Back to Journals » Clinical Interventions in Aging » Volume 14
Relationship Between Potentially Inappropriate Medications And The Risk Of Hospital Readmission And Death In Hospitalized Older Patients
Authors Wang P ![]() , Wang Q, Li F, Bian M, Yang K
, Wang Q, Li F, Bian M, Yang K
Received 9 June 2019
Accepted for publication 2 October 2019
Published 4 November 2019 Volume 2019:14 Pages 1871—1878
DOI https://doi.org/10.2147/CIA.S218849
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Peng Wang,1 Qing Wang,1 Fang Li,1 Meng Bian,2 Kun Yang3
1Department of Geriatrics, Fuxing Hospital, The Eighth Clinical Medical College, Capital Medical University, Beijing, People’s Republic of China; 2Department of Pharmacy, Fuxing Hospital, The Eighth Clinical Medical College, Capital Medical University, Beijing, People’s Republic of China; 3Centre for Evidence-Based Medicine, Xuanwu Hospital Capital Medical University, Beijing, People’s Republic of China
Correspondence: Qing Wang
Department of Geriatrics, Fuxing Hospital, The Eighth Clinical Medical College, Capital Medical University, 14 Fuwai street, Beijing 100038, People’s Republic of China
Email [email protected]
Objective: This study aimed to compare the prevalence of potentially inappropriate medications (PIMs) among hospitalized elderly patients using Beers and Chinese criteria and identify the correlation between PIMs and the risk of hospital readmission and death.
Methods: This study was conducted on geriatric patients aged ≥65 years at Beijing Fuxing Hospital between June 2015 and December 2017. The Beers criteria of 2015 and the Chinese criteria of 2017 were used to detect PIMs. Follow-ups were conducted for 12–36 months (or until patients’ death, if it came sooner). Cox proportional-hazards models were used to explore the correlations between PIM use and the risk of hospital readmission and death.
Results: Of 508 patients, 352 (69.3%) and 339 (66.7%) had at least one PIM identified using the Beers criteria and the Chinese criteria, respectively. Proton-pump inhibitors in the Beers criteria and clopidogrel in the Chinese criteria were the most leading PIMs. PIMs identified using the Beers criteria were a risk factor for the all-cause hospital readmission. After adjusting for age, gender, comorbidity, and so forth, PIM use was still an indicator of rehospitalization. PIM grouping defined using the Chinese criteria was not associated with hospital readmission. PIM grouping defined using either criteria was not associated with all-cause death.
Conclusion: The study showed a high prevalence of PIM use in China. PIMs defined using the Beers criteria increased the risk of hospital readmission. Clinicians should pay more attention to PIMs, carry out routine PIM assessment, and reduce adverse health outcomes in elderly patients.
Keywords: Beers criteria, Chinese criteria, death, elderly, potentially inappropriate medication, readmission
Introduction
Some medications are more likely to cause adverse reactions among elderly patients due to the special pharmacokinetics and pharmacodynamics of these patients.1 Sometimes, the adverse consequences of medications even overwhelm the benefits of treatment. To deal with this problem, the United States proposed the concept of the use of potentially inappropriate medications (PIMs) in the elderly patients in 1991 and established Beers criteria,2 which were revised four times until 2015.3 The US studies showed that PIM use among elderly patients was 42.6–49.0%,4,5 and patients taking PIMs had an increased incidence of adverse drug events, emergency, and readmission to hospital.6,7 The risk of hospital admission for patients taking more than three PIMs at the same time was 1.6 times that of patients taking no PIMs.8 In China, studies based on the Beers criteria showed that PIM use in elderly inpatients was 53.5%–72.4%,9–11 which was significantly higher than that in foreign countries. However, most of these studies were cross-sectional ones, with few observations about the correlation between PIM use and readmission to hospital or death. Moreover, China developed its PIM diagnostic criteria relatively late. The Chinese PIM list for the elderly was established in 2015 and revised in 2017.12 Based on the Chinese list, the percentage of PIM use among inpatients and the correlation of PIM use defined using the Beers and Chinese criteria with patients’ readmission to hospital and all-cause death need further exploration.
Methods
Patients
This prospective cohort study involved 508 elderly patients hospitalized in the Comprehensive Department of Fuxing Hospital affiliated to the Capital Medical University between June 2015 and December 2017. The inclusion criteria were as follows: patients aged 65 years and above and those who could complete the evaluation. The exclusion criteria were as follows: patients taking no medication or irregular medication; patients having severe and terminal illnesses with a short life expectancy; and bedridden patients.
The Beers criteria of 2015 and the 2017 criteria of PIMs for older adults in China (the Chinese criteria of 2017) were used to identify and measure PIM use.3,12 Patients were divided into a PIM group and a non-PIM group depending on their use of PIMs. During the follow-up observation, those who stopped PIM use and those who started taking PIMs were excluded from the PIM group and the non-PIM group, respectively.
The study was approved by the ethics committee of Fuxing Hospital (affiliated to the Capital Medical University) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants included in the study.
Data Collection
Data included age, sex, body mass index (BMI), comorbidities, prescribed drugs, length of stay, and the Charlson Comorbidity Index (CCI) calculated for each patient.
The functional status for residents was assessed using Katz activities of daily living (ADL).14 This scale reflected the dependence on six primary functions: bathing, dressing, toileting, continence, walking, and eating. The scores of this scale ranged from 0 (independence) to 6 (high dependence).
Patients’ cognitive status was assessed using the Chinese version of the Mini-Mental State Examination (CMMSE),15 which had a maximum score of 30 points. The scores were grouped according to patient’s education level: illiteracy, ≤17 points; primary school, ≤20 points; and secondary school and above, ≤24 points.
Patients’ current diagnosis for which they received medications was classified using the International Classification of Diseases-10 (ICD10). Comorbidity was quantified using the CCI.16
The Clinical Frailty Scale (CFS) scores were determined by a trained medical professional according to the Canadian Study of Health and Aging grading criteria.17 The CFS ranged from 1 (very fit) to 9 (terminally ill). The CFS results were categorized into five groups as follows: non-frail (CFS 1–3), vulnerable (CFS 4), mildly frail (CFS 5), moderately frail (CFS 6), and severely frail (CFS ≥7).
For the nutrition screening tool, a short-form mini-nutritional assessment (MNA-SF) was used, which covered six items: (1) food intake and appetite in the last 3 months; (2) changes in body weight and physique in the last 3 months; (3) mobility; (4) acute illness or psychological trauma in the last 3 months; (5) mental and psychological problems; and (6) BMI. The scores for each item ranged from 0 to 2 or 3 points. The maximum score was 14 points. The total scores were grouped as follows: normal nutritional status (12–14 points); risk of malnutrition (8–11 points); and malnutrition (0–7 points).18
End Point
A follow-up was conducted every 3 months through phone calls or home visits by the follow-up group after discharge. The outcome was all-cause hospital readmission and death.
Statistical Analysis
Statistical analysis was performed using the SAS (Version 9.2; SAS Institute Inc., NC, USA) software package. (1) Baseline data were described by mean ± standard deviation, or median (interquartile range), whereas qualitative data were described by the ratio or composition ratio. The baseline characteristics of the two groups were compared using the independent sample t-test, Wilcoxon rank-sum test, or chi-square test according to the type of data. (2) The concordance between the two PIM criteria was calculated using kappa tests (value of kappa.0.75 indicated good-to-excellent agreement; values between 0.40 and 0.75 indicated moderate agreement; value 0.40 indicated poor agreement). (3) Cox proportional-hazards regression model was used to analyze the correlation between PIM groups and elderly patients’ readmission to hospital and death while adjusting relevant influencing factors.
Results
Demographics Of Participants
Table 1 describes the characteristics of the study population. A total of 508 participants aged 65 years or older were included in the present study. The average age was 84.2 ± 5.9 years (ranging from 65 to 100 years), and 312 (61.4%) patients were male.
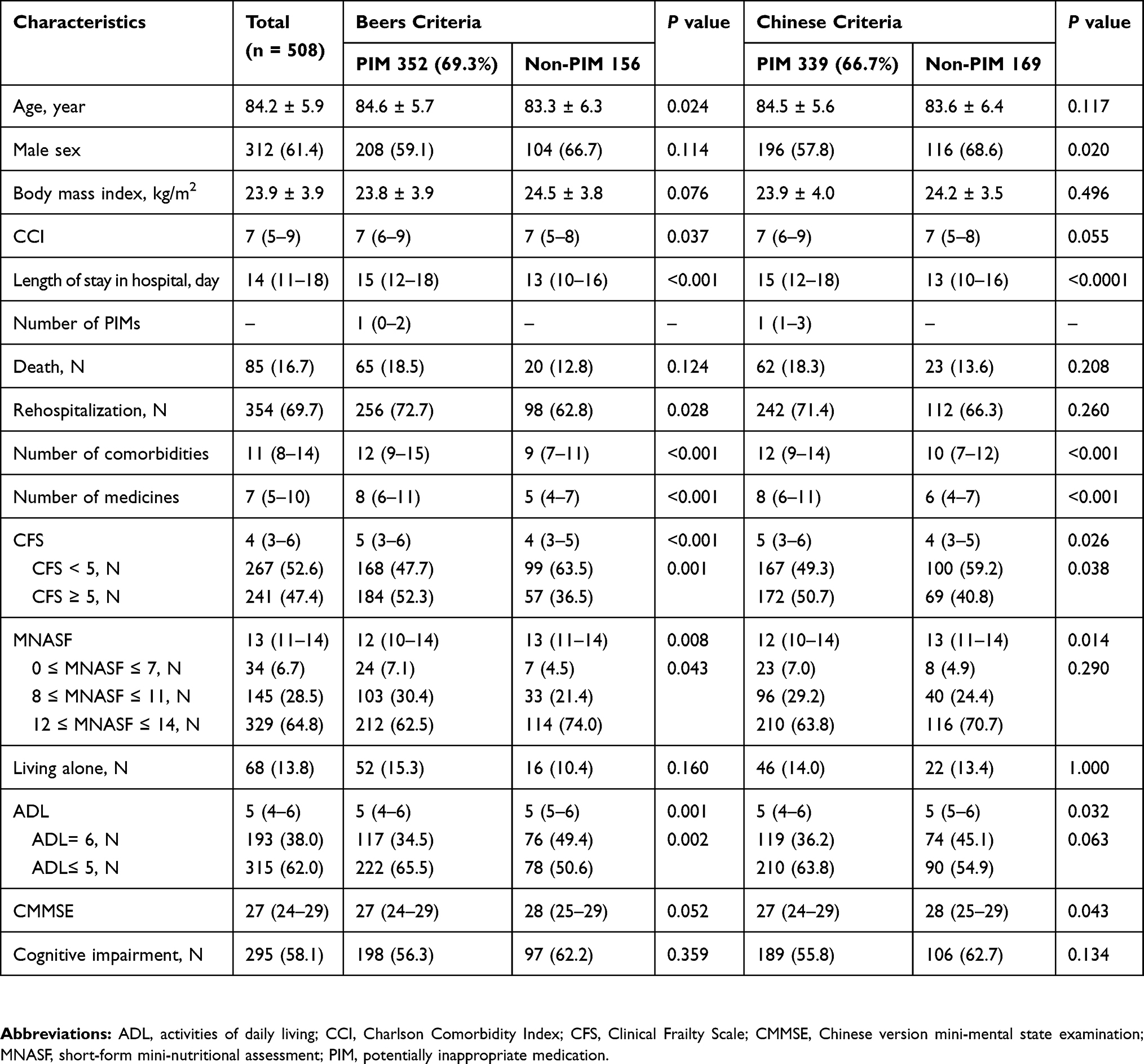 |
Table 1 Baseline And Clinical Characteristics Identified Using The Beers Criteria And Chinese Criteria |
A total of 315 patients (62.01%) had ADL = 6, indicating complete independence. Further, 267 patents (52.6%) were defined as frail using the CFS. Also, 329 patients (64.8%) had a normal nutritional status, 145 patients (28.5%) had risks of malnutrition, and 34 patients (6.7%) had malnutrition. Moreover, 295 patients (58.1%) had a cognitive impairment, and 68 patients (13.8%) lived alone. The median (IQR) CCI points, prescribed medications, and length of hospital stay were 7 points (IQR 7–9), 11 (IQR 8–14), and 14 days (IQR 11–18), respectively. Further, 85 patients (16.7%) died during the follow-up visits, and 354 (69.7%) were readmitted to hospital for all causes.
PIM Use
Beers Criteria Of 2015 Versus Chinese Criteria Of 2017
Clear differences were found between the PIM group and the non-PIM group defined using the two criteria in terms of length of stay in hospital, discharged diagnosis of diseases, number of drugs admitted, and full independence in ADL.
According to the Beers criteria of 2015, the PIM group exhibited significant differences in age (P = 0.024), malnutrition (P = 0.043), and CCI points (P = 0.037) compared with the non-PIM group.
According to the Chinese criteria 2017, the PIM group exhibited significant differences in sex (P = 0.020) and cognitive impairment (P = 0.043) compared with the non-PIM group.
The detection rate of PIMs using the Chinese criteria of 2017 and the Beers criteria of 2015 was 66.7% (339/508) and 69.3% (352/508), respectively. The median number of PIMs per person identified using the Chinese criteria and the Beers criteria was 1 (0–2) and 1 (1–3), respectively (Table 1).
The kappa statistic for Beers and Chinese criteria was κ = 0.444, indicating a moderate coherence (Table 2 and Figure 1).
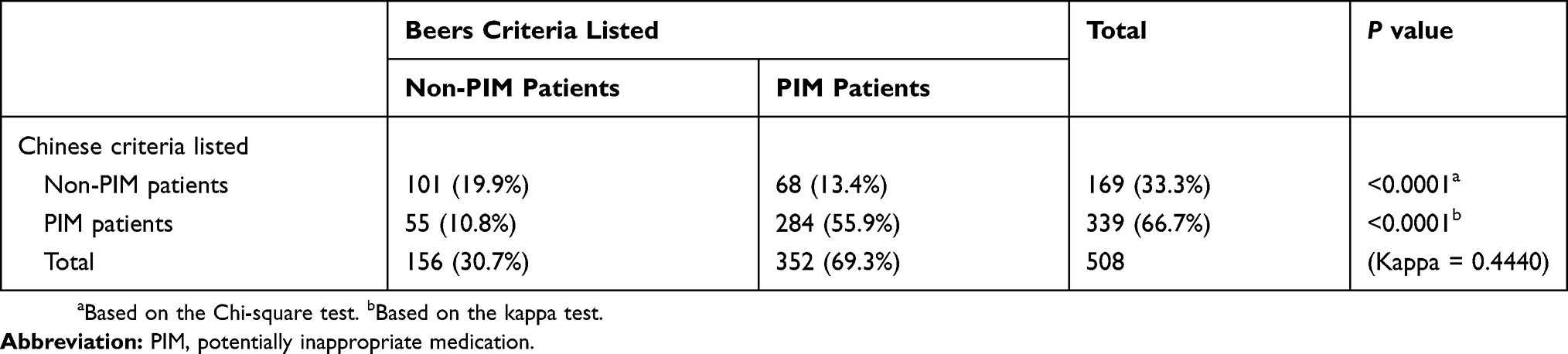 |
Table 2 Beers And Chinese Criteria Concordance |
 |
Figure 1 Beers and Chinese criteria concordance. |
Table 3 lists the top 10 PIMs recognized using the 2 criteria. In the Beers criteria, proton-pump inhibitors (PPIs) (42.6%, 150/352) accounted for the most frequent PIMs. In contrast, the most frequent PIM according to the Chinese criteria was clopidogrel (50.1%, 170/339). Estazolam ranked second in both the Beers criteria (34.4%, 121/352) and the Chinese criteria (35.7%, 121/339) (Table 3).
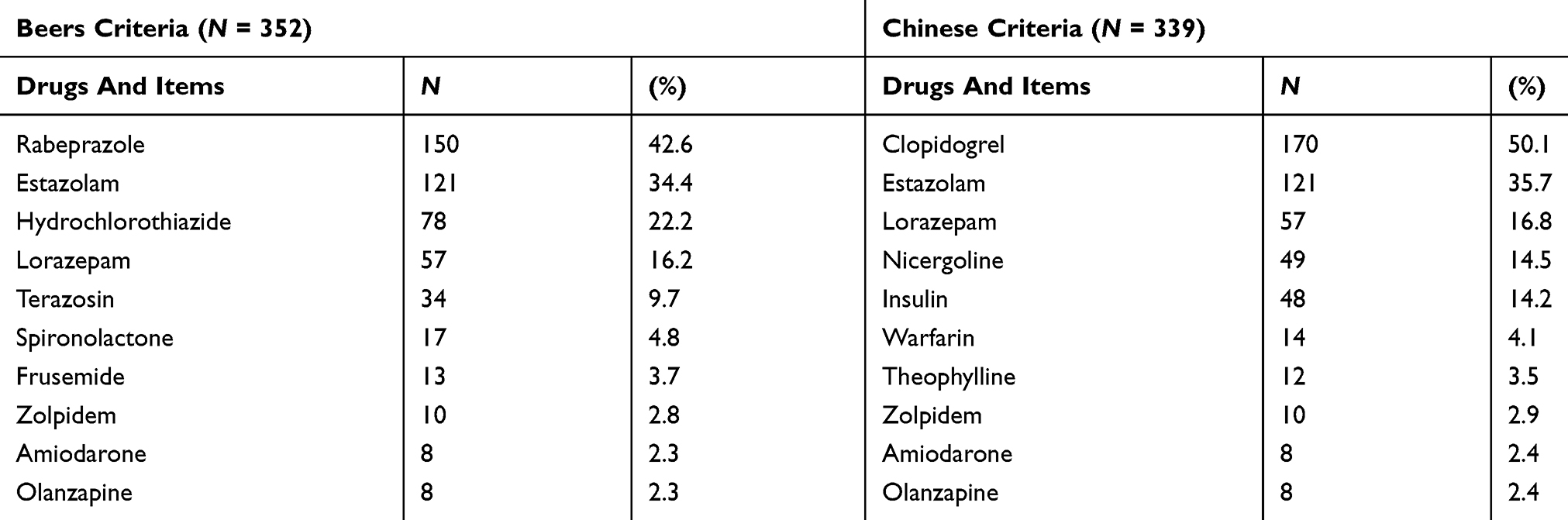 |
Table 3 Top 10 PIMs Based On The Two Sets Of PIM Criteria |
PIMs According To The Beers Criteria Of 2015 As A Predictor Of Hospital Admission
After 12–36 months of follow-up visits (with a median of 23 months), 85 (16.7%) all-cause deaths and 354 (69.7%) admissions to hospital were identified in the cohort.
Rehospitalization was compared using the Kaplan–Meier curve among the PIM groups determined based on the two criteria. As shown in Figure 2, the PIM group defined using the Beers criteria had a higher proportion of rehospitalization compared with the non-PIM group, and the log rank test result was significant (72.7% vs 62.8%, P = 0.006). No significant difference was observed in the PIM group defined using the Chinese criteria. No difference in the mortality rate was found among the groups defined using both criteria (Figure 2). The clinical outcomes were analyzed using the Cox regression model. In the Beers criteria, the risk of rehospitalization in the PIM group was 1.37 times higher than that in the non-PIM group. After adjusting for factors such as age, sex, Charlson’s index, BMI, duration, number of medicines, living alone, independence in ADL, and cognitive impairment, PIM use was still an indicator of rehospitalization risk (HR: 1.31, 95% CI: 1.03–1.66, P = 0.025). However, PIM use was not associated with all-cause death. The PIM group defined using the Chinese criteria was not associated with all-cause death and hospital readmission (Table 4).
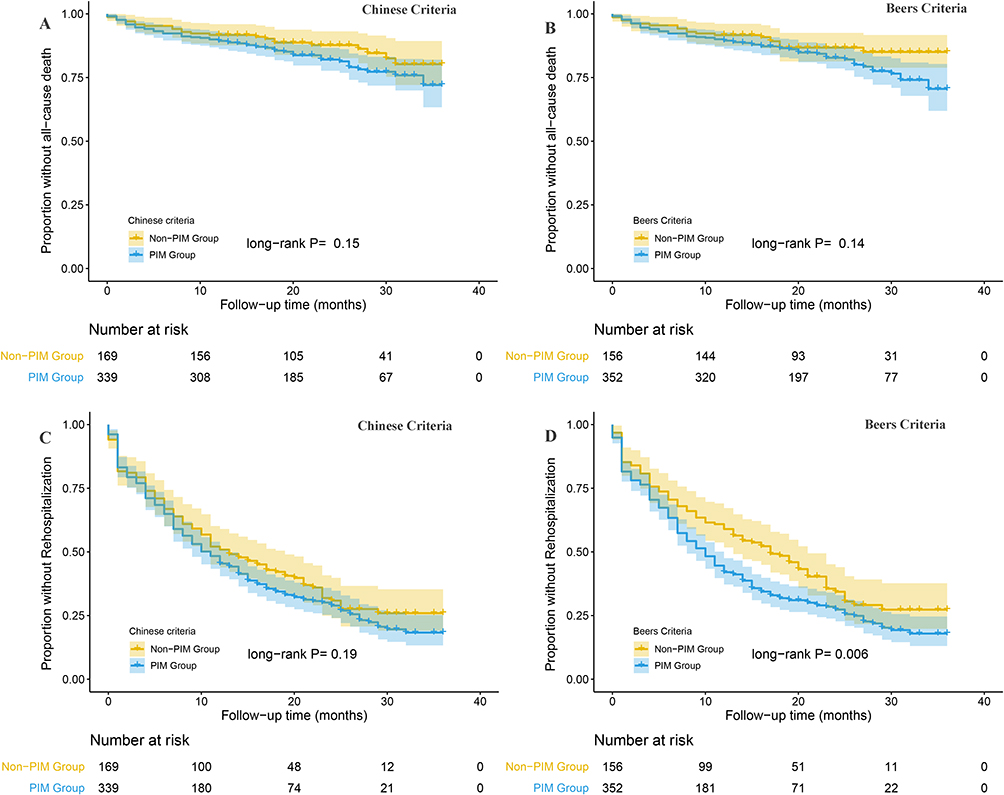 |
Figure 2 Kaplan–Meier curves comparing PIM and non- PIM groups according to Beers and Chinese criteria with health outcomes. Notes: (A) PIM group according to Chinese criteria and death. (B) PIM group according to Beers criteria and death. (C) PIM group according to Chinese criteria and readmission. (D) PIM group according to Beers criteria and readmission. |
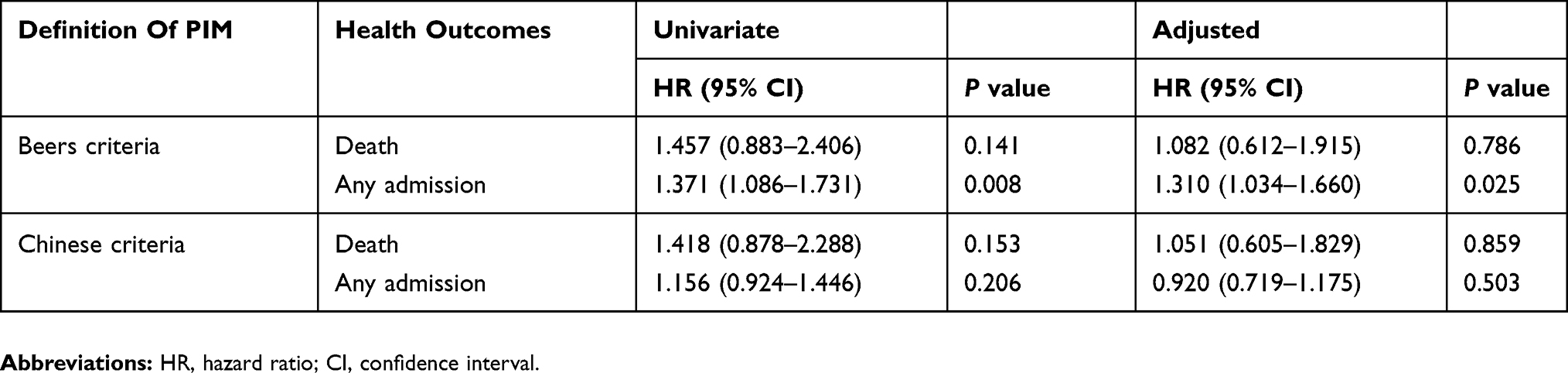 |
Table 4 Univariate And Multivariate Cox Proportional-Hazards Models To Determine The Association Of PIM Use With Health Outcomes |
Discussion
With the advent of an aging society, people have started paying increasing attention to rational medication use among elderly patients. Based on the Beers criteria, this study found that PIM use among elderly inpatients in China was 69.3%, which was similar to the findings of other studies (53.5%–72.4%).9–11 Based on the Chinese elderly PIM list, PIM use among elderly inpatients in China was 66.7%, which was at the same level as the findings based on the Beers criteria. The results based on the two criteria had a moderate coherence. China’s domestic studies, which were based on the Chinese criteria, showed detection rates of PIMs as 58.5%–80.2%.19–22 Whether it is the Chinese criteria or the Beers criteria, PIM use in China, as revealed by related studies, is higher than that in the United States and Europe (18.6–39.2%), as identified using the Beers criteria and local criteria.8,23 The substantially higher PIM use among elderly inpatients in China, compared with foreign countries, had two reasons. First, the concept of PIM use was not introduced to China for a long time, and the Chinese criteria have been established recently. Also, the understanding of PIMs among Chinese doctors is insufficient, and the use of PIM criteria to guide clinical work is not satisfactory. Second, it is believed that doctors are not solely responsible for PIM use; the elderly patients are more prone to PIM use because of their age, comorbidity, frailty, and other factors.1,8,24 Moreover, relevant studies on PIM use and adverse clinical outcomes are lacking. The present study was performed to address these issues.
Regarding the correlation between PIMs and adverse clinical outcomes, some studies showed that PIMs increased the risk of hospital readmission.1,13 This study found similar results on PIMs defined using the Beers criteria: the risk of hospital readmission for the group of patients taking PIMs was 1.3 times higher than that for the non-PIM group (HR: 1.37, 95% CI: 1.09–1.73, P = 0.008). Many factors increase the risk of readmission, such as age, severity of disease, drugs, nutritional status, and so forth. PIM use was one of the risk factors for readmission after adjusting for the aforementioned factors in the Cox regression analysis. The hazard ratio of PIM use for readmission was 1.37–1.31, confirming that PIM use increased the risk of readmission among elderly patients. However, regarding PIMs defined using the Chinese criteria, no significant difference was found between the PIM and the non-PIM groups in terms of the risk of hospital readmission. The different impacts of the two criteria on hospital readmission were associated with the different types of medications in the two lists. The top two PIMs detected using the Beers criteria were PPIs (42.6%) (150/352) and estazolam (34.4%) (121/352). According to the Beers criteria, PPIs could increase the risk of fracture in elderly patients.
An Australian prospective cohort study detected a significant correlation between the PPI use and falls in older women at high risk of falls. In the analysis, PPI therapy for the duration of at least 1 year was associated with an increased risk of fracture-related hospitalizations [adjusted odds ratio (OR) = 2.17; 95% confidence interval (CI): 1.25–3.77]. In the replication study, long-term PPI therapy (>1-year duration) was associated with an increased risk of self-reported falls (adjusted OR = 1.51; 95% CI: 1.00–2.27, P = 0.049) after adjusting for fall risk factors and vitamin D therapy.25 Some other studies also showed that the prolonged use of PPIs led to vitamin B12 deficiency and triggered peripheral neuropathy,26,27 increasing the risk of falls.28 A major risk of estazolam, as a PIM, is fall.3 A European study showed that the most common diagnoses for PIM-caused hospital readmission included falls and syncope.23 The top two medications detected using the Beers criteria were associated with a higher risk of falls and hospital readmission. The top two medications detected using the Chinese list were clopidogrel (50.1%, 170/339) and estazolam (35.7%, 121/339). A major risk of clopidogrel, as a PIM, is adverse hematological reactions, such as thrombocytopenia and gastrointestinal bleeding,12 which have less impact on hospital readmission compared with medications associated with a higher risk of falls. Although one of the top two PIMs detected using the Chinese criteria was estazolam, increased clopidogrel use in the PIM group relatively diluted the proportion of other medications associated with a higher risk of hospitalization. This explained why only the PIM group defined using the Beers criteria was associated with hospital readmission in this study. Therefore, the Beers criteria seemed to be more instructive for clinical work compared with the Chinese criteria and was more likely to direct clinicians’ attention to PIMs. The Chinese PIM list, which was updated only once since its launch in 2015, still has room for improvement, if compared with the Beers criteria revised multiple times.
This study showed that PIM grouping, whether it was based on the Beers criteria or the Chinese PIM list, was not associated with all-cause death. The result, which was consistent with the findings of other studies,29 also can be attributed to two reasons. First, patients with increased PIM use are often patients with multiple diseases. PIM use may not lead to patient death, but it may lead to increased readmission or decreased quality of life. Second, the sample size of the present study was small, and the follow-up time was relatively short. Moreover, this study was a single-center study, and hence the patients could not represent the whole Chinese elderly population. Therefore, multi-center PIM studies should be conducted in the future to reveal the adverse effects of PIM use in the elderly population in China. The results of this study suggested that PIM use was associated with readmission and not death. However, some studies showed that PIM use was related to death. The findings of the present study and related studies suggested that the assessment of PIM use was an important part of clinical work to reduce the occurrence of clinical adverse events. However, PIM use has not been popularized and promoted in China. Many clinicians do not realize that PIM use may increase the risk of adverse health events in elderly patients. A cross-sectional study was conducted on 372 elderly inpatients with an average age of 84.3 ± 6.5 years. The logistic regression analysis showed that the type of medications prescribed by doctors was a risk factor for PIM use, compared with the comorbidity, disability, and frailty of elderly patients (OR = 1.594, 95% CI: 1.411–1.800, P < 0.001).19 Therefore, clinicians’ attention to PIMs remains the key to PIM use. The ultimate purpose of this study was to make clinicians realize that PIM use might increase the risk of adverse health events. In fact, the findings also supported the correlation between PIM use and adverse clinical outcomes. The clinicians should be aware of the increase in the risk of adverse events associated with PIM use and should carry out routine PIM assessment, thus strengthening the rational use of medications, minimizing the amount of prescription medicines if possible, and avoiding PIM use.
This study had its own limitations. First, this was a single-center study. Multi-center studies with a large sample size may better reflect the influence of PIMs on adverse health events among the elderly patients in China. Second, the Chinese PIM list classifies medications as high risk and low risk. The study might have produced more significant results if the observations were based on these two levels.
In conclusion, the prevalence of PIM use is high among elderly inpatients in China. PIMs defined using the Beers criteria increase the risk of hospital readmission; however, PIMs defined using the Beers criteria and the Chinese criteria are not associated with all-cause death. Clinicians should pay more attention to PIMs, strengthen the rational use of medications, and reduce adverse health outcomes in patients.
Author Contributions
PW and QW conceived and designed the study. KY, FL and MB were involved in data acquisition and statistical analysis. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Beer C, Hyde Z, Osvaldo P, et al. Quality use of medicines and health outcomes among a cohort of community dwelling older men: anobservational study. Br J Clin Pharmacol. 2011;71(4):592–599. doi:10.1111/j.1365-2125.2010.03875.x
2. Beers MH, Ouslander JG, Rollingher I, Reuben DB, Brooks J, Beck JC. Explicit criteria for determining inappropriate medication use in nursing home residents. UCLA division of geriatric medicine. Arch Intern Med. 1991;151(9):1825–1832.
3. American Geriatrics Society 2015 Beers Criteria Update Expert Panel. American geriatrics society 2015 updated beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2015;63(11):2227–2246. doi:10.1111/jgs.13702
4. Davidoff A, Miller E, Sarpong E, et al. Prevalence of potentially inappropriate medication use in older adults using the 2012 Beers Criteria. J Am Geriatr Soc. 2015;63:486–500. doi:10.1111/jgs.13320
5. Rothberg MB, Pekow PS, Liu F, et al. Potentially inappropriate medication use in hospitalized elders. J Hosp Med. 2008;3(2):91–102. doi:10.1002/jhm.290
6. Petrarca AM, Lengel AJ, Mangan MN. Inappropriate medication use in the elderly. Consult Pharm. 2012;27(8):583–586. doi:10.4140/TCP.n.2012.583
7. Fick DM, Mion LC, Beers MH, et al. Health outcomes associated with potentially inappropriate medication use in older adults. Res Nurs Health. 2008;31(1):42–51. doi:10.1002/nur.20232
8. Reich O, Rosemann T, Rapold R, et al. Potentially inappropriate medication use in older patients in swiss managed care plans: prevalence, determinants and association with hospitali zation. PLoS One. 2014;8(9):e10542. doi:10.1371/journal.pone.0078827
9. Zhang X, Zhou S, Pan K, et al. Potentially inappropriate medications in hospitallized older patients: a cross-sectional study using the Beers 2015 criteria versus the 2012 criteria. Clin Interv Aging. 2017;12:1697–1703. doi:10.2147/CIA.S146009
10. Mo L, Yang X, He J, Dong B. Evaluation of potentially inappropriate medications in older inpatients in China. J Am Geriatr Soc. 2014;62(11):2216–2218. doi:10.1111/jgs.13118
11. Li H, Pu S, Liu Q, et al. Potentially inappropriate medications in Chinese older adults: the Beers criteria compared with the screening tool of older persons’ prescriptions criteria. Geriatr Gerontol Int. 2017;17(11):1951–1958. doi:10.1111/ggi.12999
12. Rational Drug Use Branch of Chinese Association of Geriatric. Criteria of potentially inappropriate medications for older adults in China. Adverse Drug React J. 2018;20(1):2–8.
13. Ritt M, Ritt JI, Sieber CC, Gaßmann KG. Comparing the predictive accuracy of frailty, comorbidity, and disability for mortality: a 1-year follow-up in patients hospitalized in geriatric wards. Clin Interv Aging. 2017;12:293–304. doi:10.2147/CIA.S124342
14. Katz S, Downs TD, Cash HR, Grotz RC. Progress in development of the index of ADL. Gerontologist. 1970;10(1):20–30. doi:10.1093/geront/10.1_part_1.20
15. Cui GH, Yao YH, Xu RF, et al. Cognitive impairment using education-based cutoff points for CMMSE scores in elderly Chinese people of agricultural and rural Shanghai China. Acta Neurol Scand. 2011;124(6):361–367. doi:10.1111/j.1600-0404.2010.01484.x. Epub 2011 Feb 9. PubMed PMID: 21303351.
16. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245–1251. doi:10.1016/0895-4356(94)90129-5
17. Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173:489–495. doi:10.1503/cmaj.050051
18. Cameron EJ, Bowles SK, Marshall EG, Andrew MK. Falls and long-term care: a report from the care by design observational cohort study. BMC Fam Pract. 2018;19(1):73. doi:10.1186/s12875-018-0787-5
19. Peng W, Qing W, Yun-Jing C, et al. Association between potentially inappropriate medication and comorbidity, frailty and disability in the hospitalized elderly patients. Chin J Mult Organ Dis Elderly. 2018;17(11):820–824.
20. Peng W, Meng B, Qing W, et al. Association of potentially inappropriate medications with falls in elderly patients. Chin J Mult Organ Dis Elderly. 2019;18(2):117–121.
21. Rong D, Zhen-Xiang L. Evaluaton of portential inappropriate medication in hospitalized elderly patients based on two criteria. Chin Hops Pharm J. 2017;37(19):1979–1982.
22. Ma Z, Zhang C, Cui X, et al. Comparison of three criteria for potentially inappropriate medications in Chinese older adults. Clin Interv Aging. 2018;14:65–72. doi:10.2147/CIA.S190983
23. Kersten H, Hvidsten LT, Gløersen G, et al. Clinical impact of potentially inappropriate medications during hospitalization of acutely ill older patients with multimorbidity. Scand J Prim Health Care. 2015;33(4):243–251. doi:10.3109/02813432.2015.1084766
24. Herr M, Sirven N, Grondin H, et al. Frailty, polypharmacy, and potentially inappropriate medications in old people: findings in a representative sample of the French population. J Clin Pharmacol. 2017;73(9):1165–1172. doi:10.1007/s00228-017-2276-5
25. Lewis J, Barre D, Zhu K, et al. Long-term proton pump inhibitor therapy and falls and fractures in elderly women: a prospective cohort study. J Bone Miner Res. 2014;29:2489–2497. doi:10.1002/jbmr.2279
26. Dharmarajan TS, Kanagala MR, Murakonda P, Lebelt AS, Norkus EP. Do acid-lowering agents affect vitamin B12 status in older adults? J Am Med Dir Assoc. 2008;9(3):162–167. doi:10.1016/j.jamda.2007.10.004
27. Valuck RJ, Ruscin JM. A case-control study on adverse effects: H2 blocker or proton pump inhibitor use and risk of vitamin B12 deficiency in older adults. J Clin Epidemiol. 2004;57(4):422–428. doi:10.1016/j.jclinepi.2003.08.015
28. Elaine W, Yu SR, Bauer PA. Bain, Proton pump inhibitors and risk of fractures: a meta-analysis of 11 international studies. Am J Med. 2011;124(6):519–526. doi:10.1016/j.amjmed.2011.01.007
29. Barnett K. Prevalence and outcomes of use of potentially inappropriate medicines in older people: cohort study stratified by residence in nursing home or in the community. BMJ Qual Saf. 2011;20(3):275–281. doi:10.1136/bmjqs.2009.039818
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.