Back to Journals » Therapeutics and Clinical Risk Management » Volume 11
Risk factors for osteoporosis in Japan: is it associated with Helicobacter pylori?
Authors Asaoka D, Nagahara A, Shimada Y, Matsumoto K, Ueyama H, Matsumoto K, Nakagawa Y, Takeda T, Tanaka I, Sasaki H, Osada T, Hojo M, Watanabe S
Received 9 January 2015
Accepted for publication 13 February 2015
Published 6 March 2015 Volume 2015:11 Pages 381—391
DOI https://doi.org/10.2147/TCRM.S80647
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Daisuke Asaoka, Akihito Nagahara, Yuji Shimada, Kenshi Matsumoto, Hiroya Ueyama, Kohei Matsumoto, Yuta Nakagawa, Tsutomu Takeda, Ippei Tanaka, Hitoshi Sasaki, Taro Osada, Mariko Hojo, Sumio Watanabe
Department of Gastroenterology, University of Juntendo, School of Medicine, Tokyo, Japan
Background: A number of diseases and drugs may influence bone mineral density; however, there are few reports concerning the relationship between lifestyle-related diseases and osteoporosis in Japan as determined by multivariate analysis. The aim of this study was to investigate the risk factors for osteoporosis and whether infection by or eradication of Helicobacter pylori is associated with osteoporosis.
Methods: Between February 2008 and November 2014, using a cross-sectional study design, we investigated patient profile (age, sex, BMI, alcohol, smoking), H. pylori infection status, comorbidities, internal medicine therapeutic agents (calcium channel blocker, HMG-CoA reductase inhibitors, proton pump inhibitor), serum parameters (Hb, calcium, ΥGTP), bone turn over markers (bone-specific alkaline phosphatase (BAP) and collagen type I cross-linked N telopeptide (NTX), findings on dual-energy x-ray absorptiometry (DEXA) and upper gastrointestinal endoscopy, and Frequency Scale for the Symptoms of GERD score in consecutive outpatients aged ≥50 years at our hospital. We divided the subjects into an osteoporosis group and a non-osteoporosis group and investigated risk factors for osteoporosis between the two groups by bivariate and multivariate analyses.
Results: Of the 255 eligible study subjects, 43 (16.9%) had osteoporosis. Bivariate analysis showed that advanced age, female sex, lower body mass index, lower cumulative alcohol intake, lower Brinkman index, H. pylori positivity, lower hemoglobin, bone-specific alkaline phosphatase, lower prevalence of hiatal hernia, and endoscopic gastric mucosal atrophy were related to osteoporosis. Multivariate analysis showed that advanced age (odds ratio [OR] 1.13, 95% confidence interval [CI] 1.07–1.19, P<0.001), female sex (OR 6.27, 95% CI 2.26–17.39, P<0.001), low BMI (OR 0.82, 95% CI 0.72–0.94, P=0.005), H. pylori positivity (OR 3.00, 95% CI 1.31–6.88, P=0.009), and BAP (OR 1.07, 95% CI 1.01–1.14, P=0.035) were related to osteoporosis.
Conclusion: Advanced age, low BMI, BAP, and H. pylori positivity were risk factors for osteoporosis; however, the success of H. pylori eradication was not a risk factor for osteoporosis in Japan.
Keywords: osteoporosis, risk factor, Helicobacter pylori, eradication, proton pump inhibitor, lifestyle disease
Introduction
The increase in the national cost of health care caused by the increasing numbers of patients requiring nursing care has become a serious worldwide problem in an aging society. Osteoporosis is a silent disease characterized by decreased bone mineral density (BMD) with a risk of spine and hip fractures. There are an estimated 12,800,000 patients with osteoporosis in Japan. The spine and hip fractures caused by osteoporosis are the main factors responsible for patients needing nursing care and becoming bedridden, have a significant impact on the prognosis,1 and are a social burden.2 Since it is expected that one third of the population of Japan will be elderly by 2030, prevention of osteoporosis is an urgent issue. However, the incidence of hip fracture continues to rise in Japan because the rate of diagnosis of osteoporosis before onset of fracture and awareness of risk factors for the disease are low. Intervention by physicians to diagnose osteoporosis before it becomes necessary for orthopedic surgeons to treat the resulting bone fractures is very important.
There is well established evidence regarding risk factors for bone fracture,3,4 including age and sex,5,6 body mass index (BMI),7 alcohol,8,9 and smoking.10 With the westernization of dietary habits, the number of patients in Japan with lifestyle-related diseases such as hypertension, diabetes mellitus, and hyperlipidemia has increased, and a relationship between lifestyle-related diseases and osteoporosis has been suggested. With regard to the digestive organs, several studies have pointed out that inflammatory bowel disease11–13 and gastrectomy14 are related to development of osteoporosis. In more recent years, Helicobacter pylori infection,15–20 hiatal hernia,21 reflux esophagitis,22–24 gastric mucosal atrophy,25 and proton pump inhibitor (PPI) use26,27 have also been identified as possible risk factors for osteoporosis. However, there are few reports about these as risk factors for asymptomatic osteoporosis based on multivariate analysis in Japan. H. pylori infection is a national disease that infects approximately 80% of individuals aged 50 years or older in Japan; however, there has been no report on the relationship between the success of H.pylori eradication and the risk of osteoporosis.
The aim of this study was to investigate the various risk factors for osteoporosis by multivariate analysis and to determine if infection by or eradication of H. pylori is associated with osteoporosis in Japan.
Materials and methods
Between February 2008 and November 2014, using a cross-sectional study design, we acquired information on consecutive outpatients aged ≥50 years at our hospital for the following: patient profile (age, sex, BMI, cumulative alcohol intake [kg], Brinkman index); H. pylori infection status (negative, positive, or successfully eradicated); comorbidities (type 2 diabetes mellitus and hypertension); internal medical therapeutic agents (calcium channel blockers, HMG-CoA reductase inhibitors, and PPIs); serum parameters (hemoglobin [g/dL], calcium [mg/dL], and gamma glutamyl transpeptidase [IU/L]); bone turnover markers (bone-specific alkaline phosphatase [U/L] and collagen type I cross-linked N telopeptide [NTX; nmol BCE/L]); dual-energy X-ray absorptiometry (lumbar BMD [g/cm2]; T-score, young adult mean [%], and Z-score) and lateral vertebral X-rays; findings of upper gastrointestinal endoscopy (reflux esophagitis, hiatal hernia, peptic ulcer disease, endoscopic gastric mucosal atrophy [EGA]); and score on the Frequency Scale for the Symptoms of GERD [FSSG]). We divided the subjects into two groups (with osteoporosis and without osteoporosis) and investigated risk factors for osteoporosis between the two groups by bivariate and multivariate analyses.
BMI was calculated as body weight divided by the square of body height in meters (kg/m2). The Brinkman index score was determined by the number of cigarettes smoked per day multiplied by the number of years of smoking.28 Cumulative alcohol intake was defined as the cumulative intake of ethanol (kg). H. pylori infection status was assessed by the 13C-urea breath test and/or serum antibodies to H. pylori. We defined a positive result for any of these tests as being positive for H. pylori infection. We also defined a successful eradication result by the 13C-urea breath test as negative for H. pylori infection at 4–8 weeks after eradication therapy. In this study, success of eradication of H. pylori was defined as elapse of more than one year since eradication of H. pylori. We defined cases taking a usual dose of calcium channel blocker, HMG-CoA reductase inhibitor, or PPI for more than a half year as users of that specific therapy. Serum bone-specific alkaline phosphatase as a biomarker of bone formation and serum NTX as a biomarker of bone resorption were investigated as bone turnover markers. BMD, T-score, young adult mean, and Z-score at lumbar vertebrae 2–4 (L2–4) were measured by dual-energy X-ray absorptiometry using a Discovery A system (Hologic, Bedford, MA, USA). We investigated for the presence of fragility fractures at the ribs and lumbar spine by lateral vertebral X-rays. The diagnosis of osteoporosis was made in accordance with the 2000 version of the Japanese diagnostic criteria published by the Japanese Society for Bone and Mineral Research.29 Osteoporosis was defined as a lumbar BMD less than 70% of the young adult mean, even in those without any prevalent fragility fracture. Osteoporosis was also defined as the presence of fragility fractures in any bone in a person with a BMD of less than 80% of the young adult mean. In the diagnostic criteria for primary osteoporosis (2012 revision), Soen et al explain the relationship between the World Health Organization criteria and Japanese criteria for osteoporosis as follows. The −2.5 standard deviation-based values are in close agreement with 70% young adult mean for women, but displayed some slight variability for men, although no large differences were observed.30 The FSSG was investigated by a questionnaire on gastroesophageal reflux disease.31 We investigated findings of upper gastrointestinal endoscopy (reflux esophagitis, hiatal hernia, peptic ulcer disease, and EGA). We defined reflux esophagitis as grade A, B, C, and D according to the Los Angeles Classification, and peptic ulcer disease as gastric and/or duodenal ulcer, or ulcer scarring. Hiatal hernia was defined as an apparent separation of the esophagogastric junction and diaphragm impression by more than 2 cm at endoscopy. EGA was classified as C-0 (normal), C-1, C-2, C-3, O-1, O-2, or O-3 using the Kimura-Takemoto classification system,32 which identifies the location of the endoscopic atrophic border. Overall, EGA was scored as 0 for C-0 type, 1 for C-1 type, 2 for C-2 type, 3 for C-3 type, 4 for O-1 type, 5 for O-2 type, and 6 for O-3 type.
We excluded patients with the following: gastrectomy, inflammatory bowel disease, chronic obstructive pulmonary disease, malignant disease (gastric, esophageal, colon, lung, pancreatic, liver, bile duct, gallbladder, breast, uterine, ovarian, prostate, or bladder cancer, or malignant lymphoma, leukemia, multiple myeloma), chronic kidney disease, type 1 diabetes mellitus, hypo/hyperthyroidism, a hypo/hyperparathyroid disorder, rheumatoid arthritis (including other collagen disease), and a premenopausal status. We also excluded patients who were currently or previously treated with agents affecting BMD and causing secondary osteoporosis, including glucocorticoids, hormone replacement therapy, thyroid/parathyroid drugs, psychotropic drugs, anticonvulsants, selective estrogen receptor modulators, vitamin D, calcium, and bisphosphonates. This study was conducted in accordance with the tenets of the Declaration of Helsinki.
Statistical analysis
We divided the subjects into two groups (with osteoporosis and without osteoporosis) and investigated the risk factors for osteoporosis between the two groups by bivariate and multivariate analyses. Multivariate logistic regression analysis was performed using a backward selection method (likelihood ratio). The odds ratio (OR) and 95% confidence interval (CI) were also used to identify the presence and strength of any associations. Standard techniques for model checking, including the model square test, Hosmer–Lemeshow goodness of fit test, Nagelkerke R2, and discriminant hitting ratio, were used to determine the adequacy of the multivariate logistic regression model. All statistical analyses were performed using Statistical Package for the Social Sciences version 19 software (SPSS Inc, Chicago, IL, USA). Statistical significance was inferred at P<0.05.
Results
The clinical characteristics of the 255 eligible cases (120 men [47.1%] and 135 women [52.9%]; mean age 63.2±8.5 [50–86] years; mean BMI 22.9±3.4) are summarized in Table 1.
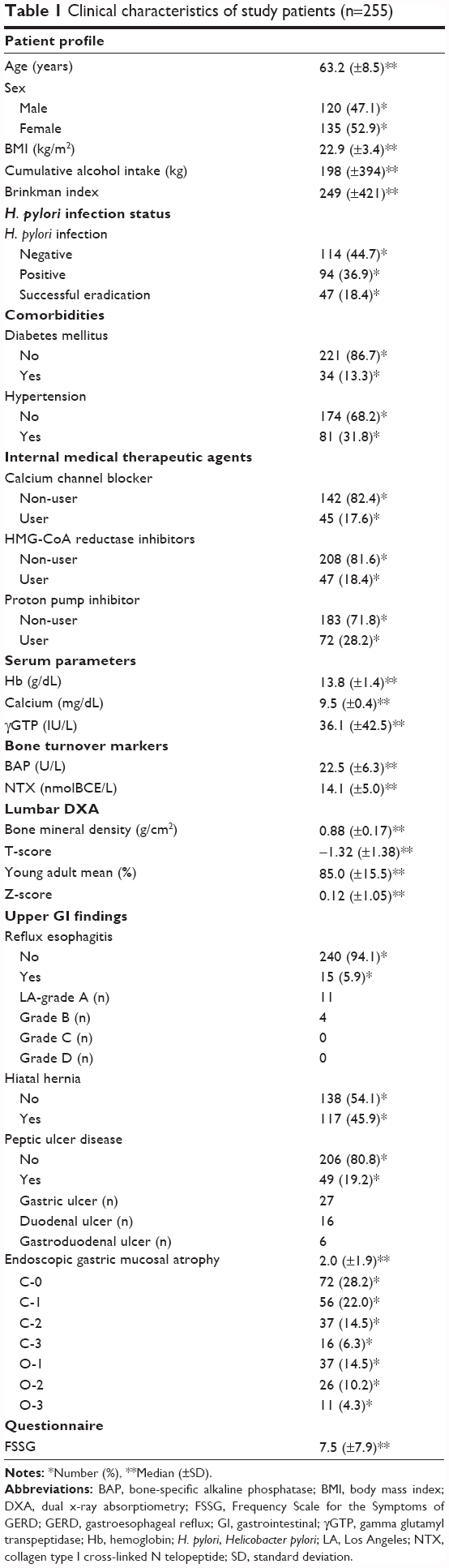 | Table 1 Clinical characteristics of study patients (n=255) |
H. pylori negative, H. pylori positive, and H. pylori successfully eradicated cases were 114 (44.7%), 94 (36.9%), and 47 (18.4%), respectively. The mean time interval since successful eradication of H. pylori was 4.4±3.7 years and the mean age of cases with successful eradication was 59.4±7.4 years (n=47). There were 34 (13.3%) and 81 (31.8%) cases of type 2 diabetes mellitus and hypertension, respectively. Calcium channel blockers, HMG-CoA reductase inhibitors, and PPIs were being taken by 45 (17.6%), 47 (18.4%), and 72 (28.2%) cases, respectively. The mean duration of PPI use among PPI users was 3.2±3.1 years (n=72). Of the 255 eligible cases, 43 (16.9%) had osteoporosis (six [14.0%] men and 37 [86.0%] women). No study patient had kyphosis or fragility fractures determined by lateral vertebral X-ray. Among cases with reflux esophagitis, 11, 4, 0, and 0, respectively, had Los Angeles grade A, B, C, and D disease. Hiatal hernia and peptic ulcer disease were observed in 117 (45.9%) and 49 (19.2%) cases, respectively.
Bivariate analysis
Results of the bivariate analysis are shown in Table 2. In the non-osteoporosis and osteoporosis groups, the mean age was 61.8±8.2 versus 69.8±7.0 years (P<0.001), the proportion of women was 46.2% (98/212) versus 86.0% (37/43; P<0.001), BMI was 23.3±3.3 versus 21.1±3.3 (P<0.001), cumulative alcohol intake was 227±423 versus 54±121 kg (P=0.015), Brinkman index was 274±429 versus 130±357 (P=0.048), those who were H. pylori positive comprised 32.5% (69/212) versus 58.1% (25/43; P=0.006), those in whom H. pylori was successfully eradicated comprised 19.8% (42/212) versus 11.6% (5/43; P=0.889), those with type 2 diabetes mellitus comprised 14.6% (31/212) versus 7.0% (3/43; P=0.190), those with hypertension comprised 32.5% (69/212) versus 27.9% (12/43; P=0.552), calcium channel blocker users comprised 16.0% (34/212) versus 25.6% (11/43; P=0.138), HMG-CoA reductase inhibitor users comprised 17.9% (38/212) versus 20.9% (9/43; P=0.643), and PPI users comprised 27.4% (58/212) versus 32.6% (14/43; P=0.490). Serum values in the non-osteoporosis group compared with the osteoporosis group were 14.0±1.3 versus 12.9±1.2 g/dL for hemoglobin (P<0.001), 9.5±0.3 versus 9.5±0.4 mg/dL for calcium (P=0.138), and 37.6±45.7 versus 28.5±19.4 IU/L for gamma glutamyl transpeptidase (P=0.198). In the non-osteoporosis and osteoporosis groups, BAP was 22.0±6.3 versus 24.9±5.4 IU/L (P=0.007) and NTX was 13.9±5.0 versus 15.2±5.2 nmol BCE/L (P=0.109). Comparing comorbidities between the non-osteoporosis group and the osteoporosis group, reflux esophagitis was present in 6.6% (14/212) versus 2.3% (1/43; P=0.299), respectively, hiatal hernia in 49.5% (105/212) versus 27.9% (12/43; P=0.011), peptic ulcer disease in 17.9% (38/212) versus 25.6% (11/43; P=0.248), and mean score of endoscopic gastric mucosal atrophy (EGA) in 1.9±1.8 versus 2.7±2.2 (P=0.009). The median score on the FSSG questionnaire was 7.7±8.1 versus 6.9±6.7 (P=0.578) for the non-osteoporosis group and the osteoporosis group, respectively.
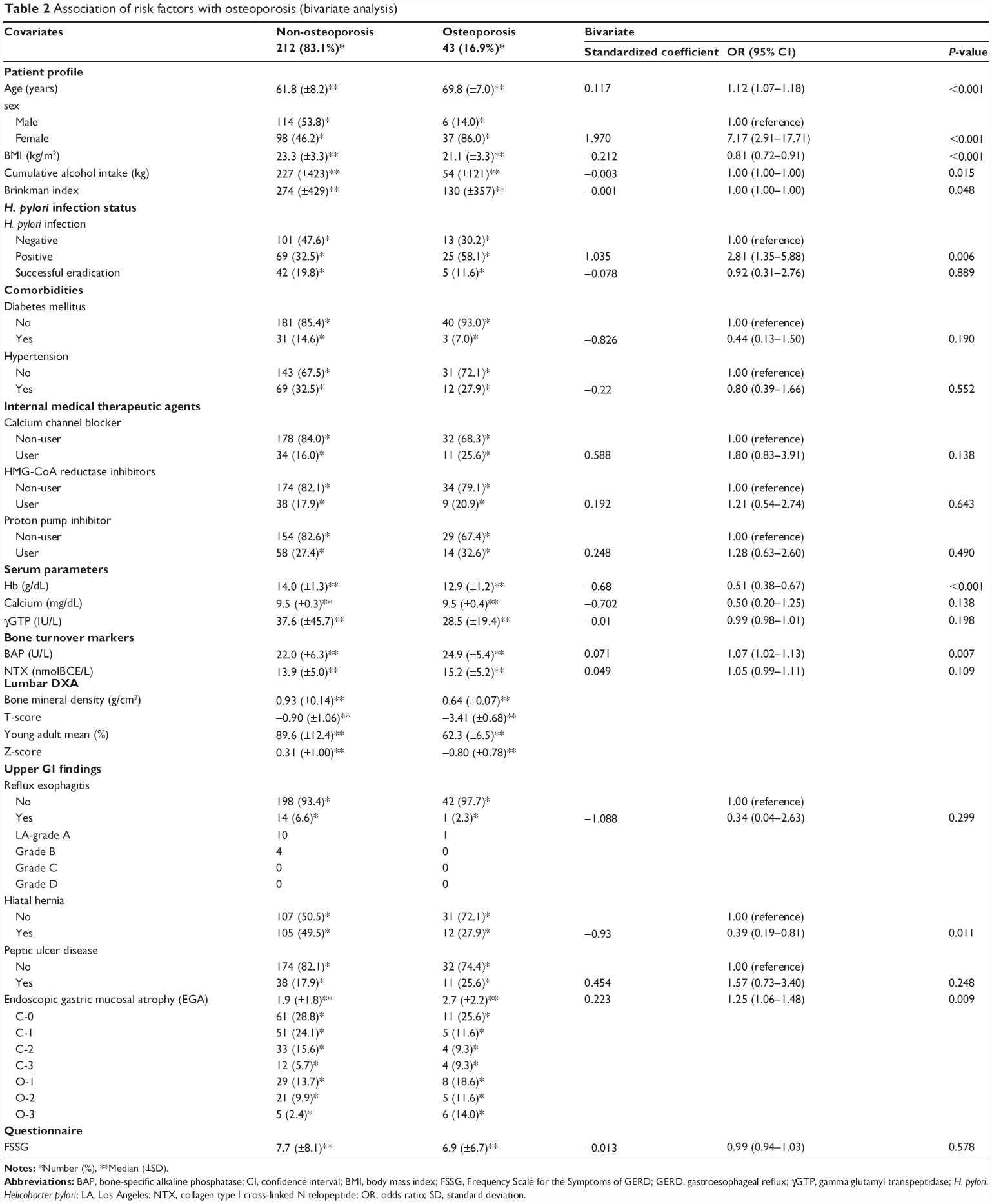 | Table 2 Association of risk factors with osteoporosis (bivariate analysis) |
Multivariate logistic regression analysis
Models were adjusted for the parameters of age, sex, BMI, cumulative alcohol intake, Brinkman index, H. pylori infection status, type 2 diabetes mellitus, calcium channel blocker, PPI, hemoglobin, calcium, gamma glutamyl transpeptidase, bone-specific alkaline phosphatase, NTX, hiatal hernia, and EGA. Statistical compatibility in the multivariate analysis was as follows: model square test, P<0.01; Hosmer–Lemeshow goodness of fit test, P=0.925; Nagelkerke R2, 0.437; and the discriminant hitting ratio, 83.1%. Multivariate logistic regression showed that advanced age (OR 1.13, 95% CI 1.07–1.19, P<0.001), female sex (OR 6.27, 95% CI 2.26–17.39, P<0.001), lower BMI (OR 0.82, 95% CI 0.72–0.94, P=0.005), H. pylori positivity (OR 3.00, 95% CI 1.31–6.88, P=0.009), and high BAP (OR 1.07, 95% CI 1.01–1.14, P=0.035) were related to osteoporosis (Table 3). PPI users tended to be associated with having osteoporosis (P=0.073) and successful eradication of H. pylori was not related to osteoporosis (P=0.657). None of the other factors examined were related to osteoporosis.
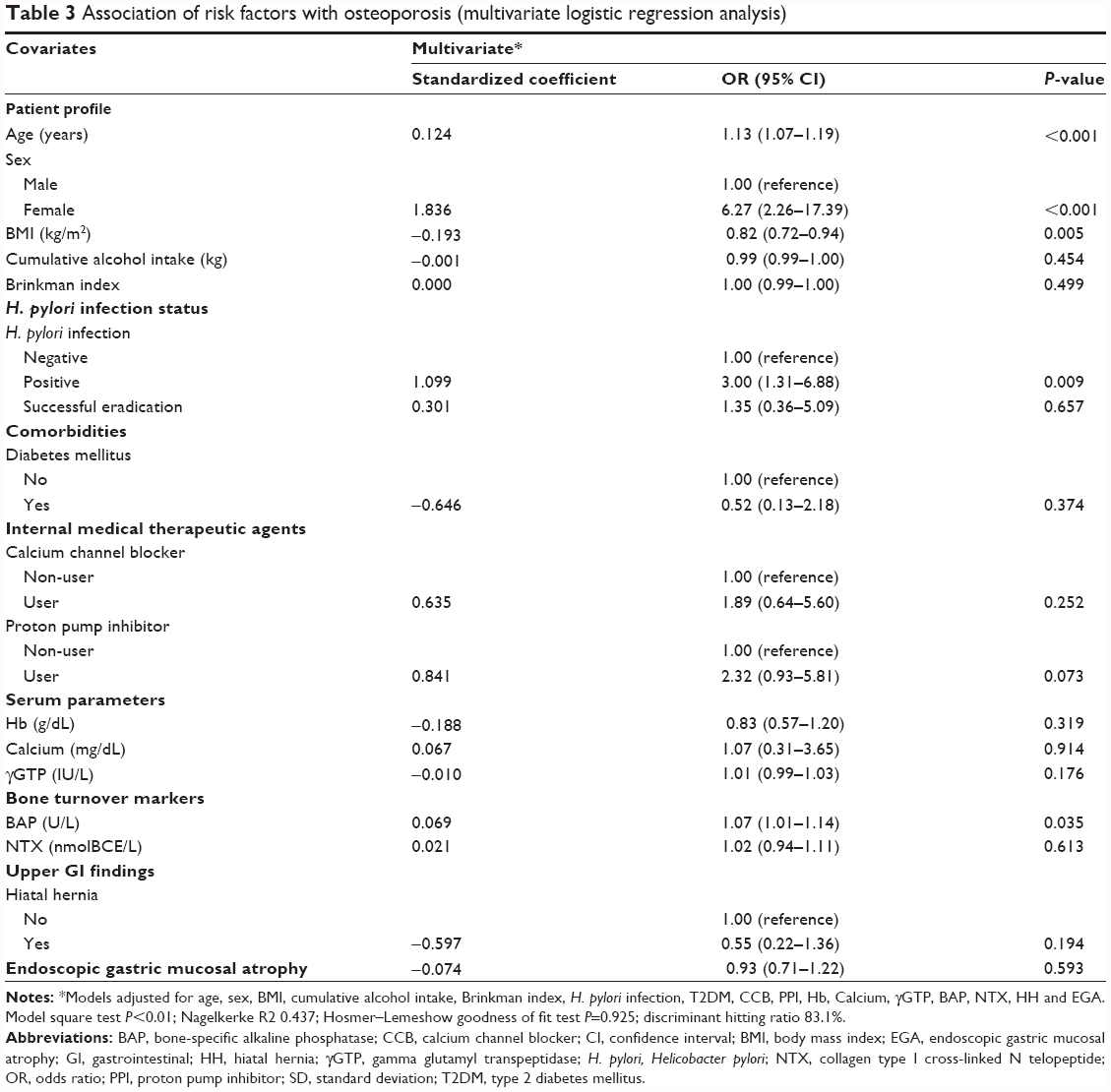 | Table 3 Association of risk factors with osteoporosis (multivariate logistic regression analysis) |
Discussion
This cross-sectional study investigated the risk of osteoporosis associated with various diseases and drugs by multivariate analysis in Japanese cases. Our results clarified for the first time that H. pylori infection is a risk factor for osteoporosis; however, the success of H.pylori eradication did not associate with osteoporosis. H. pylori chronically infects more than 50% of the human population, and the relationship between H. pylori infection and non-gastric conditions, such as lifestyle-related diseases, has recently started to attract attention.
Regarding inflammatory cytokines after eradication of H. pylori, Moss et al33 and Yamaoka et al34 reported that tumor necrosis factor-alpha and interleukin-8 significantly decreased the expression of mRNA compared to its expression before eradication. Furthermore, according to one meta-analysis, gastric mucosal atrophy of the gastric corpus and antrum was improved by successful eradication of H. pylori.35 In Japan, it was reported that gastric mucosal atrophy was improved 10 years after eradication of H. pylori.36 Iijima et al37 reported that gastric acid secretion has a tendency to increase gradually after eradication of H. pylori. Inflammatory cytokines are known to promote bone resorption38 and the decrease in gastric acid secretion causes digestive and absorption disorders relating to bone metabolism, such as for calcium.39 A decrease in levels of inflammatory cytokines and improvement in gastric mucosal atrophy after the success of H.pylori eradication may contribute to prevent the onset of osteoporosis. It was suggested that, since the mean duration after successful eradication of H. pylori was relatively long (4.4±3.7 years) and the mean age at successful eradication was relatively young (59.4±7.4 years), the improvement in BMD had may be seen in the success of H.pylori eradication.
In this study, we examined the relationship between various patient characteristics and osteoporosis, and found that advanced age, female sex, and low BMI were associated with osteoporosis, as in previous reports.5–7,40 The prevalence of H. pylori infection in this study was also similar to that reported elsewhere for Japanese patients 50 years of age or older.41
With regard to the relationship between alcohol and osteoporosis, Kanis et al8 reported that an alcohol intake >20 g per day influenced bone density, and Berg et al9 reported that excessive alcohol consumption is a risk factor for osteoporosis but that moderate drinking has a good effect on bone. In our study, there were few drinkers with a cumulative alcohol intake more than 1 kg (5.5%, 14/255), and bivariate analysis showed a lower intake of alcohol in the osteoporosis group than in the non-osteoporosis group. This result suggests that moderate drinking might favorably influence BMD.
Concerning the relationship between smoking and osteoporosis, Hopper et al reported that smoking more than 20 cigarettes per day influenced bone density.10 Because the number of smokers of more than 20 cigarettes per day was low in our subjects (9.8%, 25/255), smoking may not have influenced bone metabolism in this study.
The possibility that various diseases and drugs aside from those previously known to be risk factors could influence bone density was suggested. To investigate a possible association between these diseases and drugs with BMD, we targeted subjects who did not have diseases (such as chronic kidney disease, chronic obstructive pulmonary disease, malignancy) and who did not take drugs (steroids, bisphosphonates) for which there was previous evidence of an influence on BMD,42,43 and investigated the relationship between these factors and osteoporosis by multivariate analysis.
It was reported that even though the BMD of type 2 diabetes mellitus was similar with nondiabetic patients, the relative risk of vertebral fracture was high in patients with type 2 diabetes mellitus.44 A meta-analysis revealed that the relative risk of hip fracture increased in the patients with type 2 diabetes mellitus in comparison with a control group.45,46 In our study, we investigated the risk of osteoporosis, but not bone fracture, in type 2 diabetes mellitus, and found that type 2 diabetes mellitus was not a risk factor for osteoporosis, as reported previously. However, evaluation of risk factors for bone fracture in patients with type 2 diabetes mellitus may be clinically important in the future.
With regard to hypertension, Cappuccio et al47 reported that systolic blood pressure is related to femoral BMD. Tsuda et al48 suggested that high blood pressure might be associated with reduced BMD in females with untreated hypertension. In the association between antihypertensive agents and bone metabolism by meta-analysis, Wiens et al reported that thizide diuretics and beta-blockers appeared to lower the risk of fractures.49 There has not been a large-scale clinical study of the relationship between use of calcium channel blockers and osteoporosis. The relationship between hypertension, antihypertensive agents, and osteoporosis was not seen. The limitations were: no comparison between those having treatment and those not having treatment in patients with hypertension; we only investigated calcium channel blocker use among antihypertensive agents, therefore the relationship between hypertension, antihypertensive agents and osteoporosis might not be detected.
HMG-CoA reduces cholesterol composition by inhibiting the mevalonate metabolic pathway. Because inhibition of bone resorption is related to inhibition of this pathway, HMG-CoA may contribute to the inhibition of bone resorption.50 Chung et al reported that BMD in users of HMGCoA reductase inhibitors was increased in comparison with that in nonusers in a large-scale clinical study.51 On the other hand, Rejnmark et al reported that HMGCoA reductase inhibitors did not change BMD at the lumbar and femoral vertebrae.52 It is thought that there is not sufficient evidence to suggest an action of HMGCoA reductase inhibitors on bone, and in this study a clear association between use of HMGCoA reductase inhibitors and osteoporosis was not found.
PPIs are first-line therapy for gastroesophageal reflux disease and are the most popular gastric acid secretion inhibitors worldwide. Since ionization of calcium with gastric acid is affected by strong suppression of gastric acid secretion, it is thought that osteoporosis is caused by digestive and absorption disorders involving calcium.53 On the other hand, it is thought that PPIs inhibit bone resorption by inhibiting the proton pump in osteoclasts. In recent years, several studies have reported that high-dose PPI is a risk factor for hip fracture;26,27 however, these reports were retrospective in nature. In our cross-sectional study the multivariate analysis revealed that PPI use showed a tendency (P=0.073) toward a relationship with osteoporosis; however, as in the results of a large study in Western countries,26,54 the relationship between PPI use and osteoporosis remains controversial, and a multicenter prospective study including a large number of cases will be necessary.
There are various reports on the association between gastroesophageal reflux disease and osteoporosis. In previous reports, subjects were often already complicated by multiple vertebral fractures.21–24 In this study, conducted in the setting of internal medicine in an urban area, no case was complicated with vertebral fracture or kyphosis. In addition, results from the FSSG symptom questionnaire on gastroesophageal reflux disease did not differ between groups. Further, in bivariate analysis there was a low prevalence of hiatal hernia in the osteoporosis group compared with that in the non-osteoporosis group. The non-osteoporotic patients often had hiatal hernia and were negative for H. pylori. This result is consistent with a previous report that patients with reflux esophagitis often had hiatal hernia and were negative for H. pylori.55
Sawicki et al reported that peptic ulcer disease was an independent risk factor for osteoporosis.56 In patients with peptic ulcer disease, the gastric and duodenal epithelium are defective, and inflammation at these sites may cause malabsorption of calcium and other substances, such as macroelements, that play a crucial role in mineral homeostasis and bone metabolism.57 Our results demonstrated that peptic ulcer disease was not a risk factor for osteoporosis, and disorders of the small intestine may contribute more to absorption of various nutrients than disorders of the stomach and duodenum.
The decrease in dissolution of calcium salts by the decrease in gastric acid secretion in patients with atrophic gastritis may also result in malabsorption of calcium.39 Kim et al25 reported that atrophic gastritis was associated with an increased likelihood of osteoporosis. Results for EGA in our data did not correlate with osteoporosis in multivariate analysis, and it was suggested that EGA was a confounding factor of H. pylori.
With regard to markers of bone metabolism, it was shown that bone-specific alkaline phosphatase was related to osteoporosis. The osteoporosis patients in this study were considered to be young (mean age 69.8±7.0 years), and 86.0% (37/43) of the cases were female, suggesting that most had the high turnover type of osteoporosis. NTX was not significantly related to osteoporosis in our study. The circadian rhythm of NTX activity may have influenced the result of blood examination.
Conclusion
This cross-sectional study revealed various diseases and drugs as risk factors for osteoporosis by multivariate analysis of Japanese cases and clarified for the first time that H. pylori infection is a risk factor for osteoporosis. However, the success of H.pylori eradication is not associated with the risk of osteoporosis. Because H. pylori infection is a national disease in Japan, affecting approximately 80% of those aged 50 years or older, and osteoporosis is a serious disease causing causes hip fracture and affecting the lifespan, we believe that we should be providing medical care in consideration of these risk factors for osteoporosis in clinical practice.
This study has some limitations. The data were collected from outpatients at a university hospital (a single-center trial) in an urban community in Japan. The study participants were not a random sample of subjects, and we did not investigate their family history of osteoporosis or certain other important risk factors, such as exercise, sunlight exposure, dietary calcium intake, or other nutrients. Further, the number of participants in this cross-sectional study was not very large, so a large prospective multicenter trial will be required.
Disclosure
The authors report no conflicts of interest in this work.
References
Suzuki T, Yoshida H. Low bone mineral density at femoral neck is a predictor of increased mortality in elderly Japanese women. Osteoporos Int. 2010;21:71–79. | ||
Ding H, Koinuma N, Stevenson M, Ito M, Monma Y. The cost-effectiveness of risedronate treatment in Japanese women with osteoporosis. J Bone Miner Metab. 2008;26:34–41. | ||
Suzuki T, Yoshida H, Hashimoto T, et al. Case-control study of risk factors for hip fractures in the Japanese elderly by a Mediterranean Osteoporosis Study (MEDOS) questionnaire. Bone. 1997;21:461–467. | ||
Yoshimura N, Suzuki T, Hosoi T, Orimo H. Epidemiology of hip fracture in Japan: incidence and risk factors. J Bone Miner Metab. 2005;23 Suppl:78–80. | ||
Suzuki T. Risk factors for osteoporosis in Asia. J Bone Miner Metab. 2001;19:133–141. | ||
Fujita T. Global assessment of risk factors for osteoporosis. J Bone Miner Metab. 2001;19:131–132. | ||
Nakaoka D, Sugimoto T, Kaji H, et al. Determinants of bone mineral density and spinal fracture risk in postmenopausal Japanese women. Osteoporos Int. 2001;12:548–554. | ||
Kanis JA, Johansson H, Johnell O, et al. Alcohol intake as a risk factor for fracture. Osteoporos Int. 2005;16:737–742. | ||
Berg KM, Kunins HV, Jackson JL, et al. Association between alcohol consumption and both osteoporotic fracture and bone density. Am J Med.2008;121:406–418. | ||
Hopper JL, Seeman E. The bone density of female twins discordant for tobacco use. N Engl J Med. 1994;330:387–392. | ||
Bernstein CN, Leslie WD, Leboff MS. AGA technical review on osteoporosis in gastrointestinal diseases. Gastroenterology. 2003;124:795–841. | ||
Genant HK, Mall JC, Wagonfeld JB, Horst JV, Lanzi LH. Skeletal demineralization and growth retardation in inflammatory bowel disease. Invest Radiol. 1976;11:541–549. | ||
Schulte CM. Review article: bone disease in inflammatory bowel disease. Aliment Pharmacol Ther. 2004;20 Suppl 4:43–49. | ||
Adachi Y, Shiota E, Matsumata T, Iso Y, Yoh R, Kitano S. Osteoporosis after gastrectomy: bone mineral density of lumbar spine assessed by dual-energy X-ray absorptiometry. Calcif Tissue Int. 2000;66:119–122. | ||
Figura N, Gennari L, Merlotti D, et al. Prevalence of Helicobacter pylori infection in male patients with osteoporosis and controls. Dig Dis Sci. 2005;50:847–852. | ||
Kakehasi AM, Mendes CM, Coelho LG, Castro LP, Barbosa AJ. The presence of Helicobacter pylori in postmenopausal women is not a factor to the decrease of bone mineral density. Arq Gastroenterol. 2007;44:266–270. | ||
Akkaya N, Akkaya S, Polat Y, et al. Helicobacter pylori seropositivity in patients with postmenopausal osteoporosis. J Phys Ther Sci. 2011;23:61–64. | ||
Kakehasi AM, Rodrigues CB, Carvalho AV, Barbosa AJ. Chronic gastritis and bone mineral density in women. Dig Dis Sci. 2009;54:819–824. | ||
Asaoka D, Nagahara A, Hojo M, et al. The relationship between H. pylori infection and osteoporosis in Japan. Gastroenterol Res Pract. 2014;2014:340765. | ||
Lin SC, Koo M, Tsai KW. Association between Helicobacter pylori infection and risk of osteoporosis in elderly Taiwanese women with upper gastrointestinal diseases: a retrospective patient record review. Gastroenterol Res Pract. 2014;2014:814756. | ||
Yamaguchi T, Sugimoto T, Yamada H, et al. The presence and severity of vertebral fractures is associated with the presence of esophageal hiatal hernia in postmenopausal women. Osteoporos Int. 2002;13:331–336. | ||
Miyakoshi N, Kasukawa Y, Sasaki H, Kamo K, Shimada Y. Impact of spinal kyphosis on gastroesophageal reflux disease symptoms in patients with osteoporosis. Osteoporos Int. 2009;20:1193–1198. | ||
Imagama S, Hasegawa Y, Wakao N, Hirano K, Hamajima N, Ishiguro N. Influence of lumbar kyphosis and back muscle strength on the symptoms of gastroesophageal reflux disease in middle-aged and elderly people. Eur Spine J. 2012;21:2149–2157. | ||
Furukawa N, Iwakiri R, Koyama T, et al. Proportion of reflux esophagitis in 6,010 Japanese adults: prospective evaluation by endoscopy. J Gastroenterol. 1999;34:441–444. | ||
Kim HW, Kim YH, Han K, et al. Atrophic gastritis: a related factor for osteoporosis in elderly women. PLoS One. 2014;9:e101852. | ||
Yang YX, Lewis JD, Epstein S, Metz DC. Long-term proton pump inhibitor therapy and risk of hip fracture. JAMA. 2006;296:2947–2953. | ||
Yu EW, Bauer SR, Bain PA, Bauer DC. Proton pump inhibitors and risk of fractures: a meta-analysis of 11 international studies. Am J Med. 2011;124:519–526. | ||
Brinkman GL, Coates EO Jr. The effect of bronchitis, smoking, and occupation on ventilation. Am Rev Respir Dis. 1963;87:684–693. | ||
Orimo H, Hayashi Y, Fukunaga M, et al. Osteoporosis Diagnostic Criteria Review Committee: Japanese Society for Bone and Mineral Research. Diagnostic criteria for primary osteoporosis: year 2000 revision. J Bone Miner Metab. 2001;19:331–337. | ||
Soen S, Fukunaga M, Sugimoto T, et al. Diagnostic criteria for primary osteoporosis: year 2012 revision. J Bone Miner Metab. 2013;31:247–257. | ||
Kusano M, Shimoyama Y, Sugimoto S, et al. Development and evaluation of FSSG: Frequency Scale for the Symptoms of GERD. J Gastroenterol. 2004;39:888–891. | ||
Kimura K, Takemoto T. An endoscopic recognition of the atrophic border and its significance in chronic gastritis. Endoscopy. 1969;3:87–97. | ||
Moss SF, Legon S, Davies J, Calam J. Cytokine gene expression in Helicobacter pylori associated antral gastritis. Gut. 1994;35:1567–1570. | ||
Yamaoka Y, Kita M, Kodama T, Sawai N, Kashima K, Imanishi J. Induction of various cytokines and development of severe mucosal inflammation by cagA gene positive Helicobacter pylori strains. Gut. 1997;41:442–451. | ||
Rokkas T, Pistiolas D, Sechopoulos P, Robotis I, Margantinis G. The long-term impact of Helicobacter pylori eradication on gastric histology: a systematic review and meta-analysis. Helicobacter. 2007;12 Suppl 2:32–38. | ||
Toyokawa T, Suwaki K, Miyake Y, Nakatsu M, Ando M. Eradication of Helicobacter pylori infection improved gastric mucosal atrophy and prevented progression of intestinal metaplasia, especially in the elderly population: a long-term prospective cohort study. J Gastroenterol Hepatol. 2010;25:544–547. | ||
Iijima K, Sekine H, Koike T, Imatani A, Ohara S, Shimosegawa T. Long-term effect of Helicobacter pylori eradication on the reversibility of acid secretion in profound hypochlorhydria. Aliment Pharmacol Ther. 2004;19:1181–1188. | ||
Tilg H, Moschen AR, Kaser A, Pines A, Dotan I. Gut, inflammation and osteoporosis: basic and clinical concepts. Gut. 2008;57:684–694. | ||
Sipponen P, Härkönen M. Hypochlorhydric stomach: a risk condition for calcium malabsorption and osteoporosis? Scand J Gastroenterol. 2010;45:133–138. | ||
De Laet C, Kanis JA, Odén A, et al. Body mass index as a predictor of fracture risk: a meta-analysis. Osteoporos Int. 2005;16:1330–1338. | ||
Ueda J, Gosho M, Inui Y, et al. Prevalence of Helicobacter pylori infection by birth year and geographic area in Japan. Helicobacter. 2014;19:105–110. | ||
Jamal SA, Hayden JA, Beyene J. Low bone mineral density and fractures in long-term hemodialysis patients: a meta-analysis. Am J Kidney Dis. 2007;49:674–681. | ||
Lehouck A, Boonen S, Decramer M, Janssens W. COPD, bone metabolism, and osteoporosis. Chest. 2011;139:648–657. | ||
Yamamoto M, Yamaguchi T, Yamauchi M, Kaji H, Sugimoto T. Diabetic patients have an increased risk of vertebral fractures independent of BMD or diabetic complications. J Bone Miner Res. 2009;24:702–709. | ||
Vestergaard P. Discrepancies in bone mineral density and fracture risk in patients with type 1 and type 2 diabetes – a meta-analysis. Osteoporos Int. 2007;18:427–444. | ||
Janghorbani M, Van Dam RM, Willett WC, Hu FB. Systematic review of type 1 and type 2 diabetes mellitus and risk of fracture. Am J Epidemiol. 2007;166:495–505. | ||
Cappuccio FP, Meilahn E, Zmuda JM, Cauley JA. High blood pressure and bone-mineral loss in elderly white women: a prospective study. Study of Osteoporotic Fractures Research Group. Lancet. 1999;354:971–975. | ||
Tsuda K, Nishio I, Masuyama Y. Bone mineral density in women with essential hypertension. Am J Hypertens. 2001;14:704–707. | ||
Wiens M, Etminan M, Gill SS, Takkouche B. Effects of antihypertensive drug treatments on fracture outcomes: a meta-analysis of observational studies. J Intern Med. 2006;260:350–362. | ||
Bauer DC. HMG CoA reductase inhibitors and the skeleton: a comprehensive review. Osteoporos Int. 2003;14:273–282. | ||
Chung YS, Lee MD, Lee SK, Kim HM, Fitzpatrick LA. HMG-CoA reductase inhibitors increase BMD in type 2 diabetes mellitus patients. J Clin Endocrinol Metab. 2000;85:1137–1142. | ||
Rejnmark L, Buus NH, Vestergaard P, et al. Effects of simvastatin on bone turnover and BMD: a 1-year randomized controlled trial in postmenopausal osteopenic women. J Bone Miner Res. 2004;19:737–744. | ||
Hansen KE, Jones AN, Lindstrom MJ, et al. Do proton pump inhibitors decrease calcium resorption? J Bone Miner Res. 2010;25:2786–2795. | ||
Kaye JA, Jick H. Proton pump inhibitor use and risk of hip fractures in patients without major risk factors. Pharmacotherapy. 2008;28:951–959. | ||
Chiba H, Gunji T, Sato H, et al. A cross-sectional study on the risk factors for erosive esophagitis in young adults. Intern Med. 2012;51:1293–1299. | ||
Sawicki A, Regula A, Godwod K, Debinski A. Peptic ulcer disease and calcium intake as risk factors of osteoporosis in women. Osteoporos Int. 2003;14:983–986. | ||
Raisz LG. Physiology and pathophysiology of bone remodeling. Clin Chem. 1999;45:1353–1358. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.