Back to Journals » Research Reports in Clinical Cardiology » Volume 10
The effect of pre-seasonal strength training on central hemodynamics and cardiac function in elite powerlifting athletes
Authors Jürgenson J ![]() , Serg M, Kampus P, Kals J, Muda P, Zagura M, Viru M, Zilmer M, Eha J, Unt E
, Serg M, Kampus P, Kals J, Muda P, Zagura M, Viru M, Zilmer M, Eha J, Unt E
Received 17 December 2018
Accepted for publication 9 May 2019
Published 3 July 2019 Volume 2019:10 Pages 33—41
DOI https://doi.org/10.2147/RRCC.S198590
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Kones
Janno Jürgenson,1,2 Martin Serg,3,4 Priit Kampus,3,4 Jaak Kals,4–6 Piibe Muda,7 Maksim Zagura,3,4 Mehis Viru,1 Mihkel Zilmer,4,6 Jaan Eha,3–4,7 Eve Unt2–3,8–9
1Institute of Sport Sciences and Physiotherapy, Medical Faculty, University of Tartu, Tartu, Estonia; 2Estonian Centre of Behavioural and Health Sciences, University of Tartu, Tartu, Estonia; 3Department of Cardiology, Institute of Clinical Medicine, Medical Faculty, University of Tartu, Tartu, Estonia; 4Endothelial Centre, University of Tartu, Tartu, Estonia; 5Department of Surgery, Institute of Clinical Medicine, Medical Faculty, University of Tartu, Tartu, Estonia; 6Department of Biochemistry, Institute of Biomedicine and Translational Medicine, Centre of Excellence for Genomics and Translational Medicine, Medical Faculty, University of Tartu, Tartu, Estonia; 7Heart Clinic, Tartu University Hospital, Tartu, Estonia; 8Department of Sports Medicine and Rehabilitation, Institute of Clinical Medicine, Medical Faculty, University of Tartu, Tartu, Estonia; 9Sports Medicine and Rehabilitation Clinic, Tartu University Hospital, Tartu, Estonia
Aim: The purpose of this study was to evaluate the effect of a pre-seasonal 12-week supervised strength training program (SSTP) on arterial stiffness, brachial and central blood pressure, and systolic and diastolic function of the heart in elite powerlifting athletes.
Methods: A descriptive study was performed in 19 elite male powerlifters, who exercised for 12 weeks, four days per week with an intensity of 60–90% assessed from 1 repetition maximum and 90–120 min per session. Carotid-femoral pulse wave velocity (cfPWV), augmentation index and central blood pressure were measured by applanation tonometry using the SphygmoCor device, and an echocardiographic examination was performed at baseline and after 12-week SSTP.
Results: Subjects’ mean brachial and central systolic blood pressure decreased significantly after the training period (132.3±8.8 vs 124.3±8.7 mmHg, p=0.002 and 110.1±7.7 vs 104.5±8.7 mmHg, p=0.008, respectively). Strength training significantly improved systolic tricuspid annular velocity and mitral E/e’ ratio (p<0.05). There were no significant differences in cfPWV and augmentation index at baseline and after SSTP.
Conclusion: The 12-week supervised strength pre-seasonal training program significantly decreased brachial and central systolic blood pressure in male elite powerlifting athletes. The strength training program decreased left ventricular filling pressure and improved right ventricular systolic function. No significant effect of strength training on aortic stiffness was found.
Keywords: pulse wave velocity, resistance training, cardiovascular health, echocardiography
Introduction
The blood pressure (BP) varies throughout the arterial tree due to pulse wave reflection and arterial stiffness.1 Elevated BP is a common abnormal finding during the periodic health evaluation of athletes.2 Strength-trained athletes and weightlifters have a higher prevalence of hypertension as compared to endurance athletes.3,4 Elevated BP leads to increased afterload on the heart causing left ventricular hypertrophy, which is an independent predictor of cardiovascular risk.4,5 Furthermore, there is an increasing amount of evidence that central BP is better related to target organ damage and cardiovascular events than brachial BP.6,7
It has been previously demonstrated that arterial stiffness is associated with a number of traditional and novel cardiovascular risk factors and target organ damage in patients with atherosclerosis and hypertension.8,9 There is also evidence that a reduction in arterial stiffness results in reduced incidence of cardiovascular events.10
Data have shown the beneficial cardiovascular effect of aerobic exercise is explained by amelioration of traditional as well as novel risk factors.11 Aerobic exercise augments endothelium-dependent vasodilation,12 which in turn may reduce aortic stiffness.13 At present, little is known about the effects of high-intensity strength training on central blood pressure and arterial stiffness. High-intensity strength training involves slow-speed contractions of the muscles, which are related to transient mechanical compression of resistant vessels, increasing peripheral vascular resistance and left ventricular pressure overload during exercise.14 It is still under discussion whether chronic increase in afterload may lead to concentric ventricular hypertrophy.15 Recent meta-analysis16 revealed that acute resistance training has an adverse effect on arterial stiffness due to cardiovascular as well as non-cardiovascular mechanisms. In regard to systematic strength training, available studies have shown stiffer arteries in strength-trained athletes,17,18 while other data have shown a beneficial effect of resistance training on aortic stiffness.19,20 Inconsistent results may depend on many factors. Many of these studies were performed in relatively small samples in different age and sex groups and by a large variation in training intensities. In addition, most of the intervention studies were performed in untrained, recreational level or pre-hypertensive individuals. Thus, available studies have not revealed a clear understanding of the impact of the combination of dynamic and isometric resistance training, also known as strength training, on central blood pressure and arterial stiffness in healthy individuals.17–27 Furthermore, the effect of elite-level strength training for lowering BP and target organ damage is still unclear.
Therefore, we aimed to investigate the effect of a pre-seasonal strength training program on brachial and central BP, arterial stiffness as well as heart structure and function in elite powerlifting athletes.
Material and methods
Subjects
A total of 20 voluntary male elite powerlifting athletes (age 28.2±6.1 years; height 179.2±5.9 cm; weight 99.9±16.5 kg; body mass index 31.2±5.1; body fat percentage 16.1±7.9) were examined before and after a 12-week supervised strength training period (SSTP). Study subjects have been exercised in powerlifting sports at competitive level from 4 to 15 years. Before the study, subjects completed a questionnaire concerning their personal and medical history and lifestyle parameters. All subjects were non-smokers and were free of acute or known chronic illnesses. In our study, only those voluntary subjects were included who agreed to avoid nutritional supplements. None of the participants were currently taking any medication. Subjects were asked not to take alcohol and not to change their usual diet during the SSTP. All subjects assessed their food intake three times during the study period for five consecutive days during the 12-week SSTP. All food items consumed were analyzed using the NutriData Estonian food composition database, version 8. One subject was excluded from data analysis due to the occurrence of injury and nonadherence to the full SSTP. Thus, the final study sample was 19. Informed written consent was obtained from each athlete in accordance with the principles of the Declaration of Helsinki. The study protocol was approved by the Research Ethics Committee of the University of Tartu.
Study protocol
Before the SSTP, there was an 8-week off-season period, where systematic training sessions and competitions were not allowed. The pre-seasonal 12-week SSTP consisted of a combination of dynamic (where muscles contract concentrically during the lifting phase and eccentrically during the lengthening phase) and isometric (muscular force development without movement) resistance training. During the SSTP, one exercise session consisted of 5–8 working sets to one muscle group, and athletes exercised with an intensity of 60–90% assessed from 1 repetition maximum (1 RM). The first set was done with an intensity of 60% of 1 RM and the last one 90% of 1 RM. Variation of repetitions was decreased according to the rise of intensity in one set (4 to 12). One exercise session lasted 90–120 min. The one-week training program (athletes exercised four days per week) consisted of the following exercises covering all major muscle groups: bench press, lateral pulldown, standing shoulder press, arm curl and extension, leg press, squat, leg curl, calf press, abdominal crunch, and deadlift. All the major muscle groups were exercised twice a week.
The structure of each exercise session was divided into three parts. The first part consisted of a 15-min warm-up, which included stretching and active exercises using body weight or very light weight. After the warm-up, the second part of the workout or the main training phase started, where the structure of the training session was on the ascending pyramid principle.28 This means that the first series was started with 60% of 1 RM with 12 repetitions, the second series was 70% of 1 RM with 10 repetitions, and the third was 80% of 1 RM with 8 repetitions. The fourth to sixth series were performed with loads ranging from 80% to 90% of 1 RM and 4–6 repetitions were made. In one session, half of the muscle groups were influenced: 1) on Monday and Thursday exercises were performed on chest muscles, latissimus dorsi muscles, hamstring muscles, abdominal muscles, lower back muscles, and shoulder muscles; 2) on Tuesday and Friday exercises were performed on arm muscles (m. biceps brachii and m. triceps brachii), quadriceps muscles and calf muscles. The third part of the workout included a 15-min cool-down period, which included stretching and foam rolling for all muscles that experienced load in the training session. No aerobic exercise was involved in the training program and all the sessions were supervised by a skilled certified instructor. After the SSTP, all athletes in the study participated in the Estonian Powerlifting Championships. The training protocol used is characteristic for high-level powerlifters in the pre-seasonal phase.
Measurements
Anthropometric, hemodynamic, echocardiographic, and maximal muscular power measurements were taken one week before the SSTP while post-training period measurements were performed one week following the competitions. There were no training sessions on the day preceding the measurements (maximal muscular power, laboratory and arterial stiffness measurements). The hemodynamics (blood pressure, arterial stiffness) measurements were performed between 8 and 10
Anthropometric data
Subjects’ height and weight were determined by the Martin metal anthropometer (±0.1 cm) and clinical scales (±0.05 kg), and body mass index (BMI) was calculated (kg/m2). Body fat percentage was assessed by measuring skinfold thickness at six different anatomical sites.29
Measurements of hemodynamics
Brachial blood pressure
Brachial BP was measured in a sitting position from the non-dominant arm as a mean of three consecutive measurements at 5-min intervals using a validated oscillometric technique (OMRON M4-I; Omron Healthcare Europe BV, Hoofddorp, the Netherlands). The mean of the two closest BP readings was used in further analysis.30 Brachial pulse pressure was calculated as the difference between brachial systolic and diastolic BP.
Central blood pressure and arterial stiffness
Radial artery waveforms were recorded with a high-fidelity micromanometer (applanation tonometry) from the wrist of the dominant arm and pulse wave analysis was performed on the systolic portion (SphygmoCor, version 7.1, AtCor Medical, Sydney, Australia) of the pulse curve in accordance with established guidelines.31 The corresponding ascending aortic waveforms were then generated using a validated transfer function,31,32 from which central systolic and diastolic BP, central pulse pressure and augmentation index (AIx) were calculated. The AIx was defined as the difference between the second and the first systolic peaks of the central arterial waveform expressed as the percentage of central pulse pressure.31 Mean arterial pressure (MAP) was calculated from the integration of the radial artery waveform. The degree of pulse pressure amplification (PPA) was calculated as brachial pulse pressure divided by central pulse pressure.
Carotid-femoral pulse wave velocity
The carotid-femoral pulse wave velocity (cfPWV), a direct measure of aortic stiffness, was determined by sequential acquisition of pressure waveforms from the carotid and femoral arteries using the same tonometer (SphygmoCor, version 7.1, AtCor Medical). The timing of these waveforms was compared with that of the R wave on a simultaneously recorded ECG. The cfPWV was determined by a calculation of the difference between the carotid and the femoral path length divided by the difference in the R wave to waveform foot times. The difference between the carotid and the femoral path length was estimated from the distance of the sternal notch to the femoral pulse measured in a direct line.31 The within-observer coefficient of variation for cfPWV was 2.3%.
The pulse wave analysis and cfPWV measurements were made in duplicate, and their mean values were used in subsequent analysis.
Echocardiography
An echocardiographic examination was performed using a commercially available device (Sonos7500, Philips Medical Systems, Inc., Highland Heights, OH, USA) with a 3.5-MHz transducer and digital recording by an experienced cardiologist. The images were stored digitally, coded with a random number and read by a blinded observer. Left atrial dimension was measured using the two-dimensional echocardiography (2DE) anteroposterior linear method. For left ventricular mass calculations, the 2DE and the M-mode were used. Long-axis measurements were obtained at the level distal to the mitral valve leaflets. Left ventricular internal dimension and septal and posterior wall thickness were measured at the end of the diastole (subscript “d”) according to the recommendations of the current guidelines.33 Left ventricular mass was calculated using the formula 0.8{1.04 [(LVIDd+PWTd+SWTd)3- (LVIDd)3]}+0.6 g (LVIDd – left ventricular internal dimension, PWTd – posterior wall thickness, SWTd – septal wall thickness).33 For 2DE volume calculations, the modified Simpson’s rule was used according to the current guidelines.33 For left ventricular diastolic function assessment, we measured medial E/e’ ratio and mitral valve E/A ratio in accordance with the recent guidelines.34 Left ventricular outflow tract velocity-time interval was measured with the pulsed-wave Doppler sample volume at the level of the left ventricular outflow tract in 3- or 5-chamber view. Tissue Doppler imaging (TDI) was performed in the apical four-chamber view. Peak systolic velocity of tricuspid annulus by TDI was measured as an indicator for right ventricular systolic function.
Assessment of maximal muscular power
Maximal muscular power was tested before and after the strength training period with bench press and jumping from a half squat (JHS) with a barbell. After the warm-up, each athlete performed maximal effort in bench press and jumping from a half squat by the bar with his body weight following SSTP study protocol. The muscle power produced during squat jump was measured with a linear encoder attached to the barbell and fitted to the Musclelab system (Ergotest Innovation a.s., Porsgrunn, Norway). The method was introduced previously by Bosco et al.35
Statistical analysis
Statistical analysis was performed with SPSS for Windows software, version 22.0 (IBM Corporation, Armonk, NY, USA). All data were checked for normal distribution using the Kolmogorov–Smirnov test. Data are expressed as means (x) and standard deviations (SD). Carotid-femoral PWV was adjusted to MAP. The data were analyzed using the paired-samples t-test. The Pearson or Spearman correlations analysis was used to determine the relationships between the variables. For the observed power estimation, the general linear model, repeated measurements and power calculations were performed. Statistical significance was defined as two-sided p<0.05.
Results
Subjects’ mean body weight, body fat percentage and BMI values after the 12-week strength training period did not differ significantly from baseline values (99.9±16.5 vs 100.2±17.1 kg, p=0.614; 16.1±7.9 vs 15.8±7.7, p=0.906; 31.2±5.1 vs 31.3±5.2, p=0.603, respectively). Table 1 provides descriptive information about the powerlifters’ mean dietary intake during the study [total caloric intake, protein, fat, and carbohydrate intake in grams and total energy intake (%) for proteins, fats and carbohydrates].
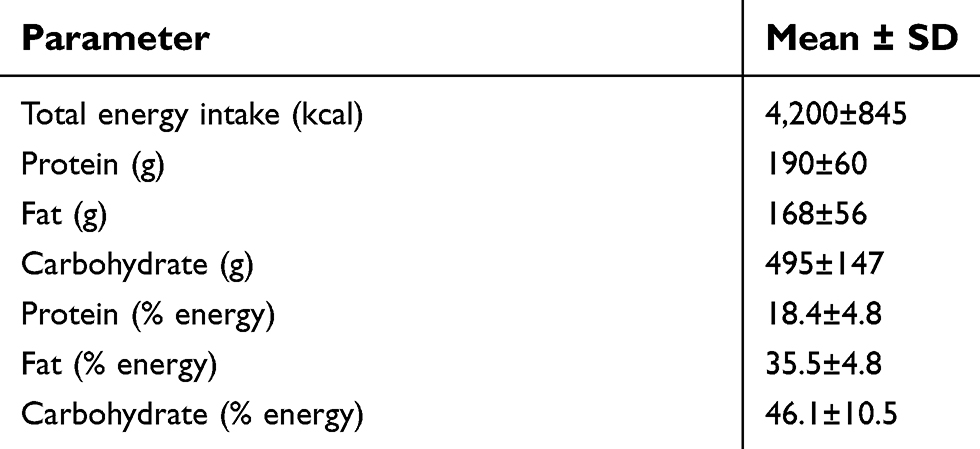 |
Table 1 Nutritional daily intake of the subjects |
Hemodynamic indices and blood pressure
The hemodynamic indices at baseline and after the 12-week strength training period are presented in Table 2. Brachial and central systolic BP decreased significantly after the training period. There were no significant differences after the training period in cfPWV (both adjusted and unadjusted) and AIx (Table 2). After the SSTP, a slight decrease was detected in central pulse pressure and brachial pulse pressure, but the decrease remained nonsignificant. No significant changes were found in MAP, PPA (brachial pulse pressure/central pulse pressure), and heart rate after the SSTP.
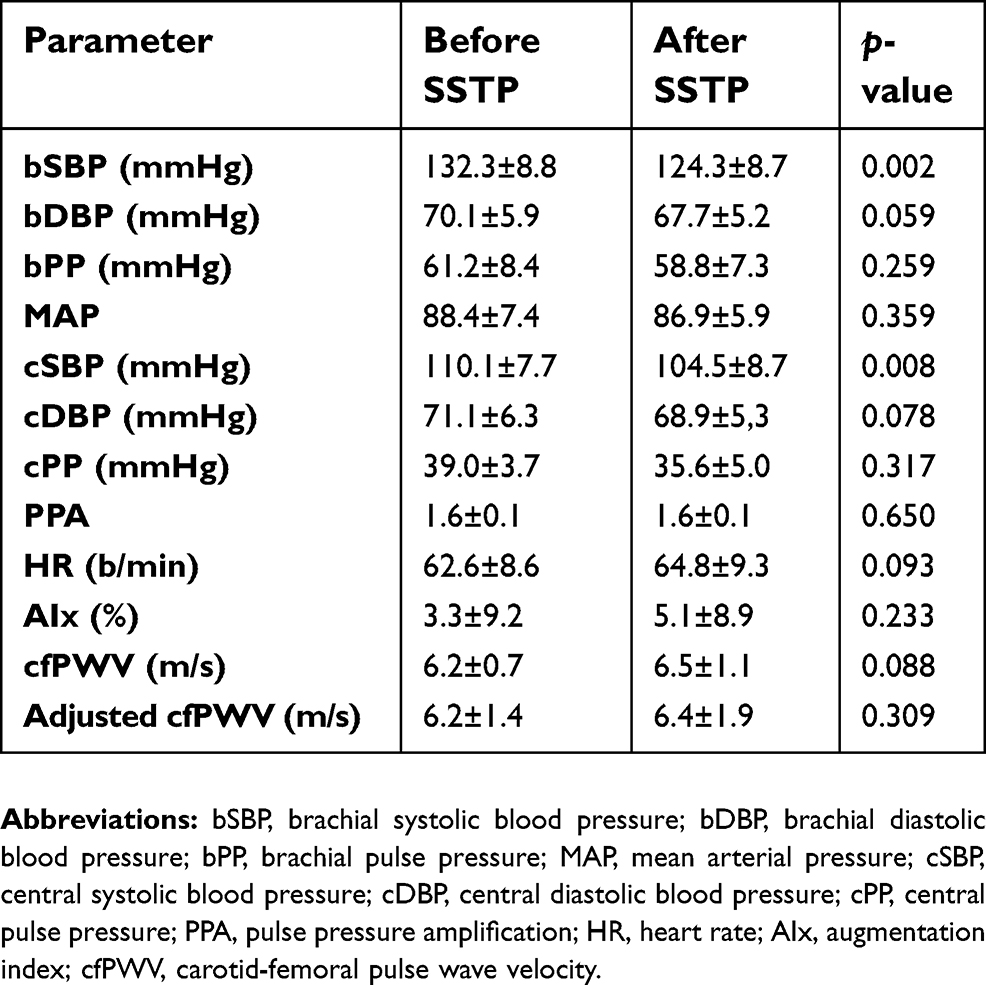 |
Table 2 Hemodynamic parameters of the subjects before and after the 12-week strength training period (SSTP) |
Echocardiography
Echocardiographic parameters at baseline and after the 12-week strength training period are presented in Table 3. At baseline, left ventricular systolic function (ejection fraction 52–72%) and mass index (49–115 g/m2) were in normal range in all study subjects. However, increased left ventricular end-diastolic volume (>64 mL/m2) was found in six subjects. Left atrial dimension and E/A ratio remained unchanged after SSTP. However, E/e’ ratio decreased significantly with SSTP (p<0.05). There was a statistically significant increase in tricuspid annular systolic velocity TDI (p<0.01). An inverse correlation was found between the change in tricuspid annular systolic velocity TDI and the change in mean arterial pressure (r=−0.5; p<0.05).
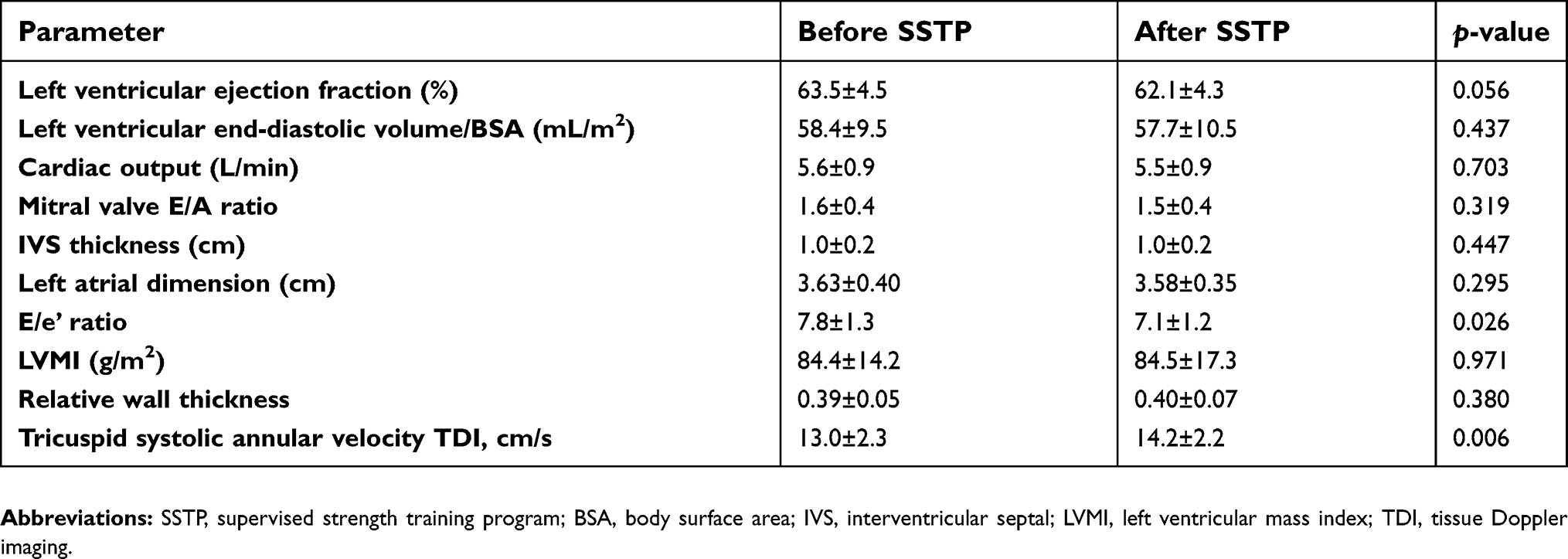 |
Table 3 Echocardiographic parameters of the subjects before and after the 12-week strength training (SSTP) |
Maximal muscular power
Descriptive data showed that mean values of bench press (BeP) and jumping from half squat (JHS) were significantly higher after the SSTP in comparison with baseline values (Figure 1), and these indices improved in all subjects. Observed power of effect size for BeP and JHS was between 0.41 and 0.46 for within-subjects effect and 0.96 and 1.0 for between-subjects effect, respectively.
 |
Figure 1 The mean power of bench press and jumping from half squat of the powerlifters before and after 12-week strength training period (SSTP). ***p<0.001, in comparison to before SSTP. Abbreviatons: BeP, bench press; JHS, jumping from half squat; SSTP, supervised strength training program. |
Discussion
Resistance exercise has been shown to have a beneficial effect on muscular strength, bone mineral density, and body composition.36 Nevertheless, there is less evidence to demonstrate a protective effect of resistance exercise on cardiovascular health, particularly on BP and hemodynamic parameters, compared to aerobic exercise.37,38 The hemodynamic effect of resistance training differs significantly from aerobic training. In general, resistance training is divided into two subgroups having different effects on the cardiovascular system. Dynamic resistance training (force development associated with movement with intensity between 30% and 100% of 1 RM) has been shown to reduce BP and is recommended as a means for cardiovascular prevention in the hypertension guidelines.24,39 Isometric resistance training (force development associated without movement with intensity between 10% and 40% of 1 RM) is not recommended for lowering BP because there are not enough studies available.24,39
Previous research indicates that isometric and isotonic exercise may have a differential effect on brachial and central blood pressure.40–42 Indeed, central systolic blood pressure was increased only after hand-grip, but not after ergometer exercises.40 It has been suggested that peripheral arterial dilatation caused by isotonic exercise might reduce the amplitude of reflected pressure waves.43 In contrast, isometric exercise could elevate arterial resistance, and thereby increase the amplitude of the radial reflected wave.43 In the present study, we found that strength training, which combines dynamic and isometric resistance training with the intensity of 60–90% of 1 RM, resulted in a significant decrease in brachial and also in central systolic BP. However, Tanaka et al evaluated central blood pressure by Omron HEM-9000AI, which is based on the measurement of late systolic pressure of peripheral pressure wave. In our study, the SphygmoCor device was used, where the estimation of central blood pressure is based on the general transfer function.44 Moreover, the novelty of our study is that we evaluated central blood pressure and arterial stiffness in elite powerlifting athletes, whereas Tanaka et al studied clinically healthy subjects from the general population.40 In our study, subjects’ mean brachial systolic and diastolic BP reduced by 8 and 2.4 mmHg, respectively. The results of our study support the evidence that strength training (combining dynamic and static exercise) has a significant BP-lowering effect in well-trained elite powerlifting athletes. In our study, the exposure to heavy training loads was supervised during the study period, and respective significant increases in maximal muscular power were revealed, which confirms that exposure to training loads was high in all subjects. Reduction of the peripheral and central blood pressure after resistance training could be explained by the change in the intensity and volume ratio of training. Despite prolonged intensive training, inactivity for several weeks can cause a loss of cardiovascular adaptation. Indeed, deconditioning is associated with a significant decrease in left ventricular wall thickness in highly trained athletes.45 Consistent with these findings, two months of inactivity resulted in a reduction of stroke volume, left ventricular end-diastolic diameter and cardiac output in highly trained subjects.46
Increased aortic stiffness is a well-known risk factor for cardiovascular disease.47 Controversy exists in the literature with regard to the effect of resistance exercise on aortic stiffness. Available mid- to long-term studies show a negative,17,18,25,48 neutral,26 or positive19,20 effect of resistance training on aortic stiffness. However, many of these studies were performed in relatively small samples in different age and sex groups and by a large variation in training intensity. Furthermore, most of the intervention studies were performed in untrained, recreational level or pre-hypertensive individuals. Most of the previously published study protocols are not comparable, especially where physical loads are very high. There are no data available for high-intensity strength training protocol, which is predominantly used by well-trained elite powerlifting athletes. In the present study, we did not find significant changes in cfPWV or AIx after the 12-week SSTP. It is possible that the changes in arterial stiffness were subtle because we studied well-trained powerlifters, who were conditioned for such strenuous training. In such a population, a 12-week training period might not be enough to evaluate the absolute effect of strength training on arterial stiffness. The BP-lowering effect of strength training is probably related to the reduction in peripheral vascular resistance27 and HR change, which moves the reflection point of the forward moving pulse wave more distally causing the BP to decrease.
Left ventricular hypertrophy is an independent cardiovascular risk factor in the general population49 and in hypertensive patients.50 In our study, there were no subjects with left ventricular hypertrophy, and there was no significant correlation between reduction in left ventricular mass and decrease in brachial BP.51 Our findings are consistent with previous research, where the 6-month resistance training did not have an effect on left ventricular remodeling.52 Furthermore, 12 weeks is a short period of time to observe structural changes in the heart.6 Left ventricular diastolic function can be used as an early marker of myocardial function change. In our study, SSTP improved left ventricular filling pressure, which indicates that change in central, not only peripheral BP, might improve left ventricular diastolic function. Moreover, to our knowledge, our study is the first one to show an increase in right ventricular systolic function and reduction in left ventricular filling pressure with resistance training. Assessment of diastolic function with echocardiography includes a complex of several variables; of these variables, E/e’ ratio is the most frequently used method for left ventricular filling pressure assessment.33 Adler et al53 showed in an acute setting, resistance training increases E/A ratio and decreases deceleration time, which are both beneficial changes in terms of diastolic function. However, tissue Doppler was not used in this study. Two major factors influencing left ventricular filling pressure are left ventricular compliance and wall thickness.54 As our subjects’ mean left ventricular wall thickness did not change significantly, it is possible that SSTP solely influenced their left ventricular compliance. While the left ventricle pumps into the systemic circulation, which has a significant reserve to decrease resistance and increase compliance with exercise, the right ventricle empties into the pulmonary circulation, which is characterized by low resistance and high compliance already at rest. Because there is a limited capacity to accommodate the blood flow in the pulmonary circulation with exercise, the right ventricle needs to maintain the necessary output.55 This explains the increase in the right ventricular systolic function parameter, ie, tricuspid annular systolic velocity TDI, in our study. Interestingly, we also found that an increase in right ventricular systolic function is associated with BP reduction. However, due to the design of our study, we cannot assess the causal relationship between these changes.
Our study has some limitations. There was no intention to involve a control group in this study due to several reasons. Firstly, it was not possible to sign elite level powerlifting athletes for 12 weeks without systematic strength training. Secondly, appropriate matched controls were not available for the present study group’s characteristics because elite level powerlifters have a higher BMI as well as significantly higher muscle mass than other age- and weight-matched men. In addition, our study lasted for 12 weeks, which might be too short to assess the change in left ventricular mass.38
On the other hand, the novelty of our study is that it was performed in elite-level powerlifters and evaluates the effect of a real training load which is characteristic only for this target group. Thus, the results of our study provide more practical knowledge about the cardiovascular risk level for competitive powerlifters and other strength-oriented athletes.
Finally, further mechanistic studies should be undertaken to assess the relationship between strength training and right ventricular function. Thus, the findings of our study may have significant implications for future research.
Conclusion
The results of our study revealed that the 12-week pre-seasonal supervised strength training program (a combination of dynamic and isometric resistance training) significantly decreased brachial and central systolic blood pressure in male elite powerlifting athletes. The strength training program decreased left ventricular filling pressure and improved right ventricular systolic function. However, there was no effect of strength training on aortic stiffness.
Acknowledgments
The current study was supported by grants of Estonian Science Foundation (Nos. 7395 and 7480), Institutional Research Fundings (No. IUT 02-7 and PRG435) and target financing No. 0180105s08 from the Ministry of Education and Research of Estonia. The authors wish to thank Helen Kaptein for her excellent technical assistance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nichols WW, O´Rourke MF. McDonald´s Blood Flow in Arteries: Theoretical, Experimental and Clinical Principles.
2. Corrado D, Basso C, Schiavon M, Pelliccia A, Thiene G. Pre-participation screening of young competitive athletes for prevention of sudden cardiac death. J Am Coll Cardiol. 2008;52(24):1981–1989. doi:10.1016/j.jacc.2008.06.053
3. Guo J, Zhang X, Wang L, Guo Y, Xie M. Prevalence of metabolic syndrome and its components among Chinese professional athletes of strength sports with different body weight categories. PLoS One. 2013;8e79758. doi:10.1371/journal.pone.0079758
4. Berge HM, Isern CB, Berge E. Blood pressure and hypertension in athletes: a systematic review. Br J Sports Med. 2015;49:716–723. doi:10.1136/bjsports-2014-093976
5. Volpe M, Battistoni A, Tocci G, et al. Cardiovascular risk assessment beyond systemic coronary risk estimation: a role for organ damage markers. J Hypertens. 2012;30:1056–1064. doi:10.1097/HJH.0b013e3283525715
6. Kampus P, Serg M, Kals J, et al. Differential effects of nebivolol and metoprolol on central aortic pressure and left ventricular wall thickness. Hypertension. 2011;57(6):1122–1128. doi:10.1161/HYPERTENSIONAHA.110.155507
7. Roman MJ, Devereux RB, Kizer JR, et al. Central pressure more strongly relates to vascular disease and outcome than does brachial pressure: the strong heart study. Hypertension. 2007;50(1):197–203. doi:10.1161/HYPERTENSIONAHA.107.089078
8. Kals J, Kampus P, Kals M, et al. Inflammation and oxidative stress are associated differently with endothelial function and arterial stiffness in healthy subjects and in patients with atherosclerosis. Scand J Clin Lab Invest. 2008;68(7):594–601. doi:10.1080/00365510801930626
9. Kampus P, Kals J, Unt E, et al. Association between arterial elasticity, C-reactive protein and maximal oxygen consumption in well-trained cadets during three days extreme physical load: a pilot study. Physiol Meas. 2008;29(4):429–437. doi:10.1088/0967-3334/29/4/001
10. Guerin AP, Blacher J, Pannier B, Marchais SJ, Safar ME, London GM. Impact of aortic stiffness attenuation on survival of patients in end-stage renal failure. Circulation. 2001;103:987–992.
11. Mora S, Cook N, Buring JE, Ridker PM, Lee IM. Physical activity and reduced risk of cardiovascular events: potential mediating mechanisms. Circulation. 2007;116(19):2110–2118. doi:10.1161/CIRCULATIONAHA.107.729939
12. Higashi Y, Sasaki S, Kurisu S, et al. Regular aerobic exercise augments endothelium-dependent vascular relaxation in normotensive as well as hypertensive subjects: role of endothelium-derived nitric oxide. Circulation. 1999;100(11):1194–1202.
13. Ashor AW, Lara J, Siervo M, Celis-Morales C, Mathers JC, Li Y. Effects of exercise modalities on arterial stiffness and wave reflection: a systematic review and meta-analysis of randomized controlled trials. PLoS One. 2014;9(10):e110034. doi:10.1371/journal.pone.0110034
14. MacDougall JD, Tuxen D, Sale DG, Moroz JT, Sutton JR. Arterial blood pressure response to heavy resistance exercise. J Appl Physiol. 1995;58:785–790. doi:10.1152/jappl.1985.58.3.785
15. Lalande S, Baldi JC. Left ventricular mass in elite olympic weight lifters. Am J Cardiol. 2007;100:1177–1180. doi:10.1016/j.amjcard.2007.05.036
16. Pierce DR, Doma K, Leicht AS. Acute effects of exercise mode on arterial stiffness and wave reflection in healthy young adults: a systematic review and meta-analysis. Front Physiol. 2018;9:73. doi:10.3389/fphys.2018.00073
17. Miyachi M. Effects of resistance training on arterial stiffness: a meta-analysis. Br J Sports Med. 2013;47(6):393–396. doi:10.1136/bjsports-2012-090488
18. Bertovic DA, Waddell TK, Gatzka CD, Cameron JD, Dart AM, Kingwell BA. Muscular strength training is associated with low arterial compliance and high pulse pressure. Hypertension. 1999;33(6):1385–1391.
19. Morra EA, Zaniqueli D, Rodrigues SL, et al. Long-term intense resistance training in men is associated with preserved cardiac structure/function, decreased aortic stiffness, and lower central augmentation pressure. J Hypertens. 2014;32(2):286–293. doi:10.1097/HJH.0000000000000035
20. Okamoto T, Masuhara M, Ikuta K. Effects of low-intensity resistance training with slow lifting and lowering on vascular function. J Hum Hypertens. 2008;22:509–511. doi:10.1038/jhh.2008.12
21. Jin YZ, Yan S, Yuan WX. Effect of isometric handgrip training on resting blood pressure in adults: a meta-analysis of randomized controlled trials. J Sports Med Phys Fitness. 2017;57(1–2):154–160. doi:10.23736/S0022-4707.16.05887-4
22. Inder JD, Carlson DJ, Dieberg G, McFarlane JR, Hess NC, Smart NA. Isometric exercise training for blood pressure management: a systematic review and meta-analysis to optimize benefit. Hypertens Res. 2016;39(2):88–94. doi:10.1038/hr.2015.111
23. Carlson DJ, Dieberg G, Hess NC, Millar PJ, Smart NA. Isometric exercise training for blood pressure management: a systematic review and meta-analysis. Mayo Clin Proc. 2014;89(3):327–334. doi:10.1016/j.mayocp.2013.10.030
24. Cornelissen VA, Smart NA. Exercise training for blood pressure: a systematic review and meta-analysis. J Am Heart Assoc. 2013;2(1):e004473. doi:10.1161/JAHA.112.004473
25. Collier SR, Kanaley JA, Carhart R
26. Rakobowchuk M, McGowan CL, de Groot PC, et al. Effect of whole body resistance training on arterial compliance in young men. Exp Physiol. 2005;90(4):645–651. doi:10.1113/expphysiol.2004.029504
27. Umpierre D, Stein R. Hemodynamic and vascular effects of resistance training: implications for cardiovascular disease. Arq Bras Cardiol. 2007;89:256–262.
28. Fleck SJ, Kraemer WJ. Types of strength training. In: Designing Resistance Training Programs.
29. Tipton CM, Oppliger RA. The Iowa wrestling study: lessons for physicians. Iowa Med. 1984;74(9):381–385.
30. Mancia G, De Backer G, Dominiczak A, et al. ESH-ESC task force on the management of arterial hypertension. 2007 guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2007;25(6):1105–1187. doi:10.1097/HJH.0b013e3281fc975a
31. Mackenzie IS, Wilkinson IB, Cockcroft JR. Assessment of arterial stiffness in clinical practice. Qjm. 2002;95:67–74.
32. Pauca AL, O’Rourke MF, Kon ND. Prospective evaluation of a method for estimating ascending aortic pressure from the radial artery pressure waveform. Hypertension. 2001;38:932–937.
33. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American society of echocardiography and the European association of cardiovascular imaging. Eur Heart J Cardiovasc Imaging. 2015;16(3):233–270. doi:10.1093/ehjci/jev014
34. Nagueh SF, Smiseth OA, Appleton CP, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the american society of echocardiography and the European association of cardiovascular imaging. J Am Soc Echocardiogr. 2016;29(4):277–314. doi:10.1016/j.echo.2016.01.011
35. Bosco C, Belli A, Astrua M, et al. A dynamometer for evaluation of dynamic muscle work. Eur J Appl Physiol Occup Physiol. 1995;70(5):379–386.
36. Gómez-Cabello A, Ara I, González-Agüero A, Casajús JA, Vicente-Rodríguez G. Effects of training on bone mass in older adults: a systematic review. Sports Med. 2012;42:301–325. doi:10.2165/11597670-000000000-00000
37. Cornelissen VA, Fagard RH. Effect of resistance training on resting blood pressure: a meta-analysis of randomized controlled trials. J Hypertens. 2005;23(2):251–259.
38. Yoon ES, Jung SJ, Cheun SK, Oh YS, Kim SH, Jae SY. Effects of acute resistance exercise on arterial stiffness in young men. Korean Circ J. 2010;40:16–22. doi:10.4070/kcj.2010.40.1.16
39. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013;34(28):2159–2219. doi:10.1093/eurheartj/eht151
40. Tanaka S, Sugiura T, Yamashita S, Dohi Y, Kimura G, Ohte N. Differential response of central blood pressure to isometric and isotonic exercises. Sci Rep. 2014;4:5439. doi:10.1038/srep05439
41. Bentley DC, Nguyen CH, Thomas SG, Cindy HN. Resting blood pressure reductions following handgrip exercise training and the impact of age and sex: a systematic review and narrative synthesis. Syst Rev. 2018;7:229. doi:10.1186/s13643-018-0876-5
42. Vanhees L, Geladas N, Hansen D, et al. Importance of characteristics and modalities of physical activity and exercise in the management of cardiovascular health in individuals with cardiovascular risk factors: recommendations from the EACPR. Part II. Eur J Prev Cardiol. 2012;19(15):1005–1033. doi:10.1177/1741826711430926
43. Hashimoto J, Westerhof BE, Westerhof N, Imai Y, O’Rourke MF. Differential role of wave reflection magnitude and timing on left ventricular mass reduction during antihypertensivse treatment. J Hypertens. 2008;26:1017–1024. doi:10.1097/HJH.0b013e3282f62a9b
44. Butlin M, Qasem A. Large artery stiffness assessment using SphygmoCor technology. Pulse. 2016;4:180–192. doi:10.1159/000452448
45. Maron BJ, Pelliccia A, Spataro A, Granata M. Reduction in left ventricular wall thickness after deconditoning in highly trained athletes. Br Heart J. 1993;69:125–128. doi:10.1136/hrt.69.2.125
46. Martin WH, Coyle EF, Bloomfield SA, Ehsani AA. Effects of physical deconditioning after intense endurance training on left ventricular dimensions and stroke volume. J Am Coll Cardiol. 1986;7:982–989.
47. Payne RA, Wilkinson IB, Webb DJ. Arterial Stiffness and hypertension: emerging concepts. Hypertension. 2010;55:9–14. doi:10.1161/HYPERTENSIONAHA.107.090464
48. Miyachi M, Kawano H, Sugawara J, et al. Unfavorable effects of resistance training on central arterial compliance: a randomized intervention study. Circulation. 2004;110(18):2858–2863. doi:10.1161/01.CIR.0000146380.08401.99
49. Levy D, Labib SB, Anderson KM, Christiansen JC, Kannel WB, Castelli WP. Determinants of sensitivity and specificity of electrocardiographic criteria for left ventricular hypertrophy. Circulation. 1990;81(3):815–820.
50. Koren MJ, Devereux RB, Casale PN, Savage DD, Laragh JH. Relation of left ventricular mass and geometry to morbidity and mortality in uncomplicated essential hypertension. Ann Intern Med. 1991;114:345–352.
51. Devereux RB, Dahlöf B, Gerdts E, et al. Regression of hypertensive left ventricular hypertrophy by losartan compared with atenolol: the Losartan Intervention for Endpoint Reduction in Hypertension (LIFE) trial. Circulation. 2004;110(11):1456–1462. doi:10.1161/01.CIR.0000141573.44737.5A
52. Spence AL, Naylor LH, Carter HH, et al. A prospective randomised longitudinal MRI study of left ventricular adaptation to endurance and resistance exercise training in humans. J Physiol. 2011;589(22):5443–5452. doi:10.1113/jphysiol.2011.217125
53. Adler Y, Fisman EZ, Koren-Morag N, et al. Left ventricular diastolic function in trained male weight lifters at rest and during isometric exercise. Am J Cardiol. 2008;102(1):97–101. doi:10.1016/j.amjcard.2008.02.105
54. Mihl D, Dassen WR, Kuipers H. Cardiac remodelling: concentric vs eccentric hypertrophy in strength and endurance athletes. Neth Heart J. 2008;16(4):129–133.
55. La Gerche A, Heidbüchel H, Burns AT, et al. Disproportionate exercise load and remodeling of the athlete’s right ventricle. Med Sci Sports Exerc. 2011;43(6):974–981. doi:10.1249/MSS.0b013e31820607a3
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.