Back to Journals » Therapeutics and Clinical Risk Management » Volume 12
Sudoscan as a noninvasive tool to assess sudomotor dysfunction in patients with Fabry disease: results from a case–control study
Authors sahuc P, Chiche L ![]() , dussol B, pouget J, franques J
, dussol B, pouget J, franques J
Received 27 October 2015
Accepted for publication 21 December 2015
Published 2 February 2016 Volume 2016:12 Pages 135—138
DOI https://doi.org/10.2147/TCRM.S99241
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Pauline Sahuc,1 Laurent Chiche,2 Bertrand Dussol,3 Jean Pouget,1 Jérôme Franques1,2,4
1Department of Neurology, La Timone Hospital, APHM, Aix-Marseille University, 2Department of Internal Medicine, European Hospital, 3Department of Nephrology, La Conception Hospital, APHM, Aix-Marseille University, 4Department of Neurology, La Casamance Hospital, Marseille, France
Abstract: Hypohidrosis is a frequent and early symptom in patients with Fabry disease. Studies have reported improved sweating in patients treated with enzyme-replacement therapy. A new method, Sudoscan, has been developed that is noninvasive, is quantitative, and can quickly evaluate sweat gland function. It is based on the electrochemical reaction between sweat chlorides and stainless-steel electrodes in contact with the palms and soles. The aim of our study was to evaluate the Sudoscan as a tool to assess sudomotor dysfunction in patients with Fabry disease. Consecutive patients were prospectively recruited who had a diagnosis of Fabry disease, which had been confirmed genetically and/or by measurement of α-galactosidase activity in leukocytes. Healthy controls, matched (1:1) for age and sex, were also enrolled. Test results were expressed immediately as electrochemical skin conductance (ESC, µS) for hands and feet. Sudomotor dysfunction was considered absent, moderate, or severe if the ESC measured on the feet was >60 µS, between 60 and 40 µS, or <40 µS, respectively. Among the 18 patients, 11 had hypohidrosis or anhidrosis. Hand and feet ESCs were significantly lower in patients compared to their controls (P=0.0015 and P=0.0047, respectively). Among patients, 8/18 (44.5%) had a sudomotor dysfunction, moderate in three and severe in five cases. Hand and feet ESCs were significantly lower in those with hypohidrosis/anhidrosis compared to those without (P=0.0014 and P=0.0056, respectively). This study showed that Sudoscan provided a quick, noninvasive, and quantitative measurement of sudomotor function in Fabry disease patients.
Keywords: electrochemical skin conductance, small fiber neuropathy, Fabry disease, sweat dysfunction, hypohidrosis
Introduction
Fabry disease (FD), a lysosomal-storage disorder with X-linked inheritance, is caused by mutations in the gene encoding the enzyme α-galactosidase A. Loss of function of this enzyme leads to accumulation of globotriaosylceramide in tissues, including the kidneys, heart, and nervous system.1 Burning “neuropathic” pain in the palms and soles and hypohidrosis often occur at a young age.1 Defective sweating had been attributed to the presence of small-fiber neuropathy (SFN)2 but alternatively may be caused by direct sweat gland dysfunction secondary to lipid accumulation in sweat glands.3 Importantly, studies have reported improved sweating in patients treated with enzyme-replacement therapy (ERT).4 Thus, sudomotor dysfunction could be used as a surrogate marker for early diagnosis and to assess treatment responses of patients with FD. However, assessment of sudomotor dysfunction requires highly technical and time-consuming procedures, such as the Quantitative Sudomotor Axon Reflex Test or skin biopsies, which limit their widespread adoption in clinical practice.4 Noninvasive tools assessing skin impedance have been tested but evidence of significant variance across dermatome sites depending on the pressure applied on skin surface was a clear limitation.5 A new method (Sudoscan®, Impeto Medical, Paris, France) has been developed that is noninvasive, is quantitative, and can quickly evaluate sweat gland function. It is based on the electrochemical reaction between sweat chlorides and stainless-steel electrodes in contact with the palms and soles. This method has been already evaluated in several pathological conditions, including diabetes, and compared to reference methods, where it has proved its reproducibility and usefulness to monitor treatment efficacy.6–8
The aim of our study was to evaluate the Sudoscan as a tool to assess sudomotor function in patients with FD.
Patients and methods
In this case–control prospective study, consecutive patients were recruited who had a diagnosis of FD, which had been confirmed genetically and/or by measurement of α-GAL activity in leukocytes (normal values: 10–20 μkat/kg). Healthy controls, matched (1:1) for age and sex, were also enrolled. The study was approved by Comité de Protection des Personnes Sud Méditerranée and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Data collected included the presence of hypo- or anhidrosis, renal dysfunction (defined as an estimated glomerular-filtration rate of <60 mL/min by the Modification of the Diet in Renal Disease [MDRD] formula) or any other causes of neuropathies, ongoing ERT. Patients and controls underwent a clinical examination to determine the amplitude of the left sensory peroneal nerve (μV). They were required to place their hands and feet, for 2 minutes, onto two large electrodes for sudomotor-function assessment using the Sudoscan. Briefly, each electrode alternately served as an anode or cathode. An incremental direct current stimulus (<4 V) was applied to the anode, inducing a current (intensity of ~0.2 mA) between the anode and cathode proportional to sweat chloride-ion concentration. Test results were expressed immediately as electrochemical skin conductance (ESC, μS), that is, the ratio between the current generated and the constant direct-current stimulus applied to the electrodes. The device produced individual ESC results for right and left hands and feet.
All ESC results corresponded to the average ESC between right and left sides for both hands and feet. According to previously defined threshold values,5–9 sudomotor dysfunction was considered absent, moderate, or severe if the ESC measured on the feet was >60 μS, between 60 and 40 μS, or <40 μS, respectively.
The number of patients to include was determined according to previous studies to obtain a difference of at least 8 μS between the two groups. Results were reported as mean ± standard deviation and comparisons were performed using Wilcoxon tests, as the distribution of data was not normal.
Results
Eighteen patients with FD (47±14 years, 14 males) and their 18 matched controls (48±14 years, 13 males) were prospectively enrolled (Table 1). Among the FD patients, 14 had received ERT for between 5 months and 27 years, 11 had hypohidrosis or anhidrosis, and 4 had renal dysfunction.
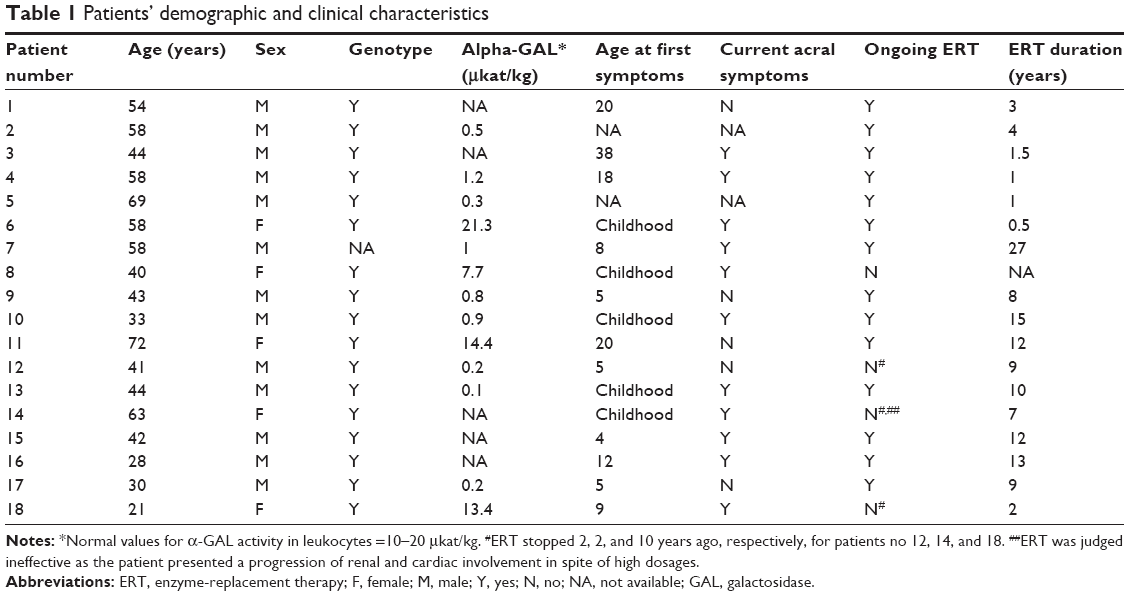 | Table 1 Patients’ demographic and clinical characteristics |
Hand and feet ESCs were significantly lower in FD patients compared to their controls (54.4±24.4 vs 76.3±10.9 μS, P=0.0015 and 58.5±25.8 vs 77.7±7.5 μS, P=0.0047, respectively) (Table 2). Conversely, no significant difference was found in the amplitude of the sensory peroneal nerves between FD patients and their controls (11.4±6.9 vs 12.7±5.8 μV, not statistically significant). A moderate correlation was observed between sensory peroneal-nerve amplitude and foot ESCs (Pearson’s correlation 0.57, P=0.018). Among FD patients, 8/18 (44.5%) had a sudomotor dysfunction, moderate in three and severe in five cases (Figure 1). Hand and feet ESCs were significantly lower in those with hypohidrosis/anhidrosis (Figure 1) compared to those without (42±22 vs 74±11 μS, P=0.0014 and 48±27 vs 76±10 μS, P=0.0056, respectively). No significant differences between hand and foot ESCs were observed between patients with or without renal dysfunction.
 | Table 2 Individual values of ESC of hands and feet in patients and controls |
 | Figure 1 Distribution of ESCs of hands (A) and feet (B) represented according to case or control status and the presence of hypohidrosis in patients with FD. |
Discussion
To the best of our knowledge, this study is the first to assess sudomotor dysfunction in patients with FD using a Sudoscan. Our results are in accordance with previous sudomotor assessment performed with methods difficult to use in routine practice. Importantly, we observed significantly impaired sudomotor function in most FD patients compared to matched controls, and the greater decrease in ESC observed in patients with hypohidrosis/anhidrosis among FD patients reinforces the validity of our findings. Sudoscan allows the assessment of sudomotor function by measuring ESC of hands and feet, in a much more practical way than with technically demanding and expensive prior technologies. Indeed, test results are robust, accomplished within minutes, require little technical training and no calculations.9
This study has several limitations. First, the small number of patients tested precluded subgroup analyses according to treatment received or correlations with extra-neurological involvements. Notably, SFN has been reported in the context of renal dysfunction; however, the lack of correlation of ESC with renal function in our cohort suggests that its decrease in FD is not just secondary to renal dysfunction. Second, this preliminary study was not designed to test diagnostic performance of Sudoscan for SFN. This would have required comparison to gold standard for the diagnosis of SFN such as skin biopsy. In the absence of such gold standard, we provided data according to the presence (or not) of hypohidrosis/anhidrosis. Importantly, a lack of such neurologic symptoms cannot be considered as synonym of preserved sudomotor function. Indeed, discrepancies between ESC and neurologic symptoms could correspond to the detection of early altered (ie, patients with no reported hypohydrosis but already low ESC) or improved (ie, delay between ESC and clinical improvement in some treated patients) sudomotor function by Sudoscan. Of note, we were not able to study the possible relation between ESC and residual enzymatic activity. Finally, no longitudinal assessment of ESC was planned in this first study.
In conclusion, this case–control study showed that Sudoscan provided a quick, noninvasive, and quantitative measurement of sudomotor function in patients with FD. Additional studies in larger cohorts of patients are warranted to evaluate its potential use to monitor treatment responses of patients with FD both in clinical practice and in clinical trials where objective and noninvasive surrogate markers are needed.10
Acknowledgments
We thank Dr Laure Swiader, Dr Roseline Froissart, and Dr Frederique Retornaz for their help in collecting the data and their careful review of the manuscript draft.
Disclosure
The authors report no conflicts of interest in this work.
References
Lidove O, Kaminsky P, Hachulla E, et al. Fabry disease ‘the new great imposter’: results of the French observatoire in internal medicine departments. Clin Genet. 2012;81:571–577. | ||
Üçeyler N, Kahn AK, Kramer D, et al. Impaired small fiber conduction in patients with Fabry disease: a neurophysiological case-control study. BMC Neurol. 2013;13:47. | ||
Lao LM, Kumakiri M, Mima H, et al. The ultrastructural characteristics of eccrine sweat glands in a Fabry disease patient with hypohidrosis. J Dermatol Sci. 1998;18:109–117. | ||
Schiffmann R, Floeter MK, Dambrosia JM, et al. Enzyme replacement therapy improves peripheral nerve and sweat function in Fabry disease. Muscle Nerve. 2003;28:703–710. | ||
Gupta SN, Ries M, Murray GJ, et al. Skin-impedance in Fabry disease: a prospective, controlled, non-randomized clinical study. BMC Neurol. 2008;8:41. | ||
Calvet JH, Dupin J, Winiecki H, Schwarz PE. Assessment of small fiber neuropathy through a quick, simple and non invasive method in a German diabetes outpatient clinic. Exp Clin Endocrinol Diabetes. 2013;121:80–83. | ||
Casellini CM, Parson HK, Richardson MS, Nevoret ML, Vinik AI. Sudoscan, a noninvasive tool for detecting diabetic small fiber neuropathy and autonomic dysfunction. Diabetes Technol Ther. 2013;15:948–953. | ||
Smith AG, Lessard M, Reyna S, Doudova M, Singleton JR. The diagnostic utility of Sudoscan for distal symmetric peripheral neuropathy. J Diabetes Complications. 2014;28:511–516. | ||
Vinik AI, Nevoret ML, Casellini C. The new age of sudomotor function testing: a sensitive and specific biomarker for diagnosis, estimation of severity, monitoring progression, and regression in response to intervention. Front Endocrinol (Lausanne). 2015;6:94. | ||
Alfadhel M, Sirrs S. Enzyme replacement therapy for Fabry disease: some answers but more questions. Ther Clin Risk Manag. 2011;7:69–82. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.