Back to Journals » Drug Design, Development and Therapy » Volume 9
Steroids as an adjunct for reducing the incidence of proliferative vitreoretinopathy after rhegmatogenous retinal detachment surgery: a systematic review and meta-analysis
Authors Shi H, Guo T, Liu P, Wang Q, Du Y, Liu QY ![]() , He M, Liu JL, Yu J
, He M, Liu JL, Yu J ![]()
Received 15 January 2015
Accepted for publication 5 February 2015
Published 6 March 2015 Volume 2015:9 Pages 1393—1400
DOI https://doi.org/10.2147/DDDT.S80983
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Shu-Feng Zhou
Hui Shi,1,2* Tao Guo,3* Peng-Cheng Liu,1 Qian-Yi Wang,1 Ya-Ru Du,1,2 Qing-Yu Liu,1 Meng-Mei He,1 Jun-Ling Liu,1 Jing Yu1
1Department of Ophthalmology, Shanghai Tenth People’s Hospital, School of Medicine, Tongji University, Shanghai, 2Department of First Clinical Medical College, Nanjing Medical University, Nanjing, Jiangsu, 3Department of Ophthalmology, Shanghai Third People’s Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Background: This meta-analysis was performed to determine the effectiveness of steroids as an adjunct following rhegmatogenous retinal detachment (RRD) surgery.
Methods: RRD patients with or without proliferative vitreoretinopathy (PVR) were included. The treatment group included patients in whom steroids were used as an adjunct and a control group in which placebo was used. Only randomized controlled trials were included. We searched the main electronic databases and included studies published until July 2014. PVR odds ratio, visual acuity, retinal reattachment rate, and complications were evaluated in three trials.
Results: Three randomized controlled trials were included in the meta-analysis. There was no significant difference in the incidence of postoperative PVR between groups (heterogeneity I2=48%, P=0.14). However, the incidence of postoperative PVR was lower in the treatment group (I2=0%, P<0.0001) than in the control group when a PVR grade C study was excluded. There was no statistically significant difference in postoperative visual acuity between the treatment and control groups (odds ratio -0.18; 95% confidence interval -0.38, 0.02; P=0.08). The two groups had similar results for primary/final retinal reattachment and reoperation rate. There was no significant difference in postoperative intraocular pressure.
Conclusion: This systematic review demonstrates that steroids may significantly reduce the incidence of postoperative PVR grade B or lower following RRD surgery.
Keywords: proliferative vitreoretinopathy, steroids, meta-analysis
Introduction
Rhegmatogenous retinal detachment (RRD) is the most common form of retinal detachment (RD). Proliferative vitreoretinopathy (PVR) is primarily a result of failure to correct RRD after initial retinal reattachment surgery, occurs in 5%–10% of patients, and may lead to recurrent RD.1 Further surgery is the only proven therapy for recurrent RD with PVR. However, the postoperative anatomic success rate is in the range of 60%–80%, and rates are lower for more severe PVR stages.2
Several drugs have shown potential benefit as adjunctive therapy for reducing the postoperative risk of PVR. Use of 5-fluorouracil and low molecular weight heparin can reduce the incidence of postoperative PVR and the associated reoperation rate.3,4 Several recent studies have indicated that postoperative treatment with oral 13-cis-retinoic acid decreases the risk of PVR and improves the operative rate of RD and visual acuity (VA).5,6 Curcumin effectively causes human fetal retinal pigment epithelium cell accumulation at the G2/M phase in vitro7 and also inhibits proliferation by causing cell death.8,9 Daunomycin inhibits formation of PVR in pigmented rabbits10 and proliferation of human retinal cells.11,12 In some hospitals, steroids, including prednisone, dexamethasone, and triamcinolone acetonide (TA), are regularly used during RRD surgery to reduce the risk of PVR.13–16
Steroids have been used to reduce intraocular inflammation since 1950.17 These agents were thought to suppress postoperative PVR by inhibition of cell proliferation and the intraocular inflammatory reaction.18–20 Further, steroids not only inhibit the production of histamine and decrease its synthesis, but can also cause release of prostaglandins and production of histamine.21 Intraoperative TA can improve the visibility of the posterior hyaloids and epiretinal membrane during pars plana vitrectomy, making surgery more safe and effective.22–24 Continuing TA after surgery can also continue to suppress the intraocular inflammation reaction.24
However, there is a lack of consensus regarding the best route of administration of steroids, the optimal dosage, and the most useful drug. The various steroid agents have different degrees of efficacy. This systematic review and meta-analysis may facilitate the comparison of such interventions.
Materials and methods
Search strategy
We searched the PubMed, EMBASE, and Cochrane Central Register electronic databases using the keywords “proliferative vitreoretinopathy”, “steroids”, “dexamethasone”, “triamcinolone acetonide”, “corticosteroids”, and “prednisolone”. The search was limited to human studies published in English up to July 2014.
Inclusion criteria
We selected papers using the following inclusion criteria: randomized controlled trial (RCT) design; inclusion limited to RRD patients with or without PVR; use of steroids as an adjunct; a placebo control group; and measurement of at least one of the outcomes of interest.
Exclusion criteria
Exclusion criteria included the following: non-RCT design; no detailed and comprehensive data; use of different evaluation outcomes; and the recent publications containing the most updated data from the same trail were included.
Data extraction and quality assessment
TG and PCL reviewed the titles and abstracts following the selection criteria independently. Full publications of appropriate studies were obtained for detailed evaluation, and the data were rechecked after extraction. Any disagreement regarding eligibility was discussed by the two reviewers. The information extracted from each study included method of allocation, blinding, first author, year, country, randomized counts, age, sex, inclusion and exclusion criteria, drugs, route of administration, duration of treatment, type of surgery, and duration of follow-up. The PVR incidence rate was compared in the meta-analysis. Secondary outcomes, including final VA, primary reattachment, and reoperation rate for retinal redetachment were extracted. Systemic and ocular complications were also noted.
Studies eligible for inclusion were assessed for methodological quality using the guidelines in the Cochrane Handbook for Systematic Reviews of Interventions (version 5.1.0, Oxford, UK).25
Statistical analysis
For both continuous and dichotomous data, the meta-analysis was conducted using the statistical software provided by the Cochrane Collaboration Review Manager 5.3.3 (Cochrane Collaboration, Nordic Cochrane Centre, Copenhagen, Denmark). The statistical summaries are presented as odds ratios (ORs) with 95% confidence intervals (CIs). The estimated effect of the data was calculated using the weighted mean difference (WMD) and 95% CI. The Q test or I2 test was used to evaluate heterogeneity. ORs and WMDs were considered to be statistically significant at the P<0.05 level. Both fixed-effects and random-effects models were used to obtain summary ORs or WMDs. In the absence of heterogeneity between groups, the fixed-effects model and the random-effects model provided concordant results. When heterogeneity was significant, the random-effects model was employed. Potential publication bias was estimated using the Egger test and by visually evaluating a funnel plot.26,27
Results
Literature search
A total of 43 articles were initially identified; 42 records were identified in the database search and one was found in a reference. Seven papers with full text that matched the inclusion criteria were assessed. Three studies investigated additional diseases, and one paper did not include quantitative data. Finally, three studies published before August 2014 were suitable for meta-analysis.28–30 Figure 1 contains a flow diagram of the search results.
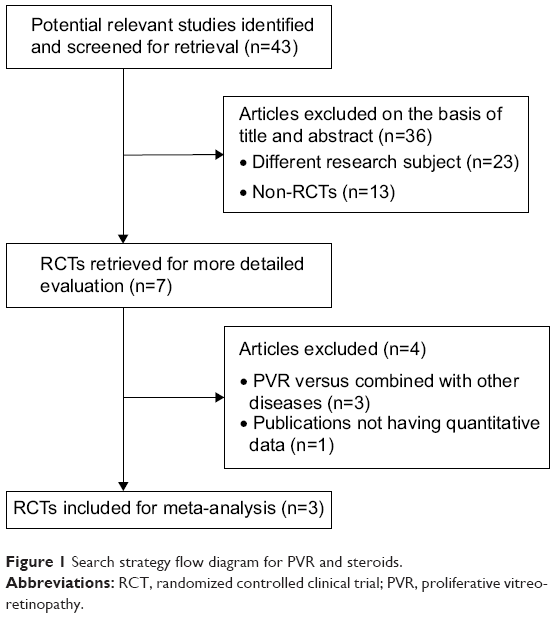 | Figure 1 Search strategy flow diagram for PVR and steroids. |
Study description
All of the studies included were RCTs conducted in Europe. The sample sizes ranged from 52 to 220. In total, 347 participants were included, comprising 237 (68.3%) males and 110 (31.7%) females. The steroid group contained 173 patients and the control group contained 174 patients. Various degrees of preoperative PVR were included (except PVR grade D). Pars plana vitrectomy or scleral buckling was performed in all patients. Two of the three trials used oral prednisone postoperatively, and the other involved injection of TA into the vitreous cavity during pars plana vitrectomy. The mean age of the participants was 52.3 years. All three studies included at least 6 months of follow-up. The outcomes were assessed in a blinded fashion. Table 1 shows the patient characteristics and baseline data for the three trials.
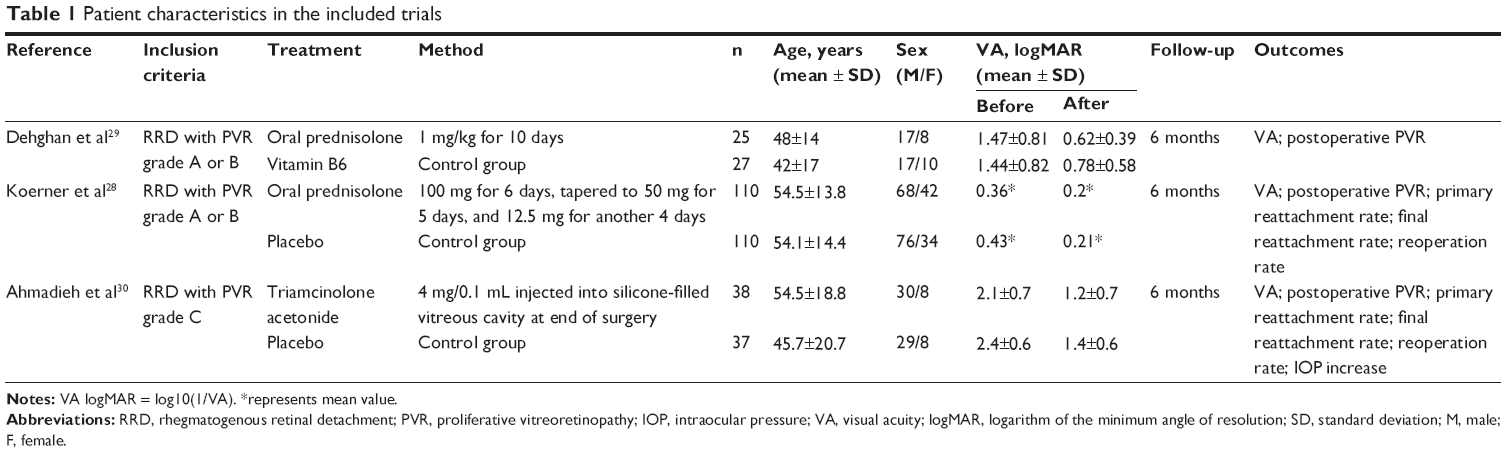 | Table 1 Patient characteristics in the included trials |
Quality assessment
In the three RCTs, the patients were divided using a random block permutation method, such as sealed envelopes, random numbers, or a computer-generated randomization list. The quality of the eligible studies is shown in Figure 2.
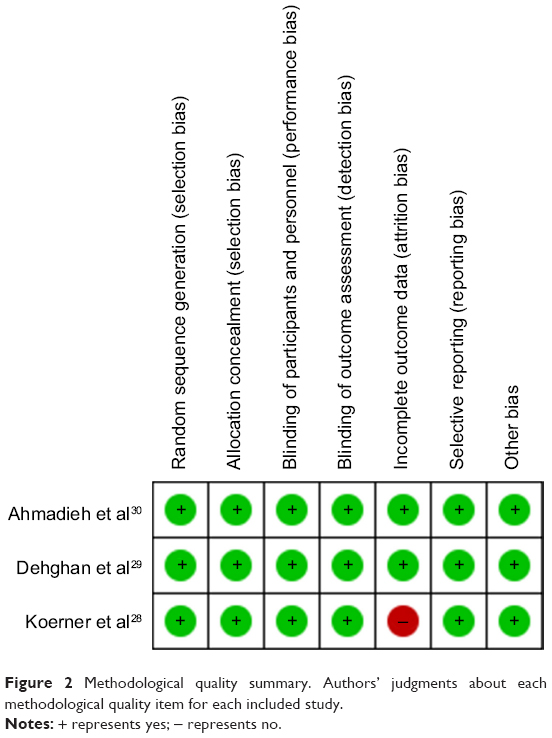 | Figure 2 Methodological quality summary. Authors’ judgments about each methodological quality item for each included study. |
Primary outcome
The OR for PVR was evaluated in the three trials, and no difference was found between the steroid and control groups (OR 0.46, 95% CI 0.20–1.10, P=0.08; Figure 3). Because the data showed significant heterogeneity (I2=48%, P=0.14), the random-effects model was used for meta-analysis. When the study with PVR grade C30 was excluded, the incidence of PVR was significantly decreased in the steroid group when compared with the control group (OR 0.30, 95% CI 0.17–0.54, P<0.0001; Figure 4).
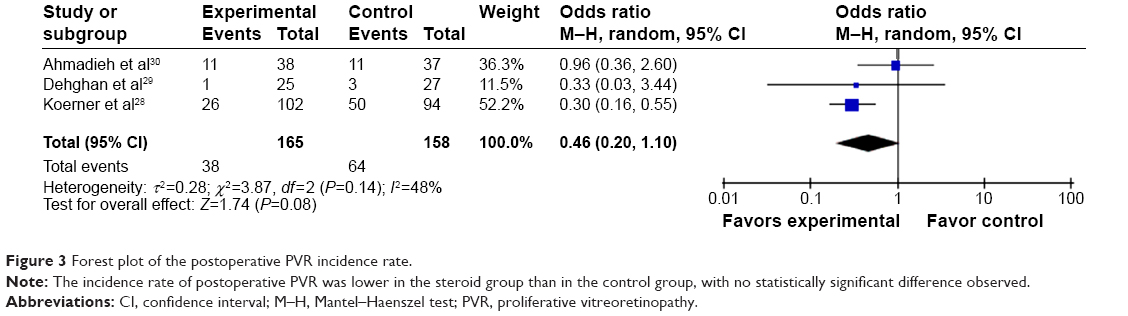 | Figure 3 Forest plot of the postoperative PVR incidence rate. |
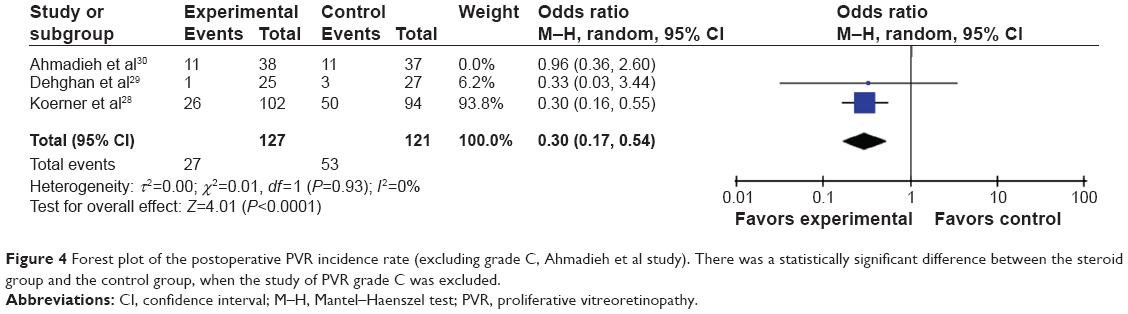 | Figure 4 Forest plot of the postoperative PVR incidence rate (excluding grade C, Ahmadieh et al study). There was a statistically significant difference between the steroid group and the control group, when the study of PVR grade C was excluded. |
Secondary outcomes
Visual acuity
One study28 was excluded from 6-month follow-up analysis because the relevant data could not be extracted from the original paper. Analysis of VA at 6 months was based on two papers (127 eyes) in which all patients were followed. There was no significant improvement in the steroid group compared with the control group (WMD -0.18, 95% CI -0.38, 0.02, P=0.08). Because the data were not heterogeneous (I2=0%, P=0.84), the fixed-effects model was used for meta-analysis (Figure 5).
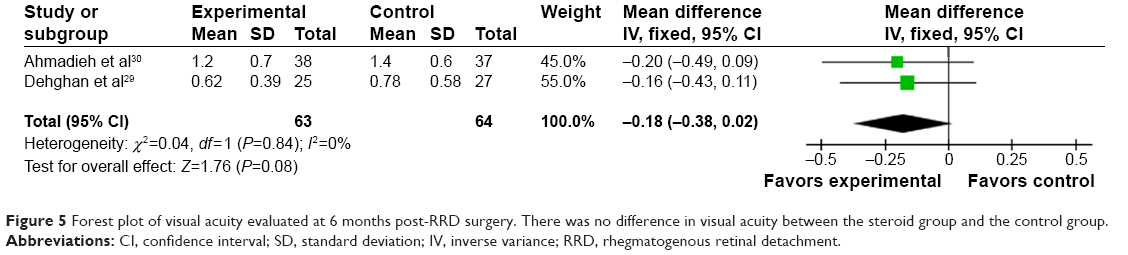 | Figure 5 Forest plot of visual acuity evaluated at 6 months post-RRD surgery. There was no difference in visual acuity between the steroid group and the control group. |
Retinal reattachment rate
One study29 was excluded from analysis of primary/final reattachment and reoperation rate for retinal redetachment because the relevant data could not be extracted from the original publication. In total, 127 eyes (85.8%) achieved retinal reattachment after primary surgery in the steroid group compared with 123 eyes (83.7%) in the control group. The primary reattachment rate showed no significant difference between the steroid and control groups (heterogeneity I2=0%, P=0.66; OR 1.18, 95% CI 0.63–2.23, P=0.61). The final reattachment rate was 94.29% (132 of 140 eyes) in the steroid group and 90.08% (118 of 131 eyes) in the control group (Table 2). The difference was not significant between the two groups (heterogeneity I2=0%, P=0.43; OR 1.81, 95% CI 0.73–4.52, P=0.20). The reoperation rate was 13.51% (20 in 148 eyes) for retinal reattachment in the steroid group; the corresponding data for the control group was 20.41% (30 in 147 eyes). The data were not heterogeneous (I2=0%, P=0.95; Table 2).
 | Table 2 Outcome indicators in the included trials |
Complications
Complication rates, including choroidal detachment, postoperative macular edema via fluorescein angiography, macular pucker formation, and intraocular pressure were not different between the two groups. There were no unexpected side effects due to administration of systemic corticosteroids.
Heterogeneity, sensitivity analysis, and publication bias
Some of the outcomes were heterogeneous. The heterogeneity for PVR incidence rate was significant. After excluding the PVR grade C study, the analysis yielded good results. A sensitivity analysis was conducted to evaluate the stability of the results by sequential removal of individual studies, and the results indicated stability. We therefore performed a heterogeneity interstudy, and the results indicated confidence in our conclusions. The random-effects model was chosen due to the high heterogeneity. The sensitivity analyses indicated that our conclusions were generally strong. Funnel plots were not used because there were fewer than ten trials available for each comparison.
Discussion
This meta-analysis examined the effectiveness and safety of steroids as an adjunct to RRD surgery. The quality of the evidence in this review was moderate. Overall, the three publications included in the meta-analysis were of good quality.
PVR is a common cause of recurrent RD, which often requires additional, multiple surgical interventions. The postoperative VA is worse, and surgical interventions have significantly increased costs.31 Therefore, it is necessary to prevent postoperative PVR.
Drug and tamponade agents are administered to patients with RRD. The clinical evidence indicates that low-dose intravitreal TA injections as an adjunct to vitrectomy and silicone oil tamponade for PVR are effective and safe.13 Jonas et al15 found that intravitreal injections of crystalline cortisone could reduce postoperative intraocular inflammation without toxicity to the intraocular structures. The above-mentioned studies suggest that steroids might be a potentially effective adjunct to PVR. However, our meta-analysis failed to identify significant differences. Due to the clinical heterogeneity, our inclusion criteria lead to a very different preoperative risk across the included studies compared to previous systemic reviews.
In fact, the treatment group showed a lower albeit not statistically significant PVR rate when compared with the control group. However, when excluding the PVR grade C study, the steroid group was more effective than the control group for PVR rate. Multiple studies have indicated that the development of epiretinal membrane results in an inflammatory cascade.32,33 Increased levels of interleukin-8 and vascular endothelial growth factor indicate an inflammatory process associated with a breakdown of the blood–retina barrier.34 Postoperative autoimmune reactions against retinal antigens can be much stronger.35 Steroids might facilitate the prevention or reduction of PVR. Overall, larger and stricter clinical trials are required.
The rate of increased intraocular pressure was lower in patients administered 4 mg TA than in those administered TA 25 mg.36,37 Blumenkranz et al38 found that steroids have an inhibitory effect on PVR at high doses and a stimulatory effect at low doses. Our meta-analysis failed to find a difference in the incidence rate of PVR grade C between the two groups. This result might be due to the following reasons. First, considering the increased intraocular pressure and systemic side effects associated with steroid use, the low doses were used more often, and might be insufficient to treat severe PVR. Second, the inclusion criteria were different between the three studies. There may be other more effective approaches, and this meta-analysis included only RCTs. In one prospective study,14 TA 4 mg was injected into the vitreous cavity filled with silicone oil after pars plana vitrectomy in patients with complicated RRD and PVR grade C2–C9. Twenty-one (87.5%) patients had attached retinas at the final follow-up visit, which is similar to the results in this meta-analysis.
Postoperative VA at 6 months was compared in this meta-analysis. No significant difference in VA was found at postoperative month 6 between the steroid and control groups. As in other studies, mean postoperative VA improved significantly in both groups. However, postoperative VA and changes in VA were not significantly different with or without TA. Overall, steroid use did not increase postoperative VA, potentially because anatomical success did not equate to functional success.
As reported by Williams et al39 the primary retinal reattachment and reoperation rates were not significantly different between the groups. The primary retinal reattachment rate was higher and the reoperation rate was lower in the steroid group; however, the rates were not significantly different. Acar et al16 found that their TA group (87.50%) had a higher albeit not statistically significant primary redetachment rate than their control group (78.12%). The final retinal reattachment rate was not different between the groups.
Use of steroids did not have any unexpected side effects. Postoperative intraocular pressure measurements did not differ significantly between the two groups and were similar to those in other studies.16,39 This might be a result of low-dose, short-term use of steroids. Unfortunately, we could not compare the postoperative cataract rate because cataract surgery is usually performed as a routine procedure along with most retinal reattachment surgeries.
Although only RCTs were included in this meta-analysis, some limitations should not be overlooked. First, only three studies were eligible for meta-analysis, which limits our ability to generalize the results, especially regarding differences between drugs. Some conclusions were difficult to reach due to the small sample sizes. Second, many factors, such as surgeon skills, PVR levels, surgical methods, approach, or steroid doses used, could have affected our results. Long-term follow-up is necessary because steroid use may have systemic side effects.
Conclusion
This meta-analysis demonstrates that use of steroids as an adjunct to RRD surgery can significantly decrease the postoperative PVR incidence rate, especially for grade B PVR.
Acknowledgments
This work was supported by the National Nature Science Foundation Project (81470648) and the New Excellence Project of Shanghai Health Bureau (XYQ2011067). No additional external funding was received.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors do not have any commercial or financial disclosures to report in this work.
References
Charteris DG, Sethi CS, Lewis GP, Fisher SK. Proliferative vitreoretinopathy – developments in adjunctive treatment and retinal pathology. Eye (Lond). 2002;16(4):369–374. | ||
Heimann H, Bartz-Schmidt KU, Bornfeld N, et al. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment: a prospective randomized multicenter clinical study. Ophthalmology. 2007;114(12):2142–2154. | ||
Wickham L, Bunce C, Wong D, McGurn D, Charteris DG. Randomized controlled trial of combined 5-fluorouracil and low-molecular-weight heparin in the management of unselected rhegmatogenous retinal detachments undergoing primary vitrectomy. Ophthalmology. 2007;114(4):698–704. | ||
Charteris DG, Aylward GW, Wong D, et al. A randomized controlled trial of combined 5-fluorouracil and low-molecular-weight heparin in management of established proliferative vitreoretinopathy. Ophthalmology. 2004;111(12):2240–2245. | ||
Fekrat S, de Juan EJ, Campochiaro PA. The effect of oral 13-cis-retinoic acid on retinal redetachment after surgical repair in eyes with proliferative vitreoretinopathy. Ophthalmology. 1995;102(3):412–418. | ||
Chang YC, Hu DN, Wu WC. Effect of oral 13-cis-retinoic acid treatment on postoperative clinical outcome of eyes with proliferative vitreoretinopathy. Am J Ophthalmol. 2008;146(3):440–446. | ||
Gong L, Jiang D, Zhu X, Guo L. [Curcumin inhibits the proliferation of cultured human fetal retinal pigment epithelium cells]. Yan Ke Xue Bao. 2004;20(4):246–248. Chinese. | ||
An JB, Ma JX, Liu DY, et al. [The effect of curcumin on DNA content, mitochondrial transmembrane potential and calcium of rabbit cultured retinal pigment epithelial cells]. Zhonghua Yan Ke Za Zhi. 2009;45(3):210–215. Chinese. | ||
Alex AF, Spitznas M, Tittel AP, Kurts C, Eter N. Inhibitory effect of epigallocatechin gallate (EGCG), resveratrol, and curcumin on proliferation of human retinal pigment epithelial cells in vitro. Curr Eye Res. 2010;35(11):1021–1033. | ||
Shinohara K, Tanaka M, Sakuma T, Kobayashi Y. Efficacy of daunorubicin encapsulated in liposome for the treatment of proliferative vitreoretinopathy. Ophthalmic Surg Lasers Imaging. 2003;34(4):299–305. | ||
Cai J, Wei R, Ma X, Zhu H, Li Y. Cytotoxic effects of antiproliferative agents on human retinal glial cells in vitro. Int Ophthalmol. 2001;24(4):225–231. | ||
Wu WC, Kao YH, Tseng HY. The cell cycle distribution of cultured human retinal pigmented epithelial cells under exposure of anti-proliferative drugs. J Ocul Pharmacol Ther. 2003;19(1):83–90. | ||
Chen W, Chen H, Hou P, et al. Midterm results of low-dose intravitreal triamcinolone as adjunctive treatment for proliferative vitreoretinopathy. Retina. 2011;31(6):1137–1142. | ||
Cheema RA, Peyman GA, Fang T, et al. Triamcinolone acetonide as an adjuvant in the surgical treatment of retinal detachment with proliferative vitreoretinopathy. Ophthalmic Surg Lasers Imaging. 2007;38(5): 365–370. | ||
Jonas JB, Hayler JK, Panda-Jonas S. Intravitreal injection of crystalline cortisone as adjunctive treatment of proliferative vitreoretinopathy. Br J Ophthalmol. 2000;84(9):1064–1067. | ||
Acar N, Kapran Z, Altan T, Unver YB, Pasaoglu E. Pars plana vitrectomy with and without triamcinolone acetonide assistance in pseudophakic retinal detachment complicated with proliferative vitreoretinopathy. Jpn J Ophthalmol. 2010;54(4):331–337. | ||
Howard JE, Harvey AM, Carey RA, Winkenwerder WL. Effects of pituitary adrenocorticotropic hormone (ACTH) on the hypersensitive state. J Am Med Assoc. 1950;144(16):1347–1349. | ||
Shen L, You Y, Sun S, et al. Intraocular and systemic pharmacokinetics of triamcinolone acetonide after a single 40-mg posterior subtenon application. Ophthalmology. 2010;117(12):2365–2371. | ||
Mankowska A, Rejdak R, Oleszczuk A, et al. [Decrease of the postoperative inflammatory reaction during pars plana vitrectomy (PPV) after administration of triamcinolone acetonide]. Klin Oczna. 2008;110(4–6):151–154. Polish. | ||
Weller M, Wiedemann P, Heimann K. Proliferative vitreoretinopathy – is it anything more than wound healing at the wrong place? Int Ophthalmol. 1990;14(2):105–117. | ||
Peyman GA, Schulman JA. Intravitreal Surgery: Principles and Practice. Norwalk, CT, USA: Appleton & Lange; 1994. | ||
Furino C, Micelli FT, Boscia F, et al. Triamcinolone-assisted pars plana vitrectomy for proliferative vitreoretinopathy. Retina. 2003;23(6):771–776. | ||
Sakamoto T, Ishibashi T. Visualizing vitreous in vitrectomy by triamcinolone. Graefes Arch Clin Exp Ophthalmol. 2009;247(9):1153–1163. | ||
Sonoda KH, Enaida H, Ueno A, et al. Pars plana vitrectomy assisted by triamcinolone acetonide for refractory uveitis: a case series study. Br J Ophthalmol. 2003;87(8):1010–1014. | ||
Moher D, Cook DJ, Jadad AR, et al. Assessing the quality of reports of randomised trials: Implications for the conduct of meta-analyses. Health Technol Assess. 1999;3(12):1–98. | ||
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088–1101. | ||
Egger M, Davey SG, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315 (7109):629–634. | ||
Koerner F, Koerner-Stiefbold U, Garweg JG. Systemic corticosteroids reduce the risk of cellophane membranes after retinal detachment surgery: a prospective randomized placebo-controlled double-blind clinical trial. Graefes Arch Clin Exp Ophthalmol. 2012;250(7):981–987. | ||
Dehghan MH, Ahmadieh H, Soheilian M, et al. Effect of oral prednisolone on visual outcomes and complications after scleral buckling. Eur J Ophthalmol. 2010;20(2):419–423. | ||
Ahmadieh H, Feghhi M, Tabatabaei H, et al. Triamcinolone acetonide in silicone-filled eyes as adjunctive treatment for proliferative vitreoretinopathy: a randomized clinical trial. Ophthalmology. 2008;115(11):1938–1943. | ||
Patel NN, Bunce C, Asaria RH, Charteris DG. Resources involved in managing retinal detachment complicated by proliferative vitreoretinopathy. Retina. 2004;24(6):883–887. | ||
Gilbert C, Hiscott P, Unger W, Grierson I, McLeod D. Inflammation and the formation of epiretinal membranes. Eye (Lond). 1988;2 Suppl:S140–S156. | ||
Joshi M, Agrawal S, Christoforidis JB. Inflammatory mechanisms of idiopathic epiretinal membrane formation. Mediators Inflamm. 2013;2013:192–582. | ||
Rasier R, Gormus U, Artunay O, et al. Vitreous levels of VEGF, IL-8, and TNF-alpha in retinal detachment. Curr Eye Res. 2010;35(6):505–509. | ||
Ricker LJ, Kijlstra A, Kessels AG, et al. Interleukin and growth factor levels in subretinal fluid in rhegmatogenous retinal detachment: a case-control study. PLoS One. 2011;6(4):e19141. | ||
Gillies MC, Simpson JM, Luo W, et al. A randomized clinical trial of a single dose of intravitreal triamcinolone acetonide for neovascular age-related macular degeneration: one-year results. Arch Ophthalmol. 2003;121(5):667–673. | ||
Jonas JB, Akkoyun I, Budde WM, Kreissig I, Degenring RF. Intravitreal reinjection of triamcinolone for exudative age-related macular degeneration. Arch Ophthalmol. 2004;122(2):218–222. | ||
Blumenkranz MS, Claflin A, Hajek AS. Selection of therapeutic agents for intraocular proliferative disease. Cell culture evaluation. Arch Ophthalmol. 1984;102(4):598–604. | ||
Williams RG, Chang S, Comaratta MR, Simoni G. Does the presence of heparin and dexamethasone in the vitrectomy infusate reduce reproliferation in proliferative vitreoretinopathy? Graefes Arch Clin Exp Ophthalmol. 1996;234(8):496–503. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.