Back to Journals » Therapeutics and Clinical Risk Management » Volume 12
Retargeting the management of hypercholesterolemia – focus on evolocumab
Authors Colletti A, Derosa G ![]() , Cicero A
, Cicero A
Received 7 July 2016
Accepted for publication 15 August 2016
Published 6 September 2016 Volume 2016:12 Pages 1365—1376
DOI https://doi.org/10.2147/TCRM.S116679
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Alessandro Colletti,1 Giuseppe Derosa,2 Arrigo FG Cicero1
1Department of Medical and Surgical Sciences, University of Bologna, Bologna, 2Department of Internal Medicine and Therapeutics, University of Pavia and Policlinico San Matteo Foundation, Pavia, Italy
Abstract: Hypercholesterolemia is one of the main risk factors for atherosclerosis and cardiovascular diseases. The treatment is based on the modification of the diet and lifestyle and if necessary on a pharmacological therapy. The most widely used drugs are the inhibitors of 3-hydroxy-3-methyl-glutaryl coenzyme A reductase (statins); nevertheless, many patients do not reach optimal levels of low-density lipoprotein-cholesterol (LDL-C) even with maximal dosage of statins (eventually associated to ezetimibe) or present side effects, which do not allow them to continue the treatment. Inhibitors of PCSK9 represent a new therapeutic approach for lowering LDL-C. Evolocumab and alirocumab are human monoclonal antibodies, which bind to extracellular PCSK9 and thus interfere with the degradation of low-density lipoprotein receptor. Evolocumab use is approved for the treatment of patients with heterozygous familial hypercholesterolemia (FH) and homozygous FH as an adjunct to diet and maximally tolerated statin therapy or for subjects with clinical atherosclerotic cardiovascular disease who require additional lowering of LDL-C. Phase III clinical trials have demonstrated the effectiveness of evolocumab (140 mg/every 2 weeks or 420 mg/month, via subcutaneous injection) in monotherapy and in combination with statins, in the treatment of patients intolerant to statins or with FH. In monotherapy, it reduces LDL-C by 55%, and its association with statins leads to a reduction of LDL-C by up to 63%–75%. Evolocumab has been demonstrated to be safe and well tolerated. Ongoing clinical trials are assessing the long-term effects of evolocumab on the incidence of cardiovascular risk, safety, and tolerability. This review resumes the available clinical evidence on the efficacy and safety of evolocumab, for which a relatively large amount of clinical data are currently available, and discusses the retargeting of cholesterol-lowering therapy in clinical practice.
Keywords: PCSK9, hyperlipidemia, evolocumab, LDL-C, familial hypercholesterolemia
Introduction
Current guidelines highlight the importance of maintaining adequate levels of low-density lipoprotein-cholesterol (LDL-C), nonhigh-density lipoprotein-cholesterol (nonHDL-C), and apolipoprotein B100 (ApoB) for the prevention of atherosclerosis and of cardiovascular events,1,2 even if the American College of Cardiology/American Heart Association (ACC/AHA) guidelines do not have a target-focused approach.1 A number of approaches to lower LDL-C have been well studied: these include lifestyle interventions, drugs, and lipid apheresis.
The first recommendation is the lifestyle improvement,2 eventually supported by some effective lipid-lowering nutraceuticals.3 Then, statins are the first drugs suggested,2 and it has been estimated that statins are able to reduce atherosclerotic cardiovascular disease (ASCVD) risk by 15%–37%, but residual 60%–80% risk still remains and a significant part of this risk is probably related to an insufficient reduction of LDL-C.4
The principle causes of the failure of the treatment are high baseline LDL-C levels, poor compliance, and statin-related side effects, such as muscle symptoms, which concern approximately 5%–29% of patients in clinical practice;5,6 moreover, some subjects present a subtherapeutic response to statins or genetic forms of hypercholesterolemia, as familial hypercholesterolemia (FH). This is a major concern because people with FH, which do not have an adequate and effective therapy, have an estimated 13-fold increased risk of cardiovascular events.7 Consequently, new therapies are needed to improve the health and the prospect of life of these patients.
Bile acid-binding resins, fibrates, niacin, and ezetimibe have been approved as nonstatin agents for treating dyslipidemia.8 However, only ezetimibe has shown a significant decrease of cardiovascular events in hypercholesterolemic subjects, when associated to statins,9 as demonstrated by the Improved Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT), in subjects with high cardiovascular risk and acute coronary syndrome.10 Other pharmacological treatments have been recently approved: lomitapide, which is a microsomal triglyceride (TG) transport protein inhibitor, and mipomersen, the antisense oligonucleotide against ApoB, have been demonstrated to lower LDL-C and are already approved for treating patients with homozygous FH (HoFH). Nevertheless, there is concern about these drugs because of the increased hepatic fat accumulation due to the inhibition of hepatic very low-density lipoprotein secretion.11
Consequently, researchers have focused their attention on new therapeutic approaches to safely reach optimal cholesterol levels and to reduce cardiovascular events in subjects at high risk of cardiovascular disease.
In the past decade, the PCSK9 gene has been identified as a potential target to lower LDL-C levels;12,13 it encodes for PCSK9, which is a serine protease that is expressed prevalently in the liver and is enzymatically inactive following autocatalytic cleavage.14 When it binds the low-density lipoprotein receptor (LDL-R) extracellularly, the complex PCSK9-LDL-R enters the hepatocyte and is degraded by lysosomes, not permitting the recycling of the receptor; therefore, lower concentrations of PCSK9 lead to increased levels of LDL-Rs on hepatocyte surface and a greater clearance of low-density lipoprotein (LDL) from the circulation. Mutations of PCSK9 with a gain of function decrease the number of LDL-Rs at the hepatocyte surface, causing FH.15
A promising therapeutic approach is represented by PCSK9 inhibitors, in particular monoclonal antibodies, which have a great potential due to their ability to bind a selected target with high specificity.16
Evolocumab is a fully human monoclonal immunoglobulin G2, created through recombinant DNA technology with a structure that binds specifically to PCSK9 in the plasma and interferes with its binding to the LDL-R.17
Currently, the Food and Drug Administration and the European Medicine Agency have approved evolocumab (Repatha; Amgen Inc., Thousand Oaks, CA, USA) for the treatment of hypercholesterolemia,18 indicating the treatment in adjunct to diet and maximally tolerated statin therapy in patients with heterozygous FH (HeFH) or HoFH or clinical ASCVD, which require additional lowering of LDL-C.19
This review discusses the clinical evidence on the evolocumab efficacy and safety, suggesting a possible retargeting of cholesterol-lowering therapy in the clinical practice. The aim is to provide a patient-specific therapy, minimizing side effects and reaching the optimal LDL-C levels in subjects with high cardiovascular risk, besides statin therapy.
Evolocumab: from pharmacokinetic data to Phase III clinical trials
In nonhuman primates, the injection of evolocumab leads to a dose-dependent reduction of LDL-C which is already significant after 3 days and maximal after 10 days from the first dose, with a parallel reduction in ApoB levels.13 Its absorption follows nonlinear pharmacokinetics at a dose of 140 mg and linear pharmacokinetics at a dose of 420 mg. After 4 hours from the evolocumab administration, the maximal suppression of unbound plasma PCSK9 can be observed. The evolocumab metabolism follows the immunoglobulin clearance pathways, being degraded to small peptides and individual amino acids.20
The approved doses of evolocumab are subcutaneous (SC) 140 mg every 2 weeks or SC 420 mg once monthly.18
Phase I clinical studies have shown evolocumab monotherapy to reduce LDL-C by up to 64% in healthy subjects and by up to 81% in hypercholesterolemic patients receiving low-to-moderate doses of statins. Phase II trials have confirmed these results, demonstrating reduction of LDL-C by 40%–80%.21 Moreover, significant reductions have also been shown in ApoB, nonHDL-C, TGs, and lipoprotein (a) (Lp[a]), with increases in HDL-C.22
The lipid-lowering effectiveness of the treatment with evolocumab in addition to statin therapy has been tested in subjects who have not had managed to achieve acceptable LDL levels despite maximum statin therapy. This combination has a great potential because statin therapy contributes itself to the increase of the expression of PCSK9 gene through the nuclear transcription factor SREBP-2, so the association of a PCSK9 inhibitor as evolocumab and statins may be particularly indicated in clinical practice.23
The Phase III of LDL-C Assessment with PCSK9 Monoclonal Antibody Inhibition Combined With Statin Therapy (LAPLACE-2) double-blind randomized study has evaluated the effects of evolocumab in association with statin therapy.24 In particular, 1,899 patients with moderate–severe hypercholesterolemia and/or mixed dyslipidemia, after receiving a statin treatment for 4 weeks (statin choices based on cholesterol levels: moderate intensity or high intensity), were randomized into different groups: evolocumab + placebo, ezetimibe + placebo, and placebo only, all in addition to the treatment with statins. At a mean of weeks 10 and 12, evolocumab reduced LDL-C levels by 63%–75% compared to placebo group. Evolocumab also lowered the concentrations of nonHDL-C, ApoB, Lp(a), and TGs (P<0.001 for all). The cases where the side effects have not allowed a continuous treatment with evolocumab were <2%.24
Phase III of Monoclonal Antibody Against PCSK9 to Reduce Elevated LDL-C in Subjects Currently Not Receiving Drug Therapy for Easing Lipid Levels-2 (MENDEL-2) double-blind randomized trial has evaluated the effects of evolocumab monotherapy in comparison with ezetimibe or placebo. This phase included 614 participants with hypercholesterolemia (LDL-C ≥100 and ≤190 mg/dL and Framingham risk scores ≤10%) divided into six groups and treated with SC injection of evolocumab 140 mg biweekly or 420 mg monthly or placebo and ezetimibe.
The reduction of the LDL-C at 12 weeks obtained by the mono-/bi-monthly treatment of evolocumab has been similar (−55%/57% in comparison to the placebo group), and has been 38%–40% greater than that observed in the ezetimibe group (P<0.001 for all compared data). A significant reduction (P<0.001) has also been observed in the values of total cholesterol, ApoB, nonHDL-C, ApoB/apolipoprotein A1, Lp(a), and total cholesterol/HDL-C, compared to both placebo and ezetimibe groups.25
Evolocumab effects on patients affected by FH
Evolocumab has also been tested in patients with FH, a relatively frequent genetic disorder based on low plasma LDL clearance.26 Genetic mutations may be present at levels of ApoB, PCSK9, or LDL-R; the majority of subjects with these genetic mutations suffer from HeFH, characterized by markedly increased cardiovascular disease risk.26 Patients with HoFH present more severe hypercholesterolemia (typically 500 mg/dL of LDL-C in untreated subjects) and an extreme risk of premature cardiovascular disease and death;27 in these subjects, the treatment with statins is able to reduce LDL-C by only 25%, due to the impairment of LDL-R function.28,29
The effectiveness of evolocumab has been tested in HeFH patients. The Reduction of LDL-C With PCSK9 Inhibition in HeFH Disorder Study (RUTHERFORD)-2 study involved 331 subjects with HeFH who, after a month of therapeutic statin stabilization, were randomized into four groups in a ratio of 2:2:1:1 (evolocumab 140 mg once every 2 weeks, evolocumab 420 mg monthly, placebo every 2 weeks, and placebo monthly, respectively). The results at 12 weeks showed that patients treated with evolocumab have reached a reduction of serum cholesterol (63%–68% managed to achieve LDL-C <70 mg/dL), which could not be obtained only with statin therapy (in the placebo group, only 2% of patients had LDL-C <70 mg/dL). The mean percentage reduction of cholesterol in the evolocumab group was 60% (P<0.001) compared with the levels at baseline. This is very relevant considering that the most part of the enrolled patients had already been treated with maximal statin dose associated with ezetimibe and that the observed effect seems not to be affected by the nature of the patient’s LDL-R mutation.30
The Trial Evaluating PCSK9 Antibody in Subjects With LDL-R Abnormalities (TESLA Part B) has evaluated the efficacy of evolocumab in 50 patients with HoFH, as well. After 4 weeks of statin therapy stabilization, patients were randomized into two groups in a 2:1 ratio (evolocumab 420 mg monthly and placebo, respectively). At 12 weeks, patients treated with evolocumab showed a 30.9% reduction of LDL-C (95% confidence interval [CI] −43.9% to −18.0%; P<0.0001) compared to placebo. In TESLA B, the LDL-C reduction under evolocumab treatment has been proportional to the residual LDL-R function; where there had been a relevant loss of function, the drug efficacy appeared to be less than in all other conditions where it had been tested.31
Statins-intolerant patients
Phase III clinical trials have evaluated the potential efficacy and tolerability of evolocumab in monotherapy in patients unable to tolerate statins due to muscle-related or other side effects.32,33
The Phase III Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin Intolerant Subjects (GAUSS-2) double-blind randomized trial has evaluated the effects of evolocumab monotherapy in comparison with ezetimibe. This study involved 307 participants who had experienced in the past intolerance to at least two or more types of statins.
Patients treated with evolocumab (140 mg every 2 weeks or 420 mg monthly) at the end of 12 weeks showed a reduction of LDL-C by 53%–56%, corresponding to treatment differences, vs 37%–39% reduction by ezetimibe (P<0.001). At 12 weeks, the treatment was completed by 96% of patients with evolocumab and 86% with ezetimibe; the subjects, who had not concluded the treatment, had for the most part side effects (six for evolocumab group and eleven for ezetimibe group). The most common side effect (muscle myalgia) had hit the 12% of the participants treated with evolocumab, a lower percentage than the 23% of patients treated with ezetimibe.32
The Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin Intolerant Subjects (GAUSS-3) is a two-stage randomized clinical trial including 511 adult patients with uncontrolled LDL-C levels and history of intolerance to two or more statins enrolled in 2013 and 2014 globally. Phase A used a 24-week crossover procedure with atorvastatin 20 mg or placebo to identify patients having symptoms only with atorvastatin but not placebo. In Phase B, after a 2-week washout, patients were randomized to ezetimibe 10 mg daily or evolocumab 420 mg monthly for 24 weeks. Of the 491 patients who entered Phase A, muscle symptoms occurred in 209 of 491 (42.6%) while taking atorvastatin but not while taking placebo. Of these, 199 entered Phase B, along with 19 who proceeded directly to Phase B due to elevated creatine kinase. LDL-C level at week 24 decreased with ezetimibe by −16.7% (95% CI −20.8% to −12.5%) and with evolocumab by −52.8% (95% CI −55.8% to −49.8%) with a between-group difference of −36.1%. Muscle symptoms were reported in 28.8% of ezetimibe-treated patients and 20.7% of evolocumab-treated patients. Active study drug was stopped due to muscle symptoms in five of 73 ezetimibe-treated patients (6.8%) and one of 145 evolocumab-treated patients (0.7%).33
The main difficulty encountered in trials on statin-intolerant subjects has been the difficulty to correctly define statin intolerance in clinical practice and to define a “real” prevalence of statin intolerance in general population.34,35
In this context, the GAUSS-3 trial has shown that, during the blinded statin–placebo phase, a large number of previously defined statin-intolerant subjects have been able to tolerate atorvastatin 20 mg, while a large number of placebo-treated subjects have claimed muscle-related adverse events. The very high tolerability of PCSK9 inhibitors in “real” statin-intolerant patients is thus relevant, especially for high-risk patients who need to achieve ambitious LDL-C targets.
Evolocumab middle- and long-term effects on patients at high cardiovascular disease risk
The profile of efficacy, safety, and tolerability of evolocumab in the long term has been the subject of the studies Durable Effect of PCSK9 Antibody Compared with Placebo Study (DESCARTES), Open-Label Study of Long-Term Evaluation against LDL Cholesterol (OSLER)-1 (for subjects who completed Phase II of a parent evolocumab trial), and OSLER-2 (for subjects who completed the Phase III). Another objective of these long-term studies has been to analyze the main cardiovascular outcomes and the incidence of cardiovascular events.
In the DESCARTES study, 905 subjects after a pretreatment (from 4 to 12 weeks) based on a dietetic change or a statin/statin and ezetimibe therapy (treatment assigned according to the risk categories delineated by ATP III of the National Cholesterol Education Program) were subjected (due to levels of LDL-C >75 mg/dL) to a treatment with evolocumab (420 mg/month) or placebo in a 2:1 ratio.
At the end of 52 weeks, patients showed on average a 57% reduction in LDL-C levels (P<0.001). In addition, there was a significant reduction in the levels of ApoB (44.2%), non-HDL-C (50.3%), Lp(a) (22.4%), and TGs (11.5%). HDL-C significantly increased by 5.4%.36
In OSLER-1 and OSLER-2 open-label studies, the safety parameters and side effects of evolocumab have been primarily evaluated, followed by the effectiveness of this active ingredient in the long term. A total of 4,465 patients (from the parent Phase II–III trials) were included in the OSLER program (1,324 in OSLER-1 and 3,141 in OSLER-2) and randomized into two groups in the ratio of 1:2. The first group was treated with standard therapy, and the second with evolocumab plus standard therapy (140 mg every 2 weeks in OSLER-1 and on the basis of patient choice 420 mg/month or 140 mg/every 2 weeks in OSLER-2), and was followed for a median of 11.1 months.
The median LDL-C at baseline before randomization in the parent study was 120 mg/dL. At 12 weeks of OSLER study, evolocumab groups showed a reduction in LDL-C by 61% (median level of LDL-C: 48 mg/dL; P<0.0001), which was similar in both OSLER-1 and OSLER-2 compared to the standard therapy groups. In addition, a significant reduction was observed in the levels of nonHDL-C (52%), ApoB (47.3%), total cholesterol (36.1%), TGs (12.6%), and Lp(a) (25.5%) (P<0.0001 for all comparisons).37
Another ongoing large long-term study, the Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk (FOURIER) trial, is involving patients at high cardiovascular risk in statin therapy to assess whether the inclusion of ongoing to standard therapy reduces cardiovascular risk and the number of events in patients with clinically evident vascular disease. The study includes 27,564 patients who have had a cardiovascular event (myocardial infarction, symptomatic peripheral artery, or an ischemic stroke) and who have not reached the target of LDL-C (<70 mg/dL) and/or nonHDL-C (≤100 mg/dL) after >2 weeks of optimized stable lipid-lowering therapy (at least atorvastatin 20 mg daily or equivalent with or without ezetimibe). The randomized double-blind, placebo-controlled trial (1:1 ongoing 140 mg/every 2 weeks or 420 mg/month vs placebo) will be completed by February 2018.38
The available clinical data, included in the Program to Reduce LDL-C and Cardiovascular Outcomes Following Inhibition of PCSK9 In Different Populations (PROFICIO) project, are used for assessing the long-term effects of ongoing on the incidence of cardiovascular risk, safety, and tolerability. According to data reported by the European Society of Cardiology in August of 2015, on a subanalysis of 3,146 patients, the administration of project (140 mg/every 2 weeks or 420 mg/month) for 10 and 12 weeks has led to a reduction of LDL-C from 56.5% to 74.9% compared to placebo and from 36.9% to 44.9% compared to ezetimibe. A significant reduction (P<0.001) has also been observed in the values of total cholesterol, ApoB, nonHDL-C, Lp(a), and TGs, compared to both placebo and ezetimibe groups. Side effects have been well tolerated and comparable in percentage to placebo.22
Finally, the Global assessment of plaque regression with a PCSK9 antibody as measured by intravascular ultrasound (GLAGOV) study, a multicenter, randomized, double-blind, placebo-controlled trial, will be the first study to assess the impact of the evolocumab treatment on the coronary atheroma volume (through a serial coronary intravascular ultrasound). Nine hundred and sixty-eight patients with clinical indication for coronary catheterization, randomized 1:1 (into two groups), will receive evolocumab 420 mg/month or placebo for 78 weeks. The GLAGOV study will be important therefore to explore the regression of atherosclerotic plaque as well as to assess the safety profiles and tolerability of the therapy.39
Tolerability and safety
PCSK9 inhibitors are overall well tolerated and safe. The most prevalent adverse events observed in evolocumab Phase II and III trials are resumed in Table 1. Reactions at the injection site were uniform and comparable to placebo (5% for each group).
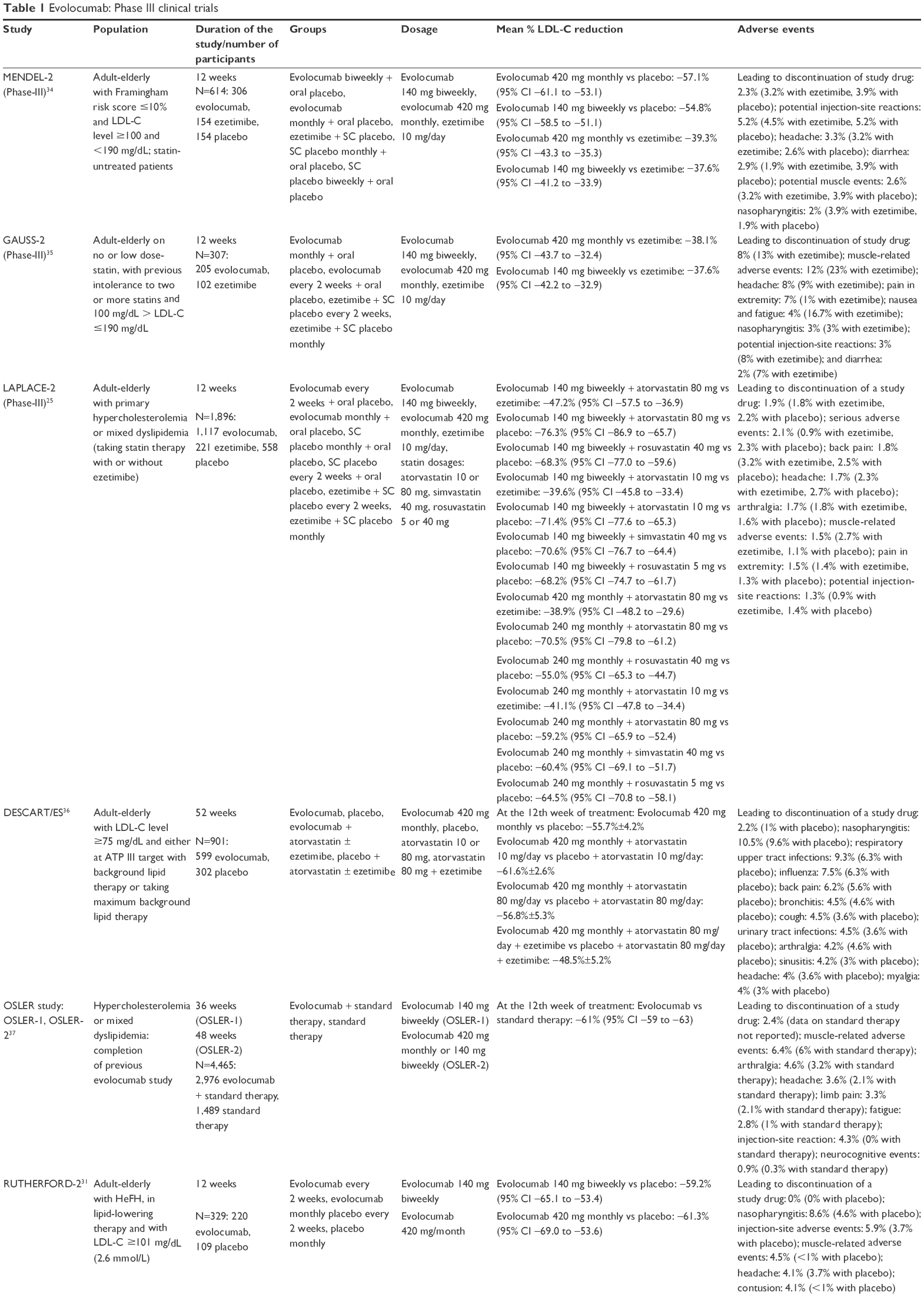 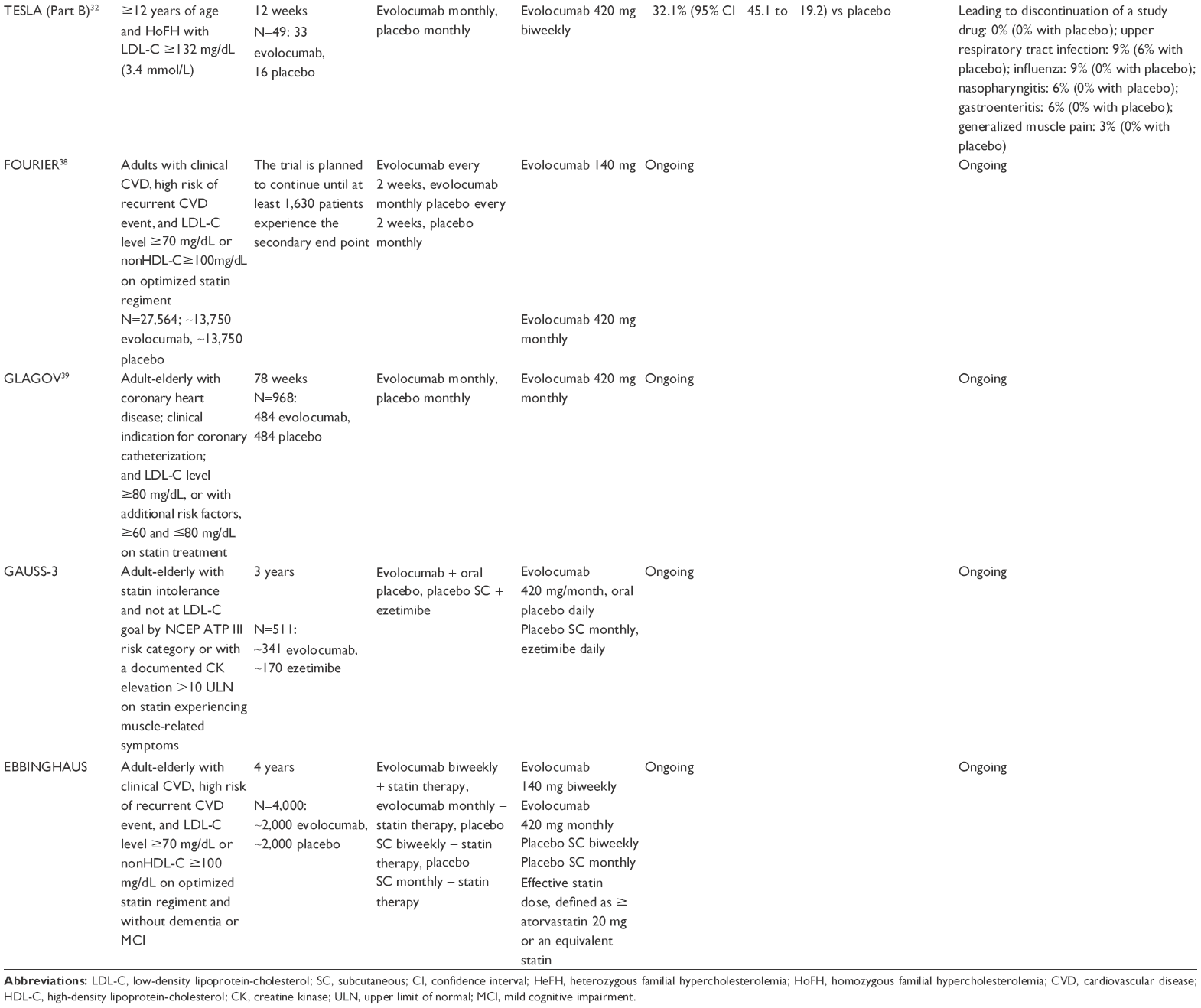 | Table 1 Evolocumab: Phase III clinical trials |
Nasopharyngitis is usually the relatively most common adverse event observed during use of PCSK9 inhibitors but is usually not associated to an increased risk of treatment interruption. The cause of this phenomenon is yet not fully explained and will require further researches.
Middle- and long-term data from the above-cited trials suggest that incidence of muscular problems in PCSK9 inhibitors-treated patients is usually <5% and comparable to the one observed in placebo-treated subjects. From a quantitative point of view, this is a clinically relevant result, considering that statin therapy is related with muscle problems in ~10%–25% of patients treated.40 The prevalence of muscle-related disorders increases when patients previously reporting statin-related side effects are treated with evolocumab but remained always significantly less than the one observed in ezetimibe-treated patients.32,33
In the OSLER trials, side effects were observed in 69.2% of the evolocumab group and 64.8% of the standard therapy group. However, the same percentage of serious side effects was found (7.5%) in both groups. Only 2.4% of patients treated with evolocumab were noncompliant due to side effects. Significant, compared to standard group, neurocognitive events (including delirium confusion, attention and memory disorders, and disorders of thought and perception) were reported by 0.9% of subjects besides the injection-site reactions (4.3%). After 1 year of evolocumab treatment, the rate of cardiovascular events was reduced from 2.18% in the standard therapy group to 0.95% in the evolocumab group (P=0.003).37
Even if available evidence indicate that neurocognitive adverse events may occur more commonly in individuals receiving an antibody to PCSK9, these events are uncommon and have not been associated with on-treatment LDL-C levels. Moreover, it is unclear to what extent closer monitoring of trial participants allocated to PCSK9 inhibitors has led to an ascertainment bias.41 The specific concern about neurocognitive effects of evolocumab will be deeply investigated in a further large trial, Evaluating PCSK9 Binding antiBody Influence oN coGnitive HeAlth in High cardiovascUlar Risk Subjects (EBBINGHAUS) (ClinicalTrials.gov Identifier: NCT02207634). Participants without dementia or mild cognitive impairment at baseline will be randomized in a double-blind, placebo-controlled, multicenter study to evaluate evolocumab + background statin therapy vs statin therapy alone. The primary outcome will be the Spatial Working Memory test, an assessment of executive function. Results are expected in September 2017 with an enrollment of 4,000 subjects.42
Even if Phase III clinical trials have demonstrated the safety of the treatment with evolocumab and the great reduction of LDL-C levels, in particular the association, evolocumab–statins combination raises questions about the potential risk of very low-density lipoprotein-cholesterol concentrations, in particular vitamin E deficiency, hemorrhagic stroke, and impaired steroid hormone synthesis. DESCARTES and OSLER-1 trials evaluated this risk and demonstrated no cases of hemorrhagic stroke in subjects with LDL-C <40 or <25 mg/dL and no increased adverse events between subjects with LDL-C <50 or >50 mg/dL.43,44 Even if cholesterol is needed for steroidogenesis, despite the very low level of LDL-C achieved during evolocumab treatment, there have not been found changes in cortisol, estradiol, or testosterone concentrations after dramatic reducton in circulating LDL-C after treatment with evolocumab. Vitamin E levels instead decreased by a mean of 16% because of the involvement of lipoproteins in the transport of liposoluble vitamins; anyhow, when LDL-C concentrations were normalized, vitamin E raised to previous levels.45 Moreover, from its discovery, we know that the human LDL-C receptor is saturated for plasma level >25 mg/dL;46 this information further supports the safety of extreme LDL-C reduction in most patients.
Discussion
Despite the great success of statin therapy in the treatment of hypercholesterolemia and in prevention of cardiovascular events, some subjects need a different approach. First, a relatively large number of patients needing to reach ambitious LDL-C target such as <70 mg/dL (for instance, diabetics in secondary prevention for cardiovascular disease) are rarely able to reach them with conventional lipid-lowering treatments.47 Then, some forms of hypercholesterolemia as HoFH or HeFH require alternative therapies in combination with standard therapy in order to achieve optimal levels of cholesterol goals and reduce the atherosclerotic cardiovascular risk.31 Thirdly, a relevant part of patients are intolerant to statin therapy (10%–15%), showing some typical side effects such as myopathy/myalgia and hepatotoxicity.48,49 For these subpopulations, it is possible to consider a new therapeutic approach through the PCSK9 inhibitors. However, while patients with myopathy/myalgia have been specifically studied as PCSK9 inhibitors target, the ones with statin-related liver disorders have been excluded from the most part of the studies so that we have yet no direct safety data on them.
Data about the acceptance and adherence to the treatment with evolocumab are important. In particular, patients showed a good acceptance of the use of an injectable therapy: the 74% of the subjects eligible for the OSLER studies decided to join the treatment, while the 26% did not participate for other reasons than tolerability.37 Moreover, the prolonged dosing intervals contributed to increase the adherence.
The treatment with evolocumab (both 420 mg/month and 140 mg/every 2 weeks) has reported in several scenarios a significant activity in reducing LDL-C (Table 1). In addition, the FOURIER study (ongoing) will give information about the relationship between the reduction of LDL-C levels and the cardiovascular risk. In addition, the FOURIER study (ongoing) will further clarify the relationship between the reduction of LDL-C levels and the cardiovascular risk. The final results of FOURIER study will probably support the known law “the lower is the better” applied to LDL-C reduction.37
Data on safety of evolocumab require confirmations in the long term. To date, only one randomized double-blind study (DESCARTES) has lasted 52 weeks. Other clinical studies had a mean duration of 12 weeks. The use of evolocumab for 12 weeks has been demonstrated to be safe and well tolerated by most of the people involved in the studies; only a small percentage of subjects gave up the therapy. The most common side effects have been injection-site reactions, nasopharyngitis, urinary tract infections, back pain, arthralgia, and headache. Myalgia has been reported in only 2% of the patients and in 12% of subjects who suffered from statins-related myalgia.
The fact that the preliminary data on another fully human antibody against PCSK9, alirocumab, are quite similar both in terms of efficacy and safety supports the above-reported data on the advantage of this new class of drugs.50
The effect of PCSK9 inhibitors on other lipid fractions has also to be taken into account. In fact, these drugs, while dramatically reducing LDL-C, are also able to significantly improve the levels of very low-density lipoprotein, TG, HDL-C, and Lp(a). The effect on Lp(a) is of particular interest since the plasma level of this proatherogenic and prothrombotic molecule is mainly genetically determined and resistant to the standard lipid-lowering therapies.51
The results of long-term trials will also give an answer to the debate about the possible development of neutralizing antidrug antibodies that may lead to a loss of the clinical response to the therapy. Current evidence has demonstrated that only 0.1% of the subjects treated with evolocumab presented binding antidrug antibodies, but they did not lower the effectiveness.20
It is important to emphasize that the entry of evolocumab in the market could redefine the strategies in current clinical practice. Possible target of evolocumab population are patients with FH, intolerant to statin therapy (to high side effects and/or poor compliance), or those at “high risk” who still need a further reduction of serum cholesterol not obtainable with only classical therapy.
The most important debate to redefine the current clinical practice will be to define classes of subjects with “high” cardiovascular risk, which then require further reduction of serum cholesterol and thus inhibitors of PCSK9 in combination with standard therapy (statin, statin + ezetimibe, or other combinations).
The results of the ongoing trials on the reduction of cardiovascular risk and improvement of the quality of life in the long term may provide further data to also evaluate the cost:benefit ratio. In fact, a great concern about evolocumab is the cost, much higher respect to other lipid-lowering therapies that may limit the use to a very limited group of subjects with restricted criteria for the treatment.52 However, a recent cost-effectiveness analysis carried out in the US shows that evolocumab treatment has been associated with both increased cost and improved quality-adjusted life years (QALY) (HeFH: incremental cost: US$153,289, incremental QALY: 2.02, incremental cost-effectiveness ratio: US$75,863/QALY; ASCVD: incremental cost: US$158,307, incremental QALY: 1.12, incremental cost-effectiveness ratio: US$141,699/QALY; and ASCVD with statin intolerance: incremental cost: US$136,903, incremental QALY: 1.36, incremental cost-effectiveness ratio: US$100,309/QALY). Evolocumab has met both the ACC/AHA and World Health Organization thresholds in each population evaluated. Thus, the use of evolocumab in these categories of patients has to be considered cost-effective.53
The use of evolocumab associated with low-dose statins in order to reduce the risk of adverse events in subjects at high risk for adverse events is a possibility as well; however, its cost-effectiveness has yet to be evaluated.
Conclusion
In summary, it is possible to state that evolocumab therapy (both 420 mg/month and 140 mg/every 2 weeks), in monotherapy or associated to statins and/or ezetimibe, significantly reduces the levels of LDL-C (53%–75%) in a large range of patients at very high cardiovascular disease risk, including statin-intolerant subjects and FH patients. Moreover, it parallely reduces the levels of ApoB, Lp(a), total cholesterol, and nonHDL-C. Adverse events incidence was comparable to placebo. Its long-term safety with the efficacy on hard cardiovascular outcome reduction is under investigation in the ongoing FOURIER trial.
Disclosure
The authors report no conflicts of interest in this work.
References
Ray KK, Kastelein JJ, Boekholdt SM, et al. The ACC/AHA 2013 guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular disease risk in adults: the good the bad and the uncertain: a comparison with ESC/EAS guidelines for the management of dyslipidaemias 2011. Eur Heart J. 2014;35(15):960–968. | ||
Piepoli MF, Hoes AW, Agewall S, et al. 2016 European guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts): developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;37(29):2315–2381. | ||
Cicero AF, Colletti A. Combinations of phytomedicines with different lipid lowering activity for dyslipidemia management: the available clinical data. Phytomedicine. 2016;23(11):1113–1118. | ||
Sampson UK, Fazio S, Linton MF. Residual cardiovascular risk despite optimal LDL cholesterol reduction with statins: the evidence, etiology, and therapeutic challenges. Curr Atheroscler Rep. 2012;14(1):1–10. | ||
Zhang H, Plutzky J, Skentzos S, et al. Discontinuation of statins in routine care settings – a cohort study. Ann Intern Med. 2013;158(7):526–534. | ||
Blom DJ, Dent R, Castro RC, Toth PP. PCSK9 inhibition in the management of hyperlipidemia: focus on evolocumab. Vasc Health Risk Manag. 2016;12:185–197. | ||
Benn M, Watts GF, Tybjaerg-Hansen A, Nordestgaard BG. Familial hypercholesterolemia in the Danish general population: prevalence, coronary artery disease, and cholesterol-lowering medication. J Clin Endocrinol Metab. 2012;97(11):3956–3964. | ||
Ridker PM. LDL cholesterol: controversies and future therapeutic directions. Lancet. 2014;384(9943):607–617. | ||
DiNicolantonio JJ, Chatterjee S, Lavie CJ, Bangalore S, O’Keefe JH. Ezetimibe plus moderate dose simvastatin after acute coronary syndrome: what are we IMPROVEing on? Am J Med. 2015;128(8):914.e1–914.e4. | ||
Cannon CP, Blazing MA, Braunwald E. Ezetimibe plus a statin after acute coronary syndromes. N Engl J Med. 2015;373(15):1476–1477. | ||
Ahn CH, Choi SH. New drugs for treating dyslipidemia: beyond statins. Diabetes Metab J. 2015;39(2):87–94. | ||
Farnier M. PCSK9: from discovery to therapeutic applications. Arch Cardiovasc Dis. 2014;107(1):58–66. | ||
Chan JC, Piper DE, Cao Q, et al. A proprotein convertase subtilisin/kexin type 9 neutralizing antibody reduces serum cholesterol in mice and nonhuman primates. Proc Natl Acad Sci U S A. 2009;106(24):9820–9825. | ||
Seidah NG, Benjannet S, Wickham L, et al. The secretory proprotein convertase neural apoptosis-regulated convertase 1 (NARC-1): liver regeneration and neuronal differentiation. Proc Natl Acad Sci U S A. 2003;100(3):928–933. | ||
Abifadel M, Varret M, Rabes JP, et al. Mutations in PCSK9 cause autosomal dominant hypercholesterolemia. Nat Genet. 2003;34(2):154–156. | ||
Sible AM, Nawarskas JJ, Anderson JR. PCSK9 inhibitors. An innovative approach to treating hyperlipidemia. Cardiol Rev. 2016;24(3):141–152. | ||
Ito MK, Santos RD. PCSK9 inhibition with monoclonal antibodies – modern management of hypercholesterolemia. J Clin Pharmacol. Epub 2016 May 16. | ||
Repatha. Thousand Oaks, CA: Amgen Inc; 2015. | ||
Cicero AF, Colletti A, Borghi C. Profile of evolocumab and its potential in the treatment of hyperlipidemia. Drug Des Devel Ther. 2015;9:3073–3082. | ||
Cicero AF, Tartagni E, Ertek S. Efficacy and safety profile of evolocumab (AMG145), an injectable inhibitor of the proprotein convertase subtilisin/kexin type 9: the available clinical evidence. Expert Opin Biol Ther. 2014;14(6):863–868. | ||
Farnier M. PCSK9 inhibitors. Curr Opin Lipidol. 2013;24:251–258. | ||
Stein EA, Giugliano RP, Koren MJ, et al; PROFICIO Investigators. Efficacy and safety of evolocumab (AMG 145), a fully human monoclonal antibody to PCSK9, in hyperlipidaemic patients on various background lipid therapies: pooled analysis of 1359 patients in four phase 2 trials. Eur Heart J. 2014;35(33):2249–2259. | ||
Dubuc G, Chamberland A, Wassef H, et al. Statins upregulate PCSK9, the gene encoding the proprotein convertase neural apoptosis-regulated convertase-1 implicated in familial hypercholesterolemia. Arterioscler Thromb Vasc Biol. 2004;24(8):1454–1459. | ||
Robinson JG, Nedergaard BS, Rogers WJ, et al; LAPLACE-2 Investigators. Effect of evolocumab or ezetimibe added to moderate- or high-intensity statin therapy on LDL-C lowering in patients with hypercholesterolemia: the LAPLACE-2 randomized clinical trial. JAMA. 2014;311(18):1870–1882. | ||
Koren MJ, Lundqvist P, Bolognese M, et al; MENDEL-2 Investigators. Anti-PCSK9 monotherapy for hypercholesterolemia: the MENDEL-2 randomized, controlled phase III clinical trial of evolocumab. J Am Coll Cardiol. 2014;63(23):2531–2540. | ||
Hovingh GK, Davidson MH, Kastelein JJ, O’Connor AM. Diagnosis and treatment of familial hypercholesterolaemia. Eur Heart J. 2013;34(13):962–971. | ||
Goldstein JL, Hobbs HH, Brown MS. Familial hypercholesterolemia. In: Scriver CR, Beaudet AL, Sly WS, Valle D, editors. The Metabolic and Molecular Bases of Inherited Disease. 8th ed. New York, NY: McGraw-Hill Inc.; 2001:2863–2913. | ||
Marais AD, Raal FJ, Stein EA, et al. A dose-titration and comparative study of rosuvastatin and atorvastatin in patients with homozygous familial hypercholesterolaemia. Atherosclerosis. 2008;197(1):400–406. | ||
Raal FJ, Pilcher GJ, Illingworth DR, et al. Expanded-dose simvastatin is effective in homozygous familial hypercholesterolaemia. Atherosclerosis. 1997;135(2):249–256. | ||
Raal FJ, Stein EA, Dufour R, et al; RUTHERFORD-2 Investigators. PCSK9 inhibition with evolocumab (AMG 145) in heterozygous familial hypercholesterolaemia (RUTHERFORD-2): a randomised, double-blind, placebo-controlled trial. Lancet. 2015;385(9965):331–340. | ||
Raal FJ, Honarpour N, Blom DJ, et al. Inhibition of PCSK9 with evolocumab in homozygous familial hypercholesterolaemia (TESLA part B): a randomised, double-blind, placebo-controlled trial. Lancet. 2015;385(9965):341–350. | ||
Stroes E, Colquhoun D, Sullivan D, et al; GAUSS-2 Investigators. Anti-PCSK9 antibody effectively lowers cholesterol in patients with statin intolerance: the GAUSS-2 randomized, placebo-controlled phase 3 clinical trial of evolocumab. J Am Coll Cardiol. 2014;63(23):2541–2548. | ||
Nissen SE, Stroes E, Dent-Acosta RE, et al; GAUSS-3 Investigators. Efficacy and tolerability of evolocumab vs ezetimibe in patients with muscle-related statin intolerance: the GAUSS-3 randomized clinical trial. JAMA. 2016;315(15):1580–1590. | ||
Patel J, Martin SS, Banach M. Expert opinion: the therapeutic challenges faced by statin intolerance. Expert Opin Pharmacother. 2016;17(11):1497–1507. | ||
Guyton JR, Bays HE, Grundy SM, Jacobson TA; The National Lipid Association Statin Intolerance Panel. An assessment by the Statin Intolerance Panel: 2014 update. J Clin Lipidol. 2014;8(3 Suppl):S72–S81. | ||
Blom DJ, Hala T, Bolognese M, et al; DESCARTES Investigators. A 52-week placebo-controlled trial of evolocumab in hyperlipidemia. N Engl J Med. 2014;370(19):1809–1819. | ||
Sabatine MS, Giugliano RP, Wiviott SD, et al; Open-Label Study of Long-Term Evaluation against LDL Cholesterol (OSLER) Investigators. Efficacy and safety of evolocumab in reducing lipids and cardiovascular events. N Engl J Med. 2015;372(16):1500–1509. | ||
Sabatine MS, Giugliano RP, Keech A, et al. Rationale and design of the Further cardiovascular OUtcomes Research with PCSK9 Inhibition in subjects with Elevated Risk trial. Am Heart J. 2016;173:94–101. | ||
Puri R, Nissen SE, Somaratne R, et al. Impact of PCSK9 inhibition on coronary atheroma progression: rationale and design of Global Assessment of Plaque Regression with a PCSK9 Antibody as Measured by Intravascular Ultrasound (GLAGOV). Am Heart J. 2016;176:83–92. | ||
Ganga HV, Slim HB, Thompson PD. A systematic review of statin-induced muscle problems in clinical trials. Am Heart J. 2014;168(1):6–15. | ||
Swiger KJ, Martin SS. PCSK9 inhibitors and neurocognitive adverse events: exploring the FDA directive and a proposal for N-of-1 trials. Drug Saf. 2015;38(6):519–526. | ||
Amgen. Evaluating PCSK9 Binding antiBody Influence oN coGnitive HeAlth in High cardiovascUlar Risk Subjects (EBBINGHAUS). Available from: https://clinicaltrials.gov/ct2/show/NCT02207634. Accessed July 23, 2016. | ||
Koren MJ, Blom D, Giugliano RP, et al. Safety and tolerability of very low LDL-C levels in patients treated with 52 weeks of evolocumab (AMG 145). Circulation. 2014;130:16865. | ||
Koren MJ, Giugliano RP, Raal FJ, et al. Efficacy and safety of longer-term administration of evolocumab (AMG 145) in patients with hypercholesterolemia: 52-week results from the open-label study of long-term evaluation against LDL-C (OSLER) randomized trial. Circulation. 2014;129(2):234–243. | ||
Blom DJ, Djedjos CS, Monsalvo ML, et al. Effects of evolocumab on vitamin E and steroid hormone levels. Results from the 52-week, phase 3, double-blind, randomized, placebo-controlled DESCARTES study. Circ Res. 2015;117:731–741. | ||
Brown MS, Goldstein JL. Receptor-mediated control of cholesterol metabolism. Science. 1976;191(4223):150–154. | ||
Ridker PM, Mora S, Rose L; JUPITER Trial Study Group. Percent reduction in LDL cholesterol following high-intensity statin therapy: potential implications for guidelines and for the prescription of emerging lipid-lowering agents. Eur Heart J. 2016;37(17):1373–1379. | ||
Glueck CJ, Shah P, Goldenberg N, et al. Eligibility for PCSK9 treatment in 734 Hypercholesterolemic patients referred to a regional cholesterol treatment center with LDL cholesterol ≥70 mg/dl despite maximal tolerated cholesterol lowering therapy. Lipids Health Dis. 2016;15(1):55. | ||
Gluba-Brzozka A, Franczyk B, Toth PP, et al. Molecular mechanisms of statin intolerance. Arch Med Sci. 2016;12(3):645–658. | ||
Yadav K, Sharma M, Ferdinand KC. Proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors: present perspectives and future horizons. Nutr Metab Cardiovasc Dis. Epub 2016 May 30. | ||
Nordestgaard BG, Chapman J, Ray K, et al; European Atherosclerosis Society Consensus Panel. Lipoprotein(a) as a cardiovascular risk factor: current status. Eur Heart J. 2010;31(23):2844–2853. | ||
(ICER) TIfCaER. PCSK9 inhibitor therapies for high cholesterol: effectiveness, value, and value-based price benchmarks. 2015. Available from: https://icer-review.org/announcements/pcsk9-draft-report-release/. Accessed August 30, 2016. | ||
Gandra SR, Villa G, Fonarow GC, et al. Cost-effectiveness of LDL-C lowering with evolocumab in patients with high cardiovascular risk in the United States. Clin Cardiol. 2016;39(6):313–320. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.