Back to Journals » Patient Preference and Adherence » Volume 10
Social support received by multidrug-resistant tuberculosis patients and related factors: a cross-sectional study in Zhejiang Province, People's Republic of China
Authors Chen B ![]() , Peng Y, Zhou L, Chai C, Yeh H, Chen S, Wang F, Zhang M, He T, Wang X
, Peng Y, Zhou L, Chai C, Yeh H, Chen S, Wang F, Zhang M, He T, Wang X
Received 2 February 2016
Accepted for publication 17 April 2016
Published 13 June 2016 Volume 2016:10 Pages 1063—1070
DOI https://doi.org/10.2147/PPA.S105655
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Naifeng Liu
Bin Chen,1 Yin Peng,1 Lin Zhou,1 Chengliang Chai,1 Hui-Chi Yeh,2 Songhua Chen,1 Fei Wang,1 Mingwu Zhang,1 Tieniu He,1 Xiaomeng Wang1
1Department of Tuberculosis Control and Prevention, Zhejiang Provincial Center for Disease Control and Prevention, Binjiang District, Hangzhou, People’s Republic of China; 2Politics & International Relations, Social Sciences, University of Southampton, Southampton, UK
Objectives: The objective of this study is to assess the social support received by patients diagnosed with multidrug-resistant tuberculosis (MDR-TB) in Zhejiang Province, People’s Republic of China and the factors that may have influenced it.
Methods: A total of 220 MDR-TB patients participated in the questionnaire-based survey, and the data from 212 valid questionnaires were analyzed. The respondents reported their sociodemographic status, disease features, and attitudes toward the disease. The social support rating scale was used to measure the patients’ social support scores. An Independent Samples t-test, one-way analysis of variance, and a multiple linear regression model were used to analyze the related factors for the social support scores.
Result: The average social support score of each MDR-TB patient was 32.56±7.86. Participants who were single, widowed or divorced, retired, and had fewer family members and lower family income were found to have lower social support scores. Participants unwilling to disclose their disease tended to have less social support (31.59<34.23, P=0.010). Participants who perceived great help from health care workers reported higher social support rating scale scores than those who perceived no help (35.36>29.89, P=0.014).
Conclusion: MDR-TB patients in Zhejiang Province were shown to have a low level of social support. Patients who were not married, had smaller families, and lower family income received less social support, suggesting that family harmony could be an important source of social support. Patients’ self-isolation may contribute to a decrease in the amount of support they receive from their surroundings. Health care organizations need to offer more social support to MDR-TB patients.
Keywords: multidrug-resistant TB, social support, factors
Introduction
The People’s Republic of China is one of the countries with highest tuberculosis (TB) burdens in the world, and it registered the second-largest number of TB patients in 2014, globally.1 Located in southeastern China, Zhejiang Province has a relatively low reported incidence of TB within the country. However, there are still >30,000 TB cases reported each year in the province because of the density of its population.2 Furthermore, the epidemic of multidrug-resistant tuberculosis (MDR-TB, defined by resistance to the two most commonly used drugs in the current four-drug regimen, isoniazid and rifampin) has posed considerable challenges for TB control in the country and the province.3–5 According to a recent provincial TB drug-resistance survey, the total rate of MDR-TB among TB patients was 6.0%, which could be estimated to be ~2,000 MDR-TB cases each year in Zhejiang Province.3
TB usually strikes vulnerable members of the population, such as the poor, homeless, undernourished, or migrant population.6–8 Unfortunately, the huge cost of the disease can incur catastrophic expenditures for individuals and households, leading to impoverishment, inadequate use of health services, suspended treatment, and increased spread of the disease.9,10 Moreover, the infectious nature of TB may generate social isolation and stigma in the community, which can have a negative psychological impact on TB patients.11,12 The situation is even worse among MDR-TB patients because the treatment is more complicated, the regimen is much longer, the results of infection are more severe, and the cost is much higher.1,4,13
In 2007, Zhejiang Province initiated an MDR-TB prevention and control program supported by the Global Fund and later established a local MDR-TB control program.14,15 As part of this program, TB patients’ sputum samples were cultured in the laboratory of the designated hospital at the county level, and culture-positive strains were transferred and tested for drug susceptibility at the municipal TB hospital. If the TB patient was diagnosed as an MDR-TB patient, he or she was treated at specialized municipal TB hospitals with the standard chemotherapy regimen recommended by the World Health Organization. Local centers for disease control and prevention undertook the tasks of patient tracing, information registry, and follow-up arrangements. The community health service center was in charge of patient follow-up, health education, and psychological support. The program provided each patient with ~15 dollars per month as a nutrition and transportation subsidy.
Social support is recognized as an effective way to help TB patients in completing their treatment.8,16,17 Social support is defined as “information leading the subjects to believe that they are cared for and loved, esteemed, and members of a network of mutual obligations”.18 Many previous studies have attempted to measure the amount of social support available to non-TB patients and disaster victims, finding a positive impact on stress relief, treatment compliance, and the establishment of beneficial behavior.19–22 In the People’s Republic of China, studies have measured the social support available to TB patients during their treatment period.23–25 However, few studies have measured social support specifically for MDR-TB patients, while the factors influencing social support acquisition continue to remain unidentified. Here, a cross-sectional study was initiated to assess the social support received by MDR-TB patients who were undergoing treatment and follow-up support in Zhejiang Province and to identify the factors affecting social support among its respondents.
Methods
Participants
A cross-sectional survey of MDR-TB patients was conducted from July 15 to August 15, 2014, in Zhejiang Province. The inclusion criteria were 1) patients who started their treatment during January 1, 2009, and June 30, 2012, in Zhejiang Province, and participants who had ended treatment at the time of the survey, so that their social support score could be measured throughout the treatment period; 2) MDR-TB patients who were undergoing follow-up through the provincial MDR-TB control program during the same period; and 3) MDR-TB patients or their caregivers who were able to clearly understand the contents of the questionnaire. A total of 307 eligible MDR-TB patients were contacted, of whom 48 patients or their caregivers could not be reached due to changes in telephone contact numbers or because they had moved to other provinces, 26 patients died before they could be contacted, and 13 patients declined to be interviewed. Finally, 220 MDR-TB patients participated in the study.
Study design
A structured questionnaire was conducted, containing items related to demographic characteristics, attributes of MDR-TB disease, attitudes toward the disease, help from the health service, and the social support rating scale (SSRS). The scale was first designed and introduced by Xiao in 199426 and has shown a high degree of reliability and validity when applied to measure social support in the Chinese population in previous studies.22,25–29 The scale consisted of ten items that measured three domains of social support: subjective support (four items), objective support (three items), and support-seeking behavior (three items). Subjective support refers to the social relationships that the individual believes he or she can rely on, and the perceived level of support from surrounding persons including family members, neighbors, friends, colleagues, and other people. Objective support refers to the actual support gained from social surroundings. Support-seeking behavior reflects the pattern of behavior utilized by an individual when he or she seeks support.30 Scores of the ten items were added together, and the total score ranged from 12 to 66, within which the subjective score ranged from 8 to 32, the objective score from 1 to 22, and the support availability from 3 to 12. A higher score reflects stronger social support. The Cronbach’s alpha coefficient for the SSRS in the current study was 0.82.
The investigators from the provincial and local Centers for Disease Control and Prevention were trained with unified criteria. Two investigators went to patients’ homes and conducted the face-to-face survey. One investigator was responsible for interviewing respondents, and the other supervised the whole process and checked the returned questionnaires. The questionnaires were collected and then the consistency was double-checked by the researchers at the provincial level. Eight questionnaires were excluded for inconsistency between the questionnaire items. Finally, the data from the 212 valid questionnaires were entered into a database for analysis.
Statistical analysis
Descriptive analysis was used to assess the basic demographic characteristics, disease characteristics, and social support score. An Independent Samples t-test and one-way analysis of variance were used to compare different social support scores among the different groups. The SSRS was set as the dependent variable, and the participants’ demographic characteristics, disease features, and attitudes were set as the independent variables. The annual family income was stratified into three groups according to the province’s income level during the study period. A multiple linear regression model was developed based on backward elimination to identify factors relevant to MDR-TB patients’ SSRS scores. The inclusion and exclusion thresholds for the variables were 0.05 and 0.10, respectively. Data analysis was performed using SPSS, Version 13.0 (SPSS Inc., Chicago, IL, USA). A P-value of <0.05 was considered statistically significant.
Ethical consideration
The study was approved by the Ethical Review Board of Zhejiang Provincial Center for Disease Control and Prevention. Informed written consents were obtained from the respondents, and their private information was carefully protected.
Results
Sociodemographic characteristics of the participants
Among all 212 participants, there were more male MDR-TB patients than female patients (69.81%>30.19%), which was representative of the sex distribution of TB patients in the province. Most of the participants were native residents, and 47 (22.17%) patients were from other provinces or other prefectures within the province. The age groups of 40–59 years and 20–39 years accounted for 43.87% and 31.13%, respectively, consisting of more than three-fourths of all the participants. The participants’ education level was relatively low with 164 (77.36%) patients who had only attended middle school or primary school or had received no education at all. Farmer (25.47%) and worker (22.64%) groups were the two most common occupations of the participants. Married patients accounted for >70% of the total, and about half of the participants’ families had two to three family members. Approximately 52% of the participants’ annual family income was between 10,001 and 50,000 Yuan (1,640–8,197 dollars), which was the middle level of all the participants (Table 1).
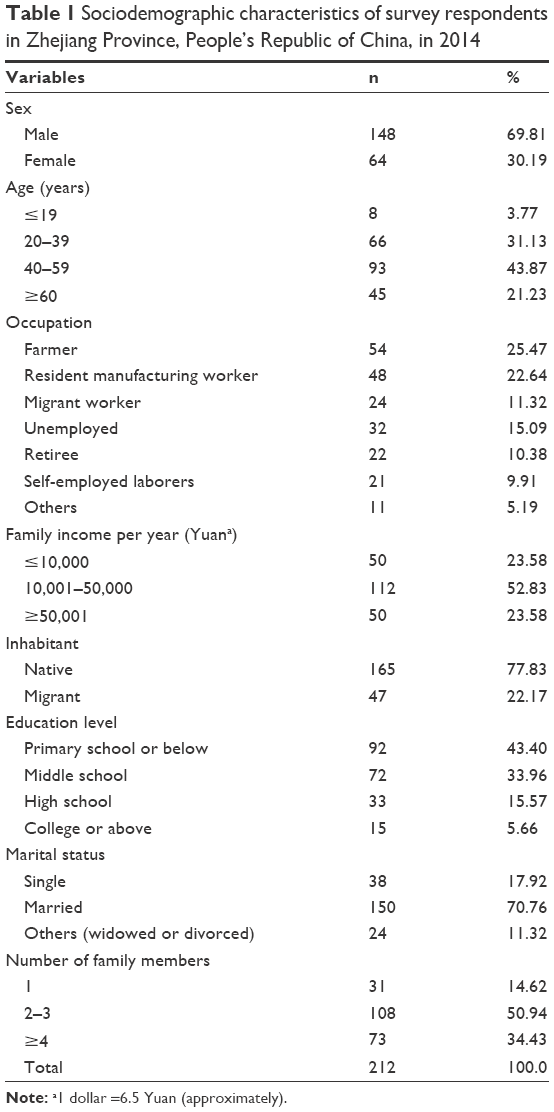 | Table 1 Sociodemographic characteristics of survey respondents in Zhejiang Province, People’s Republic of China, in 2014 |
Social support scores of the participants
The average SSRS score of the 212 participants was 32.56±7.86, consisting of the average scores of subjective support (20.36±5.42), objective support (6.66±2.66), and support-seeking behavior (5.53±2.05).
Participants’ social support scores and sociodemographic characteristics
The married MDR-TB patients had significantly higher average SSRS scores than the single, widowed, and divorced participants, and the scores of subjective support and objective support also showed the same pattern (P<0.01). Patients who had more family members tended to have significantly higher SSRS, subjective support, and objective support scores (P<0.01). The patients whose annual family income was ≥50,001 Yuan had significantly higher SSRS, subjective support, and objective support scores than the other two groups (P<0.01). The 40–59-year age group had a higher subjective support score than the other age groups (P<0.05; Table 2).
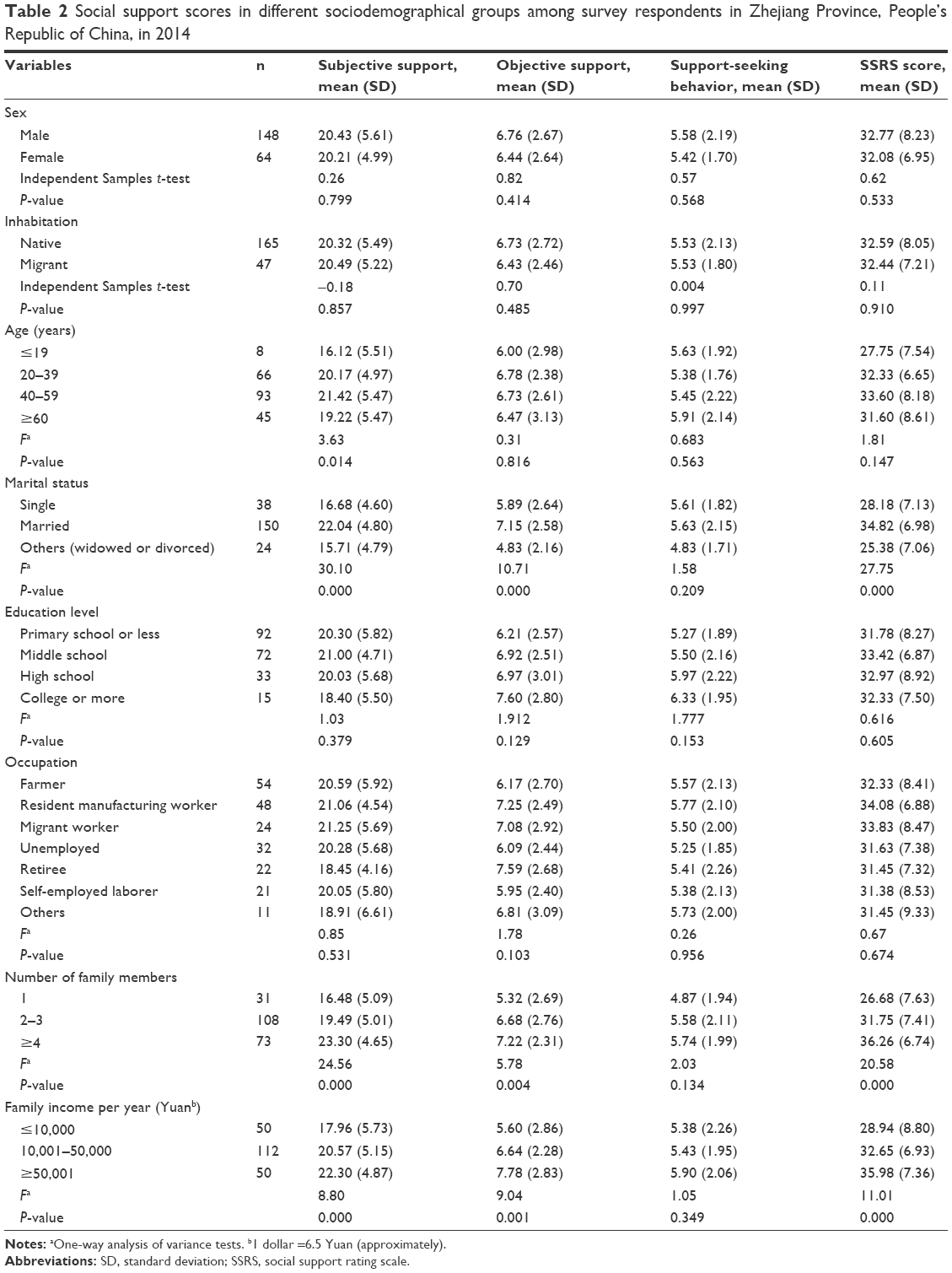 | Table 2 Social support scores in different sociodemographical groups among survey respondents in Zhejiang Province, People’s Republic of China, in 2014 |
The social support scores among participants with different disease features and attitudes
The groups with different treatment histories, disease complications, and difficulty moving during treatment showed no significant differences in SSRS, subjective support, objective support, or support-seeking behavior (Table 3).
 | Table 3 Social support scores among participants with different disease features and attitudes, Zhejiang Province, People’s Republic of China, 2014 |
The participants who objected to disclose that they had the disease had significantly lower SSRS and subjective scores than those who did not object (P<0.05). The participants who felt that their health workers were helpful had significantly higher scores than the other two groups in all domains of social support (P<0.01). If the patients felt that the government’s financial subsidy was helpful, they tended to have higher SSRS and subjective support scores (P<0.01; Table 3).
Multivariate analysis of factors associated with SSRS scores
The R2 coefficient of the final multiple linear regression model was 0.43 (P<0.01). Variables of marital status, occupation, number of family members, annual family income, difficulty moving during treatment, objections to disclose that they were MDR-TB patients, and feeling helped by health care workers were statistically significant in the model. Patients who were single, widowed, or divorced had lower SSRS scores than those who were married (P=0.000 and 0.001). Compared with patients who were retirees, resident manufacturing workers had a higher SSRS score (P=0.024). MDR-TB participants whose family members numbered four or above had higher social support scores (P=0.000). Greater annual family income (≥50,001) was associated with the higher SSRS scores of participants (P=0.014). Participants who did not object to disclose that they were MDR-TB patients tended to receive more social support (P=0.010). Patients who felt they had perceived moderate and no help from their health care workers had significantly lower SSRS scores than the other patients (P=0.007 and 0.014; Table 4).
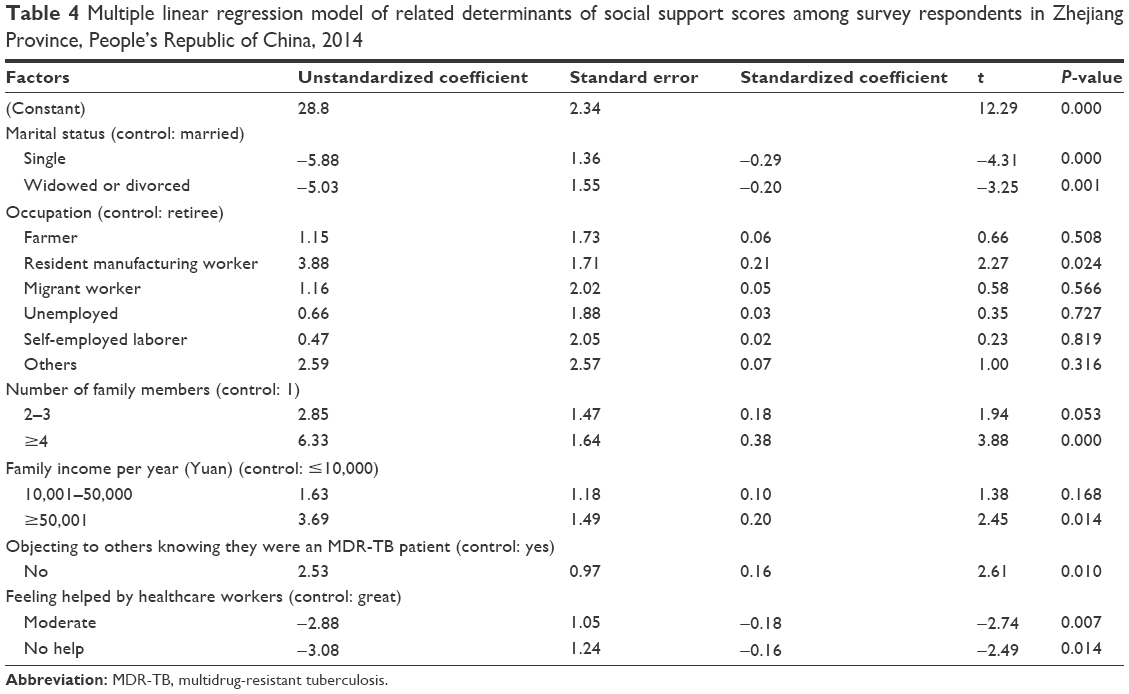 | Table 4 Multiple linear regression model of related determinants of social support scores among survey respondents in Zhejiang Province, People’s Republic of China, 2014 |
Discussion
The social support scores of MDR-TB patients in the current study were lower than the national average level of 34.56.26 The scores were also lower than that among those who did not have a TB disease in other studies.20,21,27,28 The SSRS scores of MDR-TB patients in our study were lower than those reported for TB patients in other recent domestic studies of social support among TB patients (the score ranged roughly from 32 to 36) and did not differ from the results of previous studies on MDR-TB patients.23–25,31–34 Limited social support was an important risk factor for nonadherence to medication regimes and treatment.6,25,35,36 The results indicate that MDR-TB patients may lack social support from their surroundings, including their communities, family members, and relatives. MDR-TB patients may be classified as one of the most vulnerable population groups.
Family is a reliable shelter for the MDR-TB patients, upon which they can depend during treatment. Family members are often best suited to offer emotional and financial support to patients.16,37 The results of the current study showed that patients who were married and had larger families had higher social support, subjective and objective support scores than their counterparts. Studies have also shown that financial assistance is essential for TB patients to successfully finish the treatment.8,16 Patients in families who earned more income per year tended to receive more support than those in the current study. The People’s Republic of China continues to face the challenge of an aging population and has the largest population of the elderly in the world.38 Retirees had lower SSRS scores than active workers in our study. Due to the increasing burden of care, retired MDR-TB patients may receive less social support due to lack of caregivers. The one-way analysis of variance showed differences in subjective support scores among patients >60 years, <19, 20–39 years, and 40–59 years old. Other factors, such as sex, inhabitation, and education level, had no significant relationship with the amount of social support received.
Because MDR-TB is a severe disease, treatment history, complications, and physical activity were not significantly associated with the reception of social support among MDR-TB patients. Other clinical features such as sputum smear results (positive) and symptoms (cough and cough sputum) were almost the same among MDR-TB patients, so influence on social support reception was also limited. MDR-TB patients underwent longer treatment periods and experienced more serious side effects and physical difficulties. Caregivers may also lose confidence during treatment, which may contribute to reduced social support.25,39
Fears over TB transmission, becoming the target of gossip, and discrimination from the community are believed to be the causes of patient self-discrimination.12 Attitudes, such as objecting to disclose the status of their disease or fear of contact with others, were found to likely block channels of outside social support.16 In the current study, the patients who did not object to disclose their disease status had more subjective support and SSRS scores. This may suggest that such groups of patients had been accepted by the surrounding individuals and the community who could offer support. The provision of health services is also a very important source of support for TB patients.16,17 Patients felt very supported when they interacted with doctors, nurses, and health promoters.16,37 The current results indicate that MDR-TB patients who felt supported by health care workers tended to receive more social support, which indicated the important role of health care workers.
Limitations
The current study had some limitations. The MDR-TB respondents were only from Zhejiang Province and were not representative of all MDR-TB patients. The lack of control groups hindered comparisons with other population groups. Although the majority of MDR-TB patients were interviewed, some patients died or lost contact before the study was conducted, which may have contributed to a loss of relevant information and caused the selection bias leading to overestimation of the social support. The study had not measured the adherence of participants and therefore prevented drawing conclusions on the relationship between social support and adherence in the current study.
Conclusion
This study indicated that MDR-TB patients in Zhejiang Province lack sufficient social support. The MDR-TB patients should be considered a part of the population requiring social protection. The social support received by patients may be associated with the sociodemographic status of marriage, family size, and family income. Patients who were not married, had smaller families, and had low family income tended to receive less social support, showing that family harmony could be an important source of social support. Compared with the patient group, resident manufacturing worker, the retired MDR-TB patients may require more social support. Self-isolation by patients was also identified as an obstacle to social support from the neighbors and communities in our study. Health care workers were found to play an important role in supporting MDR-TB patients and helping them finish treatment.
Acknowledgments
This study was supported by Zhejiang Provincial Science and Technology Major Project (2014C03034), Zhejiang-National Committee of Health and Family Planning Co-Sponsored Project (WKJ-ZJ-07), and Zhejiang Provincial Medical Research project (2016RCA007). We would like to thank the staff from local centers for diseases control and prevention (CDCs) for their help of field survey.
Disclosure
The authors report no conflicts of interest in this work.
References
World Health Organization. Global Tuberculosis Report 2015. Geneva: WHO Press; 2015. | ||
Huang Y, Zhong JM, Chen B, Chen SH, Qiu X, Wang XM. [Epidemiological characteristics of tuberculosis in Zhejiang province, 2010]. Dis Surveill. 2011;26(8):601–603. Chinese. | ||
Wang X, Fu Q, Li Z, et al. Drug-resistant tuberculosis in Zhejiang province, China, 1999–2008. Emerg Infect Dis. 2012;18(3):496–498. | ||
World Health Organization. Towards Universal Access to Diagnosis and Treatment of Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis by 2015: WHO Progress Report 2011. Geneva: WHO; 2011. | ||
Zhao Y, Xu S, Wang L, et al. National survey of drug-resistant tuberculosis in China. N Engl J Med. 2012;366(23):2161–2170. | ||
Figueroa-Munoz JI, Ramon-Pardo P. Tuberculosis control in vulnerable groups. Bull World Health Organ. 2008;86(9):733–735. | ||
Gao XF, Rao Y. Quality of life of a migrant population with tuberculosis in West China. Int J Tuberc Lung Dis. 2015;19(2):223–230. | ||
Potter JL, Inamdar L, Okereke E, Collinson S, Dukes R, Mandelbaum M. Support of vulnerable patients throughout TB treatment in the UK. J Public Health (Oxf). Epub 2015 Apr 17. | ||
Xu K, Evans DB, Carrin G, AM A-R. Designing Health Financing Systems to Reduce Catastrophic Health Expenditure. Technical Brief for Policy-Makers. Geneva: WHO; 2005. | ||
Grede N, Claros JM, de Pee S, Bloem M. Is there a need to mitigate the social and financial consequences of tuberculosis at the individual and household level? AIDS Behav. 2014;18(suppl 5):S542–S553. | ||
Long NH, Johansson E, Diwan VK, Winkvist A. Fear and social isolation as consequences of tuberculosis in VietNam: a gender analysis. Health Policy. 2001;58(1):69–81. | ||
Baral SC, Karki DK, Newell JN. Causes of stigma and discrimination associated with tuberculosis in Nepal: a qualitative study. BMC Public Health. 2007;7:211. | ||
Pooran A, Pieterson E, Davids M, Theron G, Dheda K. What is the cost of diagnosis and management of drug resistant tuberculosis in South Africa? PLoS One. 2013;8(1):e54587. | ||
Chen B, Wang XM, Zhong J, SH C. [Evaluation on multidrug-resistant tuberculosis control strategies in 5 pilot cities in Zhejiang province]. Chin J Public Health. 2014;30(4):385–387. Chinese. | ||
Minghui R, Scano F, Sozi C, Schwartlander B. The Global Fund in China: success beyond the numbers. Lancet Glob Health. 2015;3(2):e75–e77. | ||
Paz-Soldan VA, Alban RE, Jones CD, Oberhelman RA. The provision of and need for social support among adult and pediatric patients with tuberculosis in Lima, Peru: a qualitative study. BMC Health Serv Res. 2013;13:290. | ||
Alagna R, Diaw MM, Centis R, Cirillo DM, Besozzi G. Universal health coverage and social support in Senegal: a comprehensive approach against tuberculosis. Eur Respir J. 2015;46(3):869–871. | ||
Cobb S. Presidential Address-1976. Social support as a moderator of life stress. Psychosom Med. 1976;38(5):300–314. | ||
Tamayo T, Fischer-Betz R, Beer S, Winkler-Rohlfing B, Schneider M. Factors influencing the health related quality of life in patients with systemic lupus erythematosus: long-term results (2001–2005) of patients in the German Lupus Erythematosus Self-Help Organization (LULA Study). Lupus. 2010;19(14):1606–1613. | ||
Lin QH, Jiang CQ, Lam TH. The relationship between occupational stress, burnout, and turnover intention among managerial staff from a Sino-Japanese joint venture in Guangzhou, China. J Occup Health. 2013;55(6):458–467. | ||
Xu J, Wei Y. Social support as a moderator of the relationship between anxiety and depression: an empirical study with adult survivors of Wenchuan earthquake. PLoS One. 2013;8(10):e79045. | ||
Chen R, Tao F, Ma Y, Zhong L, Qin X, Hu Z. Associations between social support and condom use among commercial sex workers in China: a cross-sectional study. PLoS One. 2014;9(12):e113794. | ||
Yang L, Wu DL, Guo HG, Liu JW. [A study of the psychological and social factors in patients with pulmonary tuberculosis]. Chin J Tuberc Respir Dis. 2003;26(11):704–707. Chinese. | ||
XH W, LJ W, YH Y, et al. [The investigation on social support for Tuberculosis patients and the nursing strategy]. Zhonghua Hu Li Za Zhi. 2007;42(2):143–145. Chinese. | ||
Wang AM, Bai ZX, Liu JF. [Depression and social support status of multidrug-resistant tuberculosis patients]. Chin J Antituberc. 2013;35(2):142–145. Chinese. | ||
Xiao SY. [The theoretical basis and application of social support rating scale]. J Clin Psychiatry. 1994;4(2):98–100. Chinese. | ||
Deng J, Hu J, Wu W, Dong B, Wu H. Subjective well-being, social support, and age-related functioning among the very old in China. Int J Geriatr Psychiatry. 2010;25(7):697–703. | ||
Su D, Wu XN, Zhang YX, et al. Depression and social support between China’ rural and urban empty-nest elderly. Arch Gerontol Geriatr. 2012;55(3):564–569. | ||
Xu J, Ou L. Resilience and quality of life among Wenchuan earthquake survivors: the mediating role of social support. Public Health. 2014;128(5):430–437. | ||
Ke X, Liu C, Li N. Social support and quality of life: a cross-sectional study on survivors eight months after the 2008 Wenchuan earthquake. BMC Public Health. 2010;10:573. | ||
Xie RQ, Cheng JQ, Yang YZ, et al. [The social support state of the tuberculosis patient in floating population]. Chin J Behav Med Sci. 2006;15(5):437–439. Chinese. | ||
Chen TH, Zhong Q, Li PF, Jiang L, Wen LH. [The relationship between Psychological status and social support among multidrug-resistant tuberculosis patients]. Guangdong Med J. 2006;27(12):1892–1894. Chinese. | ||
Zhao R, Xiang YJ. [Study on the correlation of quality of life with social support in tuberculosis patients]. Pract Prev Med. 2012;19(11):1636–1638. Chinese. | ||
He XY, Wu LM, Cao RF, et al. [A study on the relationship between mental health status and medication adherence in tuberculosis patients]. Zhejiang Prev Med. 2014;26(3):229–241. Chinese. | ||
Jakubowiak WM, Bogorodskaya EM, Borisov SE, Danilova ID, Lomakina OB, Kourbatova EV. Social support and incentives programme for patients with tuberculosis: experience from the Russian Federation. Int J Tuberc Lung Dis. 2007;11(11):1210–1215. | ||
Lonnroth K, Glaziou P, Weil D, Floyd K, Uplekar M, Raviglione M. Beyond UHC: monitoring health and social protection coverage in the context of tuberculosis care and prevention. PLoS Med. 2014;11(9):e1001693. | ||
Munro SA, Lewin SA, Smith HJ, Engel ME, Fretheim A, Volmink J. Patient adherence to tuberculosis treatment: a systematic review of qualitative research. PLoS Med. 2007;4(7):e238. | ||
Sun R, Cao H, Zhu X, Liu JP, Dong E. Current aging research in China. Protein Cell. 2015;6(5):314–321. | ||
Cheng H. [Research on relationship between social support and mental health of the multidrug-resistant tuberculosis Patients in Wuhan]. Med Soc. 2013;26(9):77–80. Chinese. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.