Back to Journals » Therapeutics and Clinical Risk Management » Volume 16
Role of Arthrodiastasis Using Hinged Monolateral External Fixator Without Soft Tissue Release in Advanced Stage of Legg–Calve–Perthes Disease
Authors Samarah OQ ![]() , Nimer A
, Nimer A ![]() , Al Karmi F, Mustafa O, Naser S, Al Omari L, Hammad Y
, Al Karmi F, Mustafa O, Naser S, Al Omari L, Hammad Y ![]() , Ermeley Z
, Ermeley Z
Received 16 September 2020
Accepted for publication 25 October 2020
Published 16 November 2020 Volume 2020:16 Pages 1117—1124
DOI https://doi.org/10.2147/TCRM.S282404
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Omar Q Samarah,1 Abdullah Nimer,2 Fahed Al Karmi,2 Osama Mustafa,2 Suzan Naser,2 Lujain Al Omari,2 Yazan Hammad,1 Ziad Ermeley3
1Department of Special Surgery, School of Medicine, University of Jordan, Amman, Jordan; 2School of Medicine, University of Jordan, Amman, Jordan; 3Department of Health and Recreation, School of Physical Studies, University of Jordan, Amman, Jordan
Correspondence: Omar Q Samarah
School of Medicine, University of Jordan, Amman 11942, Jordan
Tel +962 6 5353 444/2451
Fax +962 6 5353 338
Email [email protected]
Purpose: Presentation with the advanced stage of Legg–Calve–Perthes disease (LCPD) carries a poor prognosis, regardless of the treatment that the patient receives. The aims of this study are to assess the clinical and radiological outcomes of arthrodiastasis in advanced cases of LCPD using a hinged monolateral external fixator without soft tissue release and to raise safety issues regarding its low rate of complications.
Patients and Methods: Six patients with LCPD who were classified as lateral pillar types B and C and were operated on in our department were included in this retrospective study. Data collected from medical files and X-ray measurements were retrospectively reviewed.
Results: A total of six male patients were included in this analysis. The mean age at onset of symptoms was 8.5 years (range 7– 10 years). The mean follow-up period was 46 months (range 40– 50 months). Five cases were Herring C and one case was Herring B at presentation. The average distraction time was 8 days (range 7– 9) and the average duration of external fixator application was 3.1 months (range 2.5– 3.5 months). The range of motion of the hip in flexion, abduction and internal rotation were improved postoperatively. Pain score and limping were also improved. At the final follow-up, the mean sphericity deviation score was 10.6. The mean epiphyseal index was improved from 19.3% to 23.8%. In addition, the mean cervical index improved from 99.7% to 89.7% at the last follow-up. Femoral fractures, pin loosening, mechanical failure of the fixator, chondrodiastasis, and hip subluxation were not seen in this group of patients.
Conclusion: Arthrodiastasis with a hinged monolateral external fixator without soft tissue release improved both the clinical and radiological outcomes in this group of patients.
Keywords: Perthes disease, hip arthrodiastasis, external fixator, distraction, safety
Introduction
Legg–Calve–Perthes disease (LCPD) is one of the most controversial conditions in pediatric orthopedics in terms of treatment-related decisions.1 Despite the wide knowledge and research about the disease, there is still a group of patients with a poor prognosis, regardless of whatever treatment they receive. These patients are those in whom the disease presents at an advanced stage (mainly Herring’s lateral pillar type C) after the age of 8 years.2
Late-presenting cases form around 20% of all cases of LCPD.3 Generally, they have poor outcomes. Several factors have been postulated to play a role in this result. These include short time remaining for growth and remodeling and advanced stage of head involvement upon presentation with rapid passage of earlier stages (such as the necrosis stage), in addition to the decreased elasticity of the acetabulum.4–7
Herring et al8 classified LCPD into three groups based on the height of the lateral pillar which is the lateral 15–30% of the femoral head width, in the fragmentation stage of the disease as seen on an anteroposterior radiographic view (Table 1). In this classification Several publications have demonstrated better clinical outcomes with surgical intervention for groups B and B/C after the age of 8 years.9,10 Several surgical procedures have addressed patients with the advanced stage of the disease; these include femoral and pelvic osteotomies.11 Both procedures change the anatomy of the hip joint, which may hinder future joint arthroplasty. The challenge of treating LCPD is to prevent degenerative arthritis by preserving the spherical shape of the femoral head.12
 |
Table 1 Herring’s Lateral Pillar Classification System |
The initial goals of treatment of LCPD are containment of the femoral head within the acetabulum, pain relief, improvement in the range of motion of the hip joint and arrest of femoral head collapse.3,13 Arthrodiastasis was introduced several years ago as an alternative procedure for severe forms of LCPD, as it provides mechanical protection and biological value to the femoral head.14,15 Different types of external fixators have been used in arthrodiastasis.15–17 Permission of the joint motion through using an articulating device during arthrodiastasis allows synovial circulation and cartilage nourishment to occur, which further promotes healing of the necrotic head.18 A paucity of data is available in literature that encourages the use of arthrodiastasis in the treatment of LCPD.19
Soft tissue release has been performed in multiple arthrodiastasis procedures.3,7,13,14 In this study, we aim to present our initial clinical and radiological results of radiological results of arthrodiastasis in LCPD presenting at an advanced stage by using a hinged monolateral external fixator without soft tissue release.
Patients and Methods
Patient Selection
We conducted a retrospective review of the medical charts of patients with LCPD who were treated in our hospital by articulated arthrodiastasis of the hip joint between 2013 and 2017. This review identified six patients who fulfilled the following inclusion criteria and were enrolled in our study.
- Patients with LCPD who had Herring lateral pillar classification types B or C
- Age 7 years or older at presentation
- Variable degrees of limitation of hip joint range of motion and pain
- Did not received any previous treatment for their condition
- Follow-up of at least 3 years
Patients who were younger than 7 years at presentation regardless of their lateral pillar classification type, patients with lateral pillar type A, and patients with femoral head necrosis from other well-known causes were excluded from this review.
The study protocol was approved by the Institutional Review Board (IRB) of Jordan University hospital (JUH) with approval reference number 67/2020/266. The study was performed in accordance with the principles of the Declaration of Helsinki. Informed consent was signed by all parents of the participating children before the start of the study. The parents were debriefed about the purpose of the study. They were informed that the participation was voluntary, and they may withdraw at any time. None of them received anything in return for their participation.
Outcome Measures
The index procedure included application of a monolateral external fixator without soft tissue release to all patients who fulfilled the abovementioned criteria. Age of the patient at presentation, gender, radiological stage of the disease based on the Herring classification, staging according to the Waldenström classification, and duration of external fixator application were collected and analyzed.
Clinically, the numeric rating scale has been used to assess pain severity (NRS);20 range of motion of the involved hip in flexion, abduction and internal rotation; and any complication, including development of ipsilateral knee stiffness, infection and mechanical failure of the device whether it happened intraoperatively, postoperatively or during the follow-up period were carried out and analyzed.
Radiologically, two anteroposterior (AP) and axial hip X-ray views were taken preoperatively. Then, AP X-ray views in the immediate postoperative period and weekly during the distraction period were performed. At the last follow-up, two views of the hip were taken that were similar to the preoperative radiographs. Improvement was assessed by evaluating sphericity deviation score,21 epiphyseal index, which is defined by the height of the epiphysis from the physis to the highest point of the epiphyseal surface contour divided by the width of the epiphysis,22 and cervical index that is defined by diameter of the neck divided by it is length. Higher ratios indicate progressive shortening of the neck. Stulberg grading was not applicable due to the skeletal immaturity of the patients.5
Operative Procedure
All children were operated on in a supine position under general anesthesia. A k-wire was used to identify axis of rotation of the hip joint under image intensifier. The k wire was inserted through a hole in the hinge of the external fixator toward the predetermined axis of rotation. Three schanz screws (5mm) were inserted in the supra-acetabular area. Another 3 schanz screws of the same size were inserted distally in the femur shaft. After completion of the device application, the range of motion of the hip joint was examined to ensure that no impairment of the hip’s motion due to the device position.
Postoperative Protocol
All patients started physiotherapy programs on postoperative day 1. With the hinged device, hip joint’s range of motion exercises in flexion-extension were performed gradually. At the same time, preservation of the ipsilateral knee range of motion was monitored carefully. Patients were starting partial weight bearing exercises same first day postoperative using crutches. Distraction started also on postoperative day 1 at a range of 0.5 mm 4 times per day. They were discharged postoperative day 2 after their pain has decreased and their parents were well educated about home exercises and pin tract care. Patients were re-evaluated one week later in outpatient clinic. During home stay, distraction was continued until the next clinic visit or stopped when the patient experienced pain that could not be resolved by analgesia. Once the aim of distraction has been achieved, no further distraction was done, and the device was held in position for an average of 3.1 months until reossification of the lateral pillar reappeared and then removed. Patients were followed biweekly in the clinic after stopping the distraction for the first month, then monthly until the device was removed. All devices were removed in the day care unit under general anaesthesia and manipulation for the hips were done after device removal. Patients were trained to increase weight bearing after device removal to achieve full weight bearing in 4–6 weeks after removal.
Results
A total of six male patients were included in this study, with a mean age of onset of symptoms of 8.5 years (range 7–10 years). The mean follow-up period was 46 months (range 40–50 months). In all, five cases were Herring C and one case was Herring B at presentation. Distraction was started on the first postoperative day at a rate of 2 mm/day, aiming for overcorrection of the Shenton line by around 5 mm or when pain prevents further distraction. The average duration of distraction was 8 days (range 7–9 days). The average duration of external fixator application was 3.1 months (range 2.5–3.5 months) (Table 2).
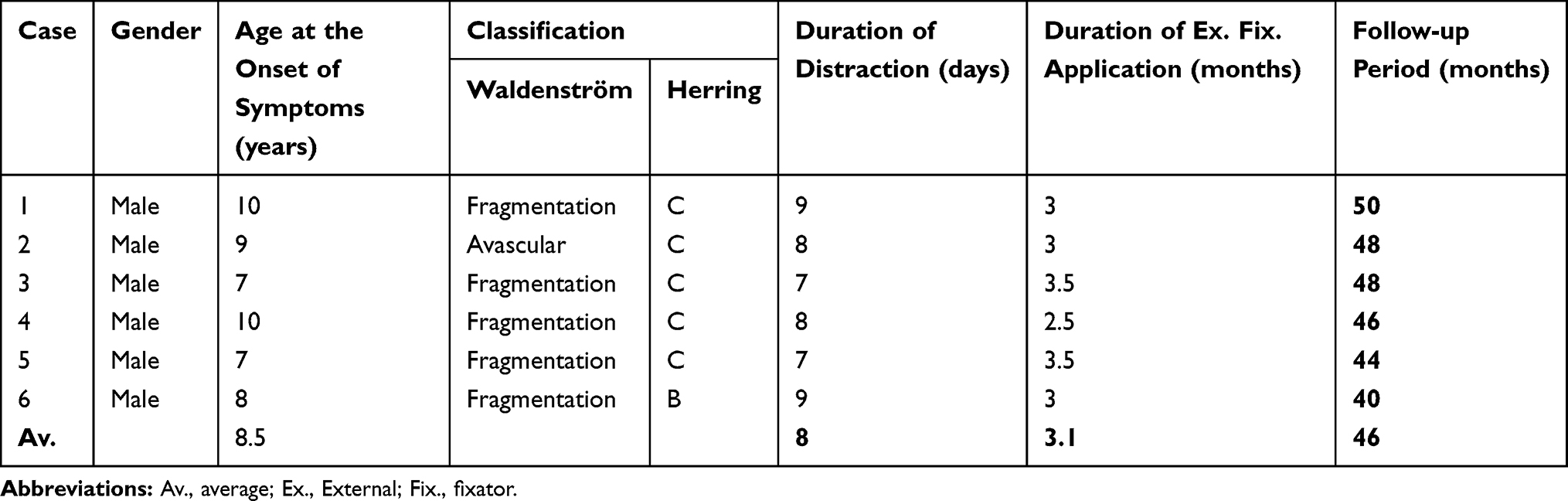 |
Table 2 Details of the Patients |
Postoperatively, all patients (100%) had significant improvement in the range of motion of the hip joint in flexion, abduction and internal rotation compared to preoperatively. Preoperatively, all patients complained of constant pain, necessitating regular use of analgesics, and had clinically evident limping. At last follow-up, all of them reported improvement in their pain score and five of six patients (83.3%) had an improvement in limping (Table 3).
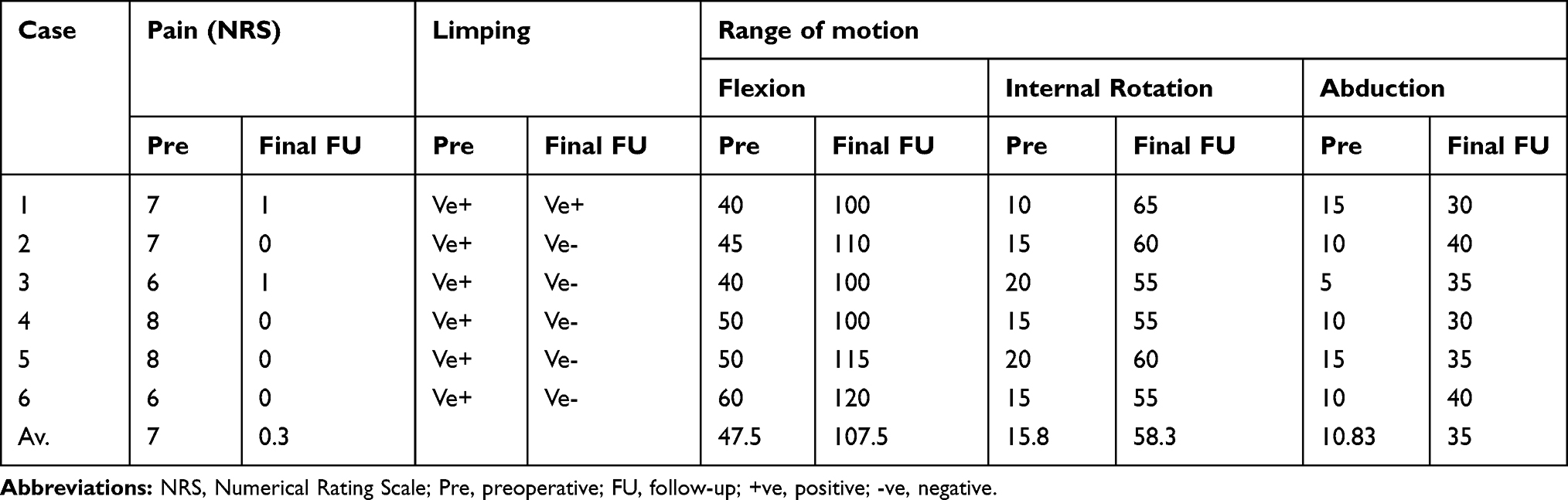 |
Table 3 Clinical Data and Outcomes of the Patients |
The average sphericity deviation score at the final follow up was 10.6. The mean epiphyseal index was improved from 19.3% preoperatively to 23.8% postoperatively at the final follow-up. In addition to that, the mean cervical index was also improved from 99.7% preoperatively to 89.7% postoperatively (Table 4).
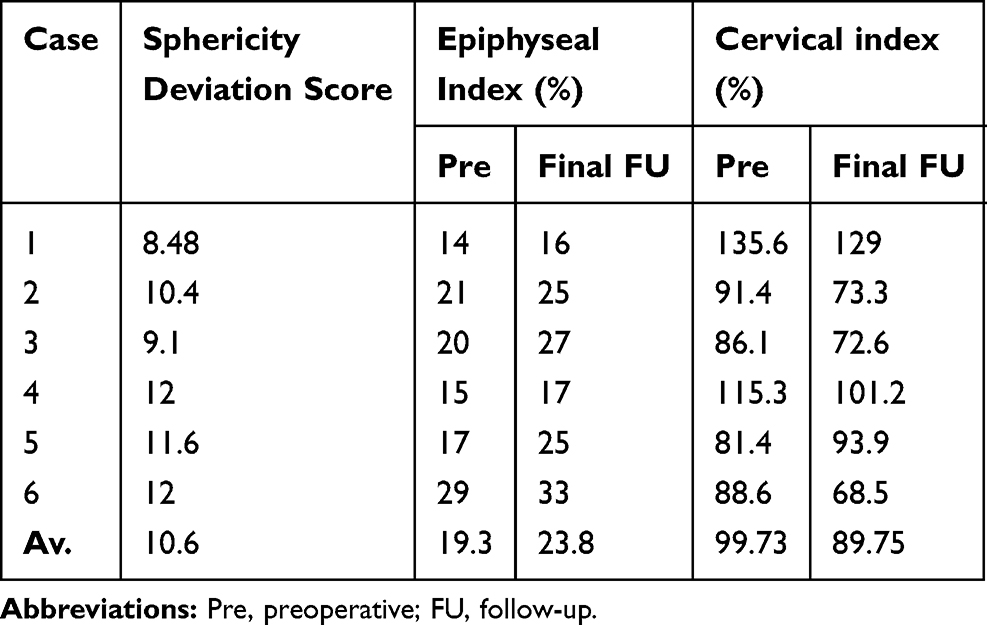 |
Table 4 Radiological Outcomes |
Pin tract infection occurred in two cases. One case improved with oral antibiotics and dressing. The second case received intravenous antibiotic with removal of the external fixator 2 weeks earlier than the other. No postoperative femoral fractures, pin loosening, mechanical failure of fixator, chondrodiastasis, or hip subluxation was seen in this group of patients.
Case Histories
Case 1
A 10-year-old male patient with Legg–Calve–Perthes disease of the left hip presented with progressive pain in the left hip of 6 months duration. The pain was exacerbated by daily life activity. Physical examination showed positive antalgic gait. Range of motion of the hip joint was limited, particularly flexion, abduction, and internal rotation. Plain radiographs showed lateral pillar type C.
He had an external fixator for 3 months. His Hip pain was improved from 7 to 1 point on the NRS at the final follow up. Moreover, the involved hip joint’s range of motion in flexion, internal rotation, and abduction was also improved compared with the preoperative values. On the radiological evaluation, the sphericity deviation score, epiphyseal index, and the cervical index were all improved at the final follow up (Tables 2-4).
Case 2
A 9-year-old-male child with Legg–Calve–Perthes disease of the right hip presented with right sided hip pain and antalgic gait of 4 months duration. The pain led restriction of daily life activities. There were no associated constitutional symptoms. He had a painful limited range of motion of his hip on physical examination. Plain radiographs showed lateral pillar type C. The patient underwent same index procedure. The external fixation device was maintained for 3 months. No intraoperative complications were encountered. Postoperative protocol was followed smoothly. The postoperative course was uneventful. After removal of the external fixator, the patient showed improvement in the pain score and had a mild Trendelenburg gait. He had also improved range of motion of the involved hip joint. Radiologically, all scores that were tested, were improved at the final follow up. (Tables 2-4) Figures 1 and 2.
 |
Figure 1 (A) Preoperative X-ray of patient No. 2 (right hip herring’s type C), (B) 2 weeks after distraction with correction of the shenton line. |
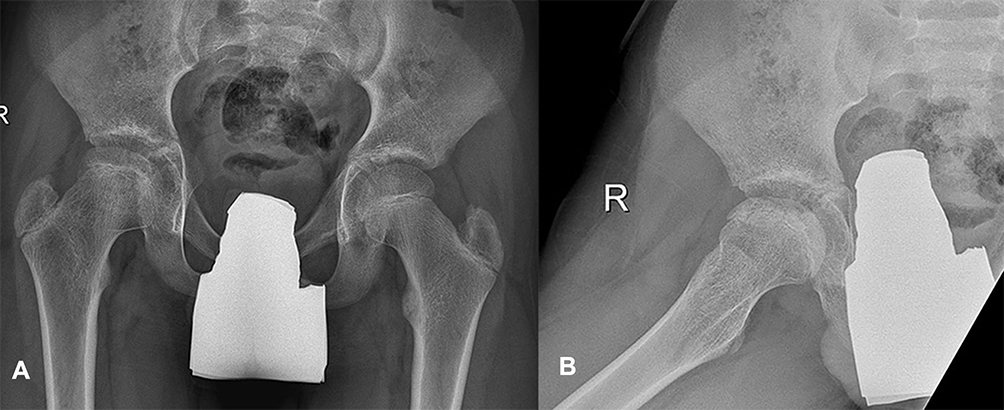 |
Figure 2 (A) Anteroposterior and (B) Lateral views of patient No. 2, 48 months postoperative showing remodeling of the femoral head. |
Case 3
A 7- year-old-male child with Legg–Calve–Perthes disease of the right hip. He presented with moderate right-sided hip pain and antalgic gait of 3 months duration. The pain led to restriction of daily life activities. There were no associated constitutional symptoms. A painful limited range of motion of his hip was clear on examination. The knee exam was normal. Plain radiographs showed lateral pillar type C. The patient underwent same index procedure, where the external fixator kept for 3.5 months. No intraoperative complications were observed. Postoperative protocol was followed smoothly. At the final follow up, he showed improvement in all physical and radiological parameters. (Tables 2-4)
Case 4
A 10-year-old- child with left hip Legg–Calve–Perthes disease. He presented with pain in the left hip of 2 months duration. It was increasing progressively that badly affected his daily life activities. Oral analgesics improved the pain temporarily. He showed antalgic gait on physical examination. In addition to that, limited hip motion, particularly flexion, abduction, and internal rotation. Pelvis X-ray showed lateral pillar type C. The patient underwent same index procedure. His external device was removed after 2.5 months of application. He followed the same postoperative protocol. Two months postoperatively, the patient developed pin tract infection involving mainly the supraacetabular screw group. He was managed with empirical oral antibiotics but did not respond well. A decision was made to remove the fixator and to debride the wound tracts and to keep him on intravenous antibiotics. Five days after fixator removal, he showed clinical improvement and discharged. Postoperative protocol was followed then smoothly. All physical and radiological parameters had been improved at the final follow up. (Tables 2-4)
Case 5
A 7-year-old-male child with Legg–Calve–Perthes disease of the left hip. He presented with complaint of pain in the left hip of 1-month duration. The pain was severe that restricted the child activity. It was associated with limping that forced him to use crutches. The patient received oral analgesics to relieve the pain with partial response. No fever or constitutional symptoms were observed.
On physical examination, flexion, abduction, and internal rotation of the hip joint were limited. Pelvis radiographs showed lateral pillar type C. The patient underwent same index procedure, where the external fixator was applied for 3.5 months. Postoperative protocol was followed smoothly. At the final follow up, he showed improvement in all physical and radiological parameters. (Tables 2-4)
Case 6
An 8-year-old-male child with Legg–Calve–Perthes disease of the left hip. He had a history of left sided hip pain of moderate severity and antalgic gait of 2 months duration. The pain restricted his sport-related activity. There were no associated constitutional symptoms. He had a painful limited range of motion of his hip on physical examination. Plain radiographs showed lateral pillar type B. The patient underwent same index procedure. Time of external fixator application was 3 months. No intra-or postoperative complications were encountered. Postoperative protocol was followed smoothly. At the final follow up, he had improved range of motion of the involved hip joint. Radiologically, all scores that were tested, were also improved. (Tables 2-4)
Discussion
Treatment of LCPD has received no consensus in the literature.9,23 Sequelae of advanced LCPD can lead to joint incongruity and flattening of the femoral head. This results in early degenerative arthritis24,25 and a painful, stiff hip. The collapse of the femoral head occurs mostly during the stages of necrosis and fragmentation.13 Several surgical procedures have been offered but no treatment has been shown convincingly to be significantly effective in improving the outcome of Perthes’ disease or of influencing its course.3
Osman et al2 showed, in their retrospective review, poor outcomes of treatment in LCPD with increasing age. Contrary to this, hip distraction has been shown to be valuable in certain cases of LCPD that have poor outcomes.16,26
The concept of arthrodiastasis was introduced by Aldegheri in 1981.26 Joint distraction aims to neutralize the forces of weight bearing and muscles around the joint, as well as to promote creeping substitution.27,28 The role of arthrodiastasis in LCPD has been evaluated in several studies. Most of these studies4,14,17 performed soft tissue release during the index procedure. They all observed an improvement of the range of motion in the hip joint. They concluded that arthrodiastasis with soft tissue release is a valid method of treatment for LCPD compared to conventional treatment methods. Our present study showed improvement of the range of motion in the hip joint after arthrodiastasis without soft tissue release for an average of 8 days distraction (range 7–9 days) and an average total time of external fixator application of 3.1 months (range 2.5–3.5 months). This good outcome is comparable to other previously published data although they utilized longer time of device application.7,17 Hosny et al16 did not believe in the theoretical advantage of soft tissue release and joint motion during distraction in LCPD as this has not proven clinically. The resulting pain at the site of the release might prevent these patients from having early mobilization of the joint during distraction. This theory might be supported by the concept of intra-articular and/or extra-articular osseous impingement as a cause of this limitation, as suggested by Tannast et al.29 The improvement in the shape of the femoral head and remodeling that occurred during follow-up after hip joint distraction might decrease this impingement and improve the range of motion in the hip joint.
Pain and Trendelenburg limping were present in all patients in our series preoperatively. Both were improved at the final follow-up. Similar results have been published by several studies.4,17 Laklouk et al17 pointed to the additive effect of length gain after distraction, which helps in improving the limping in these patients.
Hip joint stiffness may result from distraction without mobilization. Our patients showed improvement in hip joint flexion by an average of 60 degrees. Using an articulated fixator allowed the patients to mobilize their joint early during distraction. Improvement in hip flexion has been reported by Seveg et al30 utilizing soft tissue release in their operations.
Superficial pin tract infection has been shown to be the most common complication after arthrodiastasis, as demonstrated by the systemic review that was carried out by Ibrahim et al.19 Fortunately, these infections were healed with dressing and parenteral antibiotics. Deep severe infections were rare and usually treated by intravenous antibiotics. Occasionally, they might require premature removal of the fixator. Two patients in our study developed infection. One was superficial and resolved uneventfully with oral antibiotics, and the second necessitated premature removal of the external fixator 2 weeks earlier than the rest of the patients. Femoral fractures, mechanical failure of the fixator, chondrodiastasis and hip subluxation were not observed in this series. Meticulous application of the device with proper clinical determination of center of rotation of the hip decreases mechanical stress on the device and subsequently its failure. This complication has been observed in one study,27 where the device failed at the level of the hinge and another at the hinge-T-clamp coupling.
Radiologically, the remodeling process that occurred in the femoral head of patients in the present study after arthrodiastasis resulted in an improvement in both, the epiphyseal index and the cervical index (Table 4). The SDS at the final follow up was 10.6. This might also indicate a good outcome. Shah et al21 showed in their study that the risk of having Stulberg types III, IV or V at skeletal maturity was associated with SDS of more than 20. Waiting for the time of growth remaining with further improvement might result in significant changes with time. These radiological changes can be correlated with the clinical improvement seen during the follow-up of our patients.
This study has limitations. Of these, small sample size can be related to the rarity of this approach in this group of patients. Another limitation is the short follow-up period. Long-term follow-up until maturity, in addition to comparison with other surgical approaches for both the same age and pathological classification of patients, might be considered as future needs to better clarify the benefits.
Conclusions
In short-term follow-up, Arthrodiastasis with a hinged monolateral external fixator without soft tissue release improved both the clinical and radiological outcomes in this group of patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zheng P, Yang T, Ju L, Jiang B, Lou Y. Epigenetics in Legg–Calvé–Perthes disease: a study of global DNA methylation. J Int Med Res. 2015;43(6):758–764. doi:10.1177/0300060515591062
2. Osman MK, Martin DJ, Sherlock DA. Outcome of late-onset perthes’ disease using four different treatment modalities. J Child Orthop. 2009;3(3):235–242. doi:10.1007/s11832-009-0175-8
3. Maxwell SL, Lappin KJ, Kealey WD, McDowell BC, Cosgrove AP. Arthrodiastasis in perthes’ disease. Preliminary results. J Bone Joint Surg Br. 2004;86-B(2):244–250. doi:10.1302/0301-620X.86B2.14284
4. Amer AR, Khanfour AA. Arthrodiastasis for late onset perthes’ disease using a simple frame and limited soft tissue release: early results. Acta Orthop Belg. 2011;77(4):472–479.
5. Stulberg SD, Cooperman DR, Wallenstein R. The natural history of Legg-Calve-Perthes disease. J Bone Joint Surg Am. 1981;63(7):1095–1108. doi:10.2106/00004623-198163070-00006
6. Mazda K, Penneçot GF, Zeller R, Taussig G. Perthes’ disease after the age of twelve years. Role of the remaining growth. J Bone Joint Surg Br. 1999;81-B(4):696–698. doi:10.1302/0301-620X.81B4.0810696
7. Singh A, Srivastava RN, Shukla P, Pushkar A, Ali S. Management of late onset perthes: evaluation of distraction by external fixator—5-year follow-up. Adv Orthop. 2014;2014:135236. doi:10.1155/2014/135236
8. Herring JA, Neustadt JB, Williams JJ, Early JS, Browne RH. The lateral pillar classification of Legg-Calvé-Perthes disease. J Pediatr Orthop. 1992;12(2):143–150. doi:10.1097/01241398-199203000-00001
9. Hefti F, Clarke NM. The management of Legg-Calvé-Perthes’ disease: is there a consensus?: a study of clinical practice preferred by the members of the European Paediatric Orthopaedic Society. J Child Orthop. 2007;1(1):19–25. doi:10.1007/s11832-007-0010-z
10. Herring JA, Kim HT, Browne R. Legg-Calvé-Perthes disease. Part II: prospective multicenter study of the effect of treatment on outcome. J Bone Joint Surg Am. 2004;86(10):2121–2134. doi:10.2106/00004623-200410000-00002
11. Javid M, Wedge JH. Radiographic results of combined Salter innominate and femoral osteotomy in Legg-Calvé-Perthes disease in older children. J Child Orthop. 2009;3(3):229–234. doi:10.1007/s11832-009-0171-z
12. Joseph B. Legg-Calve-Perthes Disease. In: Alshryda S, Jason J, Howard JS, Huntley JGS, editors. The Pediatric and Adolescent Hip Essentials and Evidence. Switzerland: Springer Nature; 2019:169–191.
13. Luzo CA, Guarniero R, Montenegro NB, de Godoy Junior RM. Initial experience of use of an articulated external fixator in treating Legg-Calvé-Perthes disease by means of arthrodiastasis during the active phase of the disease. Rev Bras Ortop. 2016;51(3):337–345. doi:10.1016/j.rbo.2015.08.002
14. Kocaoglu M, Kilicoglu OI, Goksan SB, Cakmak M. Ilizarov fixator for treatment of Legg-Calvé-Perthes disease. J Pediatr Orthop B. 1999;8(4):276–281.
15. Volpon JB. Comparison between innominate osteotomy and arthrodistraction as a primary treatment for Legg-Calvé-Perthes disease: A prospective controlled trial. Int Orthop. 2012;36(9):1899–1905. doi:10.1007/s00264-012-1598-2
16. Hosny GA, El-Deeb K, Fadel M, Laklouk M. Arthrodiastasis of the hip. J Pediatr Orthop. 2011;31(2):S229–S234. doi:10.1097/BPO.0b013e318223b45a
17. Laklouk MA, Hosny GA. Hinged distraction of the hip joint in the treatment of perthes disease: evaluation at skeletal maturity. J Pediatr Orthop B. 2012;21(5):386–393. doi:10.1097/BPB.0b013e328354b0ab
18. Thacker MM, Feldman DS, Madan SS, Straight JJ, Scher DM. Hinged distraction of the adolescent arthritic hip. J Pediatr Orthop. 2005;25(2):178–182. doi:10.1097/01.bpo.0000150811.33920.27
19. Ibrahim YH, Kersh MA, Fahmy H. Arthrodiastasis in the management of perthes disease: a systematic review. J Pediatr Orthop B. 2020;29(6):550–555.
20. Pagé MG, Katz J, Stinson J, Isaac L, Martin-Pichora AL, Campbell F. Validation of the numerical rating scale for pain intensity and unpleasantness in pediatric acute postoperative pain: sensitivity to change over time. J Pain. 2012;13(4):359–369. doi:10.1016/j.jpain.2011.12.010
21. Shah H, Siddesh ND, Pai H, Tercier S, Joseph B. Quantitative measures for evaluating the radiographic outcome of Legg-Calvé-Perthes disease. J Bone Joint Surg Am. 2013;95(4):354–361. doi:10.2106/JBJS.L.00172
22. Shapiro F. Pediatric Orthopedic Deformities, Volume 2. Switzerland: Springer Nature; 2019:270.
23. Nguyen NA, Klein G, Dogbey G, McCourt JB, Mehlman CT. Operative versus nonoperative treatments for Legg-Calvé-Perthes disease: A meta-analysis. J Pediatr Orthop. 2012;32(7):697–705. doi:10.1097/BPO.0b013e318269c55d
24. McAndrew MP, Weinstein SL. A long-term follow-up of Legg-Calvé-Perthes disease. J Bone Joint Surg Am. 1984;66(6):860–869. doi:10.2106/00004623-198466060-00006
25. Danielsson L, Pettersson H, Sundén G. Early assessment of prognosis in perthes’ disease. Acta Orthop Scand. 1982;53(4):605–611. doi:10.3109/17453678208992266
26. Aguado-Maestro I, Abril JC, Bañuelos Diaz A, García Alonso M. Hip arthrodiastasis in Legg-Calvé-Perthes disease. Rev Esp Cir Ortop Traumatol. 2016;60(4):243–250.
27. Aldegheri R, Trivella G, Saleh M. Articulated distraction of the hip. Conservative surgery for arthritis in young patients. Clin Orthop Rel Res. 1994;(301):94–101.
28. Kucukkaya M, Kabukcuoglu Y, Ozturk I, Kuzgun U. Avascular necrosis of the femoral head in childhood: the results of treatment with articulated distraction method. J Pediatr Orthop. 2000;20(6):722–728. doi:10.1097/01241398-200011000-00005
29. Tannast M, Hanke M, Ecker TM, Murphy SB, Albers CE, Puls M. LCPD: reduced range of motion resulting from extra- and intraarticular impingement hip. Clin Orthop Rel Res. 2012;470(9):2431–2440. doi:10.1007/s11999-012-2344-1
30. Segev E, Ezra E, Wientroub S, Yaniv M. Treatment of severe late onset perthes’ disease with soft tissue release and articulated hip distraction: early results. J Pediatr Orthop B. 2004;13(3):158–165.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.