Back to Journals » Open Access Journal of Contraception » Volume 10
Unmet Need for Contraception Among Young Married Women in Eastern Ethiopia
Authors Dingeta T ![]() , Oljira L
, Oljira L ![]() , Worku A, Berhane Y
, Worku A, Berhane Y ![]()
Received 14 August 2019
Accepted for publication 25 November 2019
Published 17 December 2019 Volume 2019:10 Pages 89—101
DOI https://doi.org/10.2147/OAJC.S227260
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Tariku Dingeta,1 Lemessa Oljira,1 Alemayehu Worku,2 Yemane Berhane3
1School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 2Department of Epidemiology and Biostatistics, School of Public Health, Addis Ababa University, Addis Ababa, Ethiopia; 3Department of Epidemiology, Addis Continental Institute of Public Health, Addis Ababa, Ethiopia
Correspondence: Tariku Dingeta
School of Public Health, College of Health and Medical Sciences, Haramaya University, PO Box 235, Harar, Ethiopia
Tel +251 91 100 5126
Fax +251 25 666 8081
Email [email protected]
Purpose: Addressing the contraceptive needs of young married women is critical to improve their health and well-being. In patriarchal societies, young married women are under intense pressure to demonstrate their fecundity. Therefore, research that specifically address the needs for contraception of young married women have been generally given less emphasis in Ethiopia. This study assessed the extent of unmet needs for contraception and its associated factors among young married women in Eastern Ethiopia.
Methods: A community-based cross-sectional study was conducted among young married women (14–24 years of age) in Eastern Ethiopia. Data were collected using a structured questionnaire. The prevalence ratio (PR) with 95% confidence intervals (CIs) was calculated, and factors associated with unmet needs for contraception were identified using log-binomial regression statistical model.
Results: Among 2933 young women interviewed, the unmet need for contraception was 1014 (34.6%; 95% CI, 32.9%–36.4%). The prevalence of unmet needs for contraception decreased with increased young women’s household decision-making autonomy score (APR= 0. 76; CI=0.62–0.94). Exposure to family planning (FP) information during the last 12 months (APR= 1.24; CI=1.1–1.42), age 18 or more years (APR=1.25; CI=1.04–1.5), multiparty (APR= 1. 9; CI=1.7–2.1) and desire to have 5 children or lesser than 5 children (APR= 1. 2; CI=1.06–1.32) were associated with higher prevalence of unmet needs for contraception.
Conclusion: One-third of married young women had unmet needs for contraception. More efforts to empower women to make decisions that affect their own life and providing appropriate family planning information are necessary to reduce the burden of unmet needs among young married women in rural settings in Ethiopia.
Keywords: unmet need, contraception, married adolescent, decision-making autonomy, family planning information, Kersa HDSS
Introduction
In sub-Saharan Africa, more than 20% of 15–19-year-old adolescents and 60% of 20–24-year-old young adult women are estimated to be in marital union. More than 10% of adolescent girls in the region had their first marriage by the age of 15 years.1–3 In most parts of the region, girls are traditionally expected to give birth immediately after marriage and continue to do so uncontrolled for cultural, religious, gender and other factors, which expose them to the risk of unintended pregnancy that leads to fatal maternal and infant adverse outcome. Unintended pregnancy among married young women accounts for about half of all unintended pregnancies among reproductive-age women.4–6 Although various socio-cultural factors hinder pregnancy planning in these settings,7 unmet needs for contraception are primarily attributed to unintended pregnancies in young married women.6,8,9 Unmet need for contraception refers to the proportion of currently married women of reproductive age not using contraception while wishing either to delay the timing of the next birth for at least 2 years or to prevent if would have preferred to limit childbearing.10
Globally, young married women between the ages of 15 and 24 years experience greater unmet needs than that by married young and sexually active unmarried young women aged between 25 and 49 years.11–13 In sub-Saharan Africa, about half of young married women reported unmet need for contraception.6,14 The Ethiopian Demographic and Health Survey (DHS) revealed that 18.7% of 15–19-year-old married women reported unmet needs for contraception, which is significantly higher as compared to 14.8% of adult married women.2
Many factors are known to contribute to the unmet needs for contraception among young married women. The supply-side factors including inaccessibility of comprehensive contraceptive services and poor information dissemination are among the factors related to young women unmet need for contraception.15–17 Limited knowledge of contraceptive methods was also found to have a significant effect on the unmet need for contraception.18,19 Demographic and economic characteristics including women’s age, age of marriage, educational status, residence of living, duration after marriage, and wealth status were also associated with young married women unmet need for contraception in previous studies.15,20,21 Moreover, reproductive experience including living and ideal number of children, previous history of child or fetal loss and parity as well as interpersonal factors such as household decision-making autonomy, and partner approval of contraception were among the factors that influenced the unmet needs for contraception.16,22–26
In patriarchal societies like Ethiopia, young married women are under strong pressure to conceive immediately after marriage to demonstrate their fecundity and ability to continuously engage in reproduction. More than one in three (32%) births are unintended, and 23.2% of death among reproductive-age women was related to pregnancy which poses a heavier burden on Ethiopian young married women.27,28 Despite the high early marriage and subsequently unintended pregnancy, young married women contraceptive utilization in Ethiopia is also among the lowest in sub-Saharan Africa.29 However, contraceptive studies in Ethiopia are limited to a too broad age range of 15–49 years although young women contraceptive need found to be different from their adult counterpart,29,30 and research that specifically addresses the needs for contraception of young married women has been given less emphasis. Thus, understanding the level of unmet need for contraception has great implications in designing a targeted intervention to fill the gap between young women’s reproductive intentions and their contraceptive practice. Identifying factors associated with unmet need for contraception also assist the effort to identify effective intervention areas to meet young women’s contraceptive needs. This study therefore assessed the extent of unmet needs for contraception and its associated factors among young married women in Eastern Ethiopia.
Methods and Materials
Study Setting and Design
A community-based cross-sectional study was conducted in Kersa Demographic and Health Surveillance System (Kersa HDSS) site, Kersa District, Eastern Ethiopia. Kersa HDSS site consists of 21 rural and 3 urban kebeles (the smallest political administration in Ethiopia), with 6 health centers and 19 health posts. The site constitutes 26,061 households and 29,210 married reproductive-age women of which 11% were young women aged 15–24 years.31,32 More than four-fifth and three-fourth of married women in the study site were married and gave first birth before 20 years of age, respectively. The total fertility rate (TFR) among reproductive age in the study site was 5.5 with a 2.9% annual population growth rate.32–34
Population and Sampling Technique
The study population constituted currently married young women, less than 25 years of age, who were permanent residents of the study sites. The Kersa HDSS database maintained by Haramaya University was used as a sampling frame to identify a list of the young married woman. All young married women identified from the database were invited to participate in the study. Out of the 3102 ever married young women identified from the HDSS database, 2933 of them who were within marriage at the time of data collection were consented and included in the study.
Data Collection
Data were collected through face-to-face interviews by a trained interviewer using a pretested questionnaire. The questionnaire was originally prepared in English and translated into the local language (Afan Oromo). We pretested the questionnaire among young married women who resides in a similar setting outside our study area. Some questions and the translation were refined based on the feedback we obtained during the pre-test. Experienced female data collectors and field supervisors who were able to fluently speak the local language were recruited and trained for 3 days. The training was focused on the content of the questionnaire and on the field data collection procedures. At the household level, the interviewer introduced themselves to eligible participants and interviewed women who consented to participate. The field supervisors closely supervised the data collection process and checked a sample of the filled questionnaire for completeness on a daily basis.
Ethical Approval
This study was conducted following the Declaration of Helsinki. Ethical approval was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of Haramaya University prior to the data collection. Written informed consent was obtained from each study participant. The approval for married study participants less than 18 years to provide written informed consent on their own behalf was given by the IHRERC of Haramaya University.
Variables and Measurements
In this study, unmet need for contraception was the main outcome variable. It was defined as a proportion of young married women who were neither pregnant nor postpartum amenorrhoeic and want to space their next birth at least for 2 years or preferred to stop childbearing but not using contraception; or currently pregnant/postpartum amenorrhea but their current pregnancy/last birth was unwanted or mistimed(want to wait for at least 2 years at that time).2,35 The study participants were asked a series of questions to determine their extent of unmet need for contraception. Those with currently mistimed pregnancy were categorized as had an unmet need for spacing while those who had stopped child bearing but accidentally got the current pregnancy had unmet need for limiting. Young women who were postpartum amenorrhoeic whose last child was mistimed had an unmet need for spacing while those who had stopped childbearing but accidentally got the last child had an unmet need for limiting. Moreover, young women who were neither pregnant nor postpartum amenorrhoeic and expressed desires of having more children but want to wait at least 2 years or not sure when to have the next child and not using contraception had unmet need for spacing while those who declared to have stopped childbearing but not using contraception were considered as had an unmet need for limiting.35 The overall prevalence of unmet needs for contraception was the sum of unmet need for spacing and limiting birth.
We selected relevant independent variables that influence unmet needs based on literature. One of the key factors was self-perceived women’s household decision-making autonomy which was measured using 10 items adapted from literature.36–38 The scale was intended to measure a woman’s influence over a range of key household decisions that affect her own life. We ask women who usually make decisions about how to use money in the household, large household purchases, household purchases for daily needs, when to sell a large asset (e.g. cow), when to sell mall asset (e.g. chicken), when to visit family/relatives, self healthcare and children healthcare, when to have sex, and when to use FP. Item response options included the following: wife alone, wife and husband together, husband alone, respondent and other person, and someone else. For the measure of overall decision-making autonomy, we converted all indicators into binary variables where responses of wife alone or wife and husband together scored as 2 and all other responses scored as 1. The scale score was the sum of item scores divided by the number of items and ranges from 1 to 2. The scale had good reliability scale (Cronbach’s alpha= 0.78) Table 1.
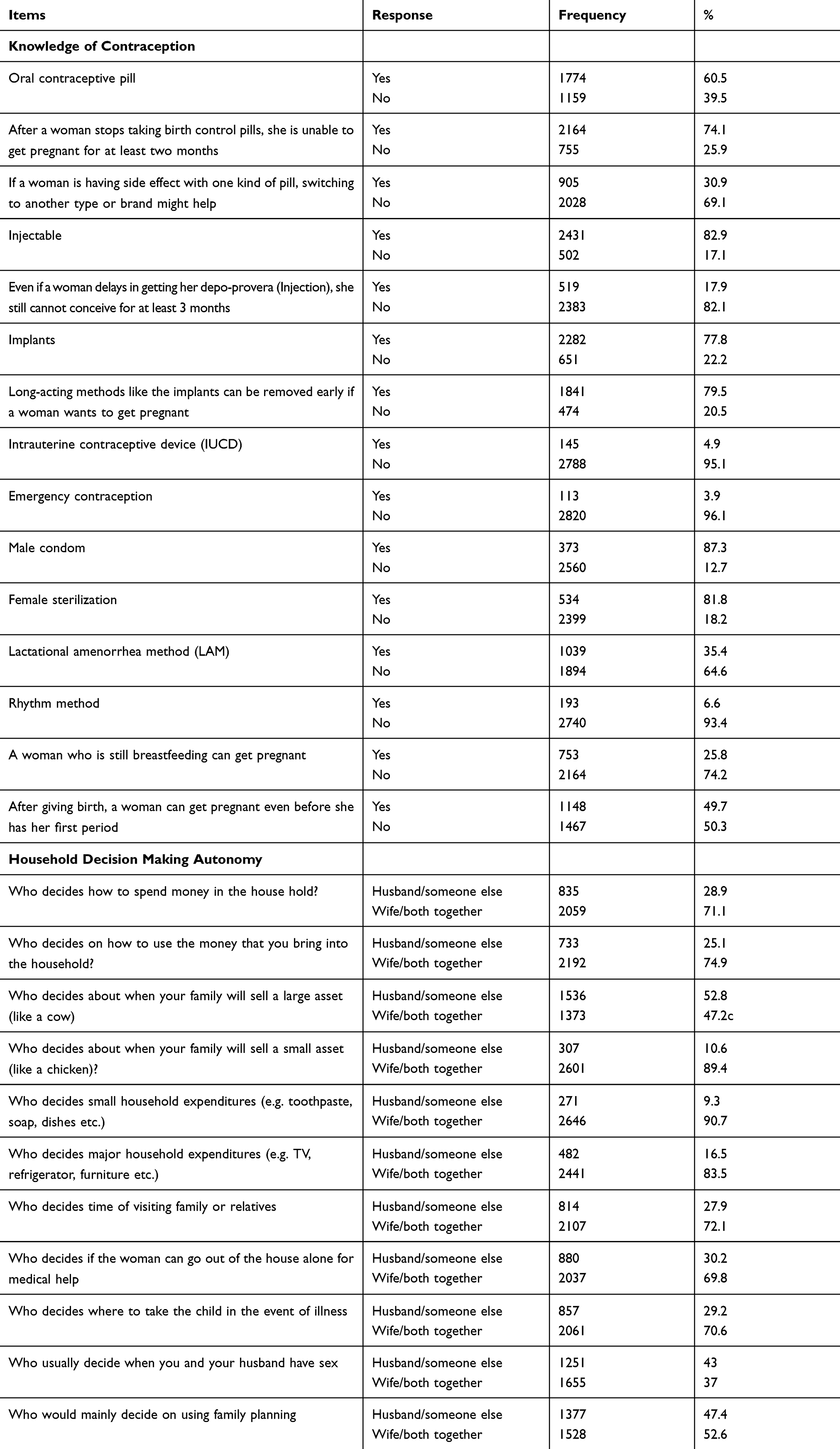 |
Table 1 Knowledge of Contraception and Household Decision-Making Status of Study Participants Living in Kersa HDSS, Ethiopia, 2018 |
Access to family planning (FP) information was another independent variable and measured using seven questions. The questions asked whether she was told about FP during health facility visit; heard FP messages on radio; watched FP messages on TV; told about FP information by Health Extension Worker (HEW) or others Health care Workers (HCWs) at home visits; read about FP on a newspaper or magazine; read FP information in a posters/leaflets; or discussed FP issues at community events/conversations in the last 12 months preceding the survey. Each question was answered as yes or no. Each yes response was recorded as a score of 1 otherwise 0. Thus, the maximum score was 7 and the minimum one was 0. The overall score was categorized into two categories as had access to FP information if a woman got at least a score of 1, yes to at least one of the questions, and had no access if the total score was zero.39
Knowledge of contraception was assessed using a 15-item scale. The responses were scored as “0” for an incorrect answer and “1” for a correct answer. The total score was then obtained by summing all items, which could range from 0 to 15 points and then categorize the score as above and below the median. Those above median scores were classified as high knowledge of contraception and those below median scores were classified as low knowledge of contraception (Table 1).40,41
Wealth index was calculated using the principal component analysis (PCA) method. Items were assessed owing to household facilities including electricity, kerosene, lantern lamp, solar, TV, radio, watch, mobile telephone and possessions such as agricultural land size and the number of animals owned (cows, oxen, goats, sheep, camel, donkey, chickens).42 Five components were extracted based on eigenvalues >1, factor loadings > |0.2|, examination of the scree plots, and the cumulative proportion of variance explained by each component. The first component or factor comprised of several heavily loaded variables and accounted for the largest variation in the data was categorized into quintiles. Each household falls into a category with the lowest score representing the poorest and the medium score and highest representing the richest households.
In addition, we considered age (14–17/18 or more years); type of residence (urban/rural); educational attainment of respondents: no formal education, primary (1–4 grade), lower secondary and higher (>grade 4); husband’s occupation: farmer and other occupation (including government employee, merchants, daily laborer); husband education attainment: no formal education, primary (1–4 grade), lower secondary and higher (>grade 4 years); age of marriage (<18, 18–20, ≥21 years); actual number of children; ideal number of children (≤5 and >5 children); parity (para one or never gave birth/above para one); and history of child/fetal lose (had history of child/fetal lose and had no history of child/fetal loss).
Data Management and Analysis
The completed questionnaires were double entered into EpiData Version 3.1, cleaned, and analyzed using STATA 14 statistical software. The relevant proportions and their 95% confidence intervals were calculated for categorical variables and means were calculated for continuous variables. We examined the associations between unmet needs and each independent variable by calculating the prevalence ratio (PR) using a log-binomial regression model which is preferable for the outcome variable with high prevalence.43 Variables with p-value of ≤0.25 in the bivariate analysis were considered in the multivariable analysis and adjusted PR (APR) along with 95% CIs were estimated and a p-value <0.05 was used to declare the statistical significance. Log-likelihood ratio test and Akaike’s and Bayesian information criterion were used to select the final model. The Pearson Chi-square and Hosmer–Lemeshow goodness-of-fit tests were used to test for model fitness. Multicollinearity between each explanatory variable included was checked by examining the correlation matrix for the regression coefficients and the standard error. Residence and number of alive children were not included in the model due to multicollinearity with husband occupation and parity, respectively.
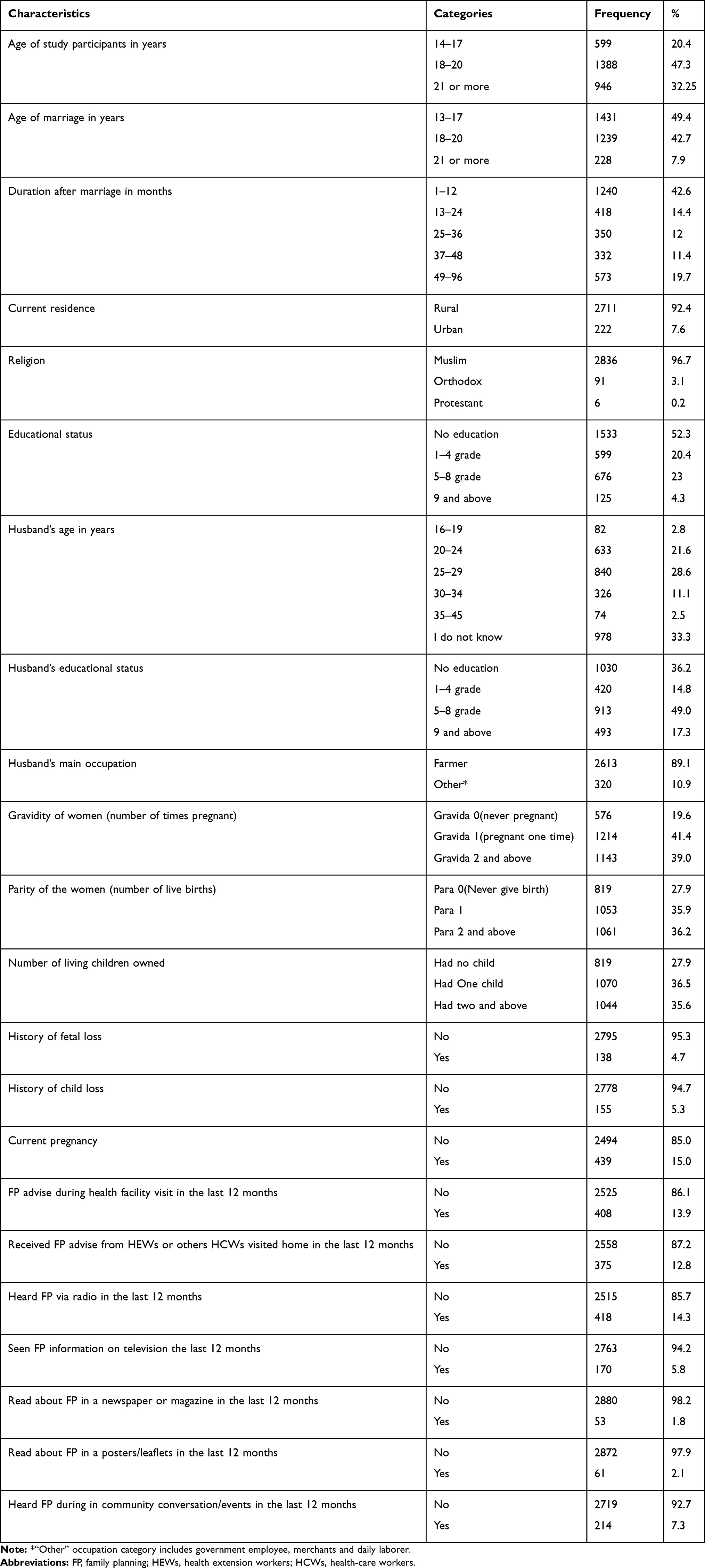 |
Table 2 Background Characteristics of Study Participants Living in Kersa HDSS, Ethiopia, 2018 |
Results
A total of 2933 young married women participated in this study. The majority of the women, 1721 (58.7%), were in the 20–24-year age group with a mean age of 19.4 (±2.5) years. Nearly all, 2741 (94.1%), were 5 years and lesser than 5 years after marriage. More than half, 1533 (52.3%), of the study participants had no education. Most of the study participants were Muslims, 2836 (96.7%), and rural residents, 2711 (92.4%). In terms of reproductive characteristics, 2114 (72.1%) ever gave birth to a child and 1061 (31.2%) had two or more children. One hundred and thirty-eight (4.7%) and 155 (5.3%) women had a history of pregnancy termination and child loss, respectively. The mean ideal number of children among the women was 5.7 children and 439 (15%) were pregnant at the time of the study. Of all study participants, 751 (25.6%) had access to FP information from different sources in the last 12 months prior to the survey Table 2.
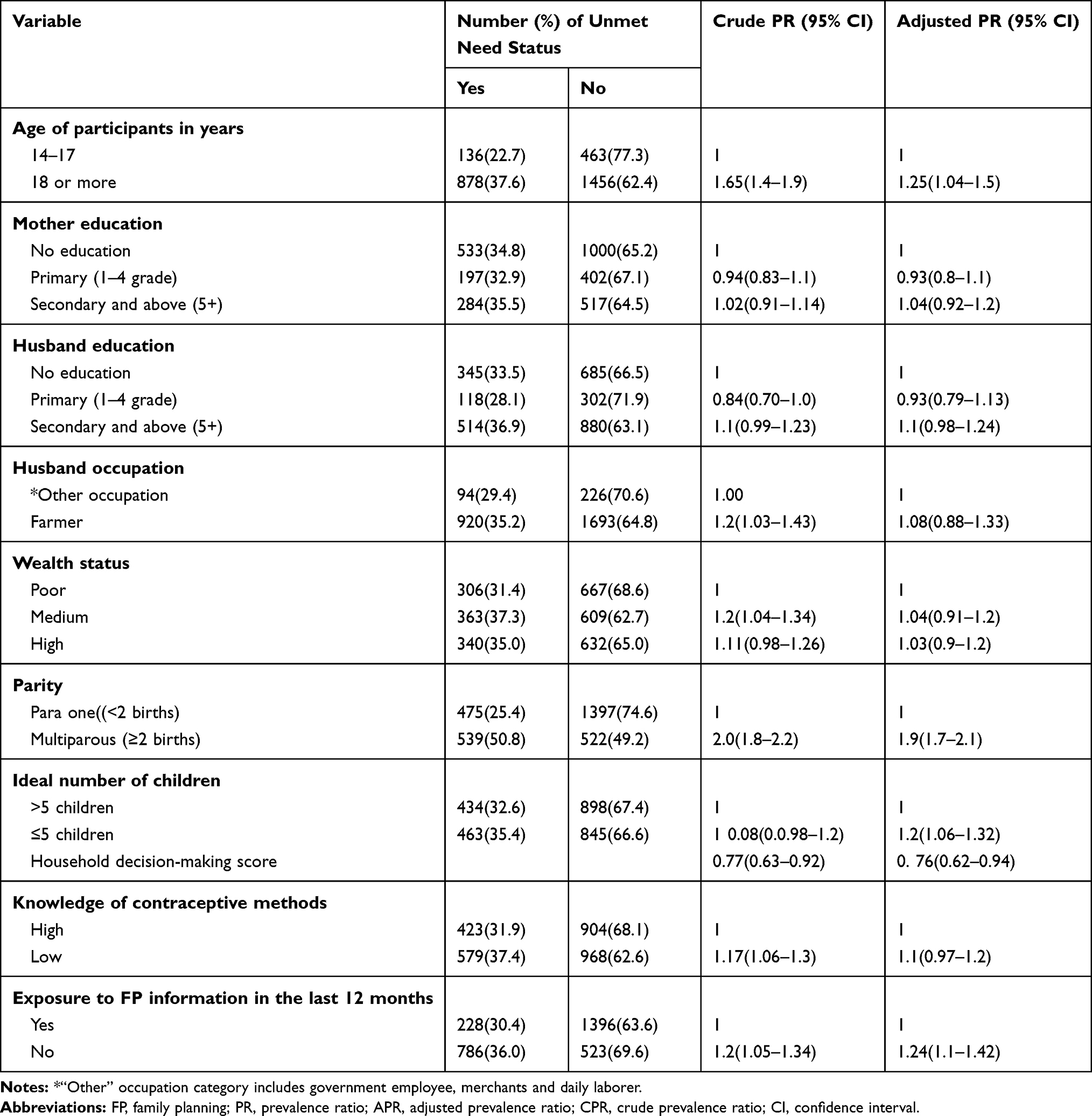 |
Table 3 Factors Associated with Unmet Need for Contraception Among Study Participants Living in Kersa HDSS, Ethiopia, 2018 |
Most of the study participants, 2803 (95.6%), knew at least one contraceptive method. Injectable (82.9%) implants (77.8) and pills (60.5%) were the most commonly known contraceptive methods while only 145 (4.9%) knew intrauterine contraceptive device (IUCD). Moreover, 1074 (37.9%) of the participants had above median household decision-making autonomy score Table 1.
The prevalence of unmet need for contraception among young married women in the study was 1014 (34.6%, 95% CI= 32.9%–36.4%) and nearly all, 978 (96.45%), of them had an unmet need for spacing (Figure 1).
 |
Figure 1 Unmet need for contraception among young married women in Eastern Ethiopia, 2018. |
Factors Associated with Married Young Women Unmet Need for Contraception
After adjusted analysis, the prevalence of unmet need for contraception was lower by 25% (APR= 0. 76; 95% CI: 0.62–0.95) with one unit increase of young married women’s household decision-making autonomy score. The prevalence of unmet need for contraception among young women who had no access to FP information in the last 12 months was 1.24 times higher compared to those who had access to FP information during the specified period (APR= 1.24; 95% CI: 1.1–1.42). The prevalence ratio of unmet need for contraception among young married women aged 18 years or more was also 1.25 times higher compared to those aged below 18 years (APR= 1.25; 95% CI: 1.04–1.5). Furthermore, the prevalence ratio of unmet need for contraception was 1.2 times higher among young married women who reported 5 and lesserideal number of children (APR=1.2; 95% CI: 1.06–1.32) and 1.8 times higher among multiparous women (had two and above birth) compared to women who gave birth once or who never gave birth (APR= 1.9; 95% CI: 1.7–2.1) (Table 3).
Exposure to family planning (FP) information during the last 12 months (APR= 1.24; CI=1.1–1.42), age 18 or more years (APR=1.31; CI=1.07–1.6), multiparty (APR= 1.9; CI=1.7–2.1) and desire to have 5 children or lesser than 5 children (APR= 1.2; CI=1.06–1.32).
Discussions
This study demonstrated that one-third of young married women had an unmet need for contraception. Increased household decision-making autonomy, access to FP information, parity, the number of children desired to have and age were significantly associated with unmet need for contraception.
The 34.6% total unmet need for contraception among young women in our study was far higher than the 20.5% national prevalence2 and 11–20.5% reported among young married women in other developing countries.16,44 Evidence showed a substantial disparity in unmet need by residence while more than 90% of the study participants were rural residents, which might be attributed to the difference with national data. However, it is comparable with a review and study from sub-Saharan African countries that found 21–46% prevalence of unmet need for contraception among 15–24-year-old married women.6,45 These confirm the evidence that showed that most sub-Saharan African countries are far from adequately meeting the needs of contraceptives in their youth population.6 Nearly all (96.45%) of the study participants reported unmet need for spacing which is expected in that younger mothers might have not reached the desired fertility and hence preferred to space childbirths than the limit. About three-fourth (74.3%) of young married women who ever gave more than two live birth were spaced between first and second child 24 months or below which is less than the recommended inter-birth interval. Hence, the high unmet need for contraception in our study mostly attributed to young mothers high intended to space births but not using contraceptive methods which is also indicated in previous literature.46
Increased household decision-making autonomy was significantly associated with a lower prevalence of unmet needs for contraception in line with several previous studies among reproductive-age women.24,25 The consistency with past studies confirms that the hypothesis of women who more involved in household decision-making would be more likely to use health services including family planning. However, many young women in a patriarchal society like Ethiopia, particularly in a rural setting, have lesser decision-making power on major household issues due to economic dependence, lesser negotiation skills, and other existing culture.47 These findings depict the need for strategies that empower young women to develop negotiation skills to choose the number of children they desire and challenge the traditional male dominance that limits their access to contraceptive services.
Qualitative studies suggested the importance of factual information that describes the contraceptive methods for young married women in developing countries since most of them are married at an early age with limited knowledge of contraception.48,49 In line with the previous literature, inaccessibility to FP information was significantly associated with increased prevalence of young married women unmet need for contraception compared to those who had access to FP information. This may be related to less emphasis given to young women in disseminating FP information by health service providers.50,51 This demonstrates the importance of extensive FP information targeting young married women by enhancing high-quality FP counseling at each health service provision junction and through all other promising modalities to reach young women. But the effect of FP information on unmet need needs to be interpreted cautiously. There could be also a reverse causality. Women who decide to adopt contraception are likely to request information from health staff, in which case information is not an influence on, but rather a consequence of, contraceptive use. Since the study is a cross-sectional study, we may not rule out the temporal relationship.
Multiparty was also significantly associated with unmet needs for contraception. The likelihood of the unmet need for contraception was 1.8 times higher among young women who gave birth more than one time compared to those who never gave birth or gave birth only once. The result is consistent with previous findings which indicated a markedly increase of young married women unmet need for contraception with parity.10,13 This would be due to increased young women’s demand for contraception as well as attaining confidence to expose their desire to space pregnancy after confirming their fertility. This is also a signal for enhancing the quality of postpartum contraceptive services among young married women.
The prevalence ratio of unmet need for contraception was 1.2 times higher among young married women reported a desire to have 5 children or lesser than 5 children. This is consistent with previous studies that identified the couple’s desire for children as a dominant factor that shapes their need for contraception.15,16 According to a study conducted in Burkina Faso and Mali, each additional child the married young women desired to have decreased the likelihood of unmet need contraception by 30%.52 Moreover, evidence also showed as younger women had a larger ideal number of children than their adult counterpart due to lower awareness of pregnancy-related challenges and then less likely have demand for contraception.53 This implies that young women’s desire for a large number of children refrain them from the need for contraceptives until they achieved their desired fertility and then lower unmet need for contraception. This highlights the importance of recently married women targeted education that emphasizes the risk of rapid-repeat pregnancy and challenges of large family size.
According to the DHS analytic studies in developing countries, unmet need for contraception was highest among the youngest married women (age 15–16) and declines with increasing age.35,54 Contrary to the previous studies, our study indicated the higher prevalence ratio of unmet need for contraception among married youth above 18 years of age compared to the adolescent age group. The majority of the participants of this study were from the rural settings where adolescent girls are under mounting pressure to conceive immediately after marriage. Thus, younger women had lower demand for contraception which depicts rural married adolescents continuing to comply with the traditional norms that dictate giving birth immediately after marriage. This demonstrates that married adolescents’ continued experiencing complex early age pregnancy’s adverse health consequences such as fistula and other pelvic floor disorder due to immature reproductive organs which were also observed in previous studies in the study area.31,55 This underscores the importance of intensifying education concerning the need to delay childbearing and contraception among adolescents in the study area.
This study has a number of limitations. We found a significant association between lack of exposure to FP information and increased unmet need for contraception. However, providers view concerning young women FP counseling when they come to the health facilities was not considered in this study although evidence indicated as provider related biases hamper young women’s access to contraceptive information and services in sub-Saharan Africa.51 Despite evidence identified considerable disagreement between the couple regarding who exercises more in the household decision-making power,47 husband’s view was not asked in this study. Moreover, responses to the outcome and independent variables measurement might be affected by the recall and social desirability bias.
Conclusions
One-third of married young women had an unmet need for contraception. Household decision-making autonomy and access to FP information were the major factors associated with the young married women unmet need for contraception. More efforts are needed to empower young women to make decisions that affect their own life and also to provide appropriate FP information to reduce the burden of unmet needs among young women in rural settings in Ethiopia. In the future, a longitudinal study is needed to inform a better approach as well as the content and standard of information to be provided for young married women.
Availability of Data
All data analyzed for this article are available with the corresponding author and can be obtained on reasonable request.
Acknowledgments
We would like to thank Haramaya University for funding this study. We extend our gratitude for Addis Continental Institute of Public Health for technical support as well as the study participants and data collectors for their kind cooperation.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Disclosure
No conflict of interest was declared by the authors.
References
1. Digitale J, Psaki S, Soler-Hampejsek E, Mensch BS. Correlates of contraceptive use and health facility choice among young women in Malawi. Ann Am Acad Pol Soc Sci. 2017;669(1):93–124.
2. CSA, ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia: Ethiopiam Central Statistical Agency and ICF International; 2017.
3. United Nations Population Fund (UNFPA). The Status Report on Adolescents and Young People in Sub-Saharan Africa: Opportunities and Challenges. Johannesburg (South Africa): United Nations Population Fund (UNFPA); 2012.
4. Oye-Adeniran BA, Adewole IF, Odeyemi KA, Ekanem EE, Umoh AV. Contraceptive prevalence among young women in Nigeria. J Obstetrics Gynaecol. 2005;25(2):182–185.
5. Hounton S, Barros A, Amouzou A, et al. Patterns and trends of contraceptive use among sexually active adolescents in Burkina Faso, Ethiopia, and Nigeria: evidence from cross-sectional studies. Glob Health Action. 2015. doi:10.3402/gha.v8.29737
6. Prata N, Weidert K, Sreenivas A. Meeting the need: youth and family planning in sub-Saharan Africa. Contraception. 2013;88(1):83–90. doi:10.1016/j.contraception.2012.10.001
7. ALCG F, Souza AI. Unmet contraceptive demand. Revista Brasileira De Saúde Materno Infantil. 2018;18:691–692. doi:10.1590/1806-93042018000400001
8. Bishwajit G, Tang S, Yaya S, Feng Z. Unmet need for contraception and its association with unintended pregnancy in Bangladesh. BMC Pregnancy Childbirth. 2017;17(1):186. doi:10.1186/s12884-017-1379-4
9. Nyarko SH. Unintended pregnancy among pregnant women in Ghana: prevalence and predictors. J Pregnancy. 2019. doi:10.1155/2019/2920491
10. Sengupta R, Das A. Contraceptive practices and unmet need among young currently married rural women in empowered action group (EAG) states of India. J Fam Welf. 2012;58(1):1–13.
11. Mutumba M, Wekesa E, Stephenson R. Community influences on modern contraceptive use among young women in low and middle-income countries: a cross-sectional multi-country analysis. BMC Public Health. 2018. doi:10.1186/s12889-018-5331-y
12. Hussain R, Sedgh G, Ashford LS. Unmet Need for Contraception in Developing Countries: Examining Women’s Reasons for Not Using a Method. New York: Guttmacher Institute; 2016.
13. MacQuarrie KLD Unmet need for family planning among young women: levels and trends. DHS Comparative Reports No.34. ICF International: USA; 2014
14. Haider TL, Sharma M. Barriers to family planning and contraception uptake in sub-Saharan Africa: a systematic review. Int Q Community Health Educ. 2012;33(4):403–413.
15. Nzokirishaka A, Itua I. Determinants of unmet need for family planning among married women of reproductive age in Burundi: a cross-sectional study. Contraception Reprod Med. 2018;3:11.
16. Islam AZ, Mostofa MG, Islam MA. Factors affecting unmet need for contraception among currently married fecund young women in Bangladesh. Eur J Contracept Reprod Health Care. 2016;21(6):443–448.
17. Yadav D, Dhillon P. Assessing the impact of family planning advice on unmet need and contraceptive use among currently married women in Uttar Pradesh, India. PLoS One. 2015;10(3):e0118584–e0118584.
18. Bhusal CK, Bhattarai S. Factors affecting unmet need of family planning among married Tharu women of Dang District, Nepal. Int J Reprod Med. 2018. doi:10.1155/2018/9312687
19. Short SE, Kiros G-E. Husbands, wives, sons, and daughters: fertility preferences and the demand for contraception in Ethiopia. Popul Res Policy Rev. 2002;21(5):377–402.
20. IPPF. Demystifying Data Fact Sheet: Sexual and Reproductive Health of Young Women in Ethiopia. International Planned Parenthood Federation(IPPF). New York: Guttmacher Institute; 2014.
21. Tadele A, Abebaw D, Ali R. Predictors of unmet need for family planning among all women of reproductive age in Ethiopia. Contracept Reprod Med. 2019;4:6. doi:10.1186/s40834-019-0087-z
22. Prusty RK. Use of contraceptives and unmet need for family planning among tribal women in India and selected hilly states. J Health Popul Nutr. 2014;32(2):342–355.
23. Bishwajit G, Yaya S. Domestic violence: a hidden barrier to contraceptive use among women in Nigeria. Open Access J Contraception. 2018;9:21–28.
24. Uddin J, Pulok MH, Sabah MN. Correlates of unmet need for contraception in Bangladesh: does couples’ concordance in household decision making matter? Contraception. 2016;94(1):18–26.
25. Fagbamigbe AF, Afolabi RF, Idemudia ES. Demand and unmet needs of contraception among sexually active in-union women in Nigeria: distribution, associated characteristics, barriers, and program implications. SAGE Open. 2018;8(1):2158244017754023.
26. Edietah EE, Njotang PN, Ajong AB, Essi MJ, Yakum MN, Mbu ER. Contraceptive use and determinants of unmet need for family planning; a cross sectional survey in the North West Region, Cameroon. BMC Women’s Health. 2018;18(171). doi:10.1186/s12905-018-0660-7
27. Tesfaye G, Loxton D, Chojenta C, Assefa N, Smith R. Magnitude, trends and causes of maternal mortality among reproductive aged women in Kersa health and demographic surveillance system, eastern Ethiopia. BMC Women’s Health. 2018;18(198). doi:10.1186/s12905-018-0690-1.
28. Tebekaw Y, Aemro B, Teller C. Prevalence and determinants of unintended childbirth in Ethiopia. BMC Pregnancy Childbirth. 2014;14:326. doi:10.1186/1471-2393-14-326
29. CSA. Ethiopia Mini Demographic and Health Survey 2014 MoH (Ethiopia), Editor. Addis Ababa, Ethiopia: Central Statistical Agency (Ethiopia); 2014.
30. Genet E, Abeje G, Ejigu T. Determinants of unmet need for family planning among currently married women in Dangila town administration, Awi Zone, Amhara regional state; a cross sectional study. Reprod Health. 2015;12:42. doi:10.1186/s12978-015-0038-3
31. Dheresa M, Worku A, Oljira L, Mengiste B, Assefa N, Berhane Y. One in five women suffer from pelvic floor disorders in Kersa district Eastern Ethiopia: a community-based study. BMC Women’s Health. 2018;18:95. doi:10.1186/s12905-018-0585-1
32. Assefa N, Oljira L, Baraki N, et al. HDSS profile: the kersa health and demographic surveillance system. Int J Epidemiol. 2016;45(1):94–101.
33. Zelalem D, Semahegn A, Tesfaye G, Sileshi B. The level and patterns of fertility among women in Kersa Demographic Surveillance and Health Research Center (KDS-HRC) Field site, Kersa District, East Ethiopia. Fertil Res Pract. 2015;1:18. doi:10.1186/s40738-015-0010-5
34. Musa A, Assefa N, Weldegebreal F, Mitiku H, Teklemariam Z. Factor associated with experience of modern contraceptive use before pregnancy among women who gave birth in Kersa HDSS, Ethiopia. BMC Public Health. 2016;16:614. doi:10.1186/s12889-016-3292-6
35. Bradley SEK, Croft TN, Fishel JD, Westoff. CF. Revising Unmet Need for Family Planning DHS Analytical Studies No. 25. Calverton, Maryland, USA: ICF International; 2012.
36. Hameed W, Azmat SK, Ali M, et al. Women’s empowerment and contraceptive use: the role of independent versus couples’ decision-making, from a lower middle income country perspective. PLoS One. 2014;9(8):e104633.
37. CARE USA. Women’s Empowerment Multidimensional Evaluation of Agency, Social Capital and Relations(WEMEASR): A Tool to Measure women’s empowerment in Sexual, Reproductive and Maternal Health Programs: A tool to measure women’s empowerment in sexual, reproductive and maternal health programs Author. Atlanta, GA: Cooperative for Assistance and Relief Everywhere, Inc. (CARE); 2014.
38. Haque SE, Rahman M, Mostofa MG, Zahan MS. Reproductive health care utilization among young mothers in Bangladesh: does autonomy matter? Women’s Health Issues. 2012;22(2):e171–e180.
39. Oluwasanu MM, John-Akinola YO, Desmennu AT, Oladunni O, Adebowale AS. Access to Information on family planning and use of modern contraceptives among married Igbo women in Southeast, Nigeria. Int Q Community Health Educ. 2019;39(4):233–243.
40. Kaye K, Suellentrop K, Sloup C. The Fog Zone: How Misperceptions, Magical Thinking, and Ambivalence Put Young Adults at Risk for Unplanned Pregnancy. Washington, DC: The National Campaign to Prevent Teen and Unplanned Pregnancy; 2009.
41. Mon MM, Liabsuetrakul T. Predictors of contraceptive use among married youths and their husbands in a rural area of Myanmar. Asia Pac J Public Health. 2012;24(1):151–160.
42. Balen J, McManus DP, Li Y-S, et al. Comparison of two approaches for measuring household wealth via an asset-based index in rural and peri-urban settings of Hunan province, China. Emerg Themes Epidemiol. 2010;7:7. doi:10.1186/1742-7622-7-7
43. Martinez BAF, Leotti VB, GdSE S, Nunes LN, Machado G, Corbellini LG. Odds ratio or prevalence ratio? An overview of reported statistical methods and appropriateness of interpretations in cross-sectional studies with dichotomous outcomes in veterinary medicine. Front Vet Sci. 2017;4:193. doi:10.3389/fvets.2017.00193
44. Sinai I, Nyenwa J, Oguntunde O. Programmatic implications of unmet need for contraception among men and young married women in northern Nigeria. Open Access J Contraception. 2018;9:81–90.
45. Atchison CJ, Cresswell JA, Kapiga S, et al. Sexuality, fertility and family planning characteristics of married women aged 15 to 19 years in Ethiopia, Nigeria and Tanzania: a comparative analysis of cross-sectional data. Reprod Health. 2019;16:6. doi:10.1186/s12978-019-0666-0
46. Juarez F, Gayet C, Mejia-Pailles G. Factors associated with unmet need for contraception in Mexico: evidence from the National survey of demographic dynamics 2014. BMC Public Health. 2018;18(1):546. doi:10.1186/s12889-018-5439-0
47. Uddin J, MZ H, Pulok MH. Couple’s concordance and discordance in household decision-making and married women’s use of modern contraceptives in Bangladesh. BMC Women’s Health. 2017;17:107. doi:10.1186/s12905-017-0462-3
48. Marshall C, Kandahari N, Raine-Bennett T. Exploring young women’s decisional needs for contraceptive method choice: a qualitative study. Contraception. 2018;97(3):243–248. doi:10.1016/j.contraception.2017.10.004
49. Cornet A. Current challenges in contraception in adolescents and young women. Curr Opin Obstet Gynecol. 2013;25(Suppl 2):S1–S10. doi:10.1097/GCO.0b013e32835e06fd
50. Schwandt HM, IS S, Corroon M. Contraceptive service provider imposed restrictions to contraceptive access in urban Nigeria. BMC Health Serv Res. 2017;17:268. doi:10.1186/s12913-017-2233-0
51. Sidze EM, Lardoux S, Speizer IS, Faye CM, Mutua MM, Badji F. Young women’s access to and use of contraceptives: the role of providers’ restrictions in urban Senegal. Int Perspect Sex Reprod Health. 2014;40(4):176–183. doi:10.1363/4017614
52. O’Regan A, Thompson G. Indicators of young women’s modern contraceptive use in Burkina Faso and mali from demographic and health survey data. Contraception Reprod Med. 2017;2:26. doi:10.1186/s40834-017-0053-6
53. Wulifan JK, Mazalale J, Kambala C, et al. Prevalence and determinants of unmet need for family planning among married women in Ghana-a multinomial logistic regression analysis of the GDHS, 2014. Contraception Reprod Med. 2019;4:2. doi:10.1186/s40834-018-0083-8
54. Islam AZ, Rahman M, Mostofa MG. Association between contraceptive use and socio-demographic factors of young fecund women in Bangladesh. Sexual Reprod Healthcare. 2017;13:7. doi:10.1016/j.srhc.2017.05.001
55. Dheresa M, Worku A, Oljira L, Mengistie B, Assefa N, Berhane Y. Factors associated with pelvic floor disorders in Kersa District, eastern Ethiopia: a community-based study. Int Urogynecol J. 2018. doi:10.1007/s00192-018-3776-2
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.