Back to Journals » Clinical Interventions in Aging » Volume 12
Understanding institutional stakeholders’ perspectives on multidrug-resistant bacterial organism at the end of life: a qualitative study
Authors Heckel M ![]() , Herbst FA
, Herbst FA ![]() , Adelhardt T, Tiedtke JM, Sturm A, Stiel S, Ostgathe C
, Adelhardt T, Tiedtke JM, Sturm A, Stiel S, Ostgathe C
Received 30 March 2017
Accepted for publication 15 July 2017
Published 3 October 2017 Volume 2017:12 Pages 1605—1613
DOI https://doi.org/10.2147/CIA.S138429
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Maria Heckel,1 Franziska A Herbst,2 Thomas Adelhardt,3 Johanna M Tiedtke,4 Alexander Sturm,5 Stephanie Stiel,2 Christoph Ostgathe1
1Department of Palliative Medicine, Comprehensive Cancer Center Erlangen-EMN, Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Universitätsklinikum Erlangen, Bavaria, Germany; 2Institute for General Practice, Hannover Medical School, Hannover, Germany; 3Division of Health Management, School of Business and Economics, Institute of Management (IFM), Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Bavaria, Germany; 4Institute of Psychogerontology, Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Bavaria, Germany; 5Department of General Internal and Geriatric Medicine, Institute for Biomedicine of Aging, Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Hospital of the Order of St John of God Regensburg, Bavaria, Germany
Background: Information lacks about institutional stakeholders’ perspectives on management approaches of multidrug-resistant bacterial organism in end-of-life situations. The term “institutional stakeholder” includes persons in leading positions with responsibility in hospitals’ multidrug-resistant bacterial organism management. They have great influence on how strategies on multidrug-resistant bacterial organism management approaches in institutions of the public health system are designed. This study targeted institutional stakeholders’ individual perspectives on multidrug-resistant bacterial organism colonization or infection and isolation measures at the end of life.
Methods: Between March and December 2014, institutional stakeholders of two study centers, a German palliative care unit and a geriatric ward, were queried in semistructured interviews. Interviews were audiotaped, transcribed verbatim, and analyzed qualitatively with the aid of the software MAXQDA for qualitative data analysis using principles of Grounded Theory. In addition, two external stakeholders were interviewed to enrich data.
Results: Key issues addressed by institutional stakeholders (N=18) were the relevance of multidrug-resistant bacterial organism in palliative and geriatric care, contradictions between hygiene principles and patients’ and family caregivers’ needs and divergence from standards, frame conditions, and reflections on standardization of multidrug-resistant bacterial organism end-of-life care procedures. Results show that institutional stakeholders face a dilemma between their responsibility in protecting third persons and ensuring patients’ quality of life. Until further empirical evidence establishes a clear multidrug-resistant bacterial organism management approach in end-of-life care, stakeholders suggest a case-based approach.
Conclusion: The institutional stakeholders’ perspectives and their suggestion of a case-based approach advance the development process of a patient-, family-, staff-, and institutional-centered approach of how to deal with multidrug-resistant bacterial organism-positive patients in end-of-life care. Institutional stakeholders play an important role in the implementation of recommendations following this approach.
Keywords: hygiene measures, hygiene procedures, management approach, geriatric care, palliative care, end-of-life care, terminal illness, comorbidity
Plain language summary
The study assessed institutional stakeholders’ perspectives on management approaches of multidrug-resistant bacterial organism in end-of-life situations.
Researchers interviewed institutional stakeholders who are in leading positions and responsible for their institutions’ multidrug-resistant bacterial organism management.
Institutional stakeholders think that multidrug-resistant bacterial organisms are a relevant issue in end-of-life care. Institutional stakeholders face a dilemma between their responsibility in protecting third persons and ensuring patients’ quality of life. Until further empirical evidence establishes a clear multidrug-resistant bacterial organism management approach in end-of-life care, stakeholders suggest a case-based approach.
Background
The management of multidrug-resistant bacterial organisms (MDROs) is an important public health issue. Limited information is available on specific strategies for patients in end-of-life care infected or colonized with MDROs, such as methicillin-resistant Staphylococcus aureus (MRSA) and multidrug-resistant gram-negative bacteria. A recent analysis of written documents on MDRO management in two hospitals reveals that in these institutions the end-of-life situation is not considered in particular in internal guidelines and informational material; only few documents mention MDRO in patients at the end of life.1 This is in contrast to the fact that the vast majority of these patients are at risk for MRSA or other MDRO. MRSA colonization rates reported in other studies were between 3% and 11.6% of positive MRSA swabs in hospice patients and patients in palliative care settings in Saudi Arabia,2 England,3,4 Ireland,5 and Germany.6 Up to now, the number of patients with MDRO other than MRSA is unknown. In a survey at our institution, which will be published elsewhere, the rate for other MDRO equaled the rate for MRSA. Prevalence rates for patients in geriatric clinics vary: 9.4% (MRSA),7 22.7% (MDRO),7 22.2% (MRSA),8 and 32.6% (MDRO).9 It is difficult to compare the prevalence rates because of different study designs (analysis approaches, populations, and settings). Studies on MRSA management strategies of palliative care units and hospices were conducted by Dand et al10 in southern England and Bükki et al11 in Germany. In both surveys, most institutions had formal MRSA protocols (95% out of n=57 institutions in southern England and 91% out of n=229 institutions in Germany). Infection control precautions and the restriction of MRSA-positive patients’ activities varied between the institutions. Participants had diverse opinions on the negative impact of MRSA protocols on patients’ quality of life.10,11 The German national “Recommendations for prevention and control of MRSA in medical and nursing facilities” dictate routine standard hygiene precautions intended to prevent MRSA transmission, such as the adherence to hand hygiene.12 Using risk analysis in medical and nursing facilities, decisions on contact precautions and barrier nursing techniques will be made. Barrier protective measures, that is, personal protective equipment and single room isolation, are required in the local written guidelines of the examined institutions. These measures might preclude patients’ social inclusion and preclude maintaining rapport at their end of life.
The study at hand is part of an interdisciplinary cooperation project (M-EndoL, Federal Ministry of Education and Research 01GY1314) that developed a patient-, family-, and staff-centered approach of how to deal with MDRO-positive hospitalized patients during their last phase of life in geriatric and palliative care. Institutional stakeholders considerably influence decisions on procedures regarding MDRO patients at the end of life. Therefore, it is important to examine their perspectives as they have great influence and responsibility on the design of institutional MDRO management strategies. For implementation, key stakeholders’ intentions, interests, resources, and the aspects they consider in decision-making are important to assess. It can be assumed that key stakeholders with significant influence on management decisions have their own opinion on how to handle MDRO in end-of-life care shaped by their professional function and personal background. The term “institutional stakeholder” as used in this article pertains to persons in leading positions with responsibility in MDRO management who have significant influence upon or importance within the organization. This includes persons responsible for public infection prevention and control, nurse managers, senior consultants, and hospital hygiene specialists.
This ancillary study targeted institutional stakeholders’ individual and professional perspectives on MDRO colonization or infection and isolation measures at the end of life and generate knowledge for developing recommendations on dealing with MDROs in end-of-life care and its implementation.
Methods
A key stakeholder analysis13,14 was conducted using semistructured in-depth interviews on the relevance and management of MDRO in end-of-life care and Grounded Theory15,16 for data analysis. The study report follows the consolidated criteria for reporting qualitative studies.17
Study plan and participant recruitment
The project group collected names and positions of all institutional key stakeholders in leading positions with responsibility in MDRO management of the two study centers – a German palliative care unit and a geriatric ward. Between March and December 2014, potential participants were purposefully sampled regarding gender, position, and years of employment, and personally invited by telephone call or email for study participation. Interview participants were asked if they knew other potential participants inside and outside the institutions. Those announcements did not lead to additional stakeholders of the participating institutions but to the inclusion of the two external stakeholders to validate the gathered information from internal stakeholders and enrich data.
The palliative care unit held six single and two double rooms and had no negative pressure isolation rooms. The single rooms had mantraps where staff members and visitors can disinfect their hands and put on protective clothing. The geriatric department was organized into wards. Geriatric patients were treated from admission to discharge including postsurgery and internal medicine as well as a specialized geriatric rehabilitation. A total of 90 beds were available in 12 single-bedded, 30 double-bedded, and 6 triple-bedded rooms. All rooms could be used for patient isolation. Trollies fitted with protective equipment were provided to enable fulfillment of hygiene precautions. The MDRO policies of both study centers varied slightly. Single-room accommodation for patients with MDRO infection or colonization is standard; the door has to stay closed and flagged with a sign. Alongside hand hygiene, personal protective equipment (including protective clothing, cap, and filtering facepiece respirators) is required for staff members (medical, nursing, and therapeutic) and visitors. The palliative care unit, which was located in the hospital campus as a separate ward, established divergent rules concerning protective measures: Visitors and staff members were allowed to enter the room without personal protective equipment for social contacts. By comparison, the geriatric wards were located in different houses. In both study centers, staff members were obliged to wear protective clothing if they had physical contact during medical or nursing tasks, for example, wound treatment.
Interviews took place in the institutional stakeholders’ offices or other places they preferred, such as seminar and meeting rooms.
Data collection
For the face-to-face interviews, a semistructured interview guideline on institutional stakeholders’ perspectives on MDRO management in end-of-life care was used (Table 1). Sociodemographic data about the participants, for example, gender, position, and years of employment, were assessed. The interviewer was TA, a junior researcher in health management and scientific staff member of the consortium project. He conducted the interviews after completing an interview training. No relationship had been established to the participants prior to study commencement. The participants knew TA’s occupational background, the overall aim of the consortium project, and the goals of the ancillary study. All interviews were digitally recorded and transcribed verbatim for further data processing and analysis. The interviewer took field notes during and after the interview. The following project phase stipulated focus groups that gave the possibility to clarify and add to previous findings.
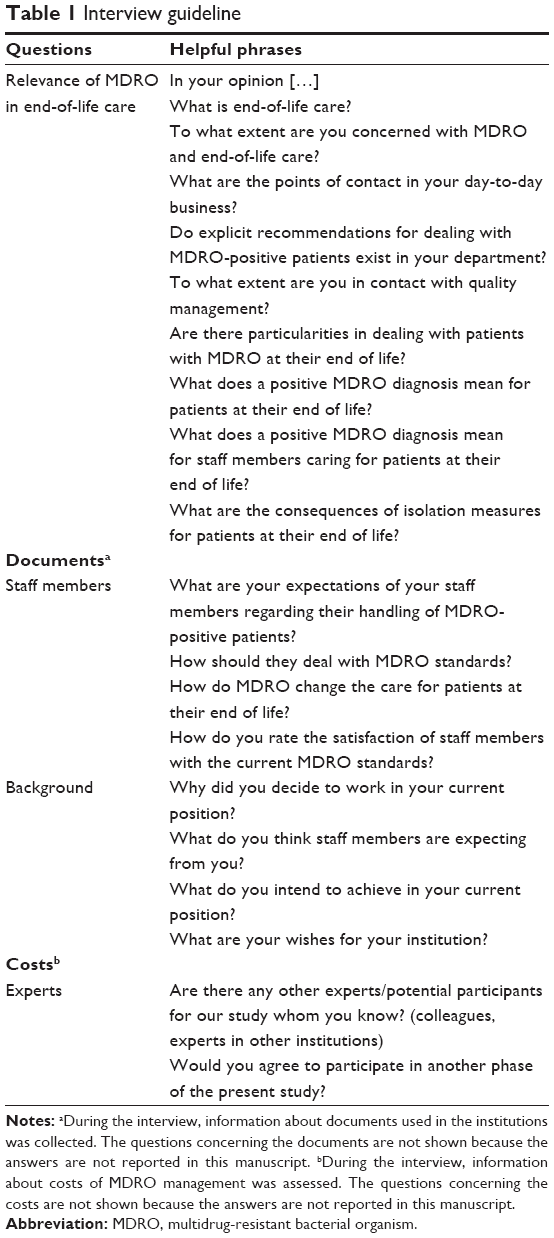 | Table 1 Interview guideline |
Data analysis
The interviews were analyzed qualitatively according to the principles of Grounded Theory15,16 using the software MAXQDA18 for data management, coding, and analysis. The data analysis was performed by junior researchers who were staff members of the consortium project with different professional backgrounds such as psychology, health and care science, health management, and medical anthropology. They perceived training in qualitative data analysis and were supervised by senior researchers (psychologist and physicians) of the project group. Grounded Theory aims at generating a theoretical framework. The methodological procedure follows a bottom-up analysis technique. Single-text phrases (so-called codes) were coded systematically, and similar codes were summarized into more superior concepts. Finally, on the highest level of abstraction, overall categories were produced inductively. Interviews were first coded independently by two trained researchers. Then coding conflicts were resolved. A third researcher reviewed consistency and precision of codes, concepts, and categories. As soon as data saturation was reached in the analysis, that is, additional interviews did not generate new codes, the recruitment procedure was stopped.
Ethics approval and consent to participate
The present study was approved by the local ethics committees (Ethics Committee of the Medical Faculty in Erlangen: 302_13 B, 15.01.2014; Institutional Review Board Regensburg) and the responsible data protection supervisors. All participants gave informed written consent for study participation. All data were saved in a depersonalized manner.
Results
Study sample and study-related information
Seventeen interviews took place at the study centers. No potential participant declined participation. In one of the interviews, two persons were queried. Nonparticipants were not present during the interviews and no repeat interviews were carried out. Participants (n=18) had leading positions in the fields of clinic, nursing, hygiene, infection control, administration, and management. They worked in their current positions between 1 and 25 years (average 8 years, n=16; 2 missing). Six of them were female and twelve were male. Two further interviews were conducted with stakeholders from external institutions who are responsible for public infection prevention and control and hospital hygiene. These two interviews were summarized and results are presented at the last paragraph of the Results section.
The mean duration of the interviews was 36.2 minutes (range 16–63 minutes; n=17).
Findings from coding analysis
The present article provides insights into key issues arising from the interviews. Key issues were 1) the relevance of MDRO in palliative and geriatric care, 2) contradictions between hygiene principles required in the local written guidelines of the examined institutions and patients’ and family caregivers’ needs and divergence from the standards, 3) frame conditions, and 4) reflections on standardization of MDRO end-of-life care procedures.
Relevance of MDRO in palliative and geriatric end-of-life care
Institutional stakeholders defined end-of-life care from caring for patients who are expected to die at the hospital in the upcoming weeks and days to caring for patients who are diagnosed with a life-limiting disease without further consideration of the time of death. The participants agree on “the complexity and difficulty to predict when the end of life will occur” [S1]. Institutional stakeholders judge the relevance of MDRO in end-of-life care:
Simultaneously, [on the geriatric ward] we take care of aged individuals who have comorbidities. In addition to their chronic diseases, they usually develop a further acute event. This is why they come see us. Due to this, we usually have a group who is at their end of life, irrespective of their infection. […] This means we have two issues: a disproportionate high number of persons who are palliative care patients according to the widely accepted definition. And second, because of the characteristics of the referring institution [ie institutions with high MDRO prevalence such as nursing homes] there is a disproportionately high number of persons who have problem germs. [S10]
Participants argue that patients at their end of life face a complex situation that is determined by a life-limiting disease, symptom burden, and social needs, and that they require holistic care other than curative therapeutic goals. “There are issues such as talking to the family, relationships, interpersonal closeness and so forth that play a completely different role [at the end of life]” [S1]. MDRO and the protective measures are considered to add to the complexity of the patients’ situation and “to be a huge strain as social rapport changes due to isolation” [S11]. The particularity of the patients’ situation at their end of life is that they are at risk not to be discharged from the hospital but to die there. Palliative care and geriatric care, hence, aim according to institutional stakeholders’ statements “to give the family the opportunity to bid farewell soundly” [S6] and “to make life as comfortable as possible for the patient in the remaining time he/she has left” [S6].
Contradictions between institutional hygiene principles required in the local written guidelines of the examined institutions and patients’ and family caregivers’ needs and divergence from the standards
Most institutional stakeholders realize a connection between hygiene standards required in the local written guidelines of the examined institutions and patients’ and family caregivers’ burden because of contact precautions:
There is a big discrepancy if you think of an end-of-life patient who is supposed to receive special care from a palliative care and hospice point of view. Thus, from the perspective of the hygiene management we want stricter isolation measures without any trade-offs. On the other hand, however, we also want that institutions provide the best care. [S5]
However, some institutional stakeholders do not consider it possible to diverge from the standards, not even in end-of-life situations:
Yes, I think we [hospital hygiene] might have adopted a different point of view. We don’t refer to a single patient but to the source of the infection. The MDRO patient is the source of infection. Our approach is to prevent that the infection gets spread on other patients. And we can’t consider the condition of this source. [S8]
Some try to strike a balance between responsible protection of third persons and comfort of the patient at the end of life:
To me it is important that everyone sticks to the isolation measures which are based on scientific findings. I think that every infection that results from carelessness is an infection too many. Especially if you see the consequences resulting from these germs. [S11]
The following solution for resolving the dilemma in end-of-life care was proposed: “I would suggest solely doing the absolutely essential hygiene measures and not everything possible” [S11]. Further, a balancing of the individual patients’ quality of life and the protection of third parties from MDRO was recommended:
Nevertheless, we have to develop [measures] in order to protect the individual patient and to ensure his quality of life, and at the same time we have to protect the entire group. This would be the best possible. [S1]
Concerning practical issues of caring for patients at the end of life, stakeholders articulated two different approaches. First, some see easily realizable possibilities to stay in touch with patients even when following MDRO protocols:
You can definitely bring together symptom control, conversations, communication, even in isolated patients. There might be fewer conversations and conversations might be shorter, for example, if you’re out in the hallway, then you might just open the door and ask, ‘Do you need anything?’ You might do this less with infected patients. And sometimes I open the door but just don’t get too close to the bed. [S7]
Second, others state that isolation measures could be adapted to the situation if common decision-making is possible: “This is what the daily life looks like and how can we facilitate it? What can we open [ie, reduction of isolation measures] to ensure a good end of life”. [S2]
Frame conditions
Stakeholders refer to different frame conditions that must be considered in order to decide whether or not to adapt isolation measures in the end-of-life context (Table 2). These conditions are considered to be vital for decision-making. Stakeholders suggest incorporating staff and family members’ perspectives in the decision-making process in the palliative care unit and the geriatric ward.
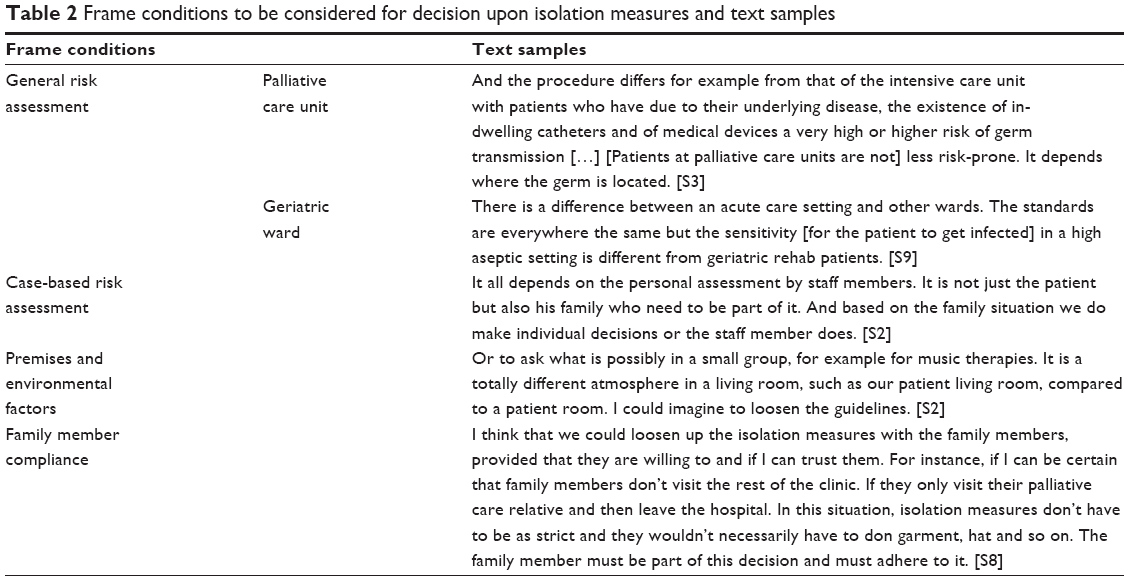 | Table 2 Frame conditions to be considered for decision upon isolation measures and text samples |
Reflections on standardization of MDRO end-of-life care procedures
Stakeholders reflect on whether standardization of MDRO end-of-life care procedures is necessary and can satisfactorily be performed. An affirmative argument is the improvement of confidence in dealing with MDRO patients:
It is important to ensure standardization. The professional treatment of the issue has positive consequences on employee satisfaction. I think they feel more secure when they have clear instructions for practice, when things go smoothly, when there is an expert […] who has the central responsibility for this issue. [S6]
But stakeholders also describe difficulties in defining a standard:
This is exactly what I talked about earlier. Nursing staff approaches me with individual situations and questions. I think it is possible, yes, but difficult in some cases […]. It is difficult to agree on and define guidelines. [S2]
And they deliberate about whether it is necessary to establish a rigid written standard because the perspective on the individual patient is of utmost importance to them:
There is a whole lot that can be written down in guidelines, in standards, nursing standards, hygiene standards, hygiene recommendations, but we still deal with human beings and sometimes I rather get a phone call of someone asking me: ‘How can I handle this situation correctly?’ instead of adhering to the guidelines. [S2]
Additionally, stakeholders emphasize the importance of taking into account staff members’ views and needs. One stakeholder suggests granting a certain freedom in decision-making and acting to staff members:
I expect every staff member to decide for themselves if they want to adhere to the strict measures suggested by the clinic or if the staff member makes a personal decision based on his expectations and needs. I don’t want to be a supervisor who imposes strict rules. I can only give incentives but in the end it is up to the staff member. We have many staff members with little children or who have chronically ill parents at home. And I am sure they view this topic from a different perspective than I do. So I don’t want to pressure any of my staff members. [S4]
Generally, the stakeholders consent that all patients should be cared for equally:
My main goal is to ensure that staff members enter this room just as any other room. And not just one, the assistant, and the rest is waiting in front of the door. Everybody should take a look at the patient, introduce themselves and spend just as much time with the patient as with any other. […] And that they receive the same kind of care as any other patients who are not infected. My task is to ensure this. [S12]
The interviews with the external stakeholders confirm the relevance of the key issues presented above, not adding further major aspects. One interviewee emphasizes that case-based risk assessment is essential and conforms to official guidelines. The other interviewee goes one step further, stating that there is no need for specific MDRO hygiene measures, but the practiced standard hygiene provides sufficient protection – also for staff members.
Theoretical framework
The analysis of face-to-face interviews results in the following theoretical framework (Figure 1). Institutional stakeholders agreed that the management of MDRO is highly relevant in palliative and geriatric care contexts. They face a dilemma between their responsibility in protecting third persons on the one hand and ensuring the patients’ quality of life on the other hand. When trying to resolve the dilemma, institutional stakeholders deliberate about practical and theoretical solutions. Practical solutions are valuable for the clinical setting and aim to support rapport and avoid patients’ social isolation. Adhering to the common hygiene standards and finding possibilities to stay in touch with the patient, nevertheless, contrast the suggestion to adapt protection and isolation measures for patients and their family caregivers in end-of-life situations. Institutional stakeholders mention frame conditions that must be fulfilled in case of adaption. From a theoretical point of view two approaches appear: first, divergences from the general standards are allowed for or a particular end-of-life standard is determined. Designing a particular standard is considered a challenging task. Second, until an empirically based solution, which also takes into account patients’, family caregivers’, and staff members’ perspectives, is found, institutional stakeholders, despite a lack of perfect consent, agree that a case-based approach would be the most acceptable.
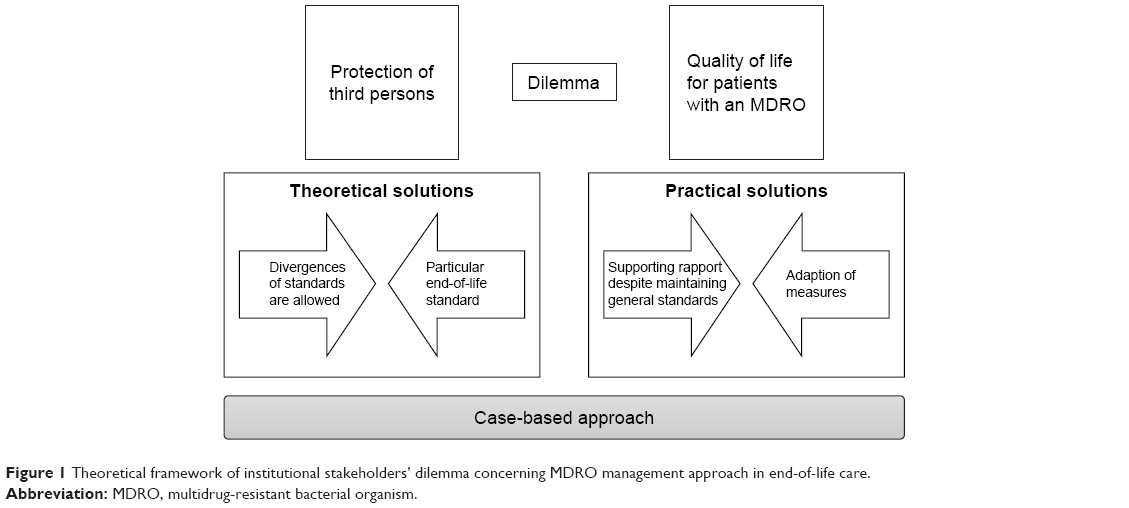 | Figure 1 Theoretical framework of institutional stakeholders’ dilemma concerning MDRO management approach in end-of-life care. |
Discussion
To the best of our knowledge, this is the first study focusing on institutional stakeholders’ perspectives on MDRO in patients in an end-of-life situation. Results presented in this paper allude to the relevance and management of MDRO in geriatric and palliative care.
The interviews furthered a better understanding of institutional stakeholders’ perspectives. Data demonstrate that decision-making in the field of MDRO at the end of life requires thorough consideration of sometimes contradictory hygiene measures and patients’, family caregivers’, and staff members’ needs in the individual situation. In addition, institutional stakeholders must have an overview of the larger organizational context19 and consider staff members’ needs.20 In a recent study, palliative care and hospice staff assess the strict application of MDRO protocols and infection control precautions to be in conflict with the comprehensive palliative care approach.11 Stakeholders in the study presented in this article apprehended this conflict of interest.
Stakeholders suggest different approaches, although they mentioned similar key issues: the relevance of MDRO, contradictions between hygiene requirements and end-of-life care, frame conditions, and standardization of MDRO end-of-life care procedures.
However, institutional stakeholders had diverse ideas concerning standardization and long for further empirical evidence in order to decide on the specificities of implementation of an MDRO management approach in end-of-life care. A possible solution could be to define a particular standard for end-of-life situations that allows for the consideration of the individual situation for which a general standard leaves little scope. A first step to establish a particular standard could be the development of empirically based recommendations on dealing with MDRO in end-of-life care. The empirical basis ensures that patients’, families’, and staff members’ perspectives are included in the recommendations. Following the evaluation of the implemented recommendations, the long-term objective could be the implementation of broader guidelines on MDRO in end-of-life care according to the guidelines for long-term care settings21,22 and the national guidelines for medical and nursing facilities.12
Limitations
This study is constrained by the limitations inherent in qualitative research. Transferability of findings to other public health settings is limited because data were collected from two study centers: a palliative care unit and a geriatric ward. The generalization of the results to other palliative care and geriatric units is limited because of the diversity of MDRO protocols in Germany. This explorative study, nevertheless, emphasizes the need for ongoing discussion and further research on dealing with MDRO in end-of-life care.
During the study, we were faced with the problem of varying definitions of “end-of-life care,” and we solved the problem by asking participants to explicate their own definitions.
Further areas of research
Future studies on institutional stakeholder perspectives are necessary to evaluate the effect of structural differences between patients at their end of life who stay at a particular palliative or geriatric ward and patients at their end of life who stay at an acute care ward or in an outpatient care setting. Implications for the development of recommendations on dealing with MDRO in end-of-life care should be examined. It will be an issue of future research to determine drawbacks and factors for implementation of the recommendations as well as develop a new approach for dealing with MDRO in end-of-life care in the sense of change management.
Conclusion
The assessment of institutional stakeholders’ perspectives on MDRO at the end of life enriches the development process of a patient-, family-, staff-, and institutional-centered approach that integrates the views of four different target groups. Institutional stakeholders will be responsible for the implementation of recommendations following this approach. Therefore, key institutional stakeholders bear an interface function between research and the clinical implementation of results.
Acknowledgments
We gratefully thank all institutional stakeholders for their participation in this study. We acknowledge all team members of the parent study group – Oliver Schöffski (Division of Health Management, Friedrich-Alexander-Universität Erlangen-Nürnberg [FAU]), Frieder R Lang (Institute of Psychogerontology, Friedrich-Alexander-Universität Erlangen-Nürnberg [FAU]), Cornel Sieber (Institute for Biomedicine of Aging [IBA], Friedrich-Alexander-Universität Erlangen-Nürnberg [FAU]; Department of General Internal and Geriatric Medicine, Hospital of the Order of St John of God Regensburg), and Christian Bogdan (Microbiology Institute, University Hospital Erlangen). They were contributors to research conception and design.
The presented study was part of the project “M-EndoL – MRSA in end-of-life care,” which was conducted with generous financial support from the German Federal Ministry of Education and Research (BMBF).
Author contributions
TA designed the interview guide and conducted the interviews. MH, FAH, TA, JMT, AS, and SS analyzed the data. CO and SS designed the study, obtained funding, and provided guidance regarding the general direction of the study and the manuscript. MH wrote the manuscript with primary responsibility. FAH was a key contributor in writing the manuscript. TA, JMT, AS, SS, and CO revised the draft manuscript. All authors read and approved the final manuscript for submission.
The present work was performed in partial fulfillment of the requirements for obtaining the degree “Dr rer. biol. hum.” for the first author MH.
Disclosure
The authors report no conflicts of interest in this work.
References
Adelhardt T, Heckel M, Stiel S, Ostgathe C, Schöffski O. MRE-Kolonisation oder-Infektion in der Versorgung von Menschen am Lebensende (End-of-Life-Care): Handlungsanweisungen und Informationsmaterialien in zwei deutschen Krankenhäusern – Eine Dokumentenanalyse. Zeitschrift für Palliativmedizin. 2016;17(17):30–37. | ||
Ghanem HM, Abou-Alia AM, Alsirafy SA. Prevalence of methicillin-resistant Staphylococcus aureus colonization and infection in hospitalized palliative care patients with cancer. Am J Hosp Palliat Care. 2013;30(4):377–379. | ||
Ali S, Sykes N, Flock P, Hall E, Buchan J. An investigation of MRSA infection in a hospice. Palliat Med. 2005;19(3):188–196. | ||
Prentice W, Dunlop R, Armes PJ, Cunningham DE, Lucas C, Todd J. Methicillin-resistant Staphylococcus aureus infection in palliative care. Palliat Med. 1998;12(6):443–449. | ||
Gleeson A, Larkin P, Walsh C, O’Sullivan N. Methicillin-resistant Staphylococcus aureus: prevalence, incidence, risk factors, and effects on survival of patients in a specialist palliative care unit: a prospective observational study. Palliat Med. 2016;30(4):374–381. | ||
Schmalz O, Strapatsas T, Alefelder C, Grebe SO. Methicillin-resistant Staphylococcus aureus in palliative care: a prospective study of Methicillin-resistant Staphylococcus aureus prevalence in a hospital-based palliative care unit. Palliat Med. 2016;30(7):703–706. | ||
Heudorf U, Farber D, Mischler D, et al. [Multidrug-Resistant Organisms (MDRO) in Rehabilitation Clinics in the Rhine-Main-District, Germany, 2014: Prevalence and Risk Factors]. Die Rehabilitation (Stuttg). 2015;54(5):339–345. German. | ||
March A, Aschbacher R, Pagani E, et al. Changes in colonization of residents and staff of a long-term care facility and an adjacent acute-care hospital geriatric unit by multidrug-resistant bacteria over a four-year period. Scand J Infect Dis. 2014;46(2):114–122. | ||
Gruber I, Heudorf U, Werner G, et al. Multidrug-resistant bacteria in geriatric clinics, nursing homes, and ambulant care prevalence and risk factors. Int J Med Microbiol. 2013;303(8):405–409. | ||
Dand P, Fyvie J, Yee A, Sykes N. A survey of methicillin-resistant Staphylococcus aureus (MRSA) management in hospices/palliative care units. Palliat Med. 2005;19(3):185–187. | ||
Bukki J, Klein J, But L, et al. Methicillin-resistant Staphylococcus aureus (MRSA) management in palliative care units and hospices in Germany: a nationwide survey on patient isolation policies and quality of life. Palliat Med. 2011;27(1):84–90. | ||
Anonymous. [Recommendations for prevention and control of methicillin-resistant staphylococcus aureus (MRSA) in medical and nursing facilities]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2014;57(6):696–732. | ||
Brugha R, Varvasovszky Z. Stakeholder analysis: a review. Health Policy Plan. 2000;15(3):239–246. | ||
Varvasovszky Z, Brugha R. A stakeholder analysis. Health Policy Plan. 2000;15(3):338–345. | ||
Stiel S, Pestinger M, Moser A, et al. The use of Grounded theory in palliative care: methodological challenges and strategies. J Palliat Med. 2010;13(8):997–1003. | ||
Strauss AL, Corbin JM. Grounded theory in practice. Thousand Oaks, CA: Sage Publications; 1997. | ||
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. | ||
MAXQDA, Software für qualitative Datenanalyse [computer program]. Berlin, Germany: Sozialforschung GmbH; 1989–2015. | ||
Salge TO, Vera A, Antons D, Cimiotti JP. Fighting MRSA infections in hospital care: how organizational factors matter. Health Serv Res. 2017;52(3):959–983. | ||
Lupion-Mendoza C, Antunez-Dominguez MJ, Gonzalez-Fernandez C, Romero-Brioso C, Rodriguez-Bano J. Effects of isolation on patients and staff. Am J Infect Control. 2015;43(4):397–399. | ||
Anonymous. [Infection prevention in the home. Recommendations of the Commission for Hospital Hygiene and Infection Production of the Robert Koch Institute (RKI)]. Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz. 2005;48(9):1061–1080. | ||
Siegel JD, Rhinehart E, Jackson M, Chiarello L; Healthcare Infection Control Practices Advisory Committee. 2007 Guideline for isolation precautions: preventing transmission of infectious agents in healthcare settings. Am J Infect Control. 2007;35(10 Suppl 2):S65–S164. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.