Back to Journals » Medical Devices: Evidence and Research » Volume 7
Results from an international multicenter trial evaluating the ease-of-use of and preference for a newly developed disposable injection pen for the treatment of growth hormone deficiency in treatment-naïve children and adults
Authors Pleil A, Darendeliler F, Dörr H, Hutchinson K, Wollmann H
Received 28 December 2013
Accepted for publication 28 January 2014
Published 11 April 2014 Volume 2014:7 Pages 61—71
DOI https://doi.org/10.2147/MDER.S59821
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Andreas M Pleil,1 Feyza Darendeliler,2 Helmuth G Dörr,3 Katherine Hutchinson,4 Hartmut A Wollmann5
1Pfizer Inc., San Diego, CA, USA; 2Istanbul Faculty of Medicine, Pediatric Endocrinology Unit, Capa, Istanbul, Turkey; 3Department of Pediatrics, University of Erlangen, Erlangen, Germany; 4Quanticate, Hitchin, UK; 5Pfizer Ltd, Walton Oaks, UK
Abstract: Previous research has reported that ease of use of and preference for a delivery device are associated with greater patient compliance – an important factor in achieving optimal therapeutic results. The objective of this study was to assess the ease-of-use of a new disposable pen (GoQuick®, Pfizer, Inc.) versus the current reusable pen (GENOTROPIN Pen®, Pfizer, Inc.) to inject a daily dose of recombinant DNA origin human growth hormone, Genotropin® (somatropin) in standard practice. In this randomized, crossover, multicenter, multinational, open-label study, ease-of-use of and preference for the two pens were assessed in three treatment-naïve populations: 1) parents of very young children; 2) parent–child dyads; and 3) adults via use of a validated self-report Injection Pen Assessment Questionnaire (IPAQ) after 2 months of at-home-use experience. The primary endpoint was the proportion of participants who reported the new disposable pen to be no different from or easier to use than the current reusable pen. Safety was also assessed and reported according to local legal requirements. Of the 120 screened patients, 119 were included in the ease-of-use analysis and all were included in the safety analyses. In all, 67.2% found the new somatropin disposable pen to be no different from or easier to use than the reusable pen (95% confidence interval: 58.8–75.7). Most adverse events were mild or moderate. No deaths or device- or treatment-related serious adverse events were reported. These results suggest that improvements made to the reusable somatropin pen are tangible and recognizable to treatment-naïve patients and their caregivers, child–caregiver dyads, and adults, and may positively impact continued compliance with therapy.
Registry information: ClinicalTrials.gov identifier: NCT01112865.
Keywords: somatropin, disposable injection pen, ease-of-use, Injection Pen Assessment Questionnaire, preference, recombinant human growth hormone
Introduction
Somatropin ([recombinant DNA origin] for injection; Genotropin®; Pfizer Inc., New York, NY) is a recombinant human growth hormone (rhGH) used for the treatment of growth hormone deficiency (GHD) and other forms of growth disturbances in children, as well as growth hormone deficiency in adults. The safety and efficacy profile of somatropin has been demonstrated in a large number of clinical trials and postmarketing studies both in the US and worldwide.1,2 Somatropin is administered by subcutaneous injection using an injection pen – most often the currently available multidose reusable somatropin pen (IMS Health, IMS MIDAS™, 2011). To achieve optimal therapeutic results with growth hormone, continuous long-term treatment adherence is essential.3 To help promote compliance, the device used for drug administration should be simple, convenient, and acceptable to the patient.3
Several steps are required for the patient or caregiver to prepare the current reusable somatropin pen, including the insertion of a two-compartment cartridge, reconstitution of the powdered somatropin, removal of air, and the selection of the correct dose for each injection. Though most pens are user friendly, continuing to improve existing features or introducing new features that can simplify the use of these pens may be warranted for certain populations or situations. These modifications may provide an advantage, as it has been reported that ease-of-use, convenience, and preference for a particular drug delivery device can be associated with greater patient compliance and, ultimately, with improved clinical outcomes.3
A recently developed disposable injection device for somatropin that changes the process of drug administration is being introduced in multiple countries.4 The new pen comes preloaded with unreconstituted medication, obviating the need to load a cartridge and reducing the chance of breakage and improper assembly. The new pen has a simplified drug reconstitution system and a dose memory feature, can deliver a range of dose increments, and allows attachment and removal of the needle without removal of the needle guard. The purpose of this study was to investigate the convenience of (as determined by ease-of-use) and preference for the new disposable somatropin pen as compared with the current reusable somatropin pen. No other manufacturers’ pens were evaluated as part of this study, though there are numerous presentations currently available across Europe.
The target population includes parents or caregivers of young children, child–caregiver dyads, and adults who self-administer. All patients were required to be treatment-naïve at study initiation.
The objective of this study was to quantify the subjective assessment from the perspective of the user of the ease-of-use of two somatropin injection pens. Both an objective measure of each pen use experience and a comparative measure between pen use experiences as assessed by the Injection Pen Assessment Questionnaire (IPAQ) were used. The primary endpoint was the proportion of participants who reported their experience with the new disposable somatropin pen to be no different from or easier to use than the current reusable somatropin pen. Secondary endpoints at the IPAQ item level and by group and category of response are included. An assessment of the safety of both pens based on adverse event reporting and a separate validation of the IPAQ instrument, were also included as study objectives.
Methods
The study was conducted over a 4-month observation period (two 2-month user experiences), with each patient assigned randomly to a sequence of exposure – the new disposable pen then the current reusable pen, or vice versa. The pen being used was switched at visit 3 and rhGH treatment was continuous; there was no washout period (see Figure 1). All participants were trained by the site coordinators on the proper use of each of the pens prior to actual use. The study was conducted between August 2010 and October 2011 at 23 centers in seven countries (the Czech Republic, Germany, the Netherlands, Slovakia, Sweden, Turkey, and the UK). Four additional centers in Germany, the Netherlands, and the UK were shipped study supplies but did not enroll any participants. All eligible participants were randomly assigned to treatment order using a central interactive voice response (IVR) system. The randomization sequence was stratified by study site to minimize any bias related to an interaction of order and site.
 | Figure 1 Study design. |
Eligible participants were treatment-naïve (ie, they had never been treated with rhGH) children and adults ≥4 years of age. Adults and children diagnosed with GHD and children diagnosed as small for gestational age (SGA) or with Ullrich-Turner syndrome were eligible to participate. Those with other conditions such as Prader–Willi syndrome or those with chronic renal insufficiency or chronic systemic disorders were excluded from the study. Moreover, no patients who had previously participated in any somatropin pen development research or had participated in any interventional clinical studies in the prior 30 days were eligible to participate.
Recruited participants were included into one of three groups: 1) the caregiver group, which consisted of the parent or adult caregiver of patients 4–7 years of age; 2) the dyad group, which comprised patients 8–17 years of age and their parent or adult caregiver; and 3) the adult group, which included all patients ≥18 years of age.
The IPAQ measure
The IPAQ is a validated, multi-item measure of ease-of-use and preference based on 13 unique features or characteristics of injection pens.5 The IPAQ is divided into two sections (Section I and Section II). Section I allows respondents to provide objective assessments on 13 ease-of-use items for each of the individual pens and a single item on overall pen ease-of-use. Section II provides a comparative measure of injection pen ease-of-use on the 13 items, an item for measuring comparative overall ease-of-use, and an overall measure of preference for a total of 43 responses per patient or patient dyads over the 4-month study observation period.
A 5-point scale was used for responses to the ease-of-use items and the overall measure of ease-of-use (ranging from very easy to very difficult, with somewhat easy, neither easy nor difficult, and somewhat difficult as the interim response categories).5 The comparative measures were scored on a 3-point categorical scale, allowing the caregiver/patient/patient dyads to indicate which pen was easier to use on the 13 items and the overall ease-of-use item, and to indicate which pen they preferred overall. A response of indifference was included in the event the caregiver/patient/patient dyads found the pens to be equivalent on that particular item or dimension.
The IPAQ was originally designed to evaluate dyad (patient plus his/her caregiver) perception of the convenience of (as determined by ease-of-use) and preference for the new disposable versus the current reusable injection pen in a US population. The items were derived from a series of focus groups of growth hormone injection pen users, were evaluated with additional dyads using a standard cognitive debriefing approach, and were subsequently field-tested in a small group of injection pen users for clarity and completeness. The IPAQ was then used in a prospective clinical trial of 136 treatment-experienced child/parent dyads in the US, demonstrating good operating characteristics and psychometric properties.5 The IPAQ was recently adapted to assess ease-of-use and preference by adult patients (either caregivers treating younger children or self-treating adults) in five European countries. Linguistic translation and cultural adaptation was achieved through the standard protocol.6 A series of cognitive debriefing interviews of injection pen users was conducted in each study country to ensure that the translated measures had the requisite content for use by adults assessing ease-of-use as partner or self-administration users. The results of the cognitive debrief along with a review of the operating characteristics of the new language versions of the IPAQ using these trial data support the content and construct validity of the IPAQ.7
Other endpoints
Prior to the initiation of this study, the new disposable somatropin pen was commercially available in some, but not all, countries included in this study. In addition to IPAQ-observed ease-of-use and preference, in those countries where choice of continued therapy was possible, physicians were asked to record which device the patient selected. Safety data were collected using standard safety assessments at day 7 by telephone (visit 2 and visit 4 in Figure 1) and at each visit in both sequences by the clinician through direct questioning of the patient and/or their caregiver.
Study conduct
This study was conducted in compliance with the ethical principles originating in or derived from the Declaration of Helsinki and with all International Conference on Harmonisation Good Clinical Practice guidelines. The protocol was reviewed and approved by a properly constituted ethics committee in each of the countries. In addition, all local regulatory requirements were followed; in particular, those affording greater protection to the safety of study participants. No data safety monitoring board was required or instituted for this study.
A signed and dated informed consent was required before any screen procedures were initiated. The investigators explained the nature, purpose, and risks associated with the study to each patient. Each participant was informed that he/she could withdraw from the study at any time and for any reason. Each participant was given sufficient time to consider the implications of the study before deciding whether to participate. Those who chose to participate signed an informed consent document. Children were offered an assent form as appropriate, based on age and ability to assent as determined by the relevant institutional review board/ethics committee and implemented by the investigator in accordance with local requirements. Children between the ages 7 and 10 years provided verbal assent, those between 11 and 16 years provided written assent unless deemed infeasible, providing oral assent as an alternative, and those aged 17 and 18 years provided assent on the informed consent document along with the parent or guardian. All assents were witnessed and documented according to local requirements.
Since the activity of preparing and injecting a dose is typically a shared activity in the 8–17 years of age group, the dyad group completed the questionnaires with the caregiver and the child answering a single questionnaire in collaboration. Parents or adult caregivers provided their assessment of ease-of-use for the 4–7 years of age caregiver group and patients in the adult group provided their assessment themselves. Questions about the dyad demographics were collected: 1) the respondent relationship; 2) who oversaw the dose preparation and administration; and 3) confirmation that the same dyad completed the IPAQ at visit 3 (end of treatment [EoT] sequence 1) and visit 5 (EoT sequence 2), or the reason for the dyad being different if this were the case. It took about 5–10 minutes to complete each of the three assessments. The two Section I assessments were completed at the conclusion of each user experience (visits 3 and 5) to evaluate participants’ experiences with the pen that they had just used, and the Section II comparative assessment was completed at the conclusion of the study (visit 5). Sites were instructed to have all the individual assessments completed at the beginning of the office visits and to have Section II assessments completed at the very end of the final visit.
Statistical analysis
The sample size was based on question 1 of Section II of the IPAQ, according to overall ease-of-use question. Planned recruitment was a minimum of 100 participants and a maximum of 130 participants, with target completion of between 92 and 120 evaluable participants. A two-sided 95% confidence interval (CI) was constructed based on the proportion of participants for whom the new disposable somatropin pen was as easy or easier to use compared with the current reusable somatropin pen. This proportion of participants was predicted to be between 65% and 80% in favor of the new disposable somatropin pen, with associated 95% CIs. For example, if at the end of the study 84 of 120 (70%) evaluable participants reported the ease-of-use of the new somatropin pen to be no different from or easier to use than the current reusable somatropin pen, the estimated 95% CI would be 61.8–78.2. If the true underlying rate is 65%, the study has 83% power that the two-sided confidence interval for the proportion of subjects indicating the new pen as easy or easier to use does not include 50%.
All participants who were randomized and used a study pen at least once to administer somatropin were included in the full analysis set (FAS). No extrapolation or imputation was used for missing data.
The primary endpoint of the study, defined a priori, was the proportion of participants who either reported the new disposable somatropin pen to be easier to use or reported no difference compared with the current reusable somatropin pen. The 95% CI for this proportion was presented. The categories of “no difference” and new somatropin pen “easier to use” were collapsed into a single category to reflect the clinical implications of a change in therapy. Previously, evaluations of the current device both in field testing as well as a large clinical study support that the current device is easy or very easy to use by the majority of patients. In this study, the primary analysis was defined to ensure that use of the new device would not reduce the ease-of-use experience when patients are prescribed somatropin. Additional secondary endpoints included pen preference, ease-of-use by pen type, and pen choice at the end of treatment all expressed as proportions and calculated from both Section I and Section II responses.
Percentages were calculated from the number of participants evaluable at the time point of interest. The IPAQ Section I 5-point scale items, all scored as for question 1 (ease-of-use), were summarized using the summary statistics of mean, median, and standard deviation (SD). All key IPAQ data were summarized overall, by respondent type (adult, dyad, and caregiver), and by pen sequence. For the key binary outcomes, a two-sided 95% CI for the proportion was generated using the normal distribution approximation to the binomial distribution. The binomial test, again using the normal distribution approximation to the binomial distribution, was used to analyze choice of pen.
Additional exploratory analyses were performed using stepwise logistic regression models8 to explore the relationship between ease-of-use and such possible factors as treatment sequence, sex, region (Eastern or Western Europe), and responder type.
The IPAQ Section I ease-of-use question was analyzed using a nonparametric crossover technique, applying the Wilcoxon signed-rank test to the difference between periods for effect of treatment9 and 95% CI using the Hodges–Lehmann estimator.10
Results
Overall, 120 participants were randomized to treatment and received at least one dose of study medication. All 120 participants completed the study. Of the 120 participants enrolled, usable data on the study endpoints were obtained from all 120 participants, although data were available for 119 participants only for the primary endpoint.
Demographic and baseline characteristics
The characteristics of the study population are illustrated in Table 1. Of the 120 participants in the study, 42 (35.0%) were adults (defined as patients ≥18 years of age); 50 (41.7%) were child and caregiver pairs (ie, dyads, defined as a patient 8–17 years of age and his/her parent/caregiver); and 28 (23.3%) were <8 years of age and being treated by a parent or other caregiver (the caregiver group). The mean (SD) age of the entire sample was 21.7 (19.0) years, with a range of 4–72 years of age. The mean (SD) age of the participants by group is presented in Table 1 as well. More than half of all participants were male (69 of 120; 57.5%) and most were white (116 of 120; 96.7%). In general, the mothers of the 78 combined dyad and caregiver groups reported being the most commonly responsible for the preparation of the device and for administering the injection. Regarding completion of the questionnaire, approximately half were completed by both parent and child, whereas about half were completed by the parent only. Of the 51 female participants, six (11.8%) were of childbearing potential. Of the 120 participants, 92 (76.7%) had a diagnosis of GHD; the mean duration since diagnosis was 9.5 months. A total of 23 patients (19.2%) had a diagnosis of SGA; the mean duration since diagnosis was 16.0 months. Five patients (4.2%) had a diagnosis of Turner’s syndrome; the mean duration since diagnosis was 5.1 months. Of the 80 patients (66.7%) with a concomitant medical condition, the most common comorbidity was hypopituitarism (30 patients; 25.0%). All other conditions were reported in <10% of the participants.
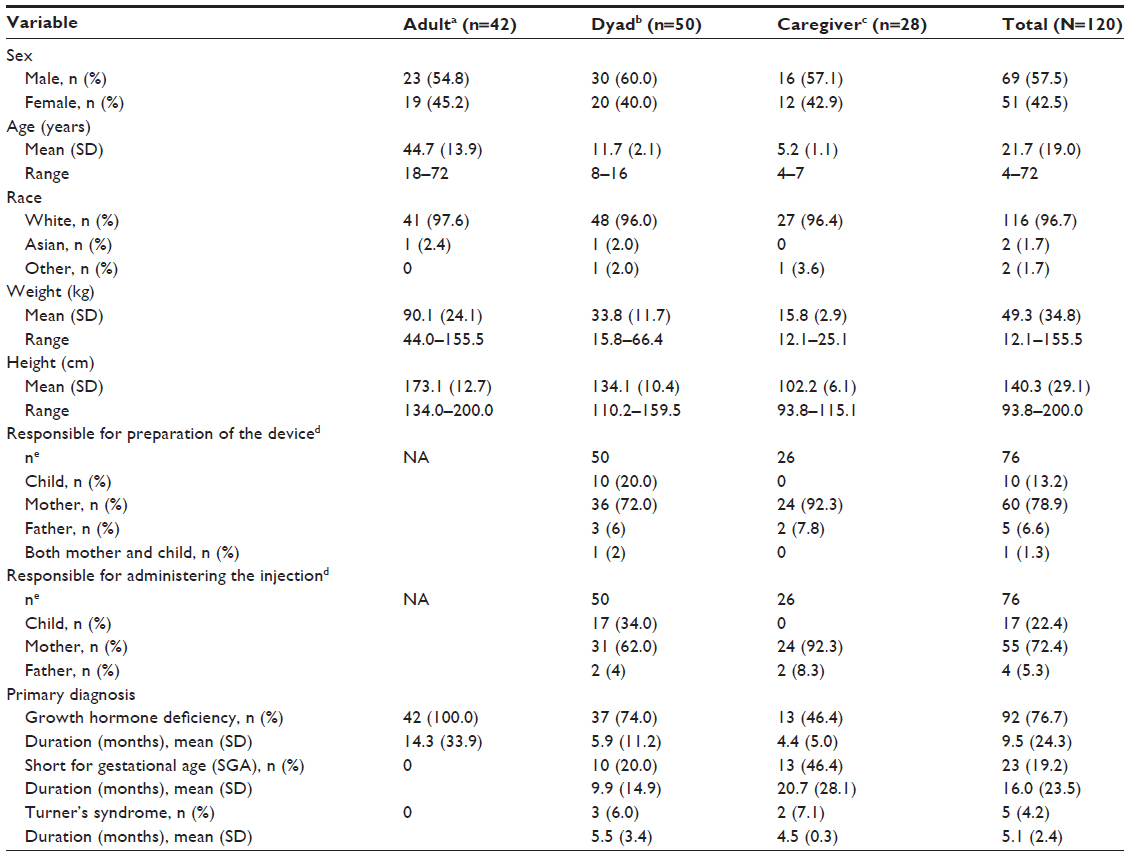 | Table 1 Summary of demographic variables by respondent type |
Ease-of-use and pen preference
For the primary endpoint of overall ease-of-use, 80 participants (67.2%; 95% CI: 58.8–75.7) either reported no difference or found the new disposable somatropin pen to be easier to use (Table 2). For the endpoint of overall preference, 77 participants (64.2%; 95% CI: 55.6–72.8) either had no preference or preferred the new disposable somatropin pen. Preferences for pen attributes as defined by individual items are reported in Table 3.
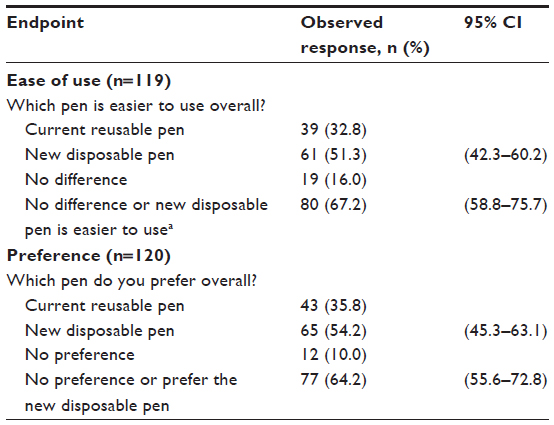 | Table 2 IPAQ Section II response: overall ease of use and preference |
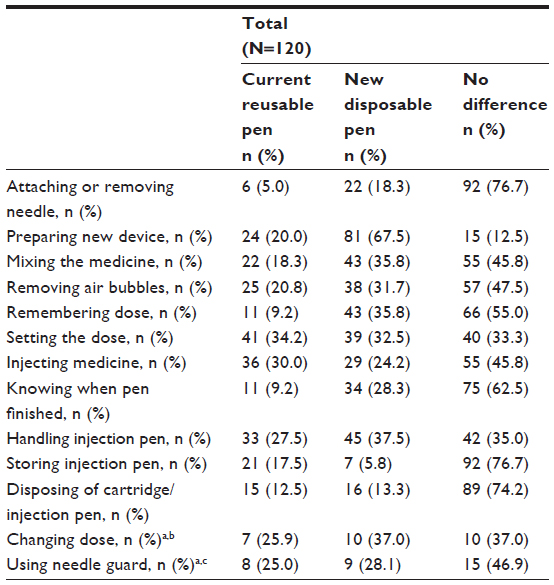 | Table 3 Summary of IPAQ Section II individual item response (easier to use) |
Comparison of ease-of-use between the new disposable somatropin pen and the current reusable somatropin pen by respondent type and pen sequence also was summarized (Table 4). The percentage of participants who either reported no difference or found the new disposable somatropin pen to be easier to use was 63.0% (95% CI: 44.8–81.2) for caregivers treating children <8 years of age, 60.0% (95% CI: 46.4–73.6) for dyads, and 78.6% (95% CI: 66.2–91.0) for self-treating adults. Similarly, the percentage of participants who reported the new disposable somatropin pen to be easier to use was 51.9% (95% CI: 33.0–70.7) for caregivers treating children <8 years of age, 48.0% (95% CI: 34.2–61.9) for dyads, and 54.8% (95% CI: 39.7%–69.8%) for self-treating adults.
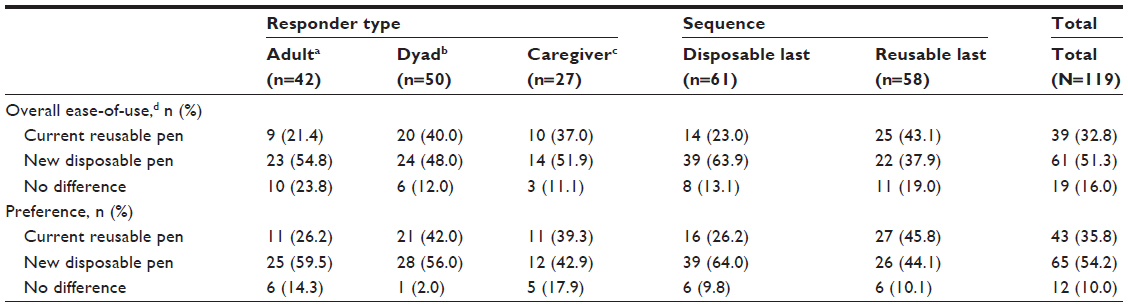 | Table 4 IPAQ overall ease of use and preference by respondent type and sequence |
A summary, according to respondent type and pen sequence, of the comparison of preference for the new disposable somatropin pen versus the current reusable somatropin pen also is presented in Table 4. The percentage of participants who had no preference or preferred the new disposable somatropin pen was 60.8% (95% CI: 42.6–78.8) for caregivers treating children <8 years of age, 58.0% (95% CI: 44.3–71.7) for dyads, and 73.8% (95% CI: 60.5–87.1) for self-treating adults. The percentage of participants who preferred the new disposable somatropin pen was 42.9% (95% CI: 24.5–61.2) for caregivers treating children <8 years of age, 56.0% (95% CI: 42.2–69.8) for dyads, and 59.5% (95% CI: 44.7–74.4) for self-treating adults.
Logistic regression modeling on the overall ease-of-use question indicated that treatment sequence was strongly associated with ease-of-use, with participants 2.54 times more likely to indicate the new disposable pen as the last pen they used (95% CI: 1.15–5.61) as easier to use. Patient demographics (age, sex, country) and group assignment (caregiver, dyad, adult) were also assessed for potential association with ease-of-use and none were evident. The secondary endpoints for this study included the following: 1) IPAQ Section I and Section II item level responses; 2) ease-of-use score; and 3) the device chosen for treatment continuation when the choice exists.
The mean overall ease-of-use score of the IPAQ Section I responses for FAS score was 4.2 (SD: 0.71) for the reusable somatropin pen and 4.5 (SD: 0.64) for the new disposable somatropin pen (P=0.0029). A greater number of participants found the new disposable somatropin pen to be very easy or somewhat easy to use compared with the current reusable somatropin pen (114 [95.8%] and 104 [87.4%] participants, respectively). In general, a greater percentage of participants, based on individual Section I responses, found the new disposable somatropin pen to be very easy or somewhat easy to use compared with the current reusable somatropin pen (see Figure 2).
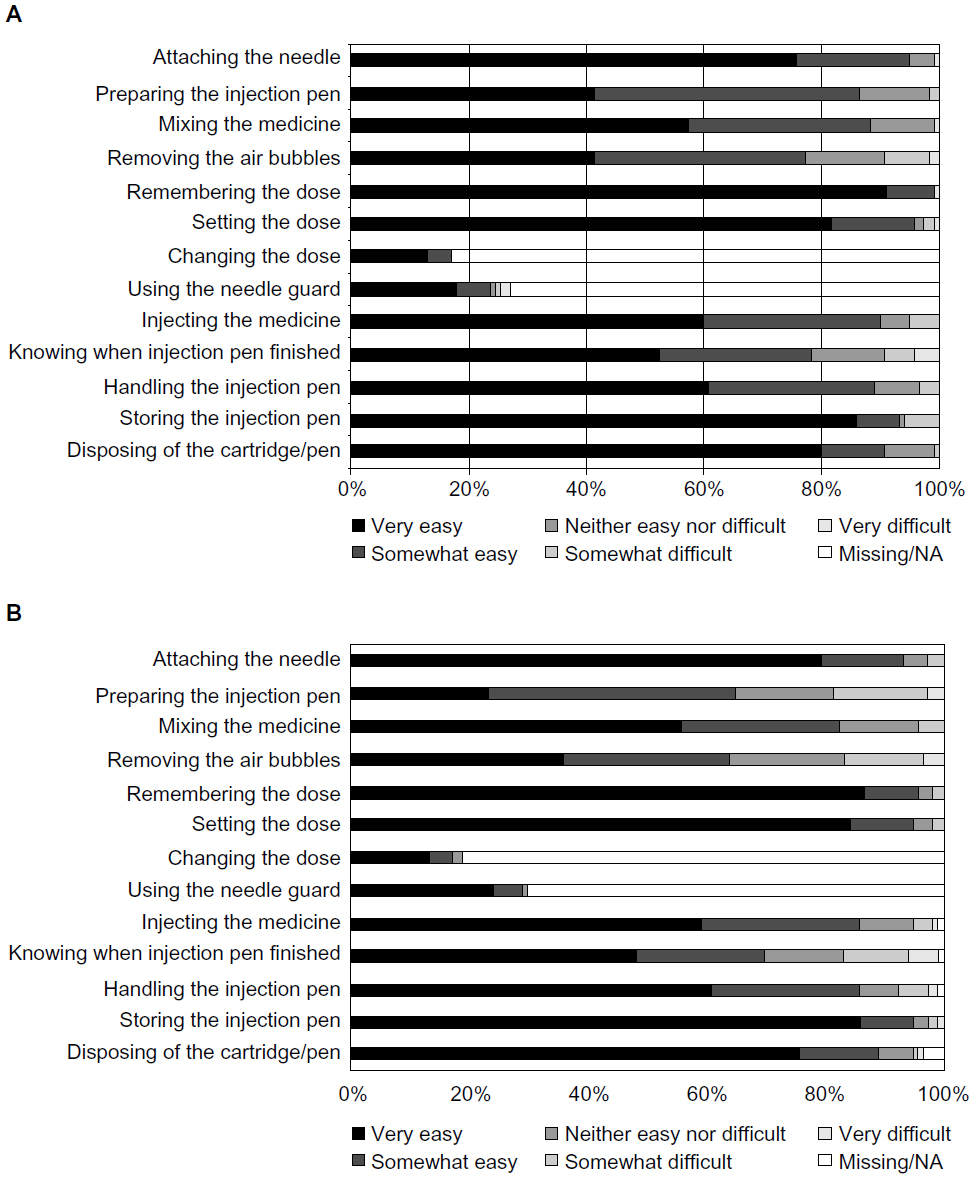 | Figure 2 Bar chart of IPAQ Section I item responses for (A) the new disposable somatropin pen and (B) the current reusable somatropin pen. |
Overall choice by respondent type, and by sequence
A summary of the device chosen for treatment continuation in the FAS was created (Table 5). This question was only completed by participants in countries where the new disposable device was commercially available. Of the 55 participants evaluated, 26 (47.3%) selected the new disposable somatropin pen and 29 (52.7%) selected the current reusable somatropin pen; the difference was not statistically significant (P=0.6858). This information also was presented by respondent type: for caregivers treating children <8 years of age and dyads, a greater percentage of participants selected the current reusable somatropin pen (73.3%; 95% CI: 50.9–95.7 and 63.2%; 95% CI: 41.5–84.9, respectively). For self-treating adults, 71.4% (95% CI: 52.1–90.7) selected the new disposable somatropin pen. This information also was summarized according to treatment sequence group. For both sequences, a greater percentage of participants selected the last device used as the method for treatment continuation.
 | Table 5 Choice of pen by respondent type and sequence |
Device-related adverse events
There were no reports of significant device failures due to errors. Of the eight reported device-related adverse events (in five patients), none were serious and seven of the eight were injection-site–related, with four of these classified as injection-site pain, and one each classified as injection site injury, injection site hematoma, and injection site reaction. The eighth adverse event reported was related to the patient self-injecting an incorrect dose because of failure of the current reusable pen. Overall, device-related adverse events were relatively evenly distributed across pen types with three reported during the disposable pen use period and five during the reusable pen period.
Discussion
Based on the physiology of endogenous growth hormone secretion, the accepted way to administer exogenous rhGH is subcutaneously daily in the evening in children as well as in adults. In the past, attention has focused on the development of easy-to-use injection devices.2 The selection of a device based on its features and the ultimate user experience associated with that choice can impact adherence and therapeutic outcomes.11 Devices that are easier to use can improve a patient’s ability and willingness to comply with treatment. It has been reported that the choice of an adequate drug delivery device is associated with greater patient compliance and improved clinical outcomes.12,13
The multidose reusable somatropin pen was introduced in 1995 and has high acceptance rates among both caregivers and patients alike. Based on responses to a questionnaire, 95% of patients surveyed preferred the reusable somatropin pen to the prestudy device, KabiPen (Pharmacia, Stockholm, Sweden), based on various reasons such as a greater certainty of correct dosing with the digital display, the possibility of correcting the set dose, and the lock function of the injection button when the injection is complete.14 In 2003, a reusable somatropin pen (Genotropin; Pfizer, Inc., New York, NY) was compared with a needle-free system, the Genotropin ZipTip® (Pfizer Inc., New York, NY). In this 2-week, two-period pediatric crossover study, over 50% of the 117 completing subjects reported no difference in bleeding, pain, soreness, or bruising, and about 20% (n=26) continued with the Genotropin ZipTip at the conclusion of the study.15
In an effort to further improve design and ease-of-use, a new disposable somatropin injection pen was developed. In this study, we asked treatment-naïve patients to try two different somatropin injection pens and to assess the ease-of-use of each one. The results provide an interesting insight into the characteristics previously identified as relevant to patients when evaluating overall ease-of-use of injection pens.
When evaluated individually, both pens were rated as easy or very easy to use overall by >90% of respondents. On the 5-point ease-of-use scale, the new pen scored slightly higher (4.5 [SD: 0.64] versus 4.2 [SD: 0.71] with the old device), which was statistically significant (P=0.0029). This suggests that regardless of which pen is selected, no significant barriers to the use of either device in treatment-naïve patients exist. At the item level, a consistent trend suggests that the differentiating features of the new pen make it easier to use. In the small number of participants who used the needle guard, some found the old version easier to use. The lower score on ease-of-use of the needle guard may have been associated with the difficulty experienced by three of the 32 users. Improved training on the use of the needle guard might be instrumental in ensuring that when that device is used, it is used correctly and without difficulty.
In the analysis, the data suggest that an order effect may have been present when identifying the pen that is easier to use or preferred. There was a higher likelihood that a participant would select the last pen in the sequence, which is a type of recency effect or possibly a learning effect. Since all of the participants were treatment-naïve, it may have become easier to manage injecting after 2 months of practice, even if they were using a slightly different device. In the US study in which participants had significant prior experience and randomization to order was not possible, the loyalty effect was minimal.9 This supports the suggestion about an order effect, but there is no direct measure of the effect; thus, it should be considered for future investigation.
Adults self-administering tended to have a preference for the new pen over the older device. Since the new pen is lighter and perhaps more easily manipulated with one hand, self-administration was less complicated for these patients. In addition, as adult doses tend to be lower than doses for children, the more refined dose increments with the new disposable pen may have influenced ease-of-use and preference.
As discussed above, the literature reinforces the fact that an association exists between ease-of-use and compliance with therapy. The argument that improved pen features and easier-to-use devices may impact patient outcomes, unfortunately, was not testable in this short study. In the trial, pen compliance was measured by pen counts and demonstrated good overall compliance regardless of pen type. This is as expected in a clinical trial. How this translates into the medical population is unclear and further assessments of the relationship between pen features and compliance outcomes are warranted.
In contrast to the 2-month study that was conducted in the US in which participants’ previous experience with the reusable pen served as the comparison,4 in the European study, the ratings with respect to the new disposable pen being no different from or easier to use than the reusable pen were lower when compared to the US study results (67.2% vs 73.7%) while preference (no different from or preferable to the reusable pen) was about the same (64.2% and 65.2%, respectively).
Although the target population in the European study differed from that in the US study, the absolute scores on the objective measures (items and overall ease-of-use) did not differ dramatically between the populations studied. In each of the studies, both pens performed well on the various scales and little difficulty was experienced by the participants. As with the treatment-experienced patients evaluated previously in the US study, the treatment-naïve patients in this study reported a high degree of ease with both pens. It appears that the pen instructions provided are sufficient and appropriate, given the low complexity of each pen.
Device-related adverse events were generally minimal and infrequent, with only eight reported in both treatment arms, three related to the use of the disposable pen and five related to the use of the current reusable pen. At the item level, the simplification of the preparation step in the new pen emerged as a visible and valued improvement. Other features related to dose and dose memory were not consistently regarded as improvements, although in no case were any of the features other than the needle guard considered to be detrimental to the ease-of-use of the new pen over the old version. The European data show that the reusable somatropin pen had already achieved a high level of quality; however, the improvements to the disposable somatropin pen were well recognized.
In a recent study by Kappelgaard16 in Japanese children, the investigators used an in-clinic usability test comparing two injection devices. Fuchs17 used a similar methodology in a small pilot study in children. In another study18 with a design similar to the previous somatropin study by Hey-Hedavi et al,4 the investigators used a prospective design and compared prior injection experience with the experience of using a new pen over a 6-week in-home use. This design is an improvement in terms of generalizability though it represents only use-experienced children. In their report, it is unclear what the prior use experience included, though there is a suggestion that it was variable across rhGH injection devices.
In contrast, this study was conducted in a real-world setting in a crossover format including treatment-naïve children and adults. Additionally, the assessment of outcome used a novel dyadic approach reflective of how growth hormone is typically used by patients and their caregivers, with an instrument with demonstrated validity. This design allows an opportunity to generalize to this group of patients.
Limitations
As with any study, there are limitations to the generalizability of the results. First and foremost, the sample size of the current study was restricted, and given the three distinct subgroups (parents, dyads, and adults), the CIs reported were somewhat exaggerated. When the results of this study are evaluated in combination with those of the US study, the data are reasonably reflective of what one might expect in clinical practice, especially given the fact that this was a true patient-use study as opposed to a contrived handling study.
The patient choice endpoint was not measurable in some countries due to the unavailability of the disposable pen at the time of the study. In the case where choice was an option, there was no cost differential to the patient, though one should be cautious in generalizing this to situations when cost is a factor in product selection.
Data were collected directly from participants at defined time points, which relied on patient self-reports over a 2-month period of user experience with each device. The amount of missing data was minimal and no imputation was required. The only significant amount of missing data was for the needle guard and dose change items on the scale, since many of the participants did not experience those features.
The study did not include any clinical outcomes, such as growth or growth velocity, as the duration of the trial was too short and nor was that the intent of the study. It would be unlikely that use of the two pens could result in dissimilar clinical outcomes due to therapeutic differences, as both pens contain the exact same drug substance in the exact same dose and strength. Any differences in outcome would be related to exogenous factors such as compliance differences.
Conclusion
The features of injection devices for rhGH have been evolving over the years. The original vial and syringe methods have been replaced with ever-increasing simplicity and patient-friendly approaches. Accordingly, both pens tested were rated as easy or very easy to use overall by >90% of respondents, with the new pen scoring slightly higher on the overall ease-of-use question. Our data show that the reusable somatropin pen had already attained a high level of ease-of-use for an injection device. In the current study, the small but recognizable enhancements of the new disposable somatropin pen were realized by both patients and their caregivers. Given the current high degree of ease reported, we may be reaching the upper limit in our ability to enhance the way in which daily injections are provided to patients who require treatment with growth hormone. Based on the recent published research, however, recent innovations in pen design to improve usability are shown to be recognized and favored by growth hormone patients. As such, continued innovation in these technologies may benefit patients and assessing their impact on outcomes is encouraged.
Acknowledgments
The authors thank all the physicians, site staff, children, their caregivers, and adult patients who participated in the study.
Disclosure
This study was funded by Pfizer Inc. At the time of this study, Dr Pleil and Dr Wollmann were full-time employees of Pfizer. Dr Darendeliler received a research grant from Pfizer for the conduct of this study and has served as a speaker for Pfizer Inc., Novo Nordisk, and Merck Serono. Dr Dörr has received research grants from Pfizer Inc., and has served as a speaker for Pfizer Inc., Novo Nordisk, Merck Serono, Ipsen, and Ferring. Ms Hutchinson is a full-time employee of Quanticate, which received payment from Pfizer for the statistical analysis and reporting for this study. The authors have indicated that they have no other conflicts of interest with regard to the content of this article. Dr Darendeliler and Dr Dörr received no compensation for the development of this manuscript.
Editorial assistance for the development of this manuscript was provided by Linda Wychowski, PhD, of Engage Scientific Solutions, Southport, CT, USA, and was funded by Pfizer.
References
Genotropin prescribing information. New York, NY: Pfizer Inc. 2011. Available at: http://www.genotropin.com/misc/prescribing-information.aspx. Accessed on June 2, 2013. | |
Finkelstein BS, Imperiale TF, Speroff T, Marrero U, Radcliffe DJ, Cuttler L. Effect of growth hormone therapy on height in children with idiopathic short stature: a meta-analysis. Arch Pediatr Adolesc Med. 2002;156:230–240. | |
Dumas H, Panayiotopoulos P, Parker D, Pongpairoichana V. Understanding and meeting the needs of those using growth hormone injection devices. BMC Endocr Disord. 2006;6:5. | |
Hey-Hadavi J, Pleil A, Deeb LC, et al. Ease of use and preference for a new disposable self-injection pen compared with a reusable pen for administering recombinant human growth hormone: A multicenter, 2-month, single-arm, open-label clinical trial in patient-caregiver dyads. Clin Ther. 2010;32:2036–2047. | |
Pleil AM, Kimel M, McCormack J, Rajicic N, Hey-Hadavi J. Psychometric assessment of the Injection Pen Assessment Questionnaire (IPAQ): measuring ease of use and preference with injection pens for human growth hormone. Health Qual Life Outcomes. 2012;10:126. | |
Wild D, Grove A, Martin M, et al. ISPOR Task Force for Translation and Cultural Adaptation. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR Task Force for Translation and Cultural Adaptation. Value Health. 2005;8:94–104. | |
Pleil A, Kimel M, Wollmann H. The adaptation of the Injection Pen Assessment Questionnaire for use in Europe – validation results from a large multicenter study of recombinant human growth hormone treatment naïve children and adults, November 2012 (poster presentation), ISPOR 15th Annual European Congress, Berlin, Germany. | |
Hodges JL, Lehmann EL. Estimates of location based on rank tests. Ann Math Statist. 1963;34:598–611. | |
Agresti A. Categorical Data Analysis. Hoboken, NJ: Wiley 2002. | |
Senn S. Cross-Over Trials in Clinical Research. 2nd ed. Hoboken, NJ: Wiley; 2002. | |
Fidotti E. A history of growth hormone injection devices. J Pediatr Endocrinol Metab. 2001;14:497–501. | |
Müller J, Skakkebæk NE, Jacobsen BB, et al. Norditropin® SimpleXx™: a liquid human growth hormone formulation, a pen system and an auto-insertion device. Horm Res. 1999;51(Suppl 3):109–112. | |
Rapaport R, Saenger P, Schmidt H, et al. Validation and ease of use of a new pen device for self-administration of recombinant human growth hormone: results from a two-center usability study. Med Devices (Auckl). 2013;6:141–146. | |
Sjöblom K, Albertsson-Wikland K, Bengtsson BA, et al. Patient evaluation of a new injection pen for growth hormone treatment in children and adults. Acta Paediatr Suppl. 1995;411:63–65. | |
Dorr HG, Zabransky S, Keller E, et al. Are needle-free injections a useful alternative for growth hormone therapy in children? Safety and pharmacokinetics of growth hormone delivered by a new needle-free injection device compared to a fine gauge needle. J Pediatr Endocrinol Metab. 2003;16:383–392. | |
Kappelgaard AM, Mikkelsen S, Knudsen TK, Fuchs GS. Patient preference for a new growth hormone injection device: results of an open-label study in Japanese pediatric patients. J Pediatr Endocrinol Metab. 2011;24(7–8):489–496. | |
Fuchs GS, Mikkelsen S, Knudsen TK, Kappelgaard AM. Ease of use and acceptability of a new pen device for the administration of growth hormone therapy in pediatric patients: an open-label, uncontrolled usability test. Clin Ther. 2009;31(12):2906–2914. | |
Tauber M, Jaquet D, Jesuran-Perelroizen M, Petrus M, Bertrand A, Coutant R. User assessment of Norditropin NordiFlex®, a new prefilled growth hormone pen: a Phase IV multicenter prospective study. Patient Prefer Adherence. 2013;7:455–462. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.