Back to Journals » International Medical Case Reports Journal » Volume 8
Unrecognized clozapine-related constipation leading to fatal intra-abdominal sepsis – a case report
Authors Oke V, Schmidt F, Bhattarai B, Basunia M, Agu C, Kaur A, Enriquez D, Quist J, Salhan D, Gayam V, Mungikar P
Received 16 April 2015
Accepted for publication 27 May 2015
Published 11 September 2015 Volume 2015:8 Pages 189—192
DOI https://doi.org/10.2147/IMCRJ.S86716
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Ronald Prineas
Vikram Oke, Frances Schmidt, Bikash Bhattarai, Md Basunia, Chidozie Agu, Amrit Kaur, Danilo Enriquez, Joseph Quist, Divya Salhan, Vijay Gayam, Prajakta Mungikar
Department of Pulmonary Medicine, Interfaith Medical Center, NY, USA
Abstract: Clozapine is the preferred antipsychotic used for the treatment of resistant schizophrenia with suicidal ideation. The drug is started at a low dose and gradually increased to a target dose of 300–450 mg/day. It is well known to cause agranulocytosis and neutropenia. Several cases of fatal sepsis have been reported in neutropenic patients and emphasis is placed on monitoring for agranulocytosis; however, clozapine also causes intestinal hypomotility and constipation, which if unrecognized can lead to intestinal obstruction, bowel necrosis, and intra-abdominal sepsis. Reduced behavioral pain reactivity in schizophrenics may alter the ability to express pain, potentially leading to a delay in the presentation for medical attention. We report a case of fatal intra-abdominal sepsis secondary to an unrecognized case of clozapine-related constipation.
Keywords: antipsychotics, clozapine, schizophrenia, syncope, constipation, sepsis
Introduction
Clozapine is an antipsychotic that is used to treat schizophrenia. It has minimal extrapyramidal side effects compared to first-generation antipsychotics.1 Several cases of fatal sepsis have been reported in neutropenic patients and emphasis is placed on monitoring for agranulocytosis.2 Clozapine-related constipation is a recognized side effect, but unfortunately not well known. If not recognized early, the consequences can be deleterious. We discuss just such a fatal case of intra-abdominal sepsis secondary to unrecognized clozapine constipation.
Case report
A 61-year-old Hispanic male with a history of undifferentiated schizophrenia was admitted to the intensive care unit after a rapid response team evaluated him in the psychiatric unit for a syncopal episode.
The patient was being managed in the psychiatry floor for agitation and aggressive behavior and had been there for 5 weeks before this presentation. Patient had multiple psychiatry admissions for similar reasons. At baseline, the patient was unable to speak in meaningful sentences but responded by answering “yes” or “no” to goal-directed questions.
The patient was on levothyroxine for hypothyroidism, which was well controlled with free thyroid-stimulating hormone of 1.20 for 2 weeks before the current presentation. He also had seizure disorder, which was being treated with divalproex sodium extended release 1,000 mg daily, and levetiracetam 750 mg twice daily.
The patient was being treated with clozapine for his schizophrenia. The treatment of the patient was started with clozapine 5 weeks back during the current psychiatric admission, and dose gradually increased to 150 mg everyday in the morning and 150 mg everyday in the evening. His evening dose was increased to 175 mg everyday in the evening 5 days before this presentation. He had glaucoma for which he was receiving dorzolamide/timolol eye drops. He was not on any other medications. He was given a regular diet and was encouraged to take plenty of fluids and fibers. He did not have any surgical history.
The patient was apparently well until the day of this presentation when the patient was noted to walk around the nursing station and appeared as if about to fall and developed a syncopal episode. The vitals were temperature 98°F (36.6°C), blood pressure 86/54 mmHg, pulse 127 beats/min, regular, respiratory rate 16 breaths/min, and oxygen saturation 100% while breathing ambient air. Intravenous access was obtained and normal saline of 500 mL bolus was administered. The patient became responsive within few minutes and tried to get up. He was moving all his limbs and did not appear to have any focal motor deficits. No seizure activity was noted. He was confused, agitated, and unable to provide any history. The patient was transferred to the intensive care unit.
Physical examination was significant for abdominal distension with hypoactive bowel sounds. Rectal examination revealed hard impacted stool in the rectal vault. Stool qualitative guaiac test was performed, which was negative.
The complete blood count revealed leukocyte count of 17,300/mm3 with neutrophil differential of 52% with absolute neutrophil count (ANC) of 9,000/mm3 with band neutrophils of 12%. Prior to the syncopal episode, the weekly leukocyte counts after the initiation of clozapine were as follows:
Week 1 – Leukocyte count 7,100/mm3 with neutrophil differential of 45% (ANC, 3,195/mm3).
Week 2 – Leukocyte count 6,600/mm3 with neutrophil differential of 61% (ANC, 4,026/mm3).
Week 3 – Leukocyte count 5,400/mm3 with neutrophil differential of 65% (ANC, 3,510/mm3).
Week 4 – Leukocyte count 5,200/mm3 with neutrophil differential of 60% (ANC, 3120/mm3).
Week 5 – Leukocyte count 6,500/mm3 with neutrophil differential of 67% (ANC, 4,355/mm3).
Hemoglobin was 18.6 g/dL, the baseline range was 13–14 g/dL. Comprehensive metabolic panel was significant for elevated blood urea nitrogen (BUN)/creatinine of 34/1.4; however, baseline BUN/creatinine range was 13.0–17.0/0.8–1.0. Liver function tests were within normal limits. Sodium, potassium, magnesium, and phosphorous were normal. Serum bicarbonate was low at 18 mmol/L with low serum chloride of 100 mmol/L and elevated anion gap of 17. Serum lactic acid was elevated at 115.4 mg/dL. Serum total protein, albumin, globulin, and creatine kinase were normal. Serum valproic level was 60 μg/mL, serum clozapine level was not available.
Electrocardiogram revealed sinus tachycardia without any acute ST-T segment changes. Serum troponin I was normal.
Urinalysis revealed high specific gravity, with no bacteria or elevated nitrate. Urine toxicology was negative.
Chest X-ray (Figure 1) was significant for elevated hemidiaphragm with low lung volumes and clear lung fields. Abdominal X-ray (Figure 2) revealed large amount of fecal content in the colon and dilated small bowel suggestive of bowel obstruction from fecal impaction. The patient was started on broad spectrum antibiotics after pan cultures were obtained and intravenous fluids were administered; however, he had a rapid decline in clinical status with worsening hypotension. Surgical evaluation was requested for possible surgical intervention of bowel obstruction; however, he was deemed to be too unstable for any surgical intervention. He was being managed as per surviving sepsis guidelines for septic shock.3 He developed cardiac arrest and unfortunately expired within 12 hours of presentation. The blood culture revealed Escherichia coli within 24 hours. Urine culture revealed no growth.
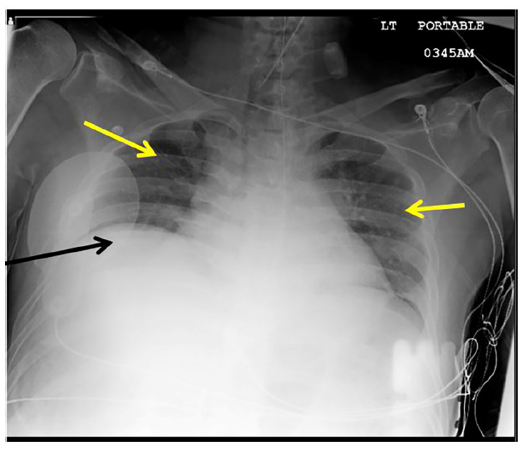 | Figure 1 Chest X-ray showing clear lung fields with low lung volumes (yellow arrows), elevated hemi diaphragm (black arrow). |
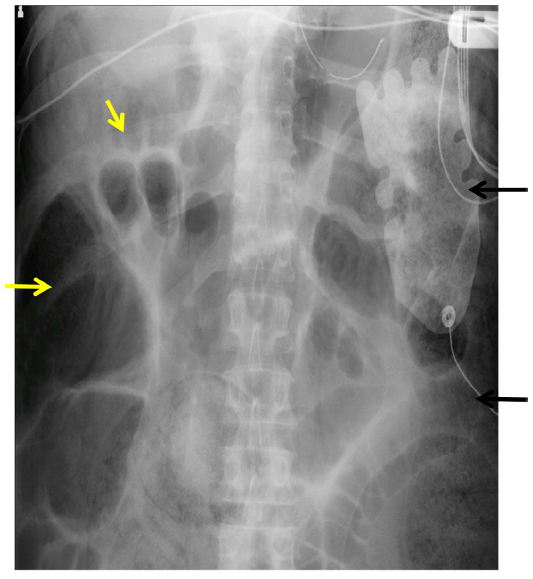 | Figure 2 Abdominal X-ray with dilated small bowel (yellow arrows) and fecal impaction (black arrows). |
The patient did not have a prior history of constipation or fecal impaction, or any other risk factors for constipation. He was described as being minimally communicative, often mumbling incoherent words, and disorganized and aggressive at times.
Discussion
Clozapine is a second-generation antipsychotic with antagonistic actions at dopamine (D1, D2, D3, D4, D5), serotonin (5-HT1A, 5-HT2A, 5-HT2C), muscarinic (M1, M2, M3, M5), α1- and α2-adrenergic, and histamine (H1) receptors. Clozapine is an agonist at muscarinic (M4) receptors.1
Clozapine leads to minimal extrapyramidal symptoms compared to first-generation antipsychotics. It is a preferred medication in patients with treatment-resistant schizophrenia and also in schizophrenia with suicidal ideation.1
Treatment is usually started at low doses of 12.5–25 mg once or twice daily and gradually increased by 25–50 mg/day until a target dose of approximately 200–400 mg/day is achieved.1,4
Clozapine is metabolized by CYP1A2 enzyme. If CYP 450 inducers and inhibitors have to be used in patients treated with clozapine, they should be used judiciously.1,4
Patients should have baseline leukocyte, including ANCs, before treatment with clozapine is initiated and these should be monitored weekly for first 6 months and then every 2 weeks.4
Agranulocytosis (ANC <1,000), severe orthostatic hypotension, bradycardia, syncope may occur with the use of clozapine. Fatal cases of myocarditis/cardiomyopathy have also occurred. Clozapine is not approved for dementia-related psychosis.2,5,6
Constipation can occur in up to 60% of patients treated with clozapine.7 Ileus is seen in close to 1.3% of patients treated with clozapine.8 Gastric outlet obstruction can occur in up to 33% of patients treated with clozapine. There have been case reports on fatal bowel ischemia on patients treated with clozapine.9–11 Mortality from complications secondary to constipation is higher with clozapine than other antipsychotic medications.12–14 These side effects can be explained by the antimuscarinic action of clozapine. Concomitant use of other antidepressants, antipsychotics, poor dietary habits with low fiber diets, and sedentary lifestyle seem to compound this problem.15 The prevalence and severity of constipation may be dose dependent.16 Doses that cause serum levels to increase above 500 mg/dL are not advised and should be lowered to target the serum level between 200 and 400 mg/dL.1,17 However, recent data indicate that there is minimal correlation between clozapine levels and side effects except for sedation, hypotension, and seizure activity, and that monitoring clozapine levels might be indicated when >600 mg/day doses are prescribed, there is a change in concomitant medications or cigarette use or suboptimal therapeutic response.18 CYP inhibitors should be avoided as they could worsen these side effects potentially by increasing serum levels of clozapine. Whether schizophrenic patients are relatively insensitive to pain is debatable. It has been reported that up to 37% of schizophrenic patients with acute appendicitis and up to 21% of patients with perforated peptic ulcer did not report pain, which led to surgical intervention late in the course of the disease.19–21 Recent studies have shown that there is little evidence to support the relative pain insensitivity in these patients. However, behavioral reactivity to pain and self-reported response to pain may be reduced. Negative symptoms of schizophrenia may alter the ability of patients from expressing pain.22 These factors may potentially lead to the delay in presentation for medical attention. Physicians should maintain a high level of suspicion of serious medical illnesses during evaluation of schizophrenic patients.23–27 Our patient was minimally communicative and likely could not report constipation by himself. Upon questioning, he denied having any pain or discomfort; however, there was no emphasis laid on asking specifically about constipation.
These symptoms of constipation may be trivialized and may not be appreciated as precursors of a possible fatal condition in the background of a psychotic condition.28 Constipation could lead to intestinal obstruction with resulting bowel necrosis.10 In the absence of an autopsy, it is very difficult to establish an exact diagnosis, but we hypothesize that fatal sepsis resulted from bacterial translocation secondary to clozapine induced constipation or its sequelae-like bowel obstruction, infarction.
Conclusion
Constipation is a recognized side effect of clozapine, which unfortunately is not as well known as it should be. Reduced behavioral reactivity to pain may alter the ability of patients to express pain. With the increasing use of clozapine for treatment of resistant schizophrenia, patients should be monitored for the development of constipation as it may herald a life-threatening complication. Physicians involved in the care of patients treated with clozapine should have a high index of suspicion for constipation and intestinal obstruction, and a bowel chart may be used for the daily assessment of admitted patients treated with clozapine. Increased fluid and fiber intake could be protective.
Disclosure
The authors report no conflicts of interest in this work.
References
American Psychiatric Association. Practice Guideline for the Treatment of Patients with Schizophrenia. 2nd ed. Arlington, VA: American Psychiatric Association; 2004:73–77. | |
Alvir JM, Lieberman JA, Safferman AZ, Schwimmer JL, Schaaf JA. Clozapine-induced agranulocytosis – incidence and risk factors in the United States. N Engl J Med. 1993;329(3):162–167. | |
Dellinger RP, Levy MM, Rhodes A, et al; Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup. Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580–637. | |
Novartis Pharmaceuticals Corporation. Clairol Prescribing Information. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2003. Available from: http://www.clozaril.com. | |
Marinkovic D, Timotijevic I, Babinski T, Totic S, Paunovic VR. The side-effects of clozapine: a four year follow-up study. Prog Neuropsychopharmacol Biol Psychiatry. 1994;18(3):537–544. | |
Safferman A, Lieberman JA, Kane JM, Szymanski S, Kinon B. Update on the clinical efficacy and side effects of clozapine. Schizophr Bull. 1991;17(2):247–261. | |
Young CR, Bowers MB, Mazure CM. Management of the adverse effects of clozapine. Schizophr Bull. 1998;24(3):381–390. | |
Lu MK. [Clinical analysis in the main side effects of clozapine: enclosed 600 cases report]. Zhonghua Shen Jing Jing Shen Ke Za Zhi. 1991;24(2):71–74. Chinese. | |
Bourgeois OD, James A. Clozapine, fluoxetine, and benztropine-associated ileus: case report. Jefferson J Psychiatry. 2007;21(1):1. | |
Tang WK, Ungvari GS. Clozapine-induced intestinal obstruction. Aust N Z J Med. 1999;29(4):560–560. | |
Townsend G, Curtis D. Case report: rapidly fatal bowel ischaemia on clozapine treatment. BMC Psychiatry. 2006;6(1):43. | |
Cohen D, Bogers JP, van Dijk D, Bakker B, Schulte PF. Beyond white blood cell monitoring: screening in the initial phase of clozapine therapy. J Clin Psychiatry. 2012;73(10):1307–1312. | |
De Hert M, Hudyana H, Dockx L, et al. Second-generation antipsychotics and constipation: a review of the literature. Eur Psychiatry. 2011;26(1):34–44. | |
Baptista T. A fatal case of ischemic colitis during clozapine administration. Rev Bras Psiquiatr. 2014;36(4):358–358. | |
Nielsen J, Meyer JM. Risk factors for ileus in patients with schizophrenia. Schizophr Bull. 2012;38(3):592–598. | |
Pare J, Riffand P, Baurdeix I. The clozapine in France. Inf Psychiatr. 1993;4:389–397. | |
Perry PJ, Miller DD, Arndt SV, Cadoret RJ. Clozapine and norclozapine plasma concentrations and clinical response of treatment-refractory schizophrenic patients. Am J Psychiatry. 1991;148(2):231–235. | |
Stark A, Scott J. A review of the use of clozapine levels to guide treatment and determine cause of death. Aust N Z J Psychiatry. 2012;46(9):816–825. | |
Dworkin RH. Pain insensitivity in schizophrenia: a neglected phenomenon and some implications. Schizophr Bull. 1994;20:235–248. | |
Marchand WE, Sarota B, Marble HC, Leary TM, Burbank CB, Bellinger MJ. Occurrence of painless acute surgical disorders in psychotic patients. N Engl J Med. 1959;260(12):580–585. | |
West BM, Hecker AO. Peptic ulcer: incidence and diagnosis in psychotic patients. Am J Psychiatry. 1952;109(1):35–37. | |
Pelizza L, De Luca P, La Pesa M, Borella D. Clozapine-induced intestinal occlusion: a serious side effect. Acta Biomed. 2007;78(2):144–148. | |
Singh MK, Giles LL, Nasrallah HA. Pain insensitivity in schizophrenia: trait or state marker? J Psychiatr Pract. 2006;12(2):90–102. | |
Bonnot O, Tordjman S. [Schizophrenia and pain reactivity]. Presse Med. 2008;37(11):1561–1568. French. | |
Autié A, Montreuil M, Moulier V, Braha S, Wojakiewicz A, Januel D. [Pain and schizophrenia: myth and reality]. Encephale. 2009;35(4):297–303. French. | |
Bonnot O, Anderson GM, Cohen D, Willer JC, Tordjman S. Are patients with schizophrenia insensitive to pain? A reconsideration of the question. Clin J Pain. 2009;25(3):244–252. | |
Rosenthal SH, Porter KA, Coffey B. Pain insensitivity in schizophrenia: case report and review of the literature. Gen Hosp Psychiatry. 1990;12(5):319–322. | |
Levin TT, Barrett J, Mendelowitz A. Death from clozapine-induced constipation: case report and literature review. Psychosomatics. 2002;43(1):71–73. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.