Back to Journals » Clinical Ophthalmology » Volume 14
The Evolution of Diabetic Retinopathy Screening Programmes: A Chronology of Retinal Photography from 35 mm Slides to Artificial Intelligence
Authors Huemer J ![]() , Wagner SK
, Wagner SK ![]() , Sim DA
, Sim DA ![]()
Received 7 May 2020
Accepted for publication 1 July 2020
Published 20 July 2020 Volume 2020:14 Pages 2021—2035
DOI https://doi.org/10.2147/OPTH.S261629
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Josef Huemer,1,2 Siegfried K Wagner,1 Dawn A Sim1
1NIHR Biomedical Research Center at Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology, London, UK; 2Vienna Institute for Research in Ocular Surgery, A Karl Landsteiner Institute, Hanusch Hospital, Vienna, Austria
Correspondence: Dawn A Sim
Moorfields Eye Hospital, NHS Foundation Trust, 62 City Road, London EC1V 2PD, United Kingdom
Tel +44 (0)20 7253 3411
Email [email protected]
Abstract: As a third of people with diabetes mellitus (DM) will suffer the microvascular complications of diabetic retinopathy (DR) and therapeutic options can effectively prevent visual impairment, systematic screening has substantially reduced disease burden in developed countries. In an effort to tackle the rising incidence of DM, screening programmes have modernized in synchrony with technical and infrastructural advancements. Patient evaluation has shifted from face-to-face ophthalmologist-based review delivered through community grassroots to asynchronous store-and-forward modern telemedicine platforms commissioned on a nationwide scale. First pioneered with primitive 35-mm slide film retinal photography, the last decade has seen an emergence of high resolution and widefield imaging devices, which may reveal extents of DR indiscernible to the clinician but with implications of potential earlier identification. Similar progress has been seen in image analysis approaches – automated image analysis of retinal photographs of DR has evolved from qualitative feature detection to rules-based algorithms to autonomous artificial intelligence-powered classification. Such models have, relatively rapidly, been validated and are now receiving approval from health regulation authorities with deployment into the clinical sphere. In this review, we chart the evolution of global DR screening programmes since their inception highlighting major milestones in healthcare infrastructure, telemedicine approaches and imaging devices that have shaped the robust and effective frameworks recognised today. We also provide an outlook for the future of DR screening in the context of recent technological advancements with respect to their limitations in current times.
Keywords: telemedicine, artificial intelligence, imaging, diabetes, retina, photography
Introduction
Despite the first description of diabetic macular changes by Eduard Jaeger and Albert von Graefe in the 1850s, the relationship between cystoid macular oedema and diabetes mellitus (DM) would remain disputed until Edward Nettleship published histopathological evidence of diabetic macular oedema in 1872.1–3 Whereas the original descriptions by Jaeger were documented by ocular fundus paintings, Jackman and Webster were the first to publish a human retinal photograph nearly 30 years later in 1886.4,5 In 1968, the Airlie House classification of diabetic retinopathy (DR) established the first standards defining formal quantitative and qualitative features of disease revealed through standardised stereoscopic color fundus photography (CFP), as will be further explained in the review of imaging modalities.6,7 This provided the basic foundation for subsequent landmark studies as the Diabetic Retinopathy Study (DRS) and Early Treatment for Diabetic Retinopathy Study (ETDRS).8
DM is a global pandemic, estimated to affect 642 million people in 2040. A third of these will suffer from some degree of retinopathy.9,10 The impacts of DR on health-related quality of life, psychological well being and visual functioning are well established.11–13 The rationale for DR screening is based on the rules set forth by the WHO for screening in medicine by Wilson and Junger in 1968, including among others that DR is an important public health problem, with suitable testing, clear benefits of early treatment, and cost-efficiency.14 Hence, systematic DR screening programs in Iceland, the United Kingdom (UK), Singapore and Ireland as well as regional programs in the US and various European countries have been established.15–20
In this article, we evaluate the features and health economic impacts of different DR screening programs based on retinal photography.
History
Iceland, being cited as a pioneer of DR screening, started a screening program for patients with insulin-dependent diabetes in 1980.19–21 Screening was undertaken by an ophthalmologist in conjunction with the annual acquisition of CFP. Regional programs in Sweden were also among the first established screening programs in this era, systematically screening all DM patients in a tertiary center in Lund with a follow-up of 5 years.22 In Stockholm, Sweden’s capital, with more than a million inhabitants, a screening program started in 1990 based on four field 45° CFP in more than 100 primary healthcare centers.23 This program was based on a national training program of doctors and nurses, which had started 10 years earlier and had led to improved DM control and awareness. Analysing referral letters for patients with DM and severe sight loss, Bäcklund et al could show that new blindness in DM was reduced by more than 30% following the implementation of DR screening.23 A consensus statement by the British Diabetes Association declared that DR screening should be based on methods that can provide a minimum sensitivity of 80% and 95% of specificity for referable DR.24 The UK is the largest country to have adopted nationwide screening for all patients with DM above the age of 12 years based on telemedicine. Screening commenced in 2003, reaching national coverage in 2008. The four constituent countries, England, Scotland, Wales and Northern Ireland provide screening programs through an asynchronous store-and-forward telemedicine approach. Dilated CFP are acquired in a community setting by trained technicians and images are assessed using hierarchical graders with subsequent referral to the hospital eye services of the National Health Service (NHS) when indicated.25 This program has an uptake of above 80% of the diabetic population, having screened more than 2,250,000 patients with DM from 2016 to 2017 in England alone.26 The value of this effort was recognised in 2010 when, for the first time in 50 years, DR was no longer the primary cause for blindness certification in the working-age population of the UK.27 Singapore was the latest nation to establish nationwide telemedicine-based DR screening. Whereas previously patients had attended ad hoc screening in the primary care clinics for CFP, now standardised two field 45° CFPs are taken by trained nurses and directly sent to a reading center, providing same-day reports and, if necessary, referrals to hospital eye services.28 Screening for DR is not limited to the nationwide programs covered in this review; many countries have adopted opportunistic screening contingent on national guidelines. As these programs, however, are neither structured nor audited, and therefore are not comparable due to the lack of publicly available data, they will not be covered in this review. There are multiple examples of regional telemedicine screenings, often covering rural areas in Australia, the US, Canada, Europe, and India.18,29-38 A graphical overview of population and selected regional DR screening programs, their implementation and outcome reporting, precisely instant or synchronous versus asynchronous store-and-forward reporting is represented in Table 1 and displayed in Figure 1.
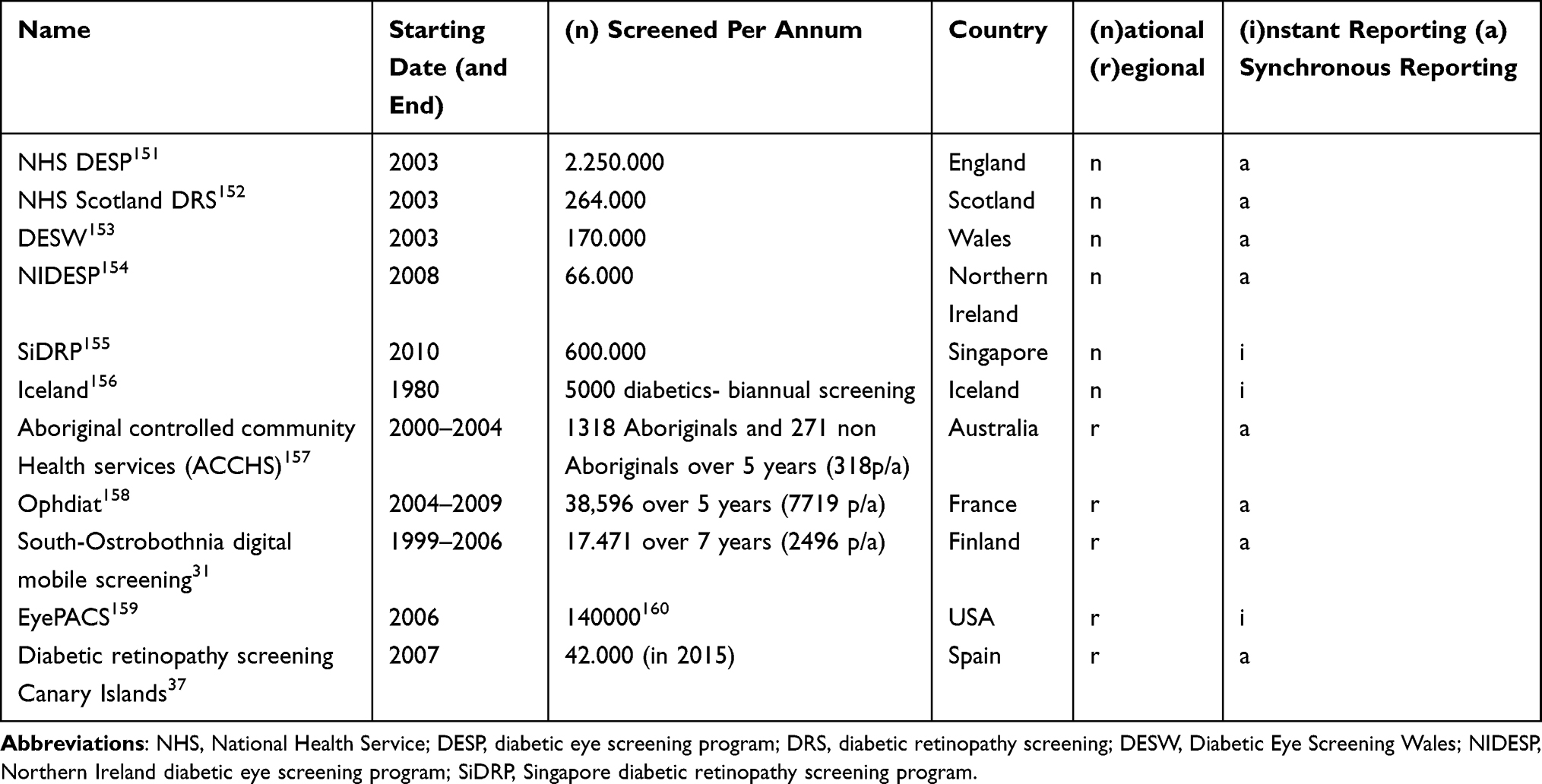 |
Table 1 Selected Population Screenings and Selected Regional Screening Programs |
 |
Figure 1 Timeline bubble chart displaying selected regional screenings with either synchronous (green) or asynchronous (blue) reporting of screening outcomes. The bubble diameter is an approximation of the number of screened patients with diabetes per annum (yellow), references can be found in Table 1. |
There is evidence that patient acceptance of telemedicine services may be superior to traditional face-to-face consultations. When conducting a randomised trial comparing telemedicine screening to direct face-to-face screening in the US, Mansberger et al demonstrated that attendance was higher when DR screening was based on a telemedicine-based methodology. Interestingly, the authors were able to show that when both groups were combined to be screened via telemedicine, the attendance proportions in both groups were comparable, showing that the acceptance of telemedicine screening is higher compared to face-to-face examinations.39
It seems conceivable that increased attendance and registration of large screening programs, therefore, is best achieved via telemedical screening programs.40
Different Imaging Approaches
The Arlie House Symposium in 1968, an international meeting of leaders in ophthalmology, internal medicine and neurosurgery sought to classify and quantify the emerging global problem of DR. Consensus of participants was established on the definition, assessment and recording of disease features identified through standardised fundus photography.8
Only three years later, a modified version of the Arlie House Classification was used for grading images based on the seven field 30° stereoscopic CFP in the first landmark trial comparing the impact of panretinal photocoagulation or observation on severe vision loss in DR.41 Over a 5-year study period, scatter photocoagulation treatment reduced the risk of severe vision loss by around 50% compared to observation, and showed a reduction of DR progression.42 The ETDRS study, another landmark trial, based its assessment on the Arlie House Classification using the seven field 30° stereoscopic CFP protocol.43 The investigators however elaborated further on the grading criteria by introducing additional granular features, such as microaneurysms and intraretinal microvascular abnormalities. Indeed, this detailed grading system has remained in use for many decades and is still considered to be the gold standard. Whereas this modality has proven to be of great value for research, it is not feasible in a screening setting.
When comparing single, two field and three field 45° CFP with the ETDRS gold standard, differences in the sensitivity and specificity have been found. The sensitivity and specificity for the detection of referrable disease was highest in three field CFP (92% and 96%), followed by two field CFP (96% and 89%) and was lowest in single-field CFP (78% and 86%).44–47 The sensitivity and specificity of two mydriatic 45° CFP, the first centered at the macula and the second on the optic disc, has been shown to be 80.2% and 96.2%, respectively.48 Despite the superior diagnostic accuracy of multiple field CFP, acquisition needs to be balanced with the greater focus on patient collaboration, resource and training. Accordingly, most screening services have adopted a two field CFP strategy as a compromise.
Due to the technological advances of digital photography and its achievements regarding resolution, the UK DR screening programs initially utilized 45° digital CFP with non-mydriatic fundus cameras on dilated patients.25 The cameras must provide a resolution of at least 30 pixels per degree on a photograph of 45° in width and 40° in height and be able to accommodate ±15 D of refractive error.25 Agreement between CFP on 35 mm film and digital CFP has been shown to be substantial to almost perfect regarding DR severity levels as well as moderate to substantial for diabetic macular edema severity levels.49 In a systematic review assessing the detection of any level of DR with digital retinal imaging, Piyasena et al could show that both non-mydriatic and mydriatic fundus imaging delivered satisfactory levels of sensitivity with 86% after exclusion of ungradable images. The proportion of ungradable images in non-mydriatic settings was 18.6% compared to 6.2% in mydriatic settings.47 With respect to the heterogeneity of the studies the authors concluded, that specificity results would depend on whether ungradable images were counted as test positive and causing difficulties in comparing specificity and proposing standardised reporting of ungradable images. In a randomised trial, Scanlon et al found age to be the strongest predictor of ungradable images, mostly related to cataracts and smaller pupil size.50 As the application of mydriatic eye drops also has potential side effects, such as mydriasis-induced acute angle closure with an incidence of 6 in 20,000 in a Caucasian population, a fine balance between image quality, gradability and patient risk needs to be emphasised.51 The Scottish DR screening is based on a single-field macular centered 45° digital CFP, only using mydriatic eye drops if the image quality is poor.52
The approach of two 45° digital CFP is also used in the first autonomous artificial intelligence (AI)-based device with FDA approval.53 In contrast to the UK, where trained technicians conduct image acquisition, for this study, a device was introduced in combination with a non-mydriatic fundus camera and AI system operator with no prior experience of fundus imaging and a standardised 4-hour training program. The AI would detect the image quality and operators would improve quality and/or perform pupil dilation for the patients if necessary. The algorithm succeeded the preset superiority endpoints for detecting referrable, in this study defined as more-than-mild DR (ETDRS level ≥35) with a sensitivity of 87% and a specificity of 90.7% as well as imageability rate of 96.1% hence becoming the first FDA autonomous artificial intelligence device in any field of medicine.53
Another increasingly popular method to conduct color fundus imaging without pupil dilation is confocal scanning ophthalmoscopy (cSO). Beams emitted by lasers or light-emitting diodes (LED) of different wavelengths scan the retina generating a composite pseudocolor image with varying fields of view. Optos (Optos plc, Scotland), a Scottish company launching their first device 25 years ago, provides various camera models consisting of a 200-degree ultra-widefield based on three lasers with different wavelengths, namely blue (488 nm), green (532 nm) and red (635 nm). The potential benefits of incorporating ultra-widefield imaging were shown in a screening setting, where the Optos revealed peripheral features of the disease in 20% of patients without discernible DR.54 The Clarus ultra-widefield camera by Carl Zeiss Meditec is able to capture a single-field image of 133°, which can be montaged to 200° on two fields with LED-based cSO.55 Another example is the multicolor scanning laser imaging module by Heidelberg Engineering, where a special lens can be mounted onto the OCT/cSO camera, providing a 105° pseudocolor image. Centervue Eidon combines a confocal scanning laser ophthalmoscopy technique with a confocal white light imaging to obtain true color CFP covering 60° per image.56,57 These technical advances may be of great interest even in a screening setting due to the advances of non-mydriatic imaging; however, further studies are warranted.
However, the aforementioned devices enabling DR screening may be costly and require technical support and infrastructure limiting their use in less affluent settings, such as the developing world. One potential option is CFP acquisition using smartphone-based camera systems in combination with AI. The Remidio Fundus on Phone camera system consists of a slit lamp-based non-mydriatic smartphone camera, which provides 45° images to detect DR and was validated against high-end fundus cameras, showing on-par performance for any DR and referable DR, thus having received FDA approval.58,59
Automated Image Analysis: Before and After AI
Telemedical assessment of CFP for DR screening requires a large amount of trained graders in reading centers to cope with the rising volume of images. For this and other reasons, the prospect of automated analysis of retinal images has garnered interest from ophthalmologists and computer scientists alike. The first publication analysing computer-aided detection (CADe) in ophthalmology was published in 1973, focusing on the detection of contour lines of retinal vessel images.60 In 1984, a French group was the first to describe microaneurysms in fluorescein angiography.61 The development of digital photography and technical advances in computing power led to computer-aided diagnosis (CADx) systems, which not only incorporate qualitative detection of features but also enable calculation of disease probability and risk stratification. To provide guidance, the American Telemedicine Association has therefore released statements on the quality,62,63 namely to validate against the gold standard ETDRS 30° seven-field stereoscopic CFP.43
Traditional machine learning techniques for image analysis were based on thresholding, edge detection, processing and filters to detect disease features with more advanced models leveraging ensemble-based approaches, multi lesion approach or content-based image retrieval.64–67 Already in 2008, Abràmoff et al published the results of an automated retinal image analysis system (ARIAS), reporting 84% sensitivity and 64% specificity for the detection of referrable DR in a retrospective analysis of 7689 CFP. In 2013, the same group reported the results of the Iowa Detection Program (IDP) for detection of referrable DR and reached 96.8% sensitivity and 59.4% specificity.68
Other examples of ARIAS based on using classic machine learning techniques have shown to provide image grades without the help of human graders.69,70 Tufail et al conducted a study in 2013 to assess the safety and cost-efficiency of three ARIAS, namely iGradingM, Retmarker and EyeArt with images from the UK National Health Service Diabetic Eye Screening Program (NHS DESP), comparing it to manual grading.71 They showed that EyeArt would provide a 94.7% sensitivity for any DR, 93.8% for referrable DR and 99.6% for PDR. Retmarker would achieve 73.0% sensitivity for any DR, 85% for referrable DR and 97.9% for PDR. iGradingM classified all images as either showing disease or being ungradable; hence, iGradingM could not be included in further analysis. Cost efficiency compared to human graders was shown for Retmarker and EyeArt. iGradingM is an ARIAS that provides binary grades for disease/no disease as well as for image quality. It has been used as a level 1 grading in the Scottish DR screening program after extensive validation since 2010.66,72,73 In a retrospective evaluation, the rate of DR was 6.6% with a sensitivity of 97.8% for referrable DR;73 the specificity was calculated as 41.2%.74 The above mentioned traditional machine learning techniques have been reviewed in detail elsewhere;75–77 their relevance today has, however, has been surpassed by the recent developments in deep learning (DL).
Although the principles of DL were described decades ago, only recently has its potential to healthcare applications become popular. The main reasons are due to improvements in computing power, especially by graphical processor units (GPU), large quantities of digital data and publically available pre-trained convolutional neural network (CNN) models like AlexNet, VGGNet or GoogleNet.78–82 DL models have outperformed traditional methods in speech recognition, computer vision, and have also been shown to be equivalent to humans in disease detection from medical imaging.83–87 One of the main differences of CNNs compared to traditional techniques is that raw data are processed by identifying features of interest through extensive training.79
With the vast amount of data collected from screening services, DL development may be ideally afforded by DR screening. The group of Abramoff et al, who had extensively reported on automated image analysis systems mentioned previously, enhanced their algorithm by incorporating DL, showing an increased, although not statistically significant sensitivity of 96.8% for referrable disease; however, they reported a steep increase from 59.4% to 87% specificity validating on the same publicly available MESSIDOR-2 dataset with an area under the receiver operator curve (AUC) of 0.98 in the detection of referrable disease.88 The algorithm, now called IDx-DR, has also been validated on a Dutch dataset labelled by three retina specialists using the International classification of diabetic retinopathy (ICDR) and the EURODIAB grading. The reported sensitivity and specificity using ICDR grades were 68% and 86%, respectively, and 91% and 84% using the EURODIAB grades.89 A key evaluation aspect in prediction models validation is that of the prospective setting. The same group subsequently published results from a prospective trial in a primary care setting, exceeding the pre-specified primary endpoint goals of a >85% sensitivity and >82.5% specificity with a sensitivity/specificity of 87.2%/90.7% and an imageability rate of 96.1%, receiving FDA approval for diagnosing more than mild DR autonomously. It is conceivable that the metrics of the IDx-DR algorithm could represent benchmark metrics for future market authorisation from the FDA.90
One concern of DL models, which are typically trained for the classification of a single disease, is their limited ability to generalise to unseen pathology. Although a given DL model may demonstrate clinical effectiveness in the detection of referable DR, what of the scenario where the image may demonstrate features of other diseases, such as glaucoma, which are known to occur with a higher incidence in people with DM?91 Ting et al have reported on a DL model to analyse DR, glaucoma and age-related macular degeneration (AMD) using CFP.92 This algorithm, now called SELENA+ was trained on almost 500,000 images;93 the authors reported a sensitivity of 90.5%, a specificity of 91.6% and an AUC of 0.936 for detecting referrable disease and was tested on the Singapore Integrated DR programme (SiDRP). To test the algorithm in multi-ethnicity environments, it was externally validated on datasets from six different countries, including Singapore, Hong Kong, China, Australia, USA and Mexico, achieving an AUC of 0.889 to 0.983 in these datasets. Of importance, this algorithm could detect possible glaucoma with a sensitivity/specificity of 96.4%/87.2% and 93.2%/88.7% for AMD when compared to human graders. Only recently, the Singaporean Health Minister announced that this algorithm will be deployed across the Singapore DR Screening program by 2022.94
In 2016, Gulshan et al published the results of a study sponsored by Google Inc, about DR detection by a CNN trained on about 128,000 CFP graded by 54 US licensed ophthalmologists and ophthalmology residents.82 Similar to IDx-DR the model could detect referrable DR with an AUC of 0.991 and 0.990 for the EyePACS-1 and MESSIDOR-2 datasets, sensitivity/specificity for EyePACS-1 were 90.3%/98.5% and 87.0%/98.% for MESSIDOR-2.
The EyeART system owned by Eyenuk is another example of a DL system used for DR grading, that has improved its performance by combining their traditional machine learning approach with CNN. EyeART v1, as aforementioned, has been evaluated in a UK-based study.71 EyeART v2.0, however, is a cloud-based technology and has been tested on >800,000 images of about 100,000 consecutive patients.95 It achieved a 91.3% sensitivity and 91.1% specificity for referrable DR with an AUC of 0.965 compared to the EyePACS graders. Furthermore, the algorithm was tested on the above mentioned Remidio Fundus on phone - smartphone-based system. Albeit a small study with only 296 patients included, EyeART achieved a sensitivity/specificity of 95.8%/80.2% for detecting any DR and 99.1%/80.4% for detection of sight-threatening DR. Remidio, the company behind the smartphone-based CFP, has developed a DL system called MEDIOS AI.96 This offline system on the same smartphone, which takes the photograph, was trained to detect more-than-mild DR achieving an impressive performance of 100% sensitivity and 87% specificity in 231 patients compared to the grading from ophthalmologists using the same images. Further studies with larger cohorts are ongoing at multiple sites.
Another, also commercially available web-based solution is called RetCAD, owned by a dutch company named Thirona. This algorithm is trained to detect DR and AMD, and has been validated on the MESSIDOR dataset with 1200 images and the AREDS dataset for AMD with 130,000 images. The sensitivity/specificity for referrable DR were 90.1%/90.6% and 91.8%/87.5% for referrable AMD, which was defined as intermediate or severe AMD; AUC were reported as 0.951 for DR and 0.949 for AMD.97 The above mentioned DL models have been reviewed in detail elsewhere and are summarised in Table 2.98,99
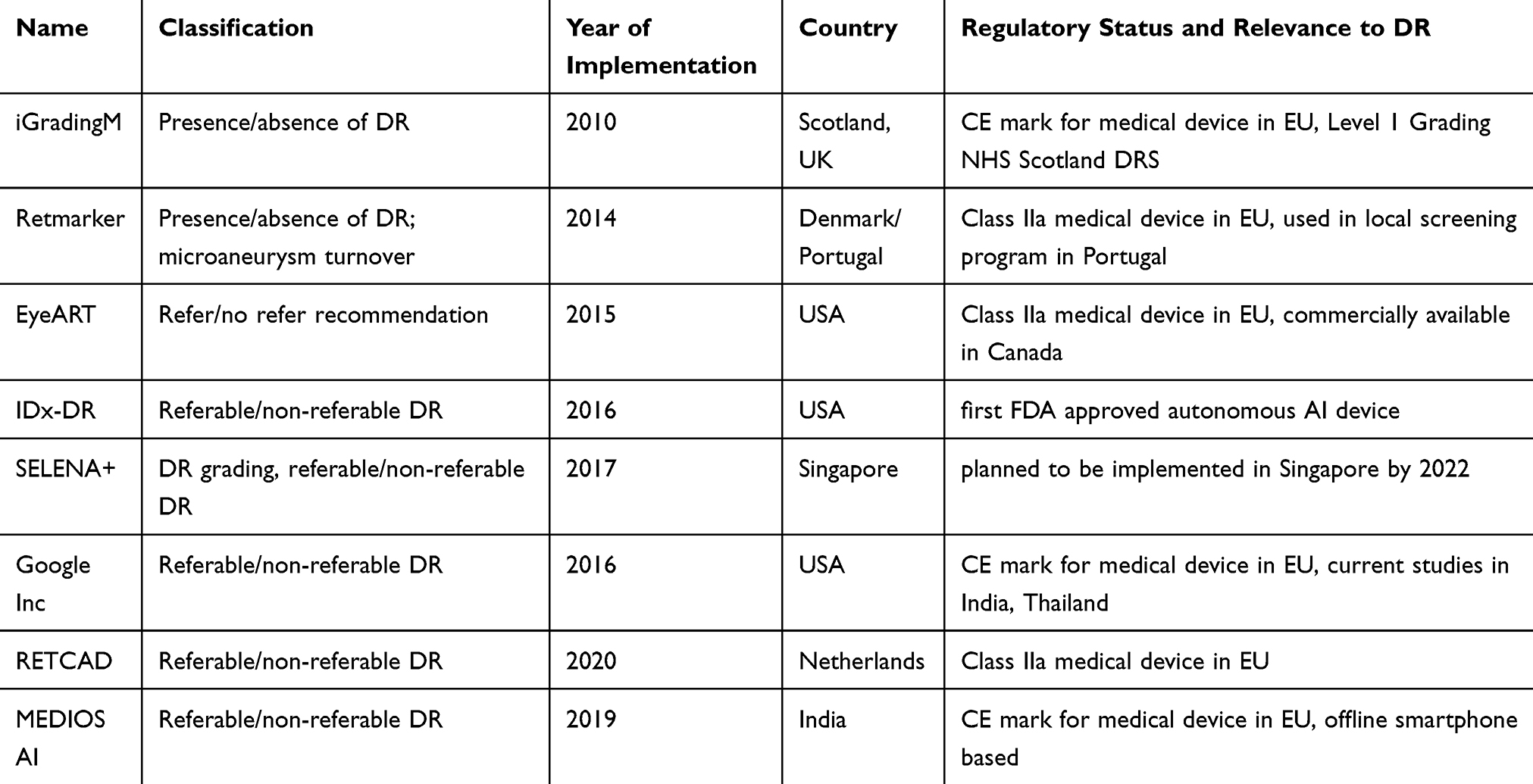 |
Table 2 Overview of Selected Diabetic Retinopathy Clinical Decision Support Systems |
DL research has additionally hinted at the potential benefits of DR screening for disease risk stratification beyond the eye. People suffering from DM have a higher incidence of several complex disorders of ageing, including cardiovascular disease and dementia, which have well-described quantifiable retinal manifestations.100,101 Deep learning, of course, is not limited to detect DR, and, depending on the labels of the images during the training of the model, other outcomes can be evaluated. Poplin et al reported in 2017 a model that was trained with the images and labels of the UK biobank study for prediction of cardiovascular risk factors from CFP using DL. The DL system could detect age with a mean absolute error within 3.26 years, smoking status (AUC 0.71) and sex with an astonishing AUC of 0.97, task retinologists were not able to conquer in 150 years of looking at the fundus.102 Poplin et al reported to have also trained models to detect HbA1c from CFP, however, were limited to the metadata from the datasets included in the study, as HbA1c was only available in one dataset.102 The same group has also developed a model to detect anemia from CFP with an AUC of 0.89, again training on images of the UK biobank study.103 Although only providing proof of concept and lacking robust evaluation, these two examples show the potential benefit of telemedicine screenings for systemic disease evaluation in patients with DR. Oculomics, a term introduced for describing ocular biomarkers for systemic disease, could be of great interest in these systematic and ideally nationwide screenings.104
Clinicians should, however, be aware, that many of the AI-related publications lack reporting standards.105 To address this scarcity, the CONSORT-AI and SPIRIT-AI steering groups are planning to extend the current statement, complementary to current reporting standards as the TRIPOD-ML initiative. It is also important to understand the metrics of the compared methods, and to judge the validation data sets on multiple ethnicities, image quality as well as being aware of flaws in methodology.106–108 So far, only the IDx-DR device has been granted FDA approval and although the promise of DL is big, the clinical value has yet to be robustly evaluated. Few studies in medical images follow a prospective and/or randomised design, and are at higher risk for bias; data and code availability are not given in most studies.
It is worth mentioning that these so-called narrow AI models are trained for specific tasks, and therefore will not be able to detect retinal comorbidities like choroidal melanomas or retinal detachments. These limitations will make human adjudication in ungradable CFPs for the foreseeable future irreplaceable.
With respect to the global distribution of diabetes, it is of paramount importance for the latter, that ARIAS are not only validated in high-income countries to provide further certainty before a potential implementation can be envisioned. This was, for example, undertaken by the groups of Abramoff et al with 6788 images from the Nakuru Eye Study in Kenya, and Bellemo et al in Zambia, validating their model on 76,370 images of 13,099 patients with diabetes.109,110 Gulshan et al conducted a prospective validation of the above mentioned DL system developed by Google inc., and evaluated the performance on data from two eye care centers in India.82,111 The performance was compared to human graders, in a binary fashion for detecting more-than-mild DR (ETDRS level ≥35) or referable diabetic macular edema. With an 88.9%/92.2% sensitivity/specificity and an AUC of 0.963 in one center and a 92.1%/95.2% sensitivity/specificity and an AUC of 0.980 at a second center, the automated DR detection was equal to or succeeded human grading.112
Health Economics
The global pandemic of DR requires efforts on different levels, and epidemiological as well as technical standpoints need to be considered.113 Almost 80% of responders in the DR Barometer study replied that the sight impairment due to their DR and diabetic macular edema make daily life activities including work difficult and sometimes impossible.114 The costs of DR have been shown to rise with the progression of the disease as published in a study by Woung et al in Taiwan,115 and have been calculated to account for 1.5% of the entire healthcare costs in Germany in 2002, estimated to reach 3.51 Billion € in this year.116 The screening for DR with the aim of early detection and timely as well as appropriate referral according to the guidelines has been shown to be cost-effective.117,118 In a systematic review recently published, Lee et al could show, that teleophthalmology is the most cost-effective intervention among all telemedicine strategies in diabetes management.119 Furthermore, the implementation of telemedicine screening when compared to family physician-based screening, both based on fundus imaging has also been shown to be cost-effective.28 The authors concluded, that firstly the costs of grading in a central reading center are lower, and secondly due to higher specificity on the grades less unnecessary referrals were generated. The US Department of Veteran Affairs concluded in a retrospective study that in order to be cost-effective, a DR screening service has to include more than 3500 patients, or patients, who are less than 80 years of age.120 However, offering annual screening to all patients with DM might not be cost-effective, as the number of patients with DM is increasing.121,122 The risk for patients with DM and no evidence of DR to develop sight-threatening DR over a period of 2 years are relatively low, independent of single-field or two field CFP screenings.21 This finding was supported by the analysis of 116,134 patients undergoing DR screening in the US by Kaiser Permanente, the largest private healthcare provider in the US, showing that patients with no or mild DR rarely required retinal intervention in the 2 years after retinal screening.123 By stratifying patients into low risk and high-risk groups due to their repeated findings in the screening services, and subsequent adaptation of the screening intervals, cost reduction could be achieved.122,124 It is, however, unclear how patient behaviour would change under extended screening intervals, giving the patient a wrong impression of the potential damage that can be caused by DR.125
The UK national diabetic eye screening program (NDESP) is by far the largest existing program, having screened 2.257.124 out of 3.175.121 eligible patients alone between 2016 and 2017.26 These images were all graded by trained graders, undergoing thorough training to be eligible, with various levels of adjudication.126 In 2011 the total amount of workload for the human graders in the NDESP was calculated to be greater than 300.000 hours per year for retinal images of roughly 1.700.000 patients.127 This labour-intensive work also contains further potential for reduction of cost. Strategies to improve the cost-effectiveness could include, of course, automated image processing using ARIAS.71,74 Tufail et al presented two strategies for calculating cost-effectiveness of two ARIAS, Retmarker and EyeArt. The grading system in the NDESP contains three levels of graders, with adjudication for different levels of DR.71 In strategy 1, the ARIAS would replace the level 1 grader, in strategy 2 the ARIAS would act as a filter before the level 1 grader. The authors concluded that, if properly implemented, ARIAS could help the impending challenge of DR in both developed and developing countries. In a preprint issued by the Lancet, Xie et al have conducted an economic analysis comparing a semi-automated DL system, a fully automated DL system and the current full human grading model of the SiDRP in Singapore.128 They could show that the semi-automated DL system, which would function as a triage prior to secondary human assessment is equally effective as full human assessment, but less cost-intensive.128 Further assessments of the costs and requirements of transition processes from human-based screening to AI-assisted programs as well as from opportunistic to population-based-programs are warranted.129
Implications for the Future
Most patients with diabetes are not aware of their current status of DR. The National Health and Nutrition Examination Survey (NHANES) in the US, the Andrah Pradesh Eye Disease Study (APEDS) in India and the Singapore Epidemiology of Eye Disease (SEED) Study all found that more than 70% of the patients with diabetes assessed in these studies were not aware of their own DR status.130–132 Due to an increasing global population, the majority of patients with diabetes now live in low- and moderate-income countries, with potentially underfunded healthcare systems.133
The International Diabetes Federation conducted the DR barometer study, with the aim to assess the awareness of DR and the access to care. This study of 2329 healthcare professionals from 41 countries reported several interesting insights: more than a third of diabetes specialists included in the survey reported that they would not discuss eye care with their patients with diabetes. Sufficient information on eye complications was only available of one in five primary care providers. The most substantial barriers to care according to the healthcare professionals were patients´ lack of knowledge or awareness of eye complications in 43%, the lack of importance given to eye examinations by patients in 33% and the high cost of care in 32%. Ophthalmologists included would complain about late screening in 66% and a lack of patient education material in 55%.134 These insights have to be interpreted critically due to the way this study was conducted, and may only give a snapshot of today’s situation.
There is undeniably a need for a global strategy to tackle the burden of DR. Patient education will be as important as raising awareness from the levels of primary care all the way through to tertiary care. Technical advances, as well as lessons learnt from large screening services, may lead the way. Initiatives, such as the Diabetic Retinopathy Network (DR-NET), supported by the VISION 2020 LINKS Programme, provide opportunities for knowledge exchange on the construction of DR screening programmes, best practice on the development of national frameworks and procedures on governance and audit. Another consideration is the advances in technology, particularly in regards to the use of digital cameras as well as cloud-based and offline screening algorithms. It is estimated that 80% of the population of sub-Saharan Africa have a mobile device, and eHealth applications and screening programs could play an important role as healthcare devices.135
Deep-learning systems need to go through robust validation processes in multiethnic cohorts to avoid biases; the ownership of data on a global level is still not regulated.136 The European Union´s General Data Protection Regulation or California´s Consumer Privacy Act are examples of recent regulations to apply rules for data transfer and collection, and may be first steps in the right direction of data protection in a fast-growing online world.137,138 An interesting proposal about the ethics of sharing and using clinical imaging data for AI was put forward by Larson et al, stating that rather than discussing the ownership of data between patients and provider organisations, they propose that clinical data would not be owned at all in a traditional sense.139 Larson et al argue that everybody involved in dealing with the data has an obligation to ensure that the data would be used for the benefit of future patients and society. It is also important to bear in mind that by installing a screening service into an already stretched system with little resources for treatment, strategies from high resource countries will not work. Thus, for instance, criteria for referrable disease could be adapted to focus on those being affected the most.110
Frequently asked questions about these DL systems almost always include the following three: will AI replace ophthalmologists, how can we open the black box, and can these algorithms be sued? The first question was addressed in a recent article by Korot el al, stating that although current AI systems may be good at dealing with high volume data related tasks; however, a clinician´s ability to interpret the complex and multivariate data-driven AI recommendations should be the next step for ophthalmologists.140 The black box problem refers to the interpretability of AI systems, and those end-to-end solutions will not provide insight to the clinicians regarding.141 As these DL systems are providing interesting results, clinicians as well as public health providers would be interested to be able to interpret, and scale the newly discovered insights, for example, individually stratifying certain risk factors. Current strategies of using again AI to analyse these black boxes by using reinforcement learning are providing a prosperous outlook, and hopefully, these black boxes can be turned into white boxes soon.142–144 So, what about the legal aspects of AI, can an algorithm be sued?145 The answer to this question will depend a lot on the regulators and the robust clinical evaluation prior to the approval.
As the current Covid19 pandemic causing global turmoil in 2020 caused by SarsCoV-2 is affecting all continents with an unclear outcome, telemedicine has arisen to the forefront of transforming healthcare delivery models.146,147 In Ophthalmology, the decoupling of clinical data gathering using virtual clinics and explanation of results using video consultations with treatments such as intravitreal injections for diabetic macular oedema will allow the sustained provision of eye care in the new era of social distancing. Not only have virtual clinics proven to be cost-effective and safe, but patients’ acceptance is also high.148,149 Once validated, simple machine learning techniques could support fully automated clinics supporting clinicians for instance by detecting non-glaucomatous visual field defects in virtual glaucoma clinics, hence enhancing patient safety.150 This model not only future proofs eye care provision but provides resilience should a second or third wave pandemic arise. Research in the patient acceptance, efficacy, safety, and cost-efficiency of these pathways will likely, in the coming years, dominate the implementation research fields of Ophthalmology.
Conclusions
The growth in global incident DM rates secondary to ageing populations and rising obesity levels are well recognised. While many parts of the developed world benefit from effective infrastructure for DR screening, there remains a scarcity of similar programmes in the developing world, where over 60% of the global DM burden is thought to exist. Fortunately, novel approaches in hardware and image analysis may afford the opportunities to address this unmet need. The latest imaging devices provide higher resolution and peripheral views previously restricted to clinical examination and the unprecedented technological environment has fostered a vibrant sphere of AI research in DR detection. The rewards of these efforts are beginning to translate into clinical benefit with the approval of some of the first autonomous AI-based DR detection tools. Hardware bears important financial considerations however the permeation of mobile smartphones in the developing world may provide a window of opportunity. Moreover, enhancing global advocacy through partnerships, such as that epitomised by the Vision 2020 LINKS programme, has helped establish robust frameworks for the implementation of DR screening in the developing world. By either engaging with clinicians through telemedicine platforms or cloud-based upload to an AI model, there are indications that we may yet be able to democratize the power of effective DR screening on a global scale.
Acknowledgments
The authors would like to thank Lauren Stafford of Big Picture Medical for the graphical design.
Disclosure
The authors report no conflict of interest in this work.
References
1. Nettleship E. On oedema or cystic disease of the retina. Roy LondHosp Rep VII. 1872;343–351:558.
2. von Graefe A. Ueber die mit Diabetes mellitus vorkommenden Sehstörungen. Dies Arch. 1858;IV(2):230–234.
3. Jaeger E. Beitr zur Pathol des Auges. Wien. 1856:33.
4. Bennett TJ, Barry CJ. Ophthalmic imaging today: an ophthalmic photographer’s viewpoint - a review. Clin Experiment Ophthalmol. 2009;37(1):2–13. doi:10.1111/j.1442-9071.2008.01812.x
5. Bernardes R, Serranho P, Lobo C. Digital ocular fundus imaging: a review. Ophthalmologica. 2011;226(4):161–181. doi:10.1159/000329597
6. Goldberg MF, Jampol LM. Knowledge of diabetic retinopathy before and 18 years after the Airlie house symposium on treatment of diabetic retinopathy. Ophthalmology. 1987;94(7):741–746. doi:10.1016/S0161-6420(87)33524-9
7. Early Treatment Diabetic Retinopathy Study Research Group. Grading Diabetic Retinopathy from Stereoscopic Color Fundus Photographs — an Extension of the Modified Airlie House Classification. Ophthalmology. 2020;127(4):S99–S119. doi:10.1016/j.ophtha.2020.01.030
8. Solomon SD, Goldberg MF. ETDRS grading of diabetic retinopathy: still the gold standard? Ophthalmic Res. 2019;62(4):190–195. doi:10.1159/000501372
9. Ogurtsova K, da Rocha Fernandes JD, Huang Y, et al. IDF diabetes atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. 2017;128:40–50. doi:10.1016/j.diabres.2017.03.024
10. Yau JWY, Rogers SL, Kawasaki R, et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35(3):556–564. doi:10.2337/dc11-1909
11. Rees G, Xie J, Fenwick EK, et al. Association between diabetes-related eye complications and symptoms of anxiety and depression. JAMA Ophthalmol. 2016;134(9):1007. doi:10.1001/jamaophthalmol.2016.2213
12. Fenwick EK, Xie J, Ratcliffe J, et al. The impact of diabetic retinopathy and diabetic macular edema on health-related quality of life in type 1 and type 2 diabetes. Invest Ophthalmol Visual Sci. 2012;53(2):677. doi:10.1167/iovs.11-8992
13. Cooper OAE, Taylor DJ, Crabb DP, Sim DA, McBain H. Psychological, social and everyday visual impact of diabetic macular oedema and diabetic retinopathy: a systematic review. Diabetic Med. 2019. doi:10.1111/dme.14125
14. PRINCIPLES AND PRACTICE OF SCREENING FOR DISEASE. Available from: https://apps.who.int/iris/bitstream/handle/10665/37650/WHO_PHP_34.pdf?sequence=17&isAllowed=y. Accessed February 23, 2020.
15. Harding S, Greenwood R, Aldington S, et al. Grading and disease management in national screening for diabetic retinopathy in England and Wales. Diabetic Med. 2003;20(12):965–971. doi:10.1111/j.1464-5491.2003.01077.x
16. Lim MCC, Lee SY, Cheng BCL, et al. Diabetic retinopathy in diabetics referred to a tertiary centre from a nationwide screening programme. Ann Acad Med Singapore. 2008;37(9):753–759.
17. Cuadros J. EyePACS - adapting telemedicine for diabetic retinopathy screening in primary diabetes care settings. J Diabetes Metab. 2010;01(01):01. doi:10.4172/2155-6156.1000024
18. Pieczynski J, Grzybowski A. Chair of ophthalmology review of diabetic retinopathy screening methods and programmes adopted in different parts of the world. Eur Ophthalmic Rev. 2015;09(01):49. doi:10.17925/eor.2015.09.01.49
19. Kristinsson JK, Stefánsson E, Jónasson F, Gíslason I, Björnsson S. Systematic screening for diabetic eye disease in insulin dependent diabetes. Acta Ophthalmol (Copenh). 2009;72(1):72–78. doi:10.1111/j.1755-3768.1994.tb02741.x
20. Kristinsson JK, Stefánsson E, Jónasson F, Gislason I, Björnsson S. Screening for eye disease in type 2 diabetes mellitus. Acta Ophthalmol (Copenh). 2009;72(3):341–346. doi:10.1111/j.1755-3768.1994.tb02770.x
21. Scanlon PH. Screening Intervals for Diabetic Retinopathy and Implications for Care. Curr Diab Rep. 2017;17(10):96. doi:10.1007/s11892-017-0928-6
22. Agardh E-D, Agardh C, Hansson-Lundblad C. The five-year incidence of blindness after introducing a screening programme for early detection of treatable diabetic retinopathy. Diabetic Med. 1993;10(6):555–559. doi:10.1111/j.1464-5491.1993.tb00120.x
23. Bäcklund LB, Algvere PV, Rosenqvist U. New blindness in diabetes reduced by more than one-third in Stockholm County. Diabet Med. 1997;14(9):732–740. doi:10.1002/(SICI)1096-9136(199709)14:9<732::AID-DIA474>3.0.CO;2-J
24. British Diabetic Association. Retinal Photography Screening for Diabetic Eye Disease. A British Diabetic Association Report. London: British Diabetic Association; 1997.
25. Scanlon PH. The English National Screening Programme for diabetic retinopathy 2003–2016. Acta Diabetol. 2017;54(6):515. doi:10.1007/s00592-017-0974-1
26. Diabetic eye screening annual data tables 2016 to 2017. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/720462/Diabetic_eye_screening_annual_data_tables_2016_to_2017.xlsx. Accessed July 3, 2020
27. Liew G, Michaelides M, Bunce C. A comparison of the causes of blindness certifications in England and Wales in working age adults (16–64 years), 1999–2000 with 2009–2010. BMJ Open. 2014;4(2):e004015. doi:10.1136/bmjopen-2013-004015
28. Nguyen HV, Tan GSW, Tapp RJ, et al. Cost-effectiveness of a national telemedicine diabetic retinopathy screening program in Singapore. Ophthalmology. 2016;123(12):2571–2580. doi:10.1016/j.ophtha.2016.08.021
29. Mak DB, Plant AJ, McAllister I. Screening for diabetic retinopathy in remote Australia: a program description and evaluation of a devolved model. Aust J Rural Health. 2003;11(5):224–230.
30. Schulze-Döbold C, Erginay A, Robert N, Chabouis A, Massin P. Ophdiat®: five-year experience of a telemedical screening programme for diabetic retinopathy in Paris and the surrounding area. Diabetes Metab. 2012;38(5):450–457. doi:10.1016/j.diabet.2012.05.003
31. Lemmetty R, Mäkelä K. Mobile digital fundus screening of type 2 diabetes patients in the Finnish county of South-Ostrobothnia. J Telemed Telecare. 2009;15(2):68–72. doi:10.1258/jtt.2008.080804
32. Boucher MC, Desroches G, Garcia-Salinas R, et al. Teleophthalmology screening for diabetic retinopathy through mobile imaging units within Canada. Can J Ophthalmol. 2008;43(6):658–668. doi:10.3129/i08-120
33. Jani PD, Forbes L, Choudhury A, Preisser JS, Viera AJ, Garg S. Evaluation of diabetic retinal screening and factors for ophthalmology referral in a telemedicine network. JAMA Ophthalmol. 2017;135(7):706. doi:10.1001/jamaophthalmol.2017.1150
34. Cuadros J, Bresnick G. EyePACS: an adaptable telemedicine system for diabetic retinopathy screening. J Diabetes Sci Technol. 2009;3(3):509–516.
35. Verma L, Prakash G, Tewari HK, Gupta SK, Murthy GVS, Sharma N. Screening for diabetic retinopathy by non-ophthalmologists: an effective public health tool. Acta Ophthalmol Scand. 2003;81(4):373–377. doi:10.1034/j.1600-0420.2003.00004.x
36. Sanchez CR, Silva PS, Cavallerano JD, Aiello LP, Aiello LM. Ocular telemedicine for diabetic retinopathy and the Joslin Vision Network. Semin Ophthalmol. 2010;25(5–6):218–224. doi:10.3109/08820538.2010.518893
37. Pareja-Ríos A, Bonaque-González S, Serrano-García M, Cabrera-López F, Abreu-Reyes P, Marrero-Saavedra MD. Tele-ophthalmology for diabetic retinopathy screening: 8 years of experience. Arch Soc Esp Oftalmol. 2017;92(2):63–70. doi:10.1016/j.oftal.2016.08.006
38. Zimmer-Galler I, Zeimer R. Results of implementation of the DigiScope for diabetic retinopathy assessment in the primary care environment. Telemed J E Health. 2006;12(2):89–98. doi:10.1089/tmj.2006.12.89
39. Mansberger SL, Sheppler C, Barker G, et al. Long-term comparative effectiveness of telemedicine in providing diabetic retinopathy screening examinations: a randomized clinical trial. JAMA Ophthalmol. 2015;133(5):518–525. doi:10.1001/jamaophthalmol.2015.1
40. Gupta A, Cavallerano J, Sun JK, Silva PS. Evidence for Telemedicine for Diabetic Retinal Disease. Semin Ophthalmol. 2017;32(1):22–28. doi:10.1080/08820538.2016.1228403
41. Diabetic retinopathy study. Report Number 6. Design, methods, and baseline results. Report number 7. A modification of the Airlie house classification of diabetic retinopathy. Prepared by the diabetic retinopathy. Invest Ophthalmol Vis Sci. 1981;21(1):147–226.
42. Diabetic Retinopathy Study Research Grou. Photocoagulation treatment of proliferative diabetic retinopathy: clinical application of diabetic retinopathy study (DRS) findings, DRS report number 8. Ophthalmology. 1981;88(7):583–600. doi:10.1016/S0161-6420(81)34978-1
43. ETDRSR Group. Grading diabetic retinopathy from stereoscopic color fundus photographs—an extension of the modified Airlie house classification. Ophthalmology. 1991;98(5):786–806. doi:10.1016/s0161-6420(13)38012-9
44. Lin DY, Blumenkranz MS, Brothers RJ, Grosvenor DM. The sensitivity and specificity of single-field nonmydriatic monochromatic digital fundus photography with remote image interpretation for diabetic retinopathy screening: a comparison with ophthalmoscopy and standardized mydriatic color photography11InternetAdvance publication at ajo.com. April 12, 2002. Am J Ophthalmol. 2002;134(2):204–213. doi:10.1016/s0002-9394(02)01522-2
45. Vujosevic S, Benetti E, Massignan F, et al. Screening for diabetic retinopathy: 1 and 3 nonmydriatic 45-degree digital fundus photographs vs 7 standard early treatment diabetic retinopathy study fields. Am J Ophthalmol. 2009;148(1):111–118. doi:10.1016/j.ajo.2009.02.031
46. Aptel F, Denis P, Rouberol F, Thivolet C. Screening of diabetic retinopathy: effect of field number and mydriasis on sensitivity and specificity of digital fundus photography. Diabetes Metab. 2008;34(3):290–293. doi:10.1016/j.diabet.2007.12.007
47. Piyasena MMPN, Murthy GVS, Yip JLY, et al. Systematic review and meta-analysis of diagnostic accuracy of detection of any level of diabetic retinopathy using digital retinal imaging. Syst Rev. 2018;7(1):182. doi:10.1186/s13643-018-0846-y
48. Scanlon PH, Malhotra R, Greenwood RH, et al. Comparison of two reference standards in validating two field mydriatic digital photography as a method of screening for diabetic retinopathy. Br J Ophthalmol. 2003;87(10):1258–1263. doi:10.1136/bjo.87.10.1258
49. Gangaputra S, Almukhtar T, Glassman AR, et al. Comparison of film and digital fundus photographs in eyes of individuals with diabetes mellitus. Invest Ophthalmol Vis Sci. 2011;52(9):6168–6173. doi:10.1167/iovs.11-7321
50. Scanlon PH, Foy C, Malhotra R, Aldington SJ. The influence of age, duration of diabetes, cataract, and pupil size on image quality in digital photographic retinal screening. Diabetes Care. 2005;28(10):2448–2453. doi:10.2337/diacare.28.10.2448
51. Liew G, Mitchell P, Wang JJ, Wong TY. Fundoscopy: to dilate or not to dilate? BMJ. 2006;332(7532):3. doi:10.1136/bmj.332.7532.3
52. NDRS Recommendations for Implementing DRS. Available from: https://www.ndrs.scot.nhs.uk/wp-content/uploads/2013/04/Recommendations-for-Implementing-DRS.pdf. Accessed July 3, 2020
53. Abràmoff MD, Lavin PT, Birch M, Shah N, Folk JC. Pivotal trial of an autonomous AI-based diagnostic system for detection of diabetic retinopathy in primary care offices. NPJ Digit Med. 2018;1(1):39. doi:10.1038/s41746-018-0040-6
54. Silva PS, Cavallerano JD, Haddad NMN, et al. Comparison of nondiabetic retinal findings identified with nonmydriatic fundus photography vs ultrawide field imaging in an ocular telehealth program. JAMA Ophthalmol. 2016;134(3):330. doi:10.1001/jamaophthalmol.2015.5605
55. Zeiss Clarus. Available from: https://www.zeiss.com/content/dam/Meditec/us/products/clarus-700/documents/clarus700_brochure_usa_cam11445.pdf. Accessed March 1, 2020.
56. EIDON - First True Color Confocal Scanner - CenterVue. CenterVue. Available from: https://www.centervue.com/products/eidon/. Accessed March 1, 2020.
57. Olvera-Barrios A, Heeren TF, Balaskas K, et al. Comparison of true-colour wide-field confocal scanner imaging with standard fundus photography for diabetic retinopathy screening. Br J Ophthalmol. 2020:
58. Rajalakshmi R, Arulmalar S, Usha M, et al. Validation of smartphone based retinal photography for diabetic retinopathy screening. PLoS One. 2015;10(9):e0138285. doi:10.1371/journal.pone.0138285
59. Sengupta S, Sindal MD, Baskaran P, Pan U, Venkatesh R. Sensitivity and Specificity of smartphone-based retinal imaging for diabetic retinopathy: a comparative study. Ophthalmol Retina. 2019;3(2):146–153. doi:10.1016/j.oret.2018.09.016
60. Matsui M, Tashiro T, Matsumoto K, Yamamoto S. [A study on automatic and quantitative diagnosis of fundus photographs. I. Detection of contour line of retinal blood vessel images on color fundus photographs (author’s transl)]. Nihon Ganka Gakkai Zasshi. 1973;77(8):907–918. Japanes.
61. Baudoin CE, Lay BJ, Klein JC. Automatic detection of microaneurysms in diabetic fluorescein angiography. Rev Epidemiol Sante Publique. 1984;32(3–4):254–261.
62. Li HK, Horton M, Bursell S-E, et al. Telehealth practice recommendations for diabetic retinopathy, second edition. Telemed J E Health. 2011;17(10):814. doi:10.1089/tmj.2011.0075
63. Al SPS et. Telemedicine and diabetic retinopathy: moving beyond retinal screening. - PubMed - NCBI. Arch Ophthalmol. 2011. https://www.ncbi.nlm.nih.gov/pubmed/21320974.
64. Patton N, Aslam TM, MacGillivray T, et al. Retinal image analysis: concepts, applications and potential. Prog Retin Eye Res. 2006;25(1):99–127. doi:10.1016/j.preteyeres.2005.07.001
65. Antal B, Hajdu A. An ensemble-based system for microaneurysm detection and diabetic retinopathy grading. IEEE Trans Biomed Eng. 2012;59(6):1720–1726. doi:10.1109/TBME.2012.2193126
66. Fleming AD, Goatman KA, Philip S, et al. The role of haemorrhage and exudate detection in automated grading of diabetic retinopathy. Br J Ophthalmol. 2010;94(6):706–711. doi:10.1136/bjo.2008.149807
67. Quellec G, Lamard M, Cazuguel G, et al. Automated assessment of diabetic retinopathy severity using content-based image retrieval in multimodal fundus photographs. Invest Ophthalmol Visual Sci. 2011;52(11):8342. doi:10.1167/iovs.11-7418
68. Abràmoff MD, Folk JC, Han DP, et al. Automated analysis of retinal images for detection of referable diabetic retinopathy. JAMA Ophthalmol. 2013;131(3):351. doi:10.1001/jamaophthalmol.2013.1743
69. Soto-Pedre E, Navea A, Millan S, et al. Evaluation of automated image analysis software for the detection of diabetic retinopathy to reduce the ophthalmologists’ workload. Acta Ophthalmol (Copenh). 2015;93(1):e52–e56. doi:10.1111/aos.12481
70. Goatman K, Charnley A, Webster L, Nussey S. Assessment of automated disease detection in diabetic retinopathy screening using two-field photography. PLoS One. 2011;6(12):e27524. doi:10.1371/journal.pone.0027524
71. Tufail A, Rudisill C, Egan C, et al. Automated diabetic retinopathy image assessment software: diagnostic accuracy and cost-effectiveness compared with human graders. Ophthalmology. 2017;124(3):343–351. doi:10.1016/j.ophtha.2016.11.014
72. Philip S, Fleming AD, Goatman KA, et al. The efficacy of automated “disease/no disease” grading for diabetic retinopathy in a systematic screening programme. Br J Ophthalmol. 2007;91(11):1512–1517. doi:10.1136/bjo.2007.119453
73. Fleming AD, Goatman KA, Philip S, Prescott GJ, Sharp PF, Olson JA. Automated grading for diabetic retinopathy: a large-scale audit using arbitration by clinical experts. Br J Ophthalmol. 2010;94(12):1606–1610. doi:10.1136/bjo.2009.176784
74. Fleming AD, Philip S, Goatman KA, Prescott GJ, Sharp PF, Olson JA. The Evidence for automated grading in diabetic retinopathy screening. Curr Diabetes Rev. 2011;7(4):246–252. doi:10.2174/157339911796397802
75. Teng T, Lefley M, Claremont D. Progress towards automated diabetic ocular screening: A review of image analysis and intelligent systems for diabetic retinopathy. Med Biol Eng Comput. 2002;40(1):2–13. doi:10.1007/bf02347689
76. Mookiah MRK, Rajendra Acharya U, Chua CK, Lim CM, Ng EYK, Laude A. Computer-aided diagnosis of diabetic retinopathy: A review. Comput Biol Med. 2013;43(12):2136–2155. doi:10.1016/j.compbiomed.2013.10.007
77. Li B, Li HK. Automated analysis of diabetic retinopathy images: principles, recent developments, and emerging trends. Curr Diab Rep. 2013;13(4):453–459. doi:10.1007/s11892-013-0393-9
78. Carin L, Pencina MJ. On deep learning for medical image analysis. JAMA. 2018;320(11):1192–1193. doi:10.1001/jama.2018.13316
79. LeCun Y, Bengio Y, Hinton G. Deep learning. Nature. 2015;521(7553):436–444. doi:10.1038/nature14539
80. Krizhevsky A, Sutskever I, Hinton GE. ImageNet classification with deep convolutional neural networks. Commun ACM. 2017;60(6):84–90. doi:10.1145/3065386
81. He K, Zhang X, Ren S, Sun J Deep Residual Learning for Image Recognition.
82. Gulshan V, Peng L, Coram M, et al. Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. JAMA. 2016;316(22):2402. doi:10.1001/jama.2016.17216
83. Hinton G, Deng L, Yu D, et al. Deep neural networks for acoustic modeling in speech recognition: the shared views of four research groups. IEEE Signal Process Mag. 2012;29(6):82–97. doi:10.1109/msp.2012.2205597
84. Zhang X, Zou J, He K, Sun J. Accelerating Very Deep Convolutional Networks for Classification and Detection. IEEE Trans Pattern Anal Mach Intell. 2016;38(10):1943–1955. doi:10.1109/tpami.2015.2502579
85. Shin H-C, Roth HR, Gao M, et al. Deep Convolutional neural networks for computer-aided detection: CNN architectures, dataset characteristics and transfer learning. IEEE Trans Med Imaging. 2016;35(5):1285–1298. doi:10.1109/tmi.2016.2528162
86. Liu X, Faes L, Kale AU, et al. A comparison of deep learning performance against health-care professionals in detecting diseases from medical imaging: a systematic review and meta-analysis. Lancet Digital Health. 2019;1(6):e271–e297. doi:10.1016/s2589-7500(19)30123-2
87. De Fauw J, Ledsam JR, Romera-Paredes B, et al. Clinically applicable deep learning for diagnosis and referral in retinal disease. Nat Med. 2018;24(9):1342–1350. doi:10.1038/s41591-018-0107-6
88. Abràmoff MD, Lou Y, Erginay A, et al. Improved automated detection of diabetic retinopathy on a publicly available dataset through integration of deep learning. Invest Ophthalmol Vis Sci. 2016;57(13):5200–5206. doi:10.1167/iovs.16-19964
89. Heijden AA, van Der, van der Heijden AA, Abramoff MD, et al. Validation of automated screening for referable diabetic retinopathy with the IDx-DR device in the hoorn diabetes care system. Acta Ophthalmol (Copenh). 2018;96(1):63–68. doi:10.1111/aos.13613
90. Schmidt-Erfurth U, Sadeghipour A, Gerendas BS, Waldstein SM, Bogunović H. Artificial intelligence in retina. Prog Retin Eye Res. 2018;67:1–29. doi:10.1016/j.preteyeres.2018.07.004
91. Song, B.J., Aiello, L.P. and Pasquale, L.R. Presence and Risk Factors for Glaucoma in Patients with Diabetes. - PubMed - NCBI. Curr Diab Rep. 2016:16;124.
92. Ting DSW, Cheung CY-L, Lim G, et al. Development and validation of a deep learning system for diabetic retinopathy and related eye diseases using retinal images from multiethnic populations with diabetes. JAMA. 2017;318(22):2211–2223. doi:10.1001/jama.2017.18152
93. EyRIS. Available from: https://www.eyris.io/technology.cfm. Accessed June 16, 2020.
94. Singapore’s national AI strategy to focus on chronic disease management and prevention. Healthcare IT News. Available from: https://www.healthcareitnews.com/news/asia-pacific/singapore-s-national-ai-strategy-focus-chronic-disease-management-and-prevention. Accessed April 9, 2020.
95. Bhaskaranand M, Ramachandra C, Bhat S, et al. The value of automated diabetic retinopathy screening with the EyeArt system: a study of more than 100,000 consecutive encounters from people with diabetes. Diabetes Technol Ther. 2019;21(11):635–643. doi:10.1089/dia.2019.0164
96. Natarajan S, Jain A, Krishnan R, Rogye A, Sivaprasad S. Diagnostic Accuracy of community-based diabetic retinopathy screening with an offline artificial intelligence system on a smartphone. JAMA Ophthalmol. 2019;137(10):1182. doi:10.1001/jamaophthalmol.2019.2923
97. González-Gonzalo C, Sánchez-Gutiérrez V, Hernández-Martínez P, et al. Evaluation of a deep learning system for the joint automated detection of diabetic retinopathy and age-related macular degeneration. Acta Ophthalmol. 2020;98(4):368–377. doi:10.1111/aos.14306
98. Sengupta S, Singh A, Leopold HA, Gulati T, Lakshminarayanan V. Ophthalmic diagnosis using deep learning with fundus images – A critical review. Artif Intell Med. 2020;102:101758. doi:10.1016/j.artmed.2019.101758
99. Grzybowski A, Brona P, Lim G, et al. Artificial intelligence for diabetic retinopathy screening: a review. Eye. 2020;34(3):451–460. doi:10.1038/s41433-019-0566-0
100. Biessels GDF, Despa F. Cognitive decline and dementia in diabetes mellitus: mechanisms and clinical implications. Nat Rev Endocrinol. 2018;14(10):591–604. doi:10.1038/s41574-018-0048-7
101. Henning RJ. Type-2 diabetes mellitus and cardiovascular disease. Future Cardiol. 2018;14(6):491–509. doi:10.2217/fca-2018-0045
102. Poplin R, Varadarajan AV, Blumer K, et al. Prediction of cardiovascular risk factors from retinal fundus photographs via deep learning. Nat Biomed Eng. 2018;2(3):158–164. doi:10.1038/s41551-018-0195-0
103. Mitani A, Huang A, Venugopalan S, et al. Detection of anaemia from retinal fundus images via deep learning. Nat Biomed Eng. 2020;4(1):18–27. doi:10.1038/s41551-019-0487-z
104. Wagner SK, Fu DJ, Faes L, et al. Insights into systemic disease through retinal imaging-based oculomics. Transl Vis Sci Technol. 2020;9(2):6. doi:10.1167/tvst.9.2.6
105. Chalmers I, Glasziou P, Heneghan C, Shepperd S, Loudon K, Bossuyt PM. Reporting guidelines for clinical trials evaluating artificial intelligence interventions are needed. Nat Med. 2019;25(10):1467–1468.
106. Faes L, Liu X, Wagner SK, et al. A clinician’s guide to artificial intelligence: how to critically appraise machine learning studies. Transl Vis Sci Technol. 2020;9(2):7. doi:10.1167/tvst.9.2.7
107. Ting DSW, Peng L, Varadarajan AV, et al. Deep learning in ophthalmology: the technical and clinical considerations. Prog Retin Eye Res. 2019;72:100759. doi:10.1016/j.preteyeres.2019.04.003
108. Liu Y, Chen P-HC, Krause J, Peng L. How to Read Articles That Use Machine Learning: users’ Guides to the Medical Literature. JAMA. 2019;322(18):1806–1816. doi:10.1001/jama.2019.16489
109. Hansen MB, Abràmoff MD, Folk JC, Mathenge W, Bastawrous A, Peto T. Results of automated retinal image analysis for detection of diabetic retinopathy from the nakuru study, Kenya. PLoS One. 2015;10(10):e0139148. doi:10.1371/journal.pone.0139148
110. Bellemo V, Lim ZW, Lim G, et al. Artificial intelligence using deep learning to screen for referable and vision-threatening diabetic retinopathy in Africa. SSRN Electronic J. 2019;1:e35. doi:10.2139/ssrn.3324738
111. Gulshan V, Rajan RP, Widner K, et al. Performance of a deep-learning algorithm vs manual grading for detecting diabetic retinopathy in India. JAMA Ophthalmol. 2019:June. doi:10.1001/jamaophthalmol.2019.2004
112. Nagendran M, Chen Y, Lovejoy CA, et al. Artificial intelligence versus clinicians: systematic review of design, reporting standards, and claims of deep learning studies. BMJ. 2020;368:m689. doi:10.1136/bmj.m689
113. Wong TY, Sabanayagam C. Strategies to tackle the global burden of diabetic retinopathy: from epidemiology to artificial intelligence. Ophthalmologica. 2020;243(1):9–20. doi:10.1159/000502387
114. Barometer DR - Shifting the needle. DR Barometer. Available from: https://drbarometer.com. Accessed April 22, 2020.
115. Woung L-C, Tsai C-Y, Chou H-K, et al. Healthcare costs associated with progressive diabetic retinopathy among National Health Insurance enrollees in Taiwan, 2000–2004. BMC Health Serv Res. 2010;10(1):136. doi:10.1186/1472-6963-10-136
116. Happich M, Reitberger U, Breitscheidel L, Ulbig M, Watkins J. The economic burden of diabetic retinopathy in Germany in 2002. Graefes Arch Clin Exp Ophthalmol. 2008;246(1):151–159. doi:10.1007/s00417-007-0573-x
117. Wong TY, Sun J, Kawasaki R, et al. Guidelines on diabetic eye care: the international council of ophthalmology recommendations for screening, follow-up, referral, and treatment based on resource settings. Ophthalmology. 2018;125(10):1608–1622. doi:10.1016/j.ophtha.2018.04.007
118. Pasquel FJ, Hendrick AM, Ryan M, Cason E, Ali MK, Narayan KMV. Cost-effectiveness of different diabetic retinopathy screening modalities. J Diabetes Sci Technol. 2015;10(2):301–307. doi:10.1177/1932296815624109
119. Lee JY. Telemedicine Cost-Effectiveness for Diabetes Management: A Systematic Review. - PubMed - NCBI. Diabetes Technol Ther. 2018. https://www.ncbi.nlm.nih.gov/pubmed/29812965
120. Kirkizlar E, Serban N, Sisson JA, Swann JL, Barnes CS, Williams MD. Evaluation of telemedicine for screening of diabetic retinopathy in the Veterans Health Administration. Ophthalmology. 2013;120(12):2604–2610. doi:10.1016/j.ophtha.2013.06.029
121. Vijan S. Cost-utility analysis of screening intervals for diabetic retinopathy in patients with type 2 diabetes mellitus. JAMA. 2000;283(7):889. doi:10.1001/jama.283.7.889
122. Scanlon PH, Aldington SJ, Leal J, et al. Development of a cost-effectiveness model for optimisation of the screening interval in diabetic retinopathy screening. Health Technol Assess. 2015;19(74):1–116. doi:10.3310/hta19740
123. Modjtahedi BS, Theophanous C, Chiu S, Luong TQ, Nguyen N, Fong DS. Two-year incidence of retinal intervention in patients with minimal or no diabetic retinopathy on telemedicine screening. JAMA Ophthalmol. 2019;137(4):445. doi:10.1001/jamaophthalmol.2018.6912
124. Lund SH, Aspelund T, Kirby P, et al. Individualised risk assessment for diabetic retinopathy and optimisation of screening intervals: a scientific approach to reducing healthcare costs. Br J Ophthalmol. 2016;100(5):683–687. doi:10.1136/bjophthalmol-2015-307341
125. Klein R. Screening interval for retinopathy in type 2 diabetes. Lancet. 2003;361(9353):190–191. doi:10.1016/S0140-6736(03)12317-3
126. The Management of Grading. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/512832/The_Management_of_Grading.pdf. Accessed April 13, 2020.
127. Sim DA, Keane PA, Tufail A, Egan CA, Aiello LP, Silva PS. Automated retinal image analysis for diabetic retinopathy in telemedicine. Curr Diab Rep. 2015;15(3):14. doi:10.1007/s11892-015-0577-6
128. Xie Y, Nguyen QD, Lim G, et al. Artificial intelligence for teleophthalmology-based diabetic retinopathy screening in a national program: a modelledn economic analysis study. SSRN Electronic J. 2020. doi:10.2139/ssrn.3498440
129. Xie Y, Gunasekeran DV, Balaskas K, et al. Health Economic and Safety Considerations for Artificial Intelligence Applications in Diabetic Retinopathy Screening. Transl Vis Sci Technol. 2020;9(2):22. doi:10.1167/tvst.9.2.22
130. Huang OS, Tay WT, Ong PG, et al. Prevalence and determinants of undiagnosed diabetic retinopathy and vision-threatening retinopathy in a multiethnic Asian cohort: the Singapore Epidemiology of Eye Diseases (SEED) study. Br J Ophthalmol. 2015;99(12):1614–1621. doi:10.1136/bjophthalmol-2014-306492
131. Kiefer MM, Silverman JB, Young BA, Nelson KM. National patterns in diabetes screening: data from the National Health and Nutrition Examination Survey (NHANES) 2005–2012. J Gen Intern Med. 2015;30(5):612–618. doi:10.1007/s11606-014-3147-8
132. Dandona R, Dandona L, Naduvilath TJ, McCarty CA, Rao GN. Awareness of eye donation in an urban population in India. Aust N Z J Ophthalmol. 1999;27(3–4):166–169. doi:10.1046/j.1440-1606.1999.00196.x
133. Ruta LM, Magliano DJ, LeMesurier R, Taylor HR, Zimmet PZ, Shaw JE. Prevalence of diabetic retinopathy in Type 2 diabetes in developing and developed countries. Diabetic Med. 2013;30(4):387–398. doi:10.1111/dme.12119
134. Cavan D, Makaroff LE, da Rocha Fernandes J, et al. Global perspectives on the provision of diabetic retinopathy screening and treatment: survey of health care professionals in 41 countries. Diabetes Res Clin Pract. 2018;143:170–178. doi:10.1016/j.diabres.2018.07.004
135. Africa smartphone penetration at tipping point - Qelp, a SYKES company. Qelp, a SYKES company. Available from: https://www.qelp.com/africa-smartphone-penetration-at-tipping-point/.Accessed April 22, 2020.
136. Panch T, Mattie H, Celi LA. The “inconvenient truth” about AI in healthcare. Npj Digital Med. 2019;2(1):1–3. doi:10.1038/s41746-019-0155-4
137. European union´s general data protection regulation. Available from: https://eur-lex.europa.eu/legal-content/EN/ALL/?uri=CELEX:32016R0679(2016). Accessed June 16, 2020.
138. California´s Consumer Privacy Act. Available from: https://leginfo.legislature.ca.gov/faces/billTextClient.xhtml?bill_id=201720180AB375. Accessed June 16, 2020.
139. Larson DB, Magnus DC, Lungren MP, Shah NH, Langlotz CP. Ethics of using and sharing clinical imaging data for artificial intelligence: a proposed framework. Radiology. 2020;192536.
140. Korot E, Wagner SK, Faes L, et al. Will AI Replace Ophthalmologists? Transl Vis Sci Technol. 2020;9(2):2. doi:10.1167/tvst.9.2.2
141. Lancet Respiratory Medicine T, The Lancet Respiratory Medicine. Opening the black box of machine learning. Lancet Respir Med. 2018;6(11):801. doi:10.1016/S2213-2600(18)30425-9
142. Yoon J, Jordon J, van der Schaar M. INVASE: instance-wise Variable Selection using Neural Networks. Int Conf Learn Represent. 2018. https://openreview.net/pdf?id=BJg_roAcK7.
143. From black boxes to white boxes. Available from: https://www.linkedin.com/pulse/from-black-boxes-white-mihaela-van-der-schaar. Accessed April 16, 2020.
144. Van der Schaar Lab. Available from: http://www.vanderschaar-lab.com/papers/NIPS2019_DBM.pdf. Accessed April 16, 2020.
145. Jha S, Allen JG, Christiani D, et al. Can an artificial intelligence algorithm be sued for malpractice? - STAT. STAT. Available from: https://www.statnews.com/2020/03/09/can-you-sue-artificial-intelligence-algorithm-for-malpractice/.Accessed April 16, 2020.
146. Sim D, Thomas P, Canning C. Tackling COVID-19 with Telemedicine. Ophthalmologist. https://theophthalmologist.com/subspecialties/tackling-covid-19-with-telemedicine. Accessed, 2020
147. Ting DSW, Carin L, Dzau V, Wong TY. Digital technology and COVID-19. Nat Med. 2020;26(4):459–461. doi:10.1038/s41591-020-0824-5
148. Kortuem K, Fasler K, Charnley A, et al. Implementation of medical retina virtual clinics in a tertiary eye care referral centre. Br J Ophthalmol. 2018;102(10):1391–1395. doi:10.1136/bjophthalmol-2017-311494
149. Kern C, Kortuem K, Hamilton R, et al. Clinical outcomes of a hospital-based teleophthalmology service: what happens to patients in a virtual clinic? Ophthalmol Retina. 2019;3(5):422–428. doi:10.1016/j.oret.2019.01.011
150. Thomas PBM, Chan T, Nixon T, Muthusamy B, White A. Feasibility of simple machine learning approaches to support detection of non-glaucomatous visual fields in future automated glaucoma clinics. Eye. 2019;33(7):1133–1139. doi:10.1038/s41433-019-0386-2
151. Diabetic eye screening annual data tables 2016 to 2017. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/720462/Diabetic_eye_screening_annual_data_tables_2016_to_2017.xlsx.
152. Diabetic retinopathy screening (DRS) in Scotland. Available from: https://www.nhsinform.scot/healthy-living/screening/diabetic-retinopathy/diabetic-retinopathy-screening-drs. Accessed April 16, 2020.
153. Public Health Wales Observatory. Public Health Wales Observatory - Diabetic Eye Screening Wales Publishes First Annual Statistical Report 2017-18. February 2019. Available from: http://www.publichealthwalesobservatory.wales.nhs.uk/news/50464.
154. Northern Ireland diabetic eye screening programme. Available from: https://www.publichealth.hscni.net/sites/default/files/2018-12/NIDESP%20Annual%20Report%201617%20Final260618.pdf. Accessed April 16, 2020.
155. Nguyen HV, Tan GSW, Tapp RJ, et al. Cost-effectiveness of a National Telemedicine Diabetic Retinopathy Screening Program in Singapore. Ophthalmology. 2016;123(12):2571–2580. doi:10.1016/j.ophtha.2016.08.021
156. Kristinsson, J.K., Stefánsson, E., Jónasson, F., Gislason, I. Screening for eye disease in type 2 diabetes mellitus. Wiley Online Lib. 1994;72:341–346. doi:10.1111/j.1755-3768.1994.tb02770.x
157. Murray, R.B., Metcalf, S.M., Lewis, P.M, et al. Sustaining remote-area programs: retinal camera use by Aboriginal health workers and nurses in a Kimberley partnership. Med J Aust. 2005;182:520.
158. Schulze-Döbold C, Erginay A, Robert N, Chabouis A, Massin P. Ophdiat(®): five-year experience of a telemedical screening programme for diabetic retinopathy in Paris and the surrounding area. Diabetes Metab. 2012;38(5):450–457. doi:10.1016/j.diabet.2012.05.003
159. Cuadros J, Bresnick G. EyePACS: an adaptable telemedicine system for diabetic retinopathy screening. - PubMed - NCBI. J Diabetes Sci Technol. 2009;3(3):509–516. doi:10.1177/193229680900300315
160. EyePACS LLC EyePACS Surpasses 750,000 patient encounters for diabetic retinopathy assessment. PR Newswire. Available from: https://www.prnewswire.com/news-releases/eyepacs-surpasses-750-000-patient-encounters-for-diabetic-retinopathy-assessment-300870295.html.Accessed May 6, 2020.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.