Back to Journals » Clinical Ophthalmology » Volume 11
Trypan blue-assisted posterior capsulorhexis in pediatric cataract surgery
Authors Lotfy A ![]() , Abdelrahman A
, Abdelrahman A ![]()
Received 25 September 2016
Accepted for publication 8 December 2016
Published 24 January 2017 Volume 2017:11 Pages 219—222
DOI https://doi.org/10.2147/OPTH.S123150
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ayman Lotfy,1,2 Ayman Abdelrahman1,2
1Ophthalmology Department, Zagazig University Hospital, 2Alpha Vision Center, Zagazig, Egypt
Purpose: To evaluate the safety and efficacy of staining the posterior capsule with trypan blue during capsulorhexis in pediatric cataract surgery.
Patients and methods: This was a prospective randomized comparative study carried out at Alpha Vision Center, Zagazig, Egypt. This study included 2 groups of children with pediatric cataract randomly allocated to undergo irrigation and aspiration. In the trypan group, which included 11 eyes, trypan blue was used to stain the posterior capsule during posterior capsulorhexis. In the control group, which included 10 eyes, no staining was performed. All surgeries were performed by the same surgeon. The 2 groups were compared for criteria such as completion of capsulorhexis, disruption of vitreous face and in-the-bag intraocular lens implantation.
Results: This study included 21 eyes of 16 patients (age range: 6 months–4 years). A statistically significant difference was observed for the following parameters between the 2 groups: capsulorhexis completion (P=0.04), vitreous face disruption (P=0.01) and in-the-bag intraocular lens implantation (P=0.022).
Conclusion: This study suggests that staining of the posterior capsule during capsulorhexis in pediatric cataract operation gives better results than capsulorhexis without staining. The stain changes the capsule texture making capsulorhexis easier with fewer complications.
Keywords: staining, capsulorhexis, pediatric, cataract, trypan
Introduction
The major preventable cause of visual impairment during childhood is pediatric cataract.1 A clear visual axis is the optimal surgical outcome of the pediatric cataract.2 The visual axis may be obstructed by opacification of posterior capsule and hyaloid face and by inflammatory membranes.3 Posterior capsule opacification (PCO) is a common postoperative complication after pediatric cataract surgery with 100% risk.4 Multiple procedures have been used to prevent PCO and maintain a clear visual axis. These techniques include lensectomy with anterior vitrectomy, posterior capsulorhexis and intraocular lens (IOL) optic capture.5 Posterior capsulorhexis is considered to be difficult as the capsule is thin and fragile.6 Trypan blue has been used for anterior capsule staining in white cataracts7 and also for performing posterior capsulorhexis in pediatric cataract in order to change the nature of the capsule and facilitate visualization. Use of trypan blue allows better controlled posterior capsulorhexis and facilitates optic capture of the IOL, thus providing better centration and consequently better optical performance.8,9
Patients and methods
This study, carried out at Alpha Vision Center, Zagazig, Egypt, was performed according to the Declaration of Helsinki and was approved by the institutional review board of Alpha Vision Center. Written informed consent was obtained from the guardian of each patient (Figure S1). This study included 21 eyes of 16 patients with congenital cataract. They were randomly divided into 2 groups: group A, the trypan group that included 11 eyes, and group B, the control group that included 10 eyes. Of the 16 patients, ages ranged from 6 months to 4 years, 9 were males, and 7 were females. All the patients underwent complete ophthalmic examination with posterior segment evaluation. All the cases were operated by the same surgeon.
Surgical technique
All the patients in both the groups were operated under general anesthesia. A corneal tunnel was made by 2.8 mm keratome, and 2 paracentesis were made by 20 G micro vitreoretinal blade. Viscoelastic material (Healon®; Abbot Medical Optics Inc., Santa Ana, CA, USA) was injected into the anterior chamber, and capsulorhexis was performed using forceps (in cases with white cataract the rhexis was done after staining the anterior capsule with trypan blue). The lens matter was removed by bimanual irrigation aspiration. In group A, the posterior capsule was stained by injection of an air bubble and then 0.1 mL of trypan blue (VisionBlue®; DORC, Zuildland, the Netherlands) was instilled under the air bubble. The dye was then washed with a balanced salt solution. High-viscosity viscoelastic was instilled both in front of and into the capsular bag. A cystotome was used to create an opening in the posterior capsule. Healon was then instilled behind the posterior capsule to create a plane between the posterior capsule and the vitreous face. The needle was then used to hook, lift and tear the capsule to create a triangular opening and capsular flap. Capsulorhexis was then completed using rhexis forceps. In group B, posterior capsulorhexis was done without staining with the dye. After opening the posterior capsule, the vitrector port was inserted below the posterior capsule. An anterior vitrectomy was performed to remove a core of the vitreous from the visual axis. A foldable 3-piece hydrophobic acrylic IOL was then implanted in-the-bag and the wounds were sutured with subconjunctival injection of antibiotic and steroids. The 2 groups were compared for completion of capsulorhexis, disruption of vitreous face and implantation of IOL (in sulcus or in-the-bag) (Figure 1). All the cases were followed up for 1 year for detection of PCO.
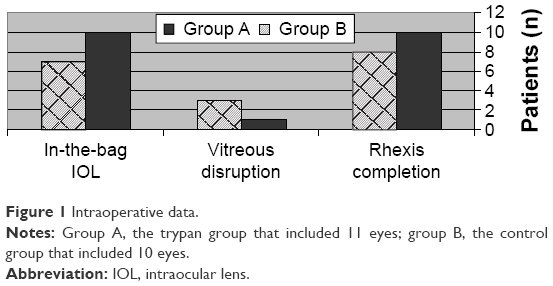 | Figure 1 Intraoperative data. |
Statistical analysis
Data analysis was performed using SPSS for Windows (version 17.0; SPSS Inc., Chicago, IL, USA). Chi-squared test was used to statistically analyze the results between the 2 groups, and the level of significance was set at P<0.05.
Results
Preoperative data are shown in Table 1. In group A, rhexis was completed in 10 cases (91%) whereas in group B, which was not stained, rhexis was completed in only 2 cases (20%) which showed statistically significant difference (P=0.04). The anterior vitreous was disrupted in only 1 case (9%) in group A and in 3 cases (30%) in group B (P=0.01; significantly different). IOL was implanted in-the-bag in 10 cases (91%) in group A and in 7 cases (70%) in group B with a statistically significant difference (P=0.022). The patients were followed up for 12 months to check whether they have developed PCO, which was not detected in both the groups. Intraoperative and postoperative data are shown in Table 2.
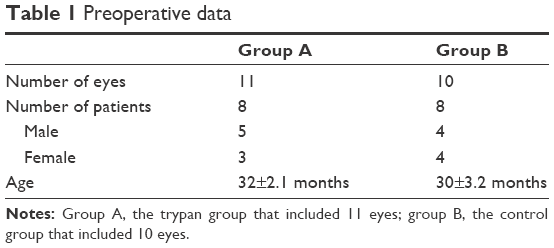 | Table 1 Preoperative data |
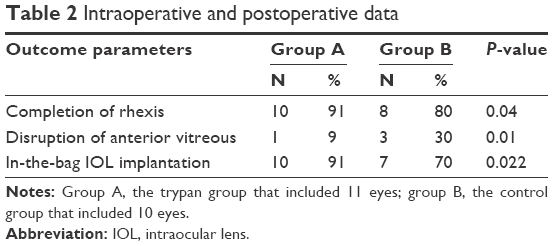 | Table 2 Intraoperative and postoperative data |
Discussion
Posterior capsulorhexis in pediatric cataract surgery has the advantage of decreasing the incidence of posterior capsular opacification postoperatively. In this study, we found it easier to visualize the posterior capsule after staining with trypan blue. Also, it was easier to properly control posterior capsulorhexis as the stained capsule was less elastic. This has been reflected in the results. Posterior capsulorhexis was completed in 91% of the cases in group A (where the dye was used) and in 80% of the cases in group B (rhexis without dye).10 Sharma et al11 used trypan blue-assisted capsulorhexis with IOL optic capture. They reported that rhexis was completed in 94.4% of the cases when the dye was used compared with 64.7% when it was not used.11 In a randomized study by Saini et al12 that included 44 eyes, 25 eyes were operated using trypan blue dye and 19 eyes without the stain; the results showed that in the group that used the dye, 82.6% of the cases had complete posterior rhexis, whereas in the group that did not use the dye, only 52.6% of cases had complete rhexis. Ivanka and Valentina13 reported the occurrence of posterior capsular opacification in 7 cases (21%). In this work, disruption of the anterior vitreous face occurred in 1 eye (10%) in group A and in 3 eyes (30%) in group B. Our results are comparable with the results published by Dholakia et al14 who studied the disturbance of vitreous face in congenital cataract and reported vitreous face disruption in 4.7% of eyes and in-the-bag IOL implantation in 92.5% of cases. In this study, in-the-bag IOL implantation was performed in 91% of cases in group A and in 70% of cases in group B.
Conclusion
Trypan blue-assisted posterior capsulorhexis is of advantage in pediatric cataract surgery. The dye helps in the completion of rhexis with safer in-the-bag IOL implantation and less postoperative PCO.
The limitation of this study is the small number of cases and the lack of objective measures for capsule elasticity.
Acknowledgments
The abstract of this paper was presented at the World Ophthalmology Congress; 2012 (Abu Dhabi, United Arab Emirates).15
Disclosure
The authors report no conflicts of interest in this work.
References
Vasavada AR, Praveen MR, Tassignon MJ, et al. Posterior capsule management in congenital cataract surgery. J Cataract Refract Surg. 2011;37(1):173–193. | ||
Taylor D, Wright KW, Amaya L, Cassidy L, Nischal K, Russell-Eggitt I. Should we aggressively treat unilateral congenital cataracts? Br J Ophthalmol. 2001;85(9):1120–1126. | ||
Ram J, Brar GS, Kaushik S, Gupta A, Gupta A. Role of posterior capsulotomy with vitrectomy and intraocular lens design and material in reducing posterior capsule opacification after pediatric cataract surgery. J Cataract Refract Surg. 2003;29(8):1579–1584. | ||
Knight-Nanan D, O’Keefe M, Bowell R. Outcome and complications of intraocular lenses in children with cataract. J Cataract Refract Surg. 1996;22(6):730–736. | ||
Pandey SK, Wilson ME, Trivedi RH, et al. Pediatric cataract surgery and intraocular lens implantation: current techniques, complications, and management. Int Ophthalmol Clin. 2001;41(3):175–196. | ||
Argento C, Badoza D, Ugrin C. Optic capture of the AcrySof intraocular lens in pediatric cataract surgery. J Cataract Refract Surg. 2001;27(10):1638–1642. | ||
Bhartiya P, Sharma N, Ray M, Sinha R, Vajpayee RB. Trypan blue assisted phacoemulsification in corneal opacities. Br J Ophthalmol. 2002;86(8):857–859. | ||
Menapace R. Posterior capsulorhexis combined with optic buttonholing: an alternative to standard in-the-bag implantation of sharp-edged intraocular lenses? A critical analysis of 1000 consecutive cases. Graefes Arch Clin Exp Ophthalmol. 2008;246(6):787–801. | ||
Sharma N, Gupta V, Vajpayee RB. Trypan-blue-assisted posterior capsule plaque removal. J Cataract Refract Surg. 2002;28(6):916–917. | ||
Grieshaber MC, Pienaar A, Stegmann R. Posterior vertical capsulotomy with optic entrapment of the intraocular lens in congenital cataracts for prevention of capsular opacification. J Cataract Refract Surg. 2005;31(5):886–894. | ||
Sharma N, Balasubramanya R, Dada VK, Vajpayee RB. Efficacy of trypan blue in posterior capsulorhexis with optic capture in pediatric cataracts. BMC Ophthalmol. 2006;21:6–12. | ||
Saini JS, Jain AK, Sukhija J, Gupta P, Saroha V. Anterior and posterior capsulorhexis in pediatric cataract surgery with or without trypan blue dye: randomized prospective clinical study. J Cataract Refract Surg. 2003;29(9):1733–1737. | ||
Ivanka P, Valentina LL. Surgical technique and postoperative complications in pediatric cataract surgery: retrospective analysis of 21 cases. Croat Med J. 2004;45(3):287–291. | ||
Dholakia SA, Praveen MR, Vasavada AR, Nihalani B. Completion rate of primary posterior continuous curvilinear capsulorhexis and vitreous disturbance during congenital cataract surgery. J AAPOS. 2006;10(4):351–356. | ||
Lotfy A, and Abdelrahman A. Trypan blue-assisted posterior capsulorhexis in pediatric cataract surgery. Abstract presented at: World Ophthalmology Congress 2012; 16–20 February 2012; Abu Dhabi, United Arab Emirates. |
Supplementary material
 | Figure S1 Consent for operation. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.