Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 12
Safety and Tolerability of PCSK9 Inhibitors: Current Insights
Authors Kosmas CE, Skavdis A, Sourlas A, Papakonstantinou EJ, Peña Genao E, Echavarria Uceta R, Guzman E
Received 31 October 2020
Accepted for publication 1 December 2020
Published 11 December 2020 Volume 2020:12 Pages 191—202
DOI https://doi.org/10.2147/CPAA.S288831
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Arthur E. Frankel
Constantine E Kosmas,1 Andreas Skavdis,2 Andreas Sourlas,3 Evangelia J Papakonstantinou,4 Edilberto Peña Genao,5 Rogers Echavarria Uceta,5 Eliscer Guzman1
1Division of Cardiology, Department of Medicine, Montefiore Medical Center, Bronx, NY, USA; 2School of Medicine, University of Athens, Athens, Greece; 3School of Medicine, University of Crete, Heraklion, Greece; 4General Directorate of Public Health and Social Welfare, Attica Region, Athens, Greece; 5Cardiology Clinic, Cardiology Unlimited, PC, New York, NY, USA
Correspondence: Constantine E Kosmas 168-24 Powells Cove Blvd., Beechhurst, NY 11357, USA
Tel +1-646-734-7969
Email [email protected]
Abstract: The current era of preventive cardiology continues to emphasize on low-density lipoprotein cholesterol (LDL-C) reduction to alleviate the burden of atherosclerotic cardiovascular disease (ASCVD). In this regard, the pharmacological inhibition of proprotein convertase subtilisin/kexin type 9 (PCSK9) enzyme via monoclonal antibodies has emerged as a novel lipid-lowering therapy, leading to a marked reduction in circulating LDL-C levels and subsequent improvement of cardiovascular outcomes. As these agents are increasingly used in current clinical practice, mounting scientific and clinical evidence supports that PCSK9 inhibitors offer an excellent safety and tolerability profile with a low incidence of adverse events. Notably, the most frequently reported side effects are injection-site reactions. In contrast to statins, PCSK9 inhibitors do not appear to exert a detrimental effect on glycemic control or to increase the incidence of new-onset diabetes mellitus. Accumulating evidence also indicates that PCSK9 inhibitors are a safe, well-tolerated and effective therapeutic strategy for patients with statin intolerance. On the other hand, as PCSK9 inhibitors reduce LDL-C to unprecedented low levels, a large body of current research has examined the effects of their long-term administration on neurocognition and on levels of vitamin E and other fat-soluble vitamins, providing encouraging results. This review aims to present and discuss the current clinical and scientific evidence pertaining to the safety and tolerability of PCSK9 inhibitors.
Keywords: hypercholesterolemia, cardiovascular disease, CVD, PCSK9 inhibitors, safety, tolerability
Introduction
Cardiovascular disease (CVD) has consistently been the leading cause of mortality worldwide, accounting for 17.8 million deaths in 2017.1 Hypercholesterolemia represents a major risk factor for CVD. The major sites for cholesterol synthesis are in hepatocytes and enterocytes. The intestinal cholesterol pool size is influenced mostly by endogenous sources, as the diet contributes only 25–30% of cholesterol per day. The reaction that represents the key point of regulation in cholesterol synthesis is the reduction of HMG-CoA to mevalonate and is catalyzed by the enzyme HMG-CoA reductase, which is inhibited by statins. The LDL receptors (LDLR), located on the cell membranes of hepatocytes and other cells, are responsible for cholesterol uptake. Reverse cholesterol transport (RCT) is the major pathway for cholesterol removal and is an essential mechanism to maintain cellular cholesterol homeostasis. Cholesterol efflux from macrophages can occur through a unidirectional ATP-dependent pathway mediated by ATP-binding cassette transporter A1 (ABCA1) and/or ATP-binding cassette transporter G1 (ABCG1), as well as by scavenger receptor class B type 1 (SR-BI), in a bidirectional ATP-independent pathway. The efflux of cholesterol can also occur through a receptor-independent diffusion of cholesterol in a gradient dependent process, which contributes to 30% of total cholesterol efflux.2
It has been unequivocally proven that increased levels of low-density lipoprotein cholesterol (LDL-C) are a causative modifiable risk factor for developing CVD, as LDL-C plays an undeniably pivotal role in the pathogenesis and progression of the atherosclerotic process.3 The use of lipid-modifying therapies has elicited a substantial decrease in the occurrence of major adverse CV events, thus being a fundamental pillar in current preventive cardiology practice.4
The recent development of proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors, which was driven by novel genetic and mechanistic insights, was a remarkable achievement that addressed several unmet needs in the management of hyperlipidemia. Regulation of PCSK9 expression is dependent upon genetic factors, as well as upon factors associated to a complex transcriptional system, mainly controlled by sterol regulatory element binding proteins. In addition, PCSK9 is further regulated by lipid-lowering drugs, particularly by statins, which increase PCSK9 secretion but decrease its stimulatory phosphorylated form.5 The physiological role of PCSK9 is the enhancement of the endosomal and lysosomal degradation of hepatic LDL-R, resulting in increased circulating LDL-C levels.6 Thus, the use of PCSK9 inhibitors, which are human monoclonal antibodies that target and inhibit the PCSK9 enzyme, leads to the upregulated recycling and expression of LDL-R at the cell surface and, ultimately, to more rapid clearance of LDL-C from the bloodstream. Indeed, many clinical studies have proven that PCSK9 inhibitors, either as a monotherapy or in combination with statins, produce a potent and robust reduction in circulating LDL-C values. Notably, a meta-analysis of 71 randomized, placebo-controlled clinical trials demonstrated that PCSK9 inhibitors provide a marked decrease of 50.7% in LDL-C serum concentrations, as compared to placebo.7 Thus, the use of PCSK9 inhibitors has been approved in both US and Europe for patients with clinical ASCVD or FH who require further LDL-C-lowering in combination with other lipid-lowering treatments, although eligibility for PCSK9 inhibitor treatment differs based on the 2018 American College of Cardiology (ACC)/American Heart Association (AHA) and 2019 European Society of Cardiology (ESC)/European Atherosclerosis Society (EAS) recommendations. More specifically, the 2019 ESC/EAS guidelines rendered 51% of all post-acute coronary syndrome (ACS) patients potentially eligible for PCSK9 inhibitor treatment, as compared to a 14% eligibility rate based on the 2018 ACC/AHA guidelines.8 On the other hand, apart from their beneficial effect in LDL-C lowering, PCSK9 inhibitors represent also an emerging therapeutic strategy for the treatment of hyperlipoproteinemia (a).9 In addition, aside from plain lipid-lowering, PCSK9 inhibition may also exert additional beneficial effects. More specifically, there are data indicating that reduced PCSK9 function increases LDLR-mediated pathogen lipid clearance and thus reduces the inflammatory response and improves outcomes in sepsis in both mice and humans.10,11
Despite a dramatic reduction in LDL-C, PCSK9 inhibitors, in contrast to statins and the recently approved LDL-C-lowering agent, bempedoic acid, do not reduce high-sensitivity C-reactive protein (hs-CRP), a major biomarker of inflammation and associated risk in CVD.12,13 This may fuel skepticism regarding the effects of PCSK9 inhibitor therapy on cardiovascular (CV) outcomes. However, long-term outcome studies have unequivocally demonstrated that the that LDL-C lowering effect of PCSK9 inhibitors also translates into substantial clinical benefit with significant improvement in CV outcomes.14,15 Notably, the higher risk patients, such as those with a more recent coronary event, those with higher baseline LDL-C levels, those with diabetes mellitus (DM) and prior revascularization, as well as those with ASCVD and peripheral arterial disease, appear to benefit the most.16 Given the above, PCSK9 inhibitors have ushered in the current era of lipid-lowering therapy, emerging as a valuable therapeutic approach for the optimal management of hyperlipidemia.17
Adding to their effectiveness in LDL-C lowering, PCSK9 inhibitors also possess a favorable safety and tolerability profile with a low incidence of adverse events and high therapeutic compliance among patients in clinical trials, in which the cost of therapy is not an impediment. Notably, the most frequently reported side effects are mild injection-site reactions. Moreover, PCSK9 inhibitors have been thoroughly assessed in patients with DM and statin intolerance, and they do not appear to exert a detrimental effect on glucose homeostasis or cause muscle-related symptoms. Notwithstanding, mainly due to the long-term use and the unprecedented low levels of LDL-C achieved by PCSK9 inhibition, concerns regarding potential adverse effects on neurocognition and fat-soluble vitamin (especially vitamin E) levels associated with the use of PCSK9 inhibitors have been raised. However, clinical trials have provided considerable evidence that no such association exists. This review aims to present and discuss the current clinical and scientific evidence pertaining to the safety and tolerability of PCSK9 inhibitors.
Adverse Events of PCSK9 Inhibitors
Many genetic and clinical studies have provided mounting evidence that the causal effect of LDL-C on the risk of CV disease is determined by both the absolute circulating levels and the cumulative duration of exposure of the vasculature to LDL-C.3 Therefore, as prompt initiation and long-term continuation of lipid-modifying therapies are supported nowadays, long-term safety and tolerability of these interventions are of utmost importance to determine therapeutic compliance, which would be a critical factor for the successful prevention of CVD and its associated mortality.18 As alluded earlier, accumulating evidence suggests that PCSK9 inhibitors have a favorable safety and tolerability profile. Common side effects of PCSK9 inhibitors are generally mild and include nasopharyngitis, injection-site reactions, and upper respiratory tract infections.17
Several clinical trials have evaluated the safety profile of PCSK9 inhibitors up to date. In the ODYSSEY LONG TERM trial, which studied 2341 patients on maximum tolerated statin therapy over a follow-up period of 78 weeks, adverse events that occurred more frequently with alirocumab, as compared with placebo, included injection-site reactions, myalgia, neurocognitive events, and ophthalmologic events. In addition, more patients in the alirocumab group, as compared with placebo, had vitamin E or vitamin K levels below the lower limit of the normal range; however, no clinically meaningful changes were demonstrated.19 Furthermore, in the OSLER-1 and OSLER-2 studies, which consisted of 4465 patients in total, the incidence of adverse events was in general similar in the evolocumab and the standard-therapy groups during 11.1 months of follow-up, although adverse neurocognitive events were reported more frequently in patients receiving evolocumab. Notably, such events were rare (<1% of patients) and were not correlated with the LDL-C levels during treatment.20 Unsurprisingly, the reported increased rate of neurocognitive events associated with PCSK9 inhibitor treatment had fueled skepticism regarding the safety profile of PCSK9 inhibition.
Fortunately, subsequent studies did not confirm the above findings. The FOURIER and ODYSSEY OUTCOMES clinical trials demonstrated that there was no significant difference in the incidence of adverse events, including neurocognitive events and new-onset diabetes mellitus, between patients receiving a PCSK9 inhibitor versus placebo. Notably, the incidence of injection-site reactions was more frequent in patients receiving PCSK9 inhibitors; however, this finding did not raise any concern, as the large majority of these reactions were mild.14,15 On the other hand, a prespecified secondary analysis of the FOURIER trial provided insights into the effect of extremely low LDL-C concentrations induced by PCSK9 inhibition, demonstrating that neither serious adverse events nor adverse events leading to drug discontinuation occurred more frequently in patients with plasma LDL-C values <15 mg/dl. This marked reduction in circulating LDL-C levels actually led to further improvement of CV outcomes, thus indicating that the approach of “the lower, the better” regarding circulating LDL-C levels may be feasible and convincing.21
Several subsequent studies provided similar results and a meta-analysis of 32 randomized, placebo-controlled clinical trials, including 57,090 patients in total, demonstrated that anti-PCSK9 monoclonal antibodies were in general safe, but for the increased risk of injection site reactions [Relative Risk (RR): 1.54; P<0.001].22 Furthermore, in the OSLER-1 study, PCSK9 inhibitor therapy demonstrated durable efficacy and a consistent safety profile during exposure of up to 5 years. Adverse events did not increase over time and were comparable to those of the standard-therapy group.23 Thus, there is optimism that the long-term administration of PCSK9 inhibitors is safe, tolerable, and efficacious, although further clinical studies are warranted to corroborate these findings.
Finally, another issue that may raise concerns with the use of monoclonal antibodies is their immunogenicity, ie, an immune response that leads to the production of anti-drug antibodies and neutralizing antibodies, which could impact on the safety and efficacy of the drugs. However, very low rates of immunogenicity were observed in clinical trials of evolocumab and alirocumab (the two approved PCSK9 inhibitors).20,24 In a study, which analyzed data from 10 trials involving 4747 patients, 5.1% of patients being treated with alirocumab developed anti-drug antibodies. However, even in those patients, the LDL-C-lowering effect of alirocumab was not adversely affected.24,25
Below, we will address more specifically the effects of PCSK9 inhibitors on the risk of DM, on the incidence of myalgias, especially in statin-intolerant patients, on neurocognition, as well as on serum soluble vitamin (especially vitamin E) levels. In addition, we will briefly discuss the cost-effectiveness of PCSK9 inhibitor therapy.
PCSK9 Inhibitors and Diabetes Mellitus
Diabetes mellitus (DM) is a chronic, multisystem metabolic disorder that constitutes a growing public health problem throughout the world. DM is a well-established CV risk factor that leads to accelerated atherosclerosis, microvascular and macrovascular disease. As dyslipidemia is very common in patients with DM, with a prevalence of 72%-85%, individuals with DM constitute an important group of patients in need of lipid-modifying therapy.26 Although statin therapy remains the cornerstone of dyslipidemia management in current clinical practice, overwhelming evidence suggests that statins adversely affect glycemic control and increase the risk of new-onset DM by 9% to 44% in different studies.27 Thus, after the development of PCSK9 inhibitors, a critical question that emerged was whether the use of this new class of lipid lowering agents could be safe, tolerable and beneficial for patients with DM.
A large body of recent research investigated the effect of several alleles at the PCSK9 locus on the incidence of DM. In a meta-analysis of genetic association studies, for certain PCSK9 genetic variants there was a 19% increase in the incidence of type 2 DM per 1 mmol/L (38.67 mg/dl) genetically predicted reduction in LDL-C (P=0.03).28 Furthermore, in a mendelian randomization analysis, after adjustment for a standard decrement of 10 mg/dl in the LDL-C level, PCSK9 variants were associated with an 11.2% increase in the risk of DM.29 In addition, a large-scale mendelian randomization study demonstrated that certain genetic PCSK9 variants, scaled to 1 mmol/L lower LDL-C, were associated with a 29% increase in the risk of type 2 DM. Moreover, these specific PCSK9 variants were associated with adverse metabolic consequences, including increased fasting glucose, bodyweight, and waist-to-hip ratio.30 Undoubtedly, these genetic studies have fueled skepticism that the long-term exposure to decreased PCSK9 and LDL-C levels, induced either by genetic variations or pharmacotherapy, may lead to impaired glucose homeostasis and DM. On the other hand, in an interesting recent study, it was shown that depression was associated also with the homeostatic model assessment index of insulin resistance (HOMA-IR), 11% of this effect operating indirectly via PCSK9.31
Based on the above, several studies assessed the effects of PCSK9 inhibitors on the incidence of DM. A prespecified analysis of the FOURIER trial demonstrated that the risk of new-onset DM in patients without DM or prediabetes at baseline was not increased with evolocumab treatment during 2.2 years of follow-up. Furthermore, the levels of glycated hemoglobin (HbA1c) and fasting plasma glucose (FPG) were not significantly different between evolocumab and placebo groups in patients with DM, prediabetes, or normoglycemia. Importantly, PCSK9 inhibition with evolocumab significantly reduced CV risk in patients with and without DM.32,33 Subsequent studies also corroborated the results obtained from the FOURIER analysis. The OSLER-1 extension study, having a longer follow-up period, documented that the annualized incidence of new-onset DM was not increased by evolocumab during 4 years of treatment. More specifically, in the OSLER-1 extension study, the annualized incidence of new-onset DM was 4% in the standard of care (SOC) treatment alone group versus 2.8% in the evolocumab plus SOC treatment group after adjustment for the duration of evolocumab exposure.33,34 Moreover, a post-hoc analysis of the ODYSSEY LONG TERM trial, comprising 812 individuals with type 2 DM, reported that FPG and HbA1c levels remained constant over 78 weeks with alirocumab treatment, regardless of the presence or absence of mixed dyslipidemia.35 In addition, the results of a large-scale meta-analysis of 38 randomized controlled trials were also in line with that of the aforementioned studies, as it was shown that treatment with PCSK9 inhibitors was effective, in terms of LDL-C lowering and reduction of adverse cardiovascular events, in patients with and without DM, while the risk of incident DM was not increased by PCSK9 inhibitor therapy.36
Given the above, sufficient evidence indicates that PCSK9 inhibitors achieve substantial CV benefit without adversely affecting glucose metabolism or increasing the incidence of new-onset DM. Notwithstanding, further clinical trials with a longer follow-up period may be needed to definitely confirm these findings.
PCSK9 Inhibitors in Patients with Statin Intolerance/Myalgias
Over the past few decades, the mainstay of lipid-lowering treatment has been statin therapy, significantly decreasing the incidence of major adverse CV events in both primary and secondary prevention.37 However, intolerance to statins, mostly due to muscle-related symptoms and weakness, may occur in some patients. This constitutes an essential barrier to maintaining long-term medication adherence, which subsequently leads to inadequate LDL-C reduction and increased mortality.38,39 In this regard, two large-scale retrospective studies provided consistent results, demonstrating that the adherence rates to statin therapy were very low, as 53% of patients discontinued their therapy.40,41
In view of the above, and as PCSK9 inhibitors represent a novel addition to the lipid-lowering armamentarium, clinical trials have sought to determine whether PCSK9 inhibitors can cause myalgia or myopathy, which would potentially prevent their administration in statin-intolerant patients. The DESCARTES study, a randomized, placebo-controlled, Phase 3 trial, which was conducted to evaluate the safety and efficacy of 52 weeks of treatment with evolocumab in 901 hyperlipidemic patients, provided encouraging results, as elevation of creatine kinase (CK) levels to more than five times the upper limit of the normal range or myalgia occurred only in 1.2% and 4% of evolocumab-treated patients, respectively. Furthermore, the occurrence of these adverse events was similar between patients receiving evolocumab or placebo.42 A subsequent meta-analysis of 35 randomized controlled trials, consisting of 45,539 patients in total, confirmed the above findings, as it demonstrated that compared with no treatment with a PCSK9 inhibitor, treatment with a PCSK9 inhibitor was associated with a trend of fewer increases in CK [Odds Ratio (OR): 0.84; P=0.06] and was not associated with a statistically significant change in the rates of myalgia (OR: 0.95; P=0.65).43
In addition, in ODYSSEY ALTERNATIVE, a randomized, double-blind, double-dummy, active-controlled, parallel-group study, which compared alirocumab with ezetimibe in 314 patients at moderate to high CV risk with statin intolerance, and included by protocol a statin rechallenge arm, it was shown that musculoskeletal adverse events were less frequent with alirocumab vs atorvastatin [hazard ratio (HR): 0.61; P=0.042]. Importantly, alirocumab decreased mean LDL-C by 45.0% vs 14.6% with ezetimibe.44
In the GAUSS-3 study, which included patients with statin intolerance due to muscle-related side effects, treatment with evolocumab compared with ezetimibe led to a significantly greater lowering of LDL-C levels after 24 weeks (52.8% vs 16.7%; P<0.001). Active study drug was discontinued owing to muscle symptoms in 5 of 73 ezetimibe-treated patients (6.8%) and only 1 of 145 evolocumab-treated patients (0.7%).45 These findings were corroborated by the results of a subset analysis of the OSLER open-label extension studies, which showed that evolocumab plus SOC therapy was consistently safe, tolerable, and efficacious for up to 2 years in statin-intolerant patients.46
Indeed, statin-intolerance currently represents an essential reason for initiating treatment with PCSK9 inhibitors, as, according to a recent study, physician-reported reasons for switching from statins to PCSK9 inhibitor therapy included myalgia in 28.6% of cases and myopathy in 11.1% of cases.47
PCSK9 Inhibitors and Neurocognitive Events
The brain is the most cholesterol-rich organ in the body, composing almost 25% of the body’s total cholesterol; however, its cholesterol synthesis and regulation is isolated from peripheral tissues. Neither cholesterol nor PCSK9 can cross the blood-brain barrier under normal conditions.48 PCSK9-inhibitors cannot also cross the blood-brain barrier in humans.49 Notwithstanding, as mentioned before, some earlier studies had reported a somewhat increased rate of adverse neurocognitive events associated with the use of PCSK9 inhibitors, as compared with placebo.19,20 However, subsequent studies did not confirm the above findings, as the FOURIER and ODYSSEY OUTCOMES clinical trials demonstrated that there was no significant difference in the rate of adverse neurocognitive events between patients receiving a PCSK9 inhibitor versus placebo.14,15 A potential explanation for this discrepancy may be the lack of standardized cognitive testing and reliance on patients’ self-reporting of what constituted as a neurocognitive deficit in the earlier trials. This may have led to a reporting bias contributing to the increase in neurocognitive deficits noted in the earlier studies and especially in the OSLER studies which were an open-label trial.50
Notwithstanding, in order to better clarify this issue, a randomized, double-blind, placebo-controlled, multicenter study (EBBINGHAUS study) was conducted, which involved a subgroup of patients from the FOURIER trial. The EBBINGHAUS study prospectively assessed the cognitive function in 1204 patients using the Cambridge Neuropsychological Test Automated Battery. The patients were followed for a median of 19 months. The mean (±SD) change from baseline over time in the raw score for the spatial working memory strategy index of executive function (primary end point) was −0.21±2.62 in the evolocumab group and −0.29±2.81 in the placebo group (P<0.001 for noninferiority; P=0.85 for superiority). Furthermore, there were no significant differences between groups in the secondary end points of scores for working memory, episodic memory, or psychomotor speed. Importantly, in an exploratory analysis, there were no associations between LDL-C levels and cognitive changes. Thus, in this randomized trial, which involved patients who received either evolocumab or placebo in addition to statin treatment, there were no significant differences observed between groups in cognitive function over a median of 19 months.51
The findings of the EBBINGHAUS study were corroborated by the results of two more recent meta-analyses, which demonstrated that there was no difference in the risk of neurocognitive deficits between PCSK9 inhibitors and control groups.50,52 In addition, no association was found between neurocognitive treatment-emergent adverse events and LDL-C<25 mg/dL.50
Furthermore, in a very recent study, which evaluated patient-reported cognition in the entire FOURIER trial using a self-survey, it was shown that the addition of evolocumab to maximally tolerated statin therapy had no impact on patient-reported cognition after an average of 2.2 years of treatment, even among patients who achieved LDL-C levels <20 mg/dl.53
Based on the above, it appears reasonable to conclude that PCSK9 inhibitor therapy does not cause any major harmful cognitive effects. However, it is unclear if this expectation can be extrapolated to periods of therapy of >3 years or to patients older than 75 years of age, those at very high ASCVD risk, or those with histories of ischemic or hemorrhagic stroke, since in these subgroups of patients there are not enough data to form a definitive conclusion. For that reason, studies with longer follow-up periods and more diverse trial populations are needed.54
Effect of PCSK9 Inhibitor Therapy on Vitamin E and Other Fat-Soluble Vitamins
Vitamin E is an essential fat-soluble micronutrient that possesses several beneficial biological activities, mostly due to its potent antioxidant properties. Vitamin E deficiency, although rare in humans, can originate from a broad spectrum of diseases and its primary clinical features include neuromuscular disorders, retinopathy, impairment of the immune response, and anemia.55 Vitamin E is transported in plasma almost exclusively by lipoproteins and preferentially apolipoprotein B (ApoB)-containing lipoproteins, including LDL.56 In this regard, abetalipoproteinemia and familial hypobetalipoproteinemia, which are genetic diseases characterized by absent or extremely low circulating LDL-C, triglycerides, and ApoB-containing lipoproteins, cause severe deficiency of fat-soluble vitamins, including vitamin E.57 The elucidation of the underlying molecular mechanisms involved in these rare genetic diseases has established the robust association between vitamin E transport and LDL-C metabolism. Thus, the above evidence gave rise to a theoretical concern that markedly low LDL-C plasma concentrations induced by pharmacotherapy may cause vitamin E deficiency.58 Therefore, clinical trials evaluated the effect of lipid-lowering therapeutic interventions, and particularly PCSK9 inhibitors that decrease LDL-C to previously unprecedented levels, on fat-soluble vitamins, especially vitamin E.
The aforementioned DESCARTES study, a phase 3, double-blind, randomized, placebo-controlled clinical trial, also assessed the safety of evolocumab with regard to vitamin E and steroid hormone levels. The investigators measured vitamin E plasma levels in 738 patients, whereas in a study subset of 80 patients vitamin E values were also measured in serum, LDL, high-density lipoprotein (HDL), and red blood cell membranes (RCM) at baseline and at 52 weeks of treatment. In patients treated with evolocumab, absolute vitamin E levels were reduced by 16% but increased by 19% after normalization for cholesterol levels. In the substudy, in patients treated with evolocumab, serum and LDL vitamin E levels were reduced by 26% and 61%, respectively, while the HDL vitamin E level increased by 31%. These changes reflected the favorable lipid changes induced by the evolocumab treatment. Serum and lipoprotein vitamin E levels did not change significantly after normalization for cholesterol. In addition, vitamin E in RCM remained unchanged from baseline to week 52 (both absolute and normalized). Unsurprisingly, no significant change in vitamin E levels was observed among placebo-treated patients. Moreover, no evidence of impairment of steroid hormone synthesis was found. Thus, in DESCARTES study, it was shown that the marked LDL-C lowering observed in evolocumab-treated patients led to a reduction of absolute serum and LDL vitamin E levels but increased vitamin E levels after normalization for cholesterol. Most importantly, treatment with evolocumab did not alter tissue vitamin E levels, as assessed by RCM vitamin E. No evidence of impairment of adrenal or gonadal steroid hormone synthesis was found, even in patients with extremely low levels of LDL-C (<15 mg/dl).56
In the ODYSSEY LONG TERM trial, as mentioned above, more patients in the alirocumab group, as compared with placebo, had vitamin E or vitamin K levels below the lower limit of the normal range; however, no clinically meaningful changes were demonstrated. Furthermore, when normalized for LDL-C levels, no meaningful changes in vitamin E were observed. In addition, no clinically meaningful effect was observed with respect to changes in levels of other fat-soluble vitamins (vitamin A and vitamin D) or cortisol.19
In a small trial of 11 Japanese patients with heterozygous familial hypercholesterolemia (HeFH) who were switched from biweekly LDL-C apheresis to biweekly subcutaneous injection therapy with evolocumab, serum vitamin E levels were decreased by 20% after 4 weeks of treatment. However, the mean vitamin E levels remained within the normal range and no subjective or objective side effects were observed.59
Furthermore, a very recent prespecified analysis of the BERSON clinical trial (a double-blind, randomized, placebo-controlled, multicenter study, which evaluated the safety and efficacy of evolocumab in combination with statin therapy in diabetic subjects with hyperlipidemia or mixed dyslipidemia) assessed the effect of 12 weeks of treatment with evolocumab on vitamin E and steroid hormones in 981 patients with type 2 diabetes mellitus and dyslipidemia. The results of this study were consistent with those obtained from the DESCARTES study. Although absolute vitamin E serum levels were reduced by 23% in patients treated with evolocumab, vitamin E concentrations normalized for plasma lipid concentrations (LDL-C, ApoB, and non-HDL-C) did not decrease.60
Finally, in a 24-week, randomized, double-blind, placebo-controlled trial to evaluate the efficacy and safety of evolocumab in pediatric patients with HeFH (HAUSER-RCT), evolocumab reduced LDL-C levels by 44.5%. The incidence of adverse events that occurred during the treatment period was similar in the evolocumab group and the placebo group. Furthermore, levels of steroid hormones, fat-soluble vitamins (vitamins A, D, E, and K), glucose, and HbA1c were similar in the two groups at week 24.61
Thus, the above evidence indicates that therapeutic PCSK9 inhibition does not seem to cause any clinically meaningful adverse effects with respect to changes in levels of fat-soluble vitamins. In addition, treatment with PCSK9 inhibitors does not adversely affect normalized and tissue vitamin E levels, nor does it affect steroid hormone synthesis.
A summary of the trials pertaining to the safety and tolerability of PCSK9 inhibitors is shown in Table 1.
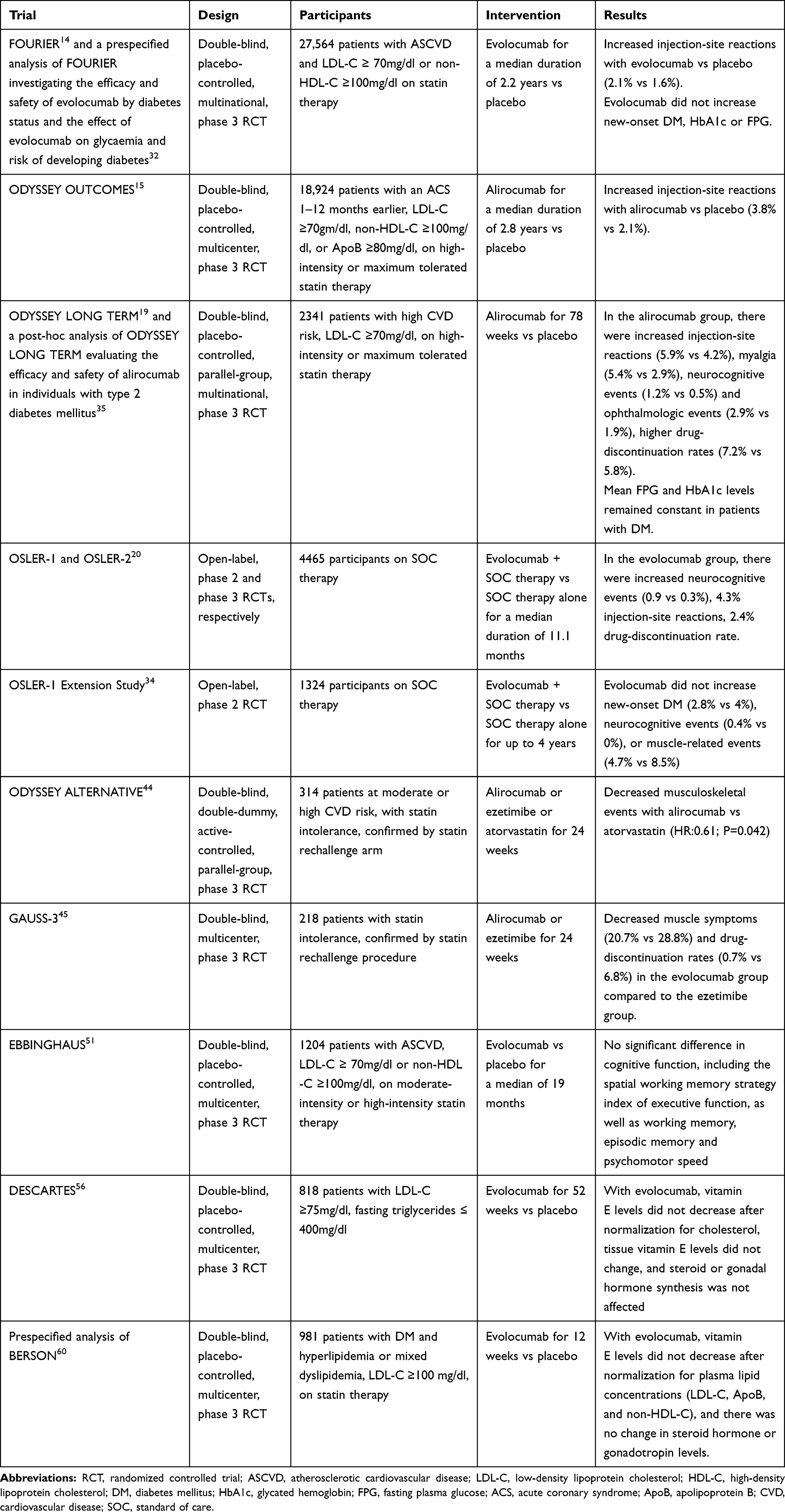 |
Table 1 Summary of Trials Pertaining to the Safety and Tolerability of PCSK9 Inhibitors |
Cost-Effectiveness of PCSK9 Inhibitor Therapy
PCSK9 inhibitors offer simple, attractive, and convenient dosing regimens, requiring only biweekly or monthly subcutaneous administration, thus leading to enhanced therapeutic compliance and adherence to therapy. On the contrary, the high economic burden that limited cost-effectiveness posed an obstacle limiting the access to PCSK9 inhibitors in clinical practice. The cost of PCSK9 inhibitors was $14,100 per annum in the US until October 2018, far exceeding the costs of other lipid-lowering interventions.62 At that price, use of PCSK9 inhibitors in patients with HeFH or ASCVD did not meet generally acceptable incremental cost-effectiveness thresholds and was estimated to increase US health care costs substantially.63 An analysis of the collected data from the OSLER and ODYSSEY LONG TERM clinical trials demonstrated the overwhelming financial implications of the administration of PCSK9 inhibitors for preventing either a major adverse CV event or a CV death.64 Another study showed that the precedent price point yielded an incremental cost of $348,807 per quality-adjusted life years (QALY), well beyond the highest acceptable willingness-to-pay threshold of $100,000 per QALY.65 The above findings emphasize the adverse cost-effectiveness of PCSK9 inhibitors, indicating that their use could not be affordable for either most health-care systems or private insurance payers.
Indeed, a study demonstrated that among 3472 patients requesting access to a PSCK9 inhibitor in 2016, only 36% of them were approved by payers. Notably, the incidence of acute CV events was higher in patients who were denied access, compared to the incidence in the overall relatively high risk patient population requesting PCSK9 inhibitors.66 Moreover, a retrospective cohort study, enrolling 13,151 patients, reported that a large proportion of patients discontinued PCSK9 inhibitor therapy at 30 and 90 days, which are the time frames for which many health plans require recertification to continue access to PCSK9 inhibitors. Overall, 42.6% of patients discontinued their therapies during the follow-up period of 6 months.67 Thus, it becomes evident that adherence to PCSK9 inhibitors is significantly lower in real-world settings than in clinical studies, in which the cost of therapy is not an impediment.
Ultimately, in October 2018 and February 2019, respectively, the main PCSK9 inhibitor manufacturing companies announced a 60% reduction in the cost of PCSK9 inhibitors, to $5850 per annum, making these agents much easier to prescribe nowadays.
Conclusions and Future Directions
The development of PCSK9 inhibitors, which are monoclonal antibodies directed against PCSK9, led to a significant enhancement of the lipid-lowering armamentarium, as PCSK9 inhibitors result in a consistent and robust reduction in LDL-C serum concentrations, substantially improving CV outcomes. The scientific and clinical experience with PCSK9 inhibitors suggests that they are a safe and well-tolerated therapeutic option with no evidence of severe medication-related adverse events. PCSK9 inhibitors have also proven to be safe and effective in patients with DM or statin intolerance.
However, there are still some aspects of the treatment with PCSK9 inhibitors that remain to be explored. The effects of PCSK9 inhibitors in patients with HIV, who are at increased risk for ASCVD and are prone to statin-related adverse events from drug-to-drug interactions with certain antiretroviral regimens, have not been clearly established. In the recent BEIJERINCK study, which sought to evaluate the efficacy and safety of evolocumab in dyslipidemic patients with HIV, evolocumab reduced LDL-C levels by 56.9% and also significantly decreased levels of non-HDL-C, ApoB, and lipoprotein(a) (all p < 0.0001). Evolocumab was well tolerated and the incidence of treatment-emergent adverse events was similar among evolocumab and placebo groups.68 However, the study had a short duration of 24 weeks and thus the effect of evolocumab on cardiovascular outcomes could not be assessed.
Furthermore, the safety of the use of PCSK9 inhibitors in pregnancy has not been established as yet. Thus, PCSK9 inhibitors are not currently approved during pregnancy. To that effect, a multinational observational study to evaluate the safety of evolocumab in pregnant women with FH is ongoing [ClinicalTrials.gov Identifier: NCT02906124].69 Given the fact that women with FH experience certain barriers to care, such as under-representation in research, under-appreciation of risk, and interrupted therapy during childbearing,70 the results of this study may help to close the gaps in care that women experience.
Notwithstanding, when all the above are considered, it becomes apparent that PCSK9 inhibitors are generally a safe, well-tolerated, and effective therapeutic strategy with an established role in the current therapeutic management of hyperlipidemia. As our experience with PCSK9 inhibitors is rapidly increasing, subsequent trials are expected to shed further light on their long-term safety and tolerability. On the other hand, other potential therapeutic strategies targeting PCSK9 are in development, including inclisiran (a small interfering RNA [siRNA] molecule), other small molecule inhibitors that disrupt the processing of PCSK9, as well as adnectins, which block the binding of PCSK9 to the LDLR.71–73
Disclosure
Dr. Kosmas and Dr. Guzman have served on the Dyslipidemia Speaker Bureau of Amgen, Inc. The authors report no other conflicts of interest in this work.
References
1. GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–1788.
2. Afonso MS, Machado RM, Lavrador MS, Quintao ECR, Moore KJ, Lottenberg AM. Molecular pathways underlying cholesterol homeostasis. Nutrients. 2018;10(6):760. doi:10.3390/nu10060760
3. Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38(32):2459–2472. doi:10.1093/eurheartj/ehx144
4. Jain S, Vaishnavi V, Chakraborty BS. The effect of dyslipidemic drugs on mortality: a meta-analysis. Indian J Pharmacol. 2009;41(1):4–8. doi:10.4103/0253-7613.48878
5. Macchi C, Banach M, Corsini A, Sirtori CR, Ferri N, Ruscica M. Changes in circulating pro-protein convertase subtilisin/kexin type 9 levels - experimental and clinical approaches with lipid-lowering agents. Eur J Prev Cardiol. 2019;26(9):930–949. doi:10.1177/2047487319831500
6. Urban D, Pöss J, Böhm M, Laufs U. Targeting the proprotein convertase subtilisin/kexin type 9 for the treatment of dyslipidemia and atherosclerosis. J Am Coll Cardiol. 2013;62(16):1401–1408. doi:10.1016/j.jacc.2013.07.056
7. Zhao Z, Du S, Shen S, et al. Comparative efficacy and safety of lipid-lowering agents in patients with hypercholesterolemia: a frequentist network meta-analysis. Medicine (Baltimore). 2019;98(6):e14400. doi:10.1097/MD.0000000000014400
8. Koskinas KC, Gencer B, Nanchen D, et al. Eligibility for PCSK9 inhibitors based on the 2019 ESC/EAS and 2018 ACC/AHA guidelines. Eur J Prev Cardiol. 2020:2047487320940102.
9. Kosmas CE, Sourlas A, Mallarkey G, et al. Therapeutic management of hyperlipoproteinemia (a). Drugs Context. 2019;8:212609. doi:10.7573/dic.212609
10. Walley KR, Thain KR, Russell JA, et al. PCSK9 is a critical regulator of the innate immune response and septic shock outcome. Sci Transl Med. 2014;6(258):258ra143. doi:10.1126/scitranslmed.3008782
11. Kosmas CE, DeJesus E, Morcelo R, Garcia F, Montan PD, Guzman E. Lipid-lowering interventions targeting proprotein convertase subtilisin/kexin type 9 (PCSK9): an emerging chapter in lipid-lowering therapy. Drugs Context. 2017;6:212511. doi:10.7573/dic.212511
12. Ruscica M, Tokgözoğlu L, Corsini A, Sirtori CR. PCSK9 inhibition and inflammation: a narrative review. Atherosclerosis. 2019;288:146–155. doi:10.1016/j.atherosclerosis.2019.07.015
13. Ruscica M, Corsini A, Ferri N, Banach M, Sirtori CR. Clinical approach to the inflammatory etiology of cardiovascular diseases. Pharmacol Res. 2020;159:104916. doi:10.1016/j.phrs.2020.104916
14. Sabatine MS, Giugliano RP, Keech AC, et al.; FOURIER Steering Committee and Investigators. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376(18):1713–1722. doi:10.1056/NEJMoa1615664.
15. Schwartz GG, Steg PG, Szarek M, et al.; ODYSSEY OUTCOMES Committees and Investigators. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med. 2018;379(22):2097–2107. doi:10.1056/NEJMoa1801174.
16. Wong ND, Shapiro MD. Interpreting the findings from the recent PCSK9 monoclonal antibody cardiovascular outcomes trials. Front Cardiovasc Med. 2019;6:14. doi:10.3389/fcvm.2019.00014
17. Chaudhary R, Garg J, Shah N, Sumner A. PCSK9 inhibitors: a new era of lipid lowering therapy. World J Cardiol. 2017;9(2):76–91. doi:10.4330/wjc.v9.i2.76
18. Bulbulia R, Armitage J. Does the benefit from statin therapy extend beyond 5 years? Curr Atheroscler Rep. 2013;15(2):297. doi:10.1007/s11883-012-0297-1
19. Robinson JG, Farnier M, Krempf M, et al. ODYSSEY LONG TERM Investigators. Efficacy and safety of alirocumab in reducing lipids and cardiovascular events. N Engl J Med. 2015;372(16):1489–1499. doi:10.1056/NEJMoa1501031
20. Sabatine MS, Giugliano RP, Wiviott SD, et al.; Open-Label Study of Long-Term Evaluation against LDL Cholesterol (OSLER) Investigators. Efficacy and safety of evolocumab in reducing lipids and cardiovascular events. N Engl J Med. 2015;372(16):1500–1509. doi:10.1056/NEJMoa1500858.
21. Giugliano RP, Pedersen TR, Park JG, et al.; FOURIER Investigators. Clinical efficacy and safety of achieving very low LDL-cholesterol concentrations with the PCSK9 inhibitor evolocumab: a prespecified secondary analysis of the FOURIER trial. Lancet. 2017;390(10106):1962–1971. doi:10.1016/S0140-6736(17)32290-0.
22. Mu G, Xiang Q, Zhou S, et al. Efficacy and safety of PCSK9 monoclonal antibodies in patients at high cardiovascular risk: an updated systematic review and meta-analysis of 32 randomized controlled trials. Adv Ther. 2020;37(4):1496–1521. doi:10.1007/s12325-020-01259-4
23. Koren MJ, Sabatine MS, Giugliano RP, et al. Long-term efficacy and safety of evolocumab in patients with hypercholesterolemia. J Am Coll Cardiol. 2019;74(17):2132–2146. doi:10.1016/j.jacc.2019.08.1024
24. Pasta A, Cremonini AL, Pisciotta L, et al. PCSK9 inhibitors for treating hypercholesterolemia. Expert Opin Pharmacother. 2020;21(3):353–363. doi:10.1080/14656566.2019.1702970
25. Roth EM, Goldberg AC, Catapano AL, et al. Antidrug antibodies in patients treated with alirocumab. N Engl J Med. 2017;376(16):1589–1590. doi:10.1056/NEJMc1616623
26. Vergès B. Pathophysiology of diabetic dyslipidaemia: where are we? Diabetologia. 2015;58(5):886–899. doi:10.1007/s00125-015-3525-8
27. Kosmas CE, Silverio D, Sourlas A, Garcia F, Montan PD, Guzman E. Impact of lipid-lowering therapy on glycemic control and the risk for new-onset diabetes mellitus. Drugs Context. 2018;7:212562. doi:10.7573/dic.212562
28. Lotta LA, Sharp SJ, Burgess S, et al. Association between low-density lipoprotein cholesterol-lowering genetic variants and risk of type 2 diabetes: a meta-analysis. JAMA. 2016;316(13):1383–1391. doi:10.1001/jama.2016.14568
29. Ference BA, Robinson JG, Brook RD, et al. Variation in PCSK9 and HMGCR and risk of cardiovascular disease and diabetes. N Engl J Med. 2016;375(22):2144–2153. doi:10.1056/NEJMoa1604304
30. Schmidt AF, Swerdlow DI, Holmes MV, et al. PCSK9 genetic variants and risk of type 2 diabetes: a mendelian randomisation study. Lancet Diabetes Endocrinol. 2017;5(2):97–105. doi:10.1016/S2213-8587(16)30396-5
31. Macchi C, Favero C, Ceresa A, et al. Depression and cardiovascular risk-association among Beck Depression Inventory, PCSK9 levels and insulin resistance. Cardiovasc Diabetol. 2020;19(1):187. doi:10.1186/s12933-020-01158-6
32. Sabatine MS, Leiter LA, Wiviott SD, et al. Cardiovascular safety and efficacy of the PCSK9 inhibitor evolocumab in patients with and without diabetes and the effect of evolocumab on glycaemia and risk of new-onset diabetes: a prespecified analysis of the FOURIER randomised controlled trial. Lancet Diabetes Endocrinol. 2017;5(12):941–950. doi:10.1016/S2213-8587(17)30313-3
33. Kosmas CE, Sourlas A, Bouza KV, et al. Proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibition with evolocumab: powerful low-density lipoprotein cholesterol (LDL-C) lowering and improved cardiovascular outcomes without an increase in the risk of diabetes mellitus. Ann Transl Med. 2018;6(7):130. doi:10.21037/atm.2018.02.20
34. Koren MJ, Sabatine MS, Giugliano RP, et al. Long-term low-density lipoprotein cholesterol-lowering efficacy, persistence, and safety of evolocumab in treatment of hypercholesterolemia: results up to 4 years from the open-label OSLER-1 extension study. JAMA Cardiol. 2017;2(6):598–607. doi:10.1001/jamacardio.2017.0747
35. Taskinen MR, Del Prato S, Bujas-Bobanovic M, et al. Efficacy and safety of alirocumab in individuals with type 2 diabetes mellitus with or without mixed dyslipidaemia: analysis of the ODYSSEY LONG TERM trial. Atherosclerosis. 2018;276:124–130. doi:10.1016/j.atherosclerosis.2018.07.017
36. Monami M, Sesti G, Mannucci E. PCSK9 inhibitor therapy: a systematic review and meta-analysis of metabolic and cardiovascular outcomes in patients with diabetes. Diabetes Obes Metab. 2019;21(4):903–908. doi:10.1111/dom.13599
37. Lardizabal JA, Deedwania PC. Benefits of statin therapy and compliance in high risk cardiovascular patients. Vasc Health Risk Manag. 2010;6:843–853.
38. Ho PM, Magid DJ, Shetterly SM, et al. Medication nonadherence is associated with a broad range of adverse outcomes in patients with coronary artery disease. Am Heart J. 2008;155(4):772–779. doi:10.1016/j.ahj.2007.12.011
39. Rodriguez F, Maron DJ, Knowles JW, Virani SS, Lin S, Heidenreich PA. Association of statin adherence with mortality in patients with atherosclerotic cardiovascular disease. JAMA Cardiol. 2019;4(3):206–213. doi:10.1001/jamacardio.2018.4936
40. Zhang H, Plutzky J, Skentzos S, et al. Discontinuation of statins in routine care settings: a cohort study. Ann Intern Med. 2013;158(7):526–534. doi:10.7326/0003-4819-158-7-201304020-00004
41. Lin I, Sung J, Sanchez RJ, et al. Patterns of statin use in a real-world population of patients at high cardiovascular risk. J Manag Care Spec Pharm. 2016;22(6):685–698.
42. Blom DJ, Hala T, Bolognese M, et al; DESCARTES Investigators. A 52-week placebo-controlled trial of evolocumab in hyperlipidemia. N Engl J Med. 2014;370(19):1809–1819. doi:10.1056/NEJMoa1316222
43. Karatasakis A, Danek BA, Karacsonyi J, et al. Effect of PCSK9 inhibitors on clinical outcomes in patients with hypercholesterolemia: a meta-analysis of 35 randomized controlled trials. J Am Heart Assoc. 2017;6(12):e006910. doi:10.1161/JAHA.117.006910
44. Moriarty PM, Thompson PD, Cannon CP, et al.; ODYSSEY ALTERNATIVE Investigators. Efficacy and safety of alirocumab vs ezetimibe in statin-intolerant patients, with a statin rechallenge arm: the ODYSSEY ALTERNATIVE randomized trial. J Clin Lipidol. 2015;9(6):758–769. doi:10.1016/j.jacl.2015.08.006.
45. Nissen SE, Stroes E, Dent-Acosta RE, et al.; GAUSS-3 Investigators. Efficacy and tolerability of evolocumab vs ezetimibe in patients with muscle-related statin intolerance: the GAUSS-3 randomized clinical trial. JAMA. 2016;315(15):1580–1590. doi:10.1001/jama.2016.3608.
46. Cho L, Dent R, Stroes ESG, et al. Persistent safety and efficacy of evolocumab in patients with statin intolerance: a subset analysis of the OSLER open-label extension studies. Cardiovasc Drugs Ther. 2018;32(4):365–372. doi:10.1007/s10557-018-6817-7
47. Rane PB, Patel J, Harrison DJ, et al. Patient characteristics and real-world treatment patterns among early users of PCSK9 inhibitors. Am J Cardiovasc Drugs. 2018;18(2):103–108. doi:10.1007/s40256-017-0246-z
48. O’Connell EM, Lohoff FW. Proprotein convertase subtilisin/kexin type 9 (PCSK9) in the brain and relevance for neuropsychiatric disorders. Front Neurosci. 2020;14:609. doi:10.3389/fnins.2020.00609
49. Bandyopadhyay D, Ashish K, Hajra A, Qureshi A, Ghosh RK. Cardiovascular outcomes of PCSK9 inhibitors: with special emphasis on its effect beyond LDL-cholesterol lowering. J Lipids. 2018;2018:3179201. doi:10.1155/2018/3179201
50. Bajaj NS, Patel N, Kalra R, et al. Neurological effects of proprotein convertase subtilisin/kexin type 9 inhibitors: direct comparisons. Eur Heart J Qual Care Clin Outcomes. 2018;4(2):132–141. doi:10.1093/ehjqcco/qcx037
51. Giugliano RP, Mach F, Zavitz K, et al.; EBBINGHAUS Investigators. Cognitive function in a randomized trial of evolocumab. N Engl J Med. 2017;377(7):633–643. doi:10.1056/NEJMoa1701131.
52. Harvey PD, Sabbagh MN, Harrison JE, et al. No evidence of neurocognitive adverse events associated with alirocumab treatment in 3340 patients from 14 randomized Phase 2 and 3 controlled trials: a meta-analysis of individual patient data. Eur Heart J. 2018;39(5):374–381. doi:10.1093/eurheartj/ehx661
53. Gencer B, Mach F, Guo J, et al.; FOURIER Investigators. Cognition after lowering LDL-cholesterol with evolocumab. J Am Coll Cardiol. 2020;75(18):2283–2293. doi:10.1016/j.jacc.2020.03.039.
54. Robinson JG. Low LDL-C levels: likely no short-term cognitive harm. J Am Coll Cardiol. 2020;75(18):2294–2296. doi:10.1016/j.jacc.2020.03.040
55. Rizvi S, Raza ST, Ahmed F, Ahmad A, Abbas S, Mahdi F. The role of vitamin e in human health and some diseases. Sultan Qaboos Univ Med J. 2014;14(2):e157–e165.
56. Blom DJ, Djedjos CS, Monsalvo ML, et al. Effects of evolocumab on vitamin E and steroid hormone levels: results from the 52-week, phase 3, double-blind, randomized, placebo-controlled DESCARTES study. Circ Res. 2015;117(8):731–741. doi:10.1161/CIRCRESAHA.115.307071
57. Welty FK. Hypobetalipoproteinemia and abetalipoproteinemia. Curr Opin Lipidol. 2014;25(3):161–168. doi:10.1097/MOL.0000000000000072
58. Qamar A, Bhatt DL. Effect of low cholesterol on steroid hormones and vitamin E levels: just a theory or real concern? Circ Res. 2015;117(8):662–664. doi:10.1161/CIRCRESAHA.115.307345
59. Kawashiri MA, Nohara A, Higashikata T, et al. Impact of evolocumab treatment on low-density lipoprotein cholesterol levels in heterozygous familial hypercholesterolemic patients withdrawing from regular apheresis. Atherosclerosis. 2017;265:225–230. doi:10.1016/j.atherosclerosis.2017.09.011
60. Blom DJ, Chen J, Yuan Z, et al. Effects of evolocumab therapy and low LDL-C levels on vitamin E and steroid hormones in Chinese and global patients with type 2 diabetes. Endocrinol Diabetes Metab. 2020;3(2):e00123. doi:10.1002/edm2.123
61. Santos RD, Ruzza A, Hovingh GK, et al.; HAUSER-RCT Investigators. Evolocumab in pediatric heterozygous familial hypercholesterolemia. N Engl J Med. 2020;383(14):1317–1327. doi:10.1056/NEJMoa2019910.
62. Kosmas CE, Silverio D, Ovalle J, Montan PD, Guzman E. Patient adherence, compliance, and perspectives on evolocumab for the management of resistant hypercholesterolemia. Patient Prefer Adherence. 2018;12:2263–2266. doi:10.2147/PPA.S149423
63. Kazi DS, Moran AE, Coxson PG, et al. Cost-effectiveness of PCSK9 inhibitor therapy in patients with heterozygous familial hypercholesterolemia or atherosclerotic cardiovascular disease. JAMA. 2016;316(7):743–753. doi:10.1001/jama.2016.11004
64. Arbel R, Hammerman A, Triki N, Greenberg D. PCSK9 inhibitors may improve cardiovascular outcomes-Can we afford them? Int J Cardiol. 2016;220:242–245. doi:10.1016/j.ijcard.2016.06.126
65. Arrieta A, Page TF, Veledar E, Nasir K. Economic evaluation of PCSK9 inhibitors in reducing cardiovascular risk from health system and private payer perspectives. PLoS One. 2017;12(1):e0169761. doi:10.1371/journal.pone.0169761
66. Baum SJ, Chen CC, Rane P, et al. Cardiovascular risk in patients denied access to PCSK9i therapy. J Am Coll Cardiol. 2018;71(11 Supplement):A1760. doi:10.1016/S0735-1097(18)32301-5
67. Hines DM, Rane P, Patel J, Harrison DJ, Wade RL. Treatment patterns and patient characteristics among early initiators of PCSK9 inhibitors. Vasc Health Risk Manag. 2018;14:409–418. doi:10.2147/VHRM.S180496
68. Boccara F, Kumar PN, Caramelli B, et al.; BEIJERINCK Investigators. Evolocumab in HIV-infected patients with dyslipidemia: primary results of the randomized, double-blind BEIJERINCK study. J Am Coll Cardiol. 2020;75(20):2570–2584. doi:10.1016/j.jacc.2020.03.025.
69. Study to Evaluate the Safety of Repatha® in Pregnancy. ClinicalTrials.gov Identifier: NCT02906124. Available from: http://clinicaltrials.gov/ct2/show/NCT02906124.
70. Balla S, Ekpo EP, Wilemon KA, Knowles JW, Rodriguez F. Women living with familial hypercholesterolemia: challenges and considerations surrounding their care. Curr Atheroscler Rep. 2020;22(10):60. doi:10.1007/s11883-020-00881-5
71. Giugliano RP, Sabatine MS. Are PCSK9 inhibitors the next breakthrough in the cardiovascular field? J Am Coll Cardiol. 2015;65(24):2638–2651. doi:10.1016/j.jacc.2015.05.001
72. Xu S, Luo S, Zhu Z, Xu J. Small molecules as inhibitors of PCSK9: current status and future challenges. Eur J Med Chem. 2019;162:212–233. doi:10.1016/j.ejmech.2018.11.011
73. Kosmas CE, Muñoz Estrella A, Skavdis A, Peña Genao E, Martinez I, Guzman E. Inclisiran for the treatment of cardiovascular disease: a short review on the emerging data and therapeutic potential. Ther Clin Risk Manag. 2020;16:1031–1037. doi:10.2147/TCRM.S230592
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.