Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
Tracheal intubation with the rigid tube for laryngoscopy – a new method
Authors Marchis IF ![]() , Radeanu D
, Radeanu D ![]() , Cosgarea M
, Cosgarea M ![]()
Received 9 October 2018
Accepted for publication 18 January 2019
Published 25 February 2019 Volume 2019:15 Pages 309—313
DOI https://doi.org/10.2147/TCRM.S190186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
This paper has been retracted
Ioan Florin Marchis, Doinel Radeanu, Marcel Cosgarea
ENT Department, Iuliu Haţieganu University of Medicine and Pharmacy, Cluj-Napoca, Romania
Background: The rigid tube for laryngoscopy is an instrument used in ENT, for inspecting the larynx and its vicinity. We used it to facilitate intubation, in ENT patients.
Methods: Twenty patients attending for surgery were included for study. Group 1 (n=10) had no airway pathology but at least two predictors of an anatomically difficult airway. Group 2 (n=10) had an obstructing airway pathology. After anesthesia induction, classical laryngoscopy was performed, and intubation grade registered. Using the retromolar approach the rigid tube advanced slowly, the epiglottis was lifted, and the vocal cords were visualized. The bougie was introduced through the rigid tube into the trachea, the rigid tube was extracted, and the intubating tube was placed in the trachea, over the bougie.
Results: The mean (SD) maneuver duration was 59.4 (18.2) sec. The Cormack-Lehane view of the glottis at classical laryngoscopy was poor in four patients in Group 1 and six patients in Group 2. The lowest desaturation was 82%. No complications other than sore throat were noted.
Conclusion: The rigid tube for laryngoscopy is a useful tool for intubation in ENT patients. We noticed an advantage against classical intubation in patients with base of tongue carcinoma, reduced mouth opening and protruding upper incisors with this instrument.
Keywords: rigid tube, laryngoscopy, intubation, difficult cases intubation, difficult airway, retromolar approach, airway introducer
Introduction
Airway management is an ongoing challenge for the anesthesiologist as difficulties or failures in securing the airway are still important factors in morbidity and mortality related to anesthesia, despite certain technical advances in recent years. The Difficult Airway Society (DAS) estimated 20 deaths per year because of loss of airway in ICU and anesthetic practice in the UK alone.1 The frequency of difficult intubation in ear, nose, and throat (ENT) surgery is high because of tumors, radiotherapy, previous airway surgery.2 Many new tools have been developed, and many educational resources are dedicated to improving the skills of airway management, but the classical laryngoscope is still the most used tool for intubation.3
Various difficult airway guidelines have been established for different scenarios of difficult airway.3 The widespread use of supraglottic devices and their extended use meant a big step forward in airway management. Some studies showed that the invasive airway control in dramatic situations is not always lifesaving mostly because of lack of practice.4 The video laryngoscope (channeled or blade), the flexible or rigid endoscopes are, without a doubt, very useful, but they require training and necessitate a supplementary investment.5,6 It is universally accepted that no instrument used to control the airway is perfect and difficult intubation is often unanticipated, so it is the practitioner’s responsibility to build a good strategy and use the appropriate tool in each case.7
It is in this context that we tested the efficiency of the rigid tube for laryngoscopy (RTL), an instrument routinely used in ENT for inspecting the larynx and surrounding areas, including the upper esophagus, to intubate patients who met at least two criteria for difficult airway. The RTL is a 15–25 cm long, straight, hollow tube with a diameter of 0.5–2.0 cm with a bevel end which has a light port and the image is obtained directly by looking through the tube (Figure 1). It resembles a rigid bronchoscope or esophagoscope, the only differences are the shorter length and the wider range of diameters available. Although the rigid bronchoscope and esophagoscope are both well mentioned and described extensively in the literature, the RTL is usually named rigid laryngoscope or rigid tube. When in use, it must be attached to a light source.8
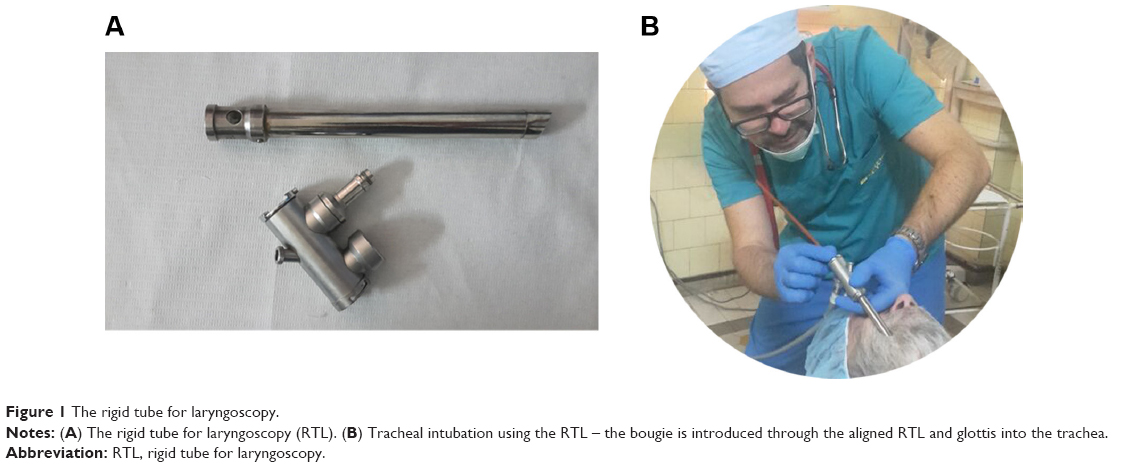 | Figure 1 The rigid tube for laryngoscopy. |
The purpose of this study was to demonstrate that the RTL is safe and fast for intubating patients with difficult airways, it offers an advantage against classical intubation regarding glottis view in some difficult airway scenarios.
Methods
This was a prospective, observational, single-center study evaluating the feasibility of tracheal intubation using the RTL with the approval of the University of Medicine and Pharmacy – Cluj Napoca Ethics Committee no 432/24.11.2016 in accordance with the Declaration of Helsinki and registered with ClinicalTrials.gov NCT03341507. The study involved adult patients with ASA physical status 1–3, requiring surgery for an ENT pathology and having a presumed anatomically difficult airway according to The Simplified Airway Risk Index (SARI) score who formed group 1.9 Patients with obstructing airway pathology: oropharyngeal tumors, cervical masses, previous neck surgery or radiotherapy, also with predicted difficult intubation were included in group 2. The two groups were used to show the efficiency of RTL versus the gold standard in intubating patients with various types of airway issues. We decided to include ten patients in each group, a reasonable number for testing a new method of airway control. Signed informed consent was obtained from all patients.
Stridor or marked laryngeal or tracheal stenosis, vocal cords polyps, emergency surgery, high aspiration risk, decompensated cardiac and pulmonary disease and patient refusal were criteria of exclusion from the study. We also decided to reject from the study patients with a Cormack-Lehane grade one glottis view.10 We also excluded patients in which mask ventilation was technically difficult causing marked desaturation, requiring prompt action to secure the airway, in which case we deemed it potentially unsafe using the experimental RTL. The investigator underwent a training period before starting the study in order to get used to maneuvering the RTL and acquire a reasonable level of skill using it. The training was provided by ENT surgeons from the Hospital’s ENT Department.
A preanesthetic exam was performed with careful assessment of the airway. Patients with features predictive for difficult intubation gathering more than four points on the SARI score and with no known airway pathology were included in group 1.9 Group 2, with obstructing airway pathology had nasofibroscopy prior to surgery. All patients had ENT evaluation of their airway. Table 1 presents other variables noted during the preanesthetic assessment phase of the study.
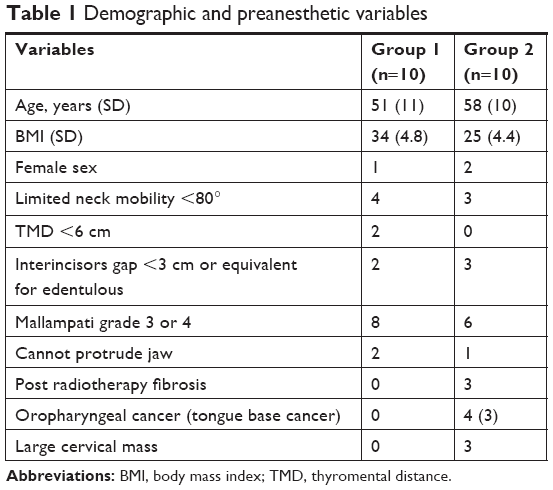 | Table 1 Demographic and preanesthetic variables |
Premedication consisted of 1 or 2 mg of Midazolam given intravenously 15 minutes before intervention, in the preoperative room. On the patient’s arrival in the operating room, standard hemodynamic and respiratory monitoring were commenced: ECG, non-invasive arterial blood pressure, oxygen saturation, respiratory frequency, end-tidal CO2. A difficult airway kit was prepared, at disposal, the RTL was in position with the light source attached and an experienced ENT surgeon was present for emergency intervention and help. Patients were preoxygenated for 5 minutes and induction of anesthesia with propofol-succinylcholine and fentanyl was performed. After 1 minute of mask ventilation, we noted the oxygen saturation on pulse oximeter, classical laryngoscopy was performed with a McCoy curved blade laryngoscope with the blade in neutral position, without the help of the movable distal end, and Cormack-Lehane glottis visualization were registered.
The RTL intubation was started with the head in extension and in sniffing position, we used a retromolar approach, with teeth protection. We used a 1.2–1.8 cm wide and 15–25 cm long tube depending on the patient’s preoperative assessment and pathology. We decided to start with a larger diameter laryngoscope tube and if it proved difficult to visualize the glottis because of obstructing anatomical or pathological structures, we tried once more with a thinner tube. The RTL was advanced slowly until it reached the epiglottis, then the epiglottis was lifted, and the vocal cords visualized. The thyroid cartilage was a land point when advancing the RTL. After that, the bougie was introduced through the RTL into the glottis, the RTL extracted, and the standard cuffed intubating tube with lubricated tip was placed in the trachea gently, over the bougie.12 The nasofibroscopy, ENT and physical exam prior to surgery guided us through the procedure and helped us choose the approaching side. Secretions were aspirated through the RTL as needed. We decided to stop the attempt at 120 seconds or if the patient desaturated to 80%.
We noted the Cormack-Lehane glottis visualization at classical laryngoscopy, the time from classical laryngoscopy until the airway was secured, the lowest oxygen saturation during the procedure and any other complications occurring during the procedure. As the purpose was to show that the technique is useful and even superior to conventional methods of airway control in certain situations we have documented every patient data regarding airway, ENT pathology, and difficult airway history. We recorded images to document the challenging cases and prove the efficiency of the RTL. We also took notice of any complications that may have arisen during or after the procedure.
Results
Over a 3-month period 31 patients were recruited for the study, all showing predictors of difficult intubation or having airway pathology. Nine of them had a Cormack-Lehane grade one glottis view at classical laryngoscopy and were excluded, while two cases were difficult to mask ventilate and desaturated, so we took the first chance to secure the airway before using the RTL.
The remaining 20 patients were included in the study, 10 in group 1 with no airway pathology and the rest in group 2 with airway pathology. The mean (SD) maneuver duration was 70.1 (18.6) seconds measured from the beginning of classical laryngoscopy until the first breath was delivered through the endotracheal tube. The mean (SD) duration of classical laryngoscopy was 10.6 (1.9) sec and the mean (SD) duration of the procedure performed with the RTL until tracheal intubation was 59.4 (18.2) sec. The Cormack-Lehane glottis visualization at classical laryngoscopy was poor, grade 3 or 4, in four patients in Group 1 and six patients in Group 2. The RTL glottis was well visualized in nine patients in group 1 and all patients of group 2. The lowest desaturation was 82%. No complications other than sore throat were noticed. We had one failure to intubate in group 1, in a patient admitted for ear surgery with buck teeth, inability to protrude the jaw and TMD <6 cm, a Cormack-Lehane grade four at classical laryngoscopy, in which the RTL attempt was also unsuccessful, and we used the laryngeal mask without further problems. Table 2 presents the correlation between difficult airway predictors and glottis view with both curved blade laryngoscope and RTL.
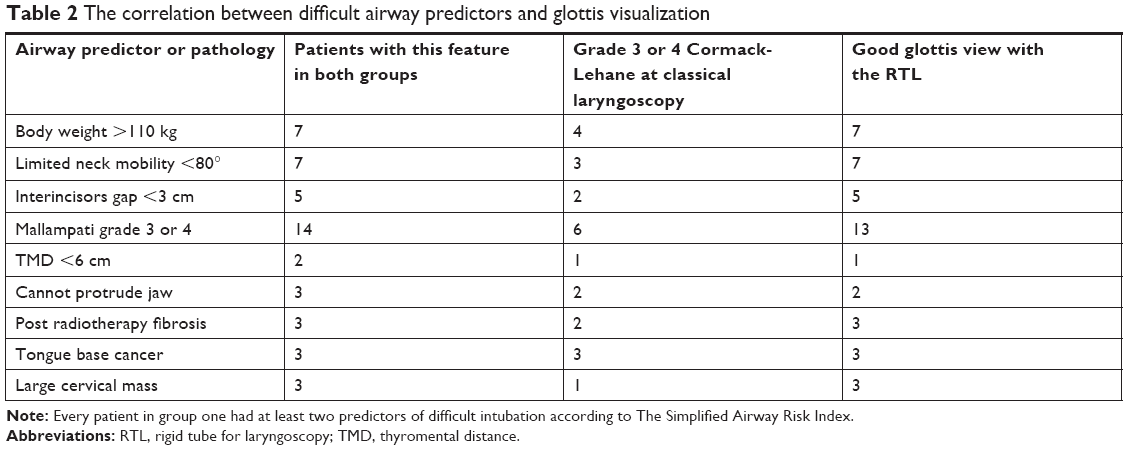 | Table 2 The correlation between difficult airway predictors and glottis visualization |
Discussion
We first used this method in a patient with previous mandibular surgery which we had to anaesthetize. Although he had a reasonable mouth opening (about 4 cm) and no other criteria of difficult intubation, we couldn’t intubate the patient. Using a McCoy laryngoscope, we’ve noted a C-L grade four at laryngoscopy. The patient was easy to mask ventilate and since we had the RTL readily available, as the patient was to be investigated with this tool, we decided to try to use it for intubation. With a retromolar approach it was surprisingly easy to visualize the glottis, to stick a bougie through the tube and glottis, retract the RTL and then intubate through the bougie without any complications.
This prospective study was aimed to demonstrate the efficiency of the RTL for intubation and the possibility of using it by anesthesiologists as a rescue option when other methods have failed. As ENT surgeons are familiar with this instrument, the technique can be easily adopted by them and used in emergency situations.
The retromolar approach, resembling the Bonfil’s Rigid Endoscope technique or the paraglossal laryngoscopy with the straight blade Miller laryngoscope offers an advantage in case of temporo-mandibular joint dysfunction, base of tongue tumors and reduced neck mobility as it can deviate from the sagittal plane.5,11,12 The improved view obtained with this technique could result from a reduced risk of backward displacement of the tongue and epiglottis. In addition, the molar or retromolar technique reduces the intrusion of maxillary structures into the line of sight, so that a better view of the glottis is achieved for the same degree of soft tissue compression as compared with the Macintosh technique.11 Another advantage is the possibility of using either the right or the left side approach, making it more versatile in dealing with oropharyngeal or large cervical tumors. The RTL also proved to be very helpful by producing a good view of the glottis making intubation easy in some cases with no airway pathology but with poor classical laryngoscopy view of the glottis, patients with protruding upper teeth, limited neck movement or reduced interincisors gap.
Suctioning secretions is easy through the RTL as opposed to Bonfil’s Endoscope or flexible endoscope and there is no risk of fogging since the RTL does not have a distal optical system.12 The RTL is a robust, metallic instrument easy to decontaminate and resistant to long-term use, while fiberscopes could be damaged accidentally during regular utilization. Being already a basic tool in ENT it does not require a supplemental investment in hospitals with an ENT Department.
The major disadvantage of RTL use, as in the case of rigid bronchoscopy, is the reduced visual field which can be improved by increasing the tube diameter. The RTL is easier to use, safer and offers a better view than the rigid bronchoscope because of its smaller size. Dental injury and bleeding during the procedure might be higher with the use of RTL as compared to classical laryngoscopy. We did not experience such incidents. The bougie intubation carries the risk of vocal cord injury and the impossibility of advancing the tracheal tube if the respiratory space is too narrow as well as airway perforation if it is inserted too deep.12–14 This is the reason we did not admit in the study patients with stridor or known limited respiratory space.
Conclusion
Our study showed that the RTL is a reliable tool for intubation when used in the manner described above. Our method proved to be efficient in patients with oropharyngeal cancer, previous radiotherapy, limited neck movement, protruding upper teeth and temporo-mandibular joint dysfunction. Although we did not find any data in the literature regarding this method of airway approach, this simple, cost efficient technique, always at hand in a hospital with an ENT department, might prove useful as a rescue option.
Informed consent
Written informed consent was obtained from all patients participating in the study and from the patient presented in Figure 1 regarding the image being published.
Data sharing statement
This study was submitted to ClinicalTrials.gov NCT03341507 where the contact information of the study principal investigator is available. Raw data such as images, video recordings or written documents related to this study are available on request by emailing to the corresponding author.
Acknowledgment
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
Henderson J, Popat M, Latto P, Pearce A. Difficult airway society guidelines [correspondence]. Anaesthesia. 2004;59:1242–1243. | ||
Arné J, Descoins P, Fusciardi J, et al. Preoperative assessment for difficult intubation in general and ENT surgery: predictive value of a clinical multivariate risk index. Br J Anaesth. 1998;80(2):140–146. | ||
Apfelbaum JL, Hagberg CA, Caplan RA, et al. Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on management of the difficult airway. Anesthesiology. 2013;118(2):251–27002. | ||
Green L. Can’t intubate, can’t ventilate! A survey of knowledge and skills in a large teaching hospital. Eur J Anaesthesiol. 2009;26(6):480–483. | ||
Halligan M, Charters P. Learning curve for the Bonfils intubation fibrescope. Br J Anaesth. 2002;89:671–672. | ||
Smith JE, Jackson AP, Hurdley J, Clifton PJ. Learning curves for fibreoptic nasotracheal intubation when using the endoscopic video camera. Anaesthesia. 1997;52(2):101–106. | ||
Nørskov AK, Rosenstock CV, Wetterslev J, Astrup G, Afshari A, Lundstrøm LH. Diagnostic accuracy of anaesthesiologists’ prediction of difficult airway management in daily clinical practice: a cohort study of 188 064 patients registered in the Danish anaesthesia database. Anaesthesia. 2015;70(3):272–281. | ||
Fagan J, De Groot M. Open access atlas of otolaryngology, head & neck operative surgery. Rigid laryngoscopy, oesophagoscopy & bronchoscopy in adults. Available from: https://vula.uct.ac.za/access/content/group/ba5fb1bd-be95-48e5-81be-586fbaeba29d/Rigid%20laryngoscopy%2C%20oesophagoscopy%20and%20bronchoscopy%20in%20adults.pdf. Accessed May 20, 2018. | ||
Nørskov AK, Wetterslev J, Rosenstock CV, et al. Effects of using the simplified airway risk index vs usual airway assessment on unanticipated difficult tracheal intubation – a cluster randomized trial with 64,273 participants. Br J Anaesth. 2016;116(5):680–689. | ||
Krage R, van Rijn C, van Groeningen D, et al. Cormack-Lehane classification revisited. Br J Anaesth. 2010;105(2):220–227. | ||
Henderson JJ. The use of paraglossal straight blade laryngoscopy in difficult tracheal intubation. Anaesthesia. 1997;52(6):552–560. | ||
Dogra S, Falconer R, Latto IP. Successful difficult intubation. Tracheal tube placement over a Gum-Elastic bougie. Anaesthesia. 1990;45(9):774–776. | ||
Paul A, Gibson AA, Robinson OD, Koch J. The traffic light bougie: a study of a novel safety modification. Anaesthesia. 2014;69(3):214–218. | ||
Grape S, Schoettker P. The role of tracheal tube introducers and stylets in current airway management. J Clin Monit Comput. 2017;31(3):531–537. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.