereas the opposite trend was discovered in the study by Aapro et al.28
Safety
Palonosetron, like other members of the 5-HT3RAs, has the potential to affect electrocardiographic parameters, in particular prolongation of the QT interval, which has been associated with life threatening arrhythmias and death.4,35,36 One meta-analysis suggested that palonosetron was safer than first generation 5-HT3RAs with respect to the change in QT interval.4 Additionally, Yavas et al35 and Dogan et al36 have also conducted prospective studies to determine the effect of antiemetic prophylaxis on QT interval. In both studies, patients were administered 8 mg of dexamethasone and 0.25 mg of palonosetron intravenously. Although changes in QT interval were found by both studies, neither groups found their results to be statistically significant. In both cases then, it was thus concluded that palonosetron has no acute arrhythmogenic potential.35,36
The most common side effects among these studies were headache and constipation, both of which were reported as mild to moderate in intensity. Treatments were well tolerated overall, as severe side effects experienced by test subjects were deemed unrelated to the dexamethasone and palonosetron regimen.29,31,34
Combination studies – palonosetron, dexamethasone, and aprepitant
Studies have also been conducted to determine the efficacy of the combination of palonosetron, dexamethasone, and aprepitant in patients receiving HEC (Tables 5 and 6).5,37–41 Three studies examined the combination in patients receiving cisplatin-based chemotherapy, each lasting 3 days.5,37,38 Each study utilized a single oral dose of aprepitant 125 mg on day 1, followed by single oral doses of aprepitant 80 mg on days 2 and 3. Longo et al37 and Grote et al38 both administered palonosetron as a single IV dose of 0.25 mg before chemotherapy to 222 patients and 58 patients, respectively. Palonosetron was not given to patients during the remaining 2 days in either study. Gao et al5 on the other hand, administered palonosetron over the entire 3-day period as IV doses of 0.5 mg once daily to 41 patients. Dexamethasone was also administered differently between each study. Gao et al5 revealed the lowest percentage of patients with CRs in both the acute and delayed stages (63.4% and 78.0% respectively), but noted that the efficacy of the study is maintained over multiple cycles. Longo et al37 had the largest sample size of the three studies (n=222), and also reported the highest percentages in completed responses over the acute phase (97.7%). Despite slight differences in regimen, each study found the combination of medications to be effective and well tolerated. Constipation, headache, and fatigue were the most commonly reported side effects. However, Grote et al38 reported that the majority of side effects experienced were mild in nature.
The triple therapy was also studied in patients receiving doxorubicin and cyclophosphamide (AC).39,40 Hesketh and Sanz-Altamira39 administered aprepitant 125 mg, dexamethasone 8–10 mg and palonosetron 0.25 mg on day 1, followed by dexamethasone 4 mg and aprepitant 80 mg once daily for days 2–3 to 36 patients. Grunberg et al40 on the other hand, opted to administer aprepitant 286 mg, dexamethasone 20 mg, and palonosetron 0.25 mg on day 1 only to 41 patients. Both studies found the treatment to be well tolerated overall, with the majority of side effects to be minor in nature. Despite having a similar regimen to the studies involving cisplatin-based chemotherapy, Hesketh and Sanz-Altamira39 found that further improvement in efficacy is warranted, as a only half of the study patients were able to achieve CR overall.39 On the other hand, single-day triple-therapy may be effective against MEC, and requires more study.40
Despite the vast research that has been conducted using the triple therapy, one group concluded that this combination with palonosetron as the 5-HT3RA did not significantly improve CINV compared to those containing another 5-HT3RA in patients receiving multiday HEC.41 The CR and CC rates in both study arms were similar with 89.0% and 87.7%, respectively in palonosetron-based triple therapy.
Combination studies – netupitant and palonosetron (NEPA)
A few studies have been conducted to evaluate the efficacy of a new NK-1 RA called netupitant that works in combination with palonosetron to improve control of CINV. The antiemetic effect is due to the ability of palonosetron to inhibit crosstalk between 5-HT3 and NK-1 receptors as well as both palonosetron and netupitant working to inhibit SP.42 The characteristics of these studies have been summarized in Tables 5 and 6. A Phase II study was conducted to determine an appropriate clinical dose of NEPA to evaluate in subsequent Phase III trials.43 Subjects were randomized to “PALO”, “NEPA100”, “NEPA200”, “NEPA300”, or “APR + OND” arms. The 136 patients in the PALO (palonosetron) arm received of 0.50 mg oral palonosetron, 20 mg oral dexamethasone, and placebo, followed by 8 mg of oral dexamethasone for days 2–4. There were 135, 136, 142, and 143 patients in each NEPA arm that received 100, 200, or 300 mg of netupitant rather than placebo, respectively. For the APR (aprepitant) + OND (ondansetron) arm, 125 mg oral aprepitant, 32 mg IV ondansetron, and 12 mg oral dexamethasone were given to subjects on day 1 followed by 80 mg oral aprepitant and 4 mg oral dexamethasone on days 2–4. Compared to the PALO arm, this group found that each NEPA dose increased the prevention of both acute and delayed CINV following HEC (Table 6). The CR of the PALO arm was 89.7% in the acute phase whereas the NEPA arms ranged from 92.7% to 98.5%. In the delayed phase, the CR of the PALO arm was 80.1% and the NEPA arms ranged from 90.4% to 91.2%. This group suggested NEPA300 was an appropriate dose due to the higher CR rate of 98.5% in the acute phase and 90.4% in the delayed phase, as observed in their patient group.43
A subsequent Phase III study compared the safety and efficacy of the additional 300 mg netupitant to palonosetron.42 Aapro et al42 randomized patients being treated with MEC to receive either NEPA plus dexamethasone (n=724) or palonosetron plus dexamethasone (n=725). The researchers showed that NEPA plus a single dose of dexamethasone was significantly better than the combination of palonosetron and dexamethasone in preventing CINV in both the acute and delayed phases. Adding dexamethasone to NEPA increased the CR rate from 85.0% to 88.4% in the acute setting and from 69.5% to 76.9% in the delayed setting.42
In both studies, the most common reported adverse event was headache (3.2%, and 0.7%–2.2%, respectively). Additionally, constipation and hiccups were also noted to be common adverse events (5.1% occurrence). The majority of these events were considered to be mild or moderate in nature.42,43
Patient satisfaction and quality of life
Only a few studies discussed patient satisfaction with antiemetic therapy9,30 and the impact of treatment on quality of life.9,28,30,37 Global satisfaction was rated based on a visual analog scale from 0 (completely unsatisfied) to 10 (completely satisfied).9,30 Di Renzo et al9 found that patients receiving single dose palonosetron had a median global satisfaction score of 8.0 (based on a visual analog scale from 1 to 10) with the antiemetic therapy. With the administration of dexamethasone, the median patient reported global satisfaction score was 9.0.30
Longo et al37 found that fatigue and pain were the major factors that affected quality of life. In addition, 33% of patients felt a reduction in their social activity during antiemetic therapy.37 However, a study conducted by Aapro et al28 found that, overall, the quality of life was preserved. Evaluated with the functional living index-emesis (FLIE) questionnaire for nausea and vomiting, it was found that no statistically significant differences in quality of life were observed with respect to therapy.28
Discussion
Nausea and vomiting is a common side effect of chemotherapy that can be difficult to prevent and subsequently control. The reason for this is likely multifactorial in nature, but may be due to the lack of complete understanding surrounding the mechanism of CINV, in addition to interpatient differences in toxicity to chemotherapy agents.1
Many studies have been conducted in order to prevent the occurrence of CINV. Historically, dopamine receptors have been the targets of interest; however, since the discovery of 5-HT3 receptor involvement in the pathophysiology of CINV, a near paradigm shift has occurred in how this chemotherapy-induced toxicity is managed.
Palonosetron, a second generation 5-HT3RA, has a strong binding affinity to the 5-HT3 receptor and has been shown to be an effective treatment for both acute and delayed phase CINV.9 In addition to its ability to bind tightly to serotonin receptors, palonosetron partitions into tissue to a high extent and as a result demonstrates a relatively long half-life of approximately 40 hours, which may contribute to its effect in the delayed phase of CINV.10,12–16
Many studies have found evidence supporting the potential role of palonosetron in CINV treatment. A Phase II study concerning palonosetron as a treatment with 34 patients given LEC found it to be an effective alternative, citing the fact that more than 50% of patients taking part achieved CC.18 A number of studies have also examined its use in patients receiving MEC. Di Renzo et al9 in particular found very promising results in terms of its effectiveness, as more than 75% of 86 patients were able to achieve CC in both acute and delayed phases. Treatment has also been conducted in 44 patients receiving HEC, where significantly higher rates of CR and CC have been found for palonosetron in the delayed phase.24 Overall, palonosetron alone has been shown to be effective in emetogenic chemotherapy, particularly in the delayed phase. With respect to treatment following HEC, however, some studies have not been successfully reproduced, warranting further examination.23
Formulations of palonosetron include oral and IV routes. Boccia et al19 found that while oral administration provided greater results in the acute phase, an IV injection was more effective in the delayed phase, at comparable doses. In comparison to existing treatments; studies have suggested that palonosetron is superior or noninferior compared with first generation 5-HT3RAs, such as dolasetron and ondansetron, when administered at much lower doses.20,21
Several studies have also combined the palonosetron regimen with other. With the addition of dexamethasone, Boccia et al20 found greater CR rates in the acute and delayed phases, with the increase in the acute phase being more pronounced. Evidence also favors the combination’s effect in response to many forms of chemotherapy.26–34
Various studies have attempted to further increase the efficacy of the palonosetron–dexamethasone combination by adding yet another antiemetic known as aprepitant. Aprepitant is an NK-1 RA, and its addition was tested in patients receiving HEC. Although dosing regimens differed, the triple-therapy was found to be very well tolerated.37–39 Some studies however, have found contrary evidence, citing disparities in efficacy.40 In MEC cohorts, Grunberg et al40 found that single-day triple-therapy may be effective in treating CINV. This represents yet another step toward realizing the full potential of this combination, and future studies should seek to establish its place in therapy as well. Overall, more research is required in order to establish the triple therapy’s place in CINV treatment. However, current results stand as a testament as to the steps that have been taken toward CINV treatment, particularly in individuals receiving HEC.
The combination of NEPA has also been examined. This combination has been reported to be very well tolerated, and it was found that CINV prevention increased with larger doses of netupitant. It is dosed at 300 mg once daily and has been shown to be very successful in the prevention of CINV following HEC and MEC.35,36
Overall, a major drawback of first generation 5-HT3RAs includes prolongation of the QT interval. Studies have shown alterations in the QT interval while on palonosetron are not statistically significant, making it less concerning for use in patients suffering from cardiac diseases.42 While some severe adverse reactions have been reported, study coordinators have dubbed them as unrelated to the treatment regimen. Overall, side effects as a result of palonosetron administration, alone and in combination with other antiemetics, have all been mild to moderate in nature, with headache, constipation, and fatigue being the most common.
Overall, palonosetron stands as an effective option for CINV treatment. It is very well tolerated, and its use is advantageous over first generation serotonin receptor antagonists. Several studies have examined its relative efficacy and have deemed it superior to current antiemetic CINV treatments, as it is able to prevent both acute and delayed phase emesis. Future research should identify the most promising antiemetic combinations, especially for patients receiving HEC.
Acknowledgments
We thank the generous support of the Bratty Family Fund, Michael and Karyn Goldstein Cancer Research Fund, Pulenzas Cancer Research Fund, Joseph and Silvana Melara Cancer Research Fund, and Ofelia Cancer Research Fund.
Disclosure
The authors report no conflicts of interest in this work.
References
Navari RM. Management of chemotherapy-induced nausea and vomiting. Drugs. 2013;73:249–262. | ||
Grunberg SM, Slusher B, Rugo HS. Emerging treatments in chemotherapy-induced nausea and vomiting. Clin Adv Hematol Oncol. 2013;11(2 Suppl 1):1–18. | ||
Rojas C, Slusher BS. Pharmacological mechanisms of 5-HT3 and tachykinin NK1 receptor antagonism to prevent chemotherapy-induced nausea and vomiting. Eur J Pharmacol. 2012;684(1–3):1–7. | ||
Popovic M, Warr DG, Deangelis C, et al. Efficacy and safety of palonosetron for the prophylaxis of chemotherapy-induced nausea and vomiting (CINV): a systematic review and meta-analysis of randomized controlled trials. Support Care Cancer. 2014;22(6):1685–1697. | ||
Gao HF, Liang Y, Zhou NN, Zhang DS, Wu HY. Aprepitant plus palonosetron and dexamethasone for prevention of chemotherapy-induced nausea and vomiting in patients receiving multiple-day cisplatin chemotherapy. Intern Med J. 2013;43(1):73–76. | ||
Rojas C, Raje M, Tsukamoto T, Slusher BS. Molecular mechanisms of 5-HT3 and NK1 receptor antagonists in prevention of emesis. Eur J Pharmocol. 2014;722:26–37. | ||
Aziz F. Neurokinin-1 receptor antagonists for chemotherapy-induced nausea and vomiting. Ann Palliat Med. 2012;1(2):130–136. | ||
Navari RM. Role of neurokinin-1 receptor antagonists in chemotherapy-induced emesis: summary of clinical trials. Cancer Invest. 2004;22(4):569–576. | ||
Di Renzo N, Montanini A, Mannina D, et al. Single-dose palonosetron for prevention of chemotherapy-induced nausea and vomiting in patients with aggressive non-Hodgkin’s lymphoma receiving moderately emetogenic chemotherapy containing steroids: results of a phase II study from the Gruppo Italiano per lo Studio dei Linfomi (GISL). Support Care Cancer. 2011;19:1505–1510. | ||
Product Monograph. Aloxi®. Missisauga, ON: Eisai Limited; 2012. | ||
Rojas C, Li Y, Zhang J, et al. The antiemetic 5-HT3 receptor antagonist Palonosetron inhibits substance P-mediated responses in vitro and in vivo. J Pharmacol Exp Ther. 2010;335(2):362–368. | ||
Stoltz R, Cyong JC, Shah A, Parisi S. Pharmacokinetic and safety evaluation of palonosetron, a 5-hydroxytryptamine-3 receptor antagonist, in U.S. and Japanese healthy subjects. J Clin Pharmacol. 2004;44(5):520–531. | ||
Eisenberg P, Mackintosh FR, Ritch P, Cornett PA, Macciocchi A. Efficacy, safety and pharmacokinetics of palonosetron in patients receiving highly emetogenic cisplatin-based chemotherapy: a dose-ranging clinical study. Ann Oncol. 2004;15(2):330–337. | ||
Ikari Y, Ogata K, Nakashima Y, et al. Safety and pharmacokinetic evaluation of repeated intravenous administration of palonosetron 0.75 mg in patients receiving highly or moderately emetogenic chemotherapy. Support Care Cancer. 2014;22(7):1959–1964. | ||
Shah A, DeGroot T, Apseloff G. Pharmacokinetic evaluation and safety profile of a 15-minute versus 30-second infusion of palonosetron in healthy subjects. J Clin Pharmacol. 2006;46(10):1139–1145. | ||
Hunt TL, Gallagher SC, Cullen MT Jr, Shah AK. Evaluation of safety and pharmacokinetics of consecutive multiple-day dosing of palonosetron in healthy subjects. J Clin Pharmacol. 2005;45(5):589–596. | ||
Sadaba B, del Barrio A, Campanero MA, et al. Randomized pharmacokinetic study comparing subcutaneous and intravenous palonosetron in cancer patients treated with platinum based chemotherapy. PLoS One. 2014;9(2):e89747. | ||
Hesketh PJ, Morrow G, Komorowski AW, Ahmed R, Cox D. Efficacy and safety of palonosetron as salvage treatment in the prevention of chemotherapy-induced nausea and vomiting in patients receiving low emetogenic chemotherapy (LEC). Support Care Cancer. 2012;20(1):2633–2677. | ||
Boccia R, Grunberg S, Franco-Gonzales E, et al. Efficacy of oral palonosetron compared to intravenous palonosetron for the prevention of chemotherapy-induced nausea and vomiting associated with moderately emetogenic chemotherapy: a phase 3 trial. Support Care Cancer. 2013;21:1453–1460. | ||
Eisenberg P, Figueroa-Vadillo J, Zamora R, et al. Improved prevention of moderately emetogenic chemotherapy-induced nausea and vomiting with palonosetron, a pharmacologically novel 5-HT3 receptor antagonist: results of a phase III, single-dose trial versus dolasetron. Cancer. 2003;98(11):2473–2482. | ||
Gralla R, Lichinitser M, Van Der Vegt S, et al. Palonosetron improves prevention of chemotherapy-induced nausea and vomiting following moderately emetogenic chemotherapy: results of a double-blind randomized phase III trial comparing single doses of palonosetron with ondansetron. Ann Oncol. 2003;14(10):1570–1577. | ||
Choi BS, Borsaru GP, Ballinari G, Voisin D, Di Renzo N. Multicenter phase IV study of palonosetron in the prevention of chemotherapy-induced nausea and vomiting (CINV) in patients with non-Hodgkin lymphomas undergoing repeated cycles of moderately emetogenic chemotherapy. Leuk Lymphoma. 2014;55(3):544–550. | ||
Mattiuzzi GN, Cortes JE, Blamble DA, et al. Daily palonosetron is superior to ondansetron in the prevention of delayed chemotherapy-induced nausea and vomiting in patients with acute myelogenous leukemia. Cancer. 2010;116(24):5659–5666. | ||
Dong X, Huang J, Cao R, Liu L. Palonosetron for prevention of acute and delayed nausea and vomiting in non-small-cell lung carcinoma patients. Med Oncol. 2011;28:1425–1429. | ||
Tian W, Wang Z, Zhou J. Randomized, double-blind, crossover study of palonosetron compared with granisetron for the prevention of chemotherapy-induced nausea and vomiting in a Chinese population. Med Oncol. 2011;28:71–78. | ||
Maemondo M, Masuda N, Sekine I, et al. A phase II study of palonosetron combined with dexamethasone to prevent nausea and vomiting induced by highly emetogenic chemotherapy. Ann Oncol. 2009;20(11):1860–1866. | ||
Massa E, Astara G, Madeddu C, et al. Palonosetron plus dexamethasone effectively prevents acute and delayed chemotherapy-induced nausea and vomiting following highly or moderately emetogenic chemotherapy in pre-treated patients who have failed to respond to a previous antiemetic treatment: comparison between elderly and non-elderly patient response. Crit Rev Oncol Hematol. 2009;70(1):83–91. | ||
Aapro M, Fabi A, Nolè F, et al. Double-blind, randomized, controlled study of the efficacy and tolerability of palonosetron plus dexamethasone for 1 day with or without dexamethasone on days 2 and 3 in the prevention of nausea and vomiting induced by moderately emetogenic chemotherapy. Ann Oncol. 2010;21(5):1083–1088. | ||
Celio L, Frustaci S, Denaro A, et al. Palonosetron in combination with 1-day versus 3-day dexamethasone for prevention of nausea and vomiting following moderately emetogenic chemotherapy: a randomized, multicenter, phase III trial. Support Care Cancer. 2011;19(8):1217–1225. | ||
Brugnatelli S, Gattoni E, Grasso D, Rossetti F, Perrone T, Danova M. Single-dose palonosetron and dexamethasone in preventing nausea and vomiting induced by moderately emetogenic chemotherapy in breast and colorectal cancer patients. Tumori. 2011;97(3):362–366. | ||
Rozzi A, Nardoni C, Corona M, et al. Palonosetron for the prevention of chemotherapy-induced nausea and vomiting in glioblastoma patients treated with temozolomide: a phase II study. Support Care Cancer. 2011;19(5):697–701. | ||
Lorusso V, Giampaglia M, Petrucelli L, Saracino V, Perrone T, Gnoni A. Antiemetic efficacy of single-dose palonosetron and dexamethasone in patients receiving multiple cycles of multiple day-based chemotherapy. Support Care Cancer. 2012;20(12):3241–3246. | ||
Aogi K, Sakai H, Yoshizawa H, et al. A phase III open-label study to assess safety and efficacy of palonosetron for preventing chemotherapy-induced nausea and vomiting (CINV) in repeated cycles of emetogenic chemotherapy. Support Care Cancer. 2012;20(7):1507–1514. | ||
Lorusso V, Spedicato A, Petrucelli L, Saracino V, Giampaglia M, Perrone T. Single dose of palonosetron plus dexamethasone to control nausea, vomiting and to warrant an adequate food intake in patients treated with highly emetogenic chemotherapy (HEC). Preliminary results. Support Care Cancer. 2009;17(12):1469–1473. | ||
Yavas C, Dogan U, Yavas G, Araz M, Ata OY. Acute effect of palonosetron on electrocardiographic parameters in cancer patients: a prospective study. Support Care Cancer. 2012;20(10):2343–2347. | ||
Dogan U, Yavas G, Tekinalp M, Yavas C, Ata OY, Ozdemir K. Evaluation of the acute effect of palonosetron on transmural dispersion of myocardial repolarization. Eur Rev Med Pharmacol Sci. 2012;16(4):462–468. | ||
Longo F, Mansueto G, Lapadula V, et al. Palonosetron plus 3-day aprepitant and dexamethasone to prevent nausea and vomiting in patients receiving highly emetogenic chemotherapy. Support Care Cancer. 2011;19(8):1159–1164. | ||
Grote T, Hajdenberg J, Cartmell A, Ferguson S, Ginkel A, Charu V. Combination therapy for chemotherapy-induced nausea and vomiting in patients receiving moderately emetogenic chemotherapy: palonosetron, dexamethasone, and aprepitant. J Support Oncol. 2006;4(8):403–408. | ||
Hesketh PJ, Sanz-Altamira P. Aprepitant, dexamethasone, and palonosetron in the prevention of doxorubicin/cyclophosphamide-induced nausea and vomiting. Support Care Cancer. 2012;20(3):653–656. | ||
Grunberg SM, Dugan M, Muss H, et al. Effectiveness of a single-day three-drug regimen of dexamethasone, palonosetron, and aprepitant for the prevention of acute and delayed nausea and vomiting caused by moderately emetogenic chemotherapy. Support Care Cancer. 2009;17(5):589–594. | ||
Kim KI, Lee DE, Cho I, et al. Effectiveness of palonosetron versus other serotonin 5-HT3 receptor antagonists in triple antiemetic regimens during multiday highly emetogenic chemotherapy. Ann Pharmacother. 2012;46(12):1637–1644. | ||
Aapro M, Rugo H, Rossi G, et al. A randomized phase III study evaluating the efficacy and safety of NEPA, a fixed-dose combination of netupitant and palonosetron, for prevention of chemotherapy-induced nausea and vomiting following moderately emetogenic chemotherapy. Ann Oncol. 2014;25(7):1328–1333. | ||
Hesketh PJ, Rossi G, Rizzi G, et al. Efficacy and safety of NEPA, an oral combination of netupitant and palonosetron, for prevention of chemotherapy-induced nausea and vomiting following highly emetogenic chemotherapy: a randomized dose-ranging pivotal study. Ann Oncol. 2014;25(7):1340–1346. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.