Back to Journals » Research Reports in Clinical Cardiology » Volume 11
Relationship Between Isovolumic Acceleration (IVA) and TEI Index with Pro-BNP in Heart Failure
Authors Shahlaee S, Alimi H, Poorzand H, Morovatdar N, Vakilian F, Shahlaee S
Received 25 May 2020
Accepted for publication 4 November 2020
Published 18 November 2020 Volume 2020:11 Pages 57—63
DOI https://doi.org/10.2147/RRCC.S253688
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Kones
Shokufeh Shahlaee,1 Hedieh Alimi,2 Hoorak Poorzand,3 Negar Morovatdar,1 Farveh Vakilian,4 Shirin Shahlaee5
1Department of Cardiology, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran; 2Vascular and Endovascular Surgery Research Center, Quaem Hospital, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran; 3Vascular and Endovascular Surgery Research Center, Imam Reza Hospital, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran; 4Clinical Research Unit, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran; 5Nuclear Medicine Department, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
Correspondence: Hedieh Alimi
Vascular and Endovascular Surgery Research Center, Quaem Hospital, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
Tel +98 9155145632
Email [email protected]
Background: Heart failure (HF) is a common disorder and leads to many costs for the healthcare system. Brain natriuretic peptide (BNP) is a cardiac neurohormone and has an important function in diagnosis and prognosis of left ventricular (LV) dysfunction. The TEI index is a novel non-invasive Doppler-based indicator, which evaluates systolic and diastolic myocardial function. There are few data regarding the prognostic role of TEI and isovolumic acceleration (IVA) indexes in HF and the relationship with neurohormonal activation. In this study, we evaluated the TEI and IVA index correlation with Pro-BNP in patients with systolic HF.
Patients and Methods: This was a cross-sectional study. We included consecutively patients with HF, admitted to Imam Reza Hospital, Mashhad, Iran between March 2017 and February 2019. A single investigator would perform echocardiography the next morning, for all patients. A checklist was completed for each patient and included demographic data, clinical data and different echocardiographic variables. We also recorded in-hospital mortality and outcome of patients during the follow-up stage.
Results: We finally included 65 patients according to inclusion and exclusion criteria. The mean age of participants was 63.38± 12.85 years. Most of them were male (61.5%). We showed that there is a direct and significant relationship between RVIVA (r=0.317, P=0.010) and LVIVA (r=0.254, P=0.041) with LVEF. There was no significant correlation between Pro-BNP level and NYHA classification (r=0.151, P=0.231). We showed that there was no correlation between Pro-BNP level and RV TEI index (r=0.065, P=0.490) and LV TEI index (r=0.071, P=0.419). In sub-group analysis, in patients with EF< 20%, we showed a significant correlation between the level of Pro-BNP and RV TEI index.
Conclusion: We showed that the IVA index is correlated to EF in both RV and LV and can differ in large-scale in a population study. We also showed that RV TEI index is significantly correlated with Pro-BNP in patients with EF< 20%. Large-scale studies are recommended.
Keywords: left ventricular heart failure, LVHF, brain natriuretic peptide, BNP, TEI index, isovolumic acceleration, IVA
Introduction
Heart failure is a common rising complex, clinical syndrome and worldwide disorder, and makes many costs for the healthcare system in both developing and developed countries.1,2 Left ventricular systolic dysfunction (LVSD)-associated heart failure is characterized by neurohormonal activation3 and is associated with high morbidity and mortality.4 Ejection fraction is one of the most important prognostic factors in heart failure. However, it can be affected specially in elderly patients.5
Brain natriuretic peptide (BNP) is a cardiac neurohormone, released by ventricles toward the enormous stretching ventricle myocytes. It may be co-released from some atrial granules.6,7 BNP has a diagnostic and prognostic role in LV dysfunction with various causes.8 NT-pro BNP is released in a proportion equivalent to BNP. According to longer NT-pro BNP half-life, it seems to be more sensitive than BNP.9 BNP plasma levels increase in abnormal conditions, leading to RV pressure or volume overload.10
Another novel non-invasive Doppler-derived indicator is the TEI index. It includes both systolic and diastolic myocardial function.11 It is determined with the summation of the isovolumic contraction time (ICT) and the isovolumic relaxation time (IRT) divided by the ejection time (ET). It is independent from heart rate and blood pressure, and could be acquired in simple and repeatable acquisition and characterized by a low interobserver and intraobserver variability.12,13
It has been demonstrated that the TEI index can be helpful for assessment of overall ventricular performance and is a separate predictor for cardiovascular mortality in patients with amyloidosis,14 idiopathic dilated cardiomyopathy15 and primary pulmonary hypertension.16
Myocardial acceleration during isovolumic contraction (IVA) and isovolumic contraction myocardial velocity (IVV) are indexes which are less influenced by the loading status. So, they can estimate left and right ventricular functions in a relatively load-independent route.17 Estimation of contractility by myocardial acceleration within the isovolumic contraction period is a more sensitive method than a tissue Doppler imaging (TDI)-derived peak systolic velocity method.18 Recently, an investigation in patients with mitral stenosis demonstrated that IVA was a good predictor of RV systolic dysfunction.19
Despite many researches in patients with HF, there are limited data about the predictive value of TEI and IVA indexes and the relationship with neurohormonal activation. In this study, we evaluated the TEI and IVA index correlation with Pro-BNP in patients with systolic HF.
Patients and Methods
Population
In this cross-sectional investigation, we enrolled consecutively patients with HF, admitted to Imam Reza Hospital, Mashhad, Iran during March 2017 and February 2019.
We included patients with systolic HF, ejection fraction lesser than 40%, sinus rhythm and good view in echocardiographic evaluation. To increase our investigation power, we excluded patients with significant cardiac valvular disorders equal to or more than moderate degree stenosis or regurgitation, liver and pulmonary failure, acute coronary artery syndrome, history of revascularization within 3 months before admission, chronic obstructive pulmonary disease (COPD), consumption of drugs like diuretics, angiotensin converting enzyme inhibitors (ACEi), angiotensin II receptor blockers (ARBs), beta-blockers, spironolactone or digoxin. The diagnosis of HF was according to the past medical history, physical exam and electrocardiographic and echocardiographic assessments.
Ethics
This investigation was approved by the ethical committee of Mashhad University of Medical Sciences with code IR.MUMS.fm.REC.1396.453. All patients completed informed written consent before enrolment.
Echocardiographic Assessment
Echocardiography was done by a single user the next morning after the hospital admission to eliminate the bias related to circadian change. An Ultrasound Philips EPIQ 7 echocardiography tool with a 3.25-MHz probe was used. Three to five heart cycles were saved and echocardiography was done at admission, 3 months and 6 months later.
Two-Dimensional Echocardiography
LV diameters were determined according to the American Society of Echocardiography guideline.20 LV systolic function was measured by Simpson’s method.
Doppler Echocardiography
Trans-mitral flow was saved from the apical 4-chamber view with a 1 to 2 mm sample volume located at the tips of mitral valve leaflets. Peak E velocity (cm/s), peak A velocity (cm/s), E/A ratio, deceleration time (DT) (ms) and A wave duration (ms) were acquired. Isovolumetric relaxation time (IVRT) (ms) was determined as the time between ending aortic flow to the initiating mitral in-flow wave from an apical 5-chamber view.
The TEI index was evaluated from tissue Doppler documentation in the base of the interventricular septum. Tissue Doppler imaging (TDI) enables us to measure both relaxation and contraction velocities simultaneously. The TEI index was calculated as (A_B)/B. A is the time interval from the end of a-wave to the onset of e-wave, and corresponds to the sum of the isovolumetric contraction time (ICT), ejection time (ET) and isovolumetric relaxation time. Ejection time or B interval is the time from the onset to the end of the s-wave21 (Figure 1A). Myocardial acceleration during isovolumic contraction was measured by dividing the peak velocity (IVV) by the time interval from onset of the wave (zero-crossing) during isovolumic contraction to the time at the peak velocity of this wave (Figure 1B).
 |
Figure 1 The TEI index was calculated from tissue Doppler documentation as (A_B)/B. A is the time interval from the end of a-wave to the onset of e-wave and B interval is the time from the onset to the end of the s-wave (A). Myocardial acceleration during isovolumic contraction was measured by dividing the peak velocity (IVV) by the time interval from onset of the wave (zero-crossing) during isovolumic contraction to the time at the peak velocity of this wave (B). |
Pro-BNP Measurement
We obtained venous blood samples for Pro-BNP analysis, from fasted patients after 30 minutes resting and a supine position, and they were maintained in EDTA tubes. Serum Pro-BNP level was measured with a fully automated non-competitive electro-chemiluminescence immunoassay (Roche Diagnostics Co.). Diagnosis limit was 5 pg/mL.
Patient Management
We completed a checklist for each patient including age, gender, past medical history such as diabetes, ischemic heart disease, CABG, laboratory data such as Na, BUN, creatinine, hemoglobin, physical and echocardiographic exam like NYHA classification, EF, ESV, EDV, EDD, ESD, E/Em, mid RV diameter, TEI LV, TEI RV, RVIVA, LVIVA and followed them for 6 months. We recorded in-hospital mortality and outcome of patients during the follow-up.
Statistics
All data were entered in SPSS (Statistical Package for Social Sciences for Windows, version 12; Chicago, IL, USA) software and analyzed. We used mean and standard deviation for quantitative characteristics. K2 test was used for categorical characteristics comparison. For correlation between variables, the Spearman test was done. P-value less than 0.05 was considered as significant.
Findings
We finally enrolled 65 patients according to the inclusion and exclusion criteria. The mean age of subjects was 63.38±12.85 years. Most of them were male (61.5%). The demographics of the participants are listed in Table 1.
 |
Table 1 The Demographics of Participants in the Study |
ECG changes were observed in 80% of participants. The pattern of electrocardiographic changes of participants is shown in Table 2. The most observed pattern was PRP and Q wave in leads V1 to V6.
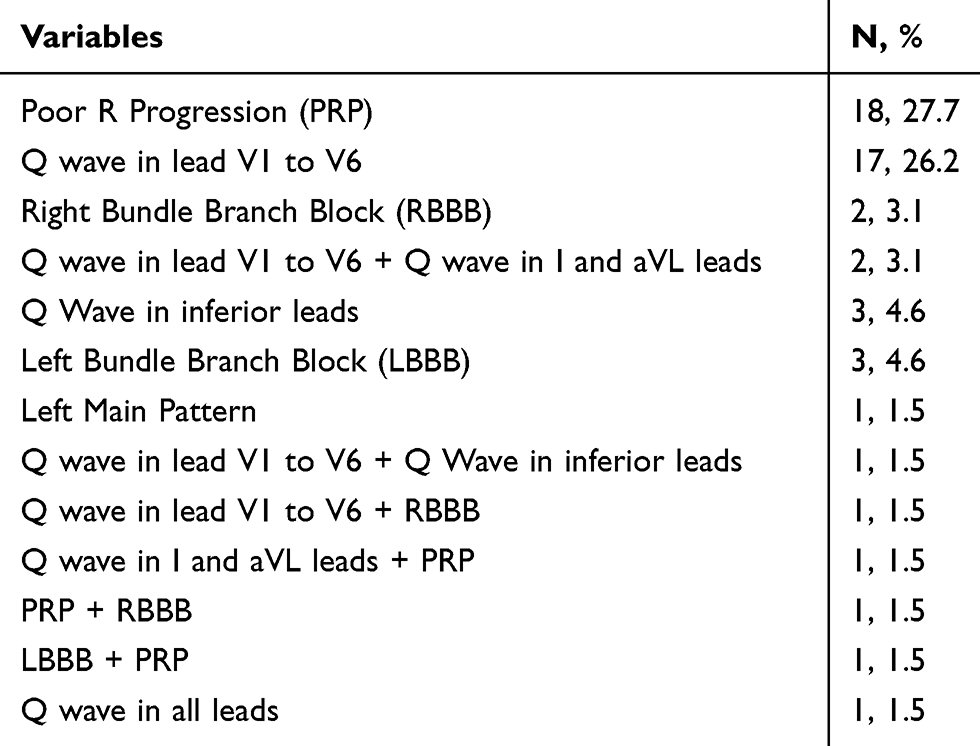 |
Table 2 The Patterns of ECG Changes in Participant Groups |
The mean value of ejection fraction was 27.52±6.69%. The values of echocardiographic and laboratory data are summarized in Table 3.
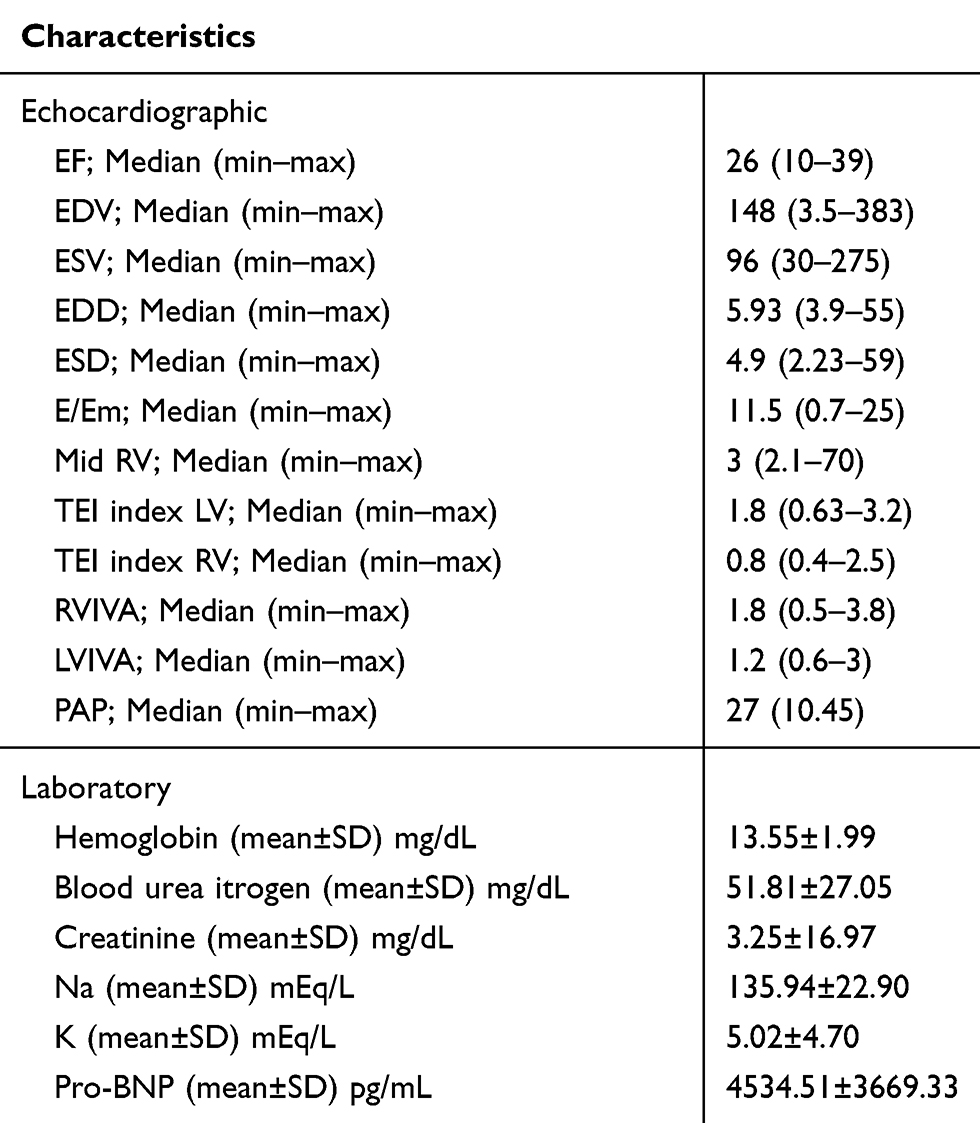 |
Table 3 The Values of Echocardiographic and Laboratory Data of Participants |
We showed a direct and significant relationship between RVIVA (r=0.317, P=0.010) and LVIVA (r=0.254, P=0.041) with EF. There was no significant correlation between Pro-BNP level and NHYA classification (r=0.151, P=0.231). We showed that there was no correlation between Pro-BNP level and RV TEI index (r=0.065, P=0.490) and LV TEI index (r=0.071, P=0.419). We also showed no significant correlation between Pro-BNP level and RVIVA (r=0.057, P=0.652) and LVIVA (r=−0.178, P=0.159) (Figure 2). In sub-group analysis, we showed there was a significant correlation between Pro-BNP level and RV TEI index in patients with EF<20% (Figure 3).
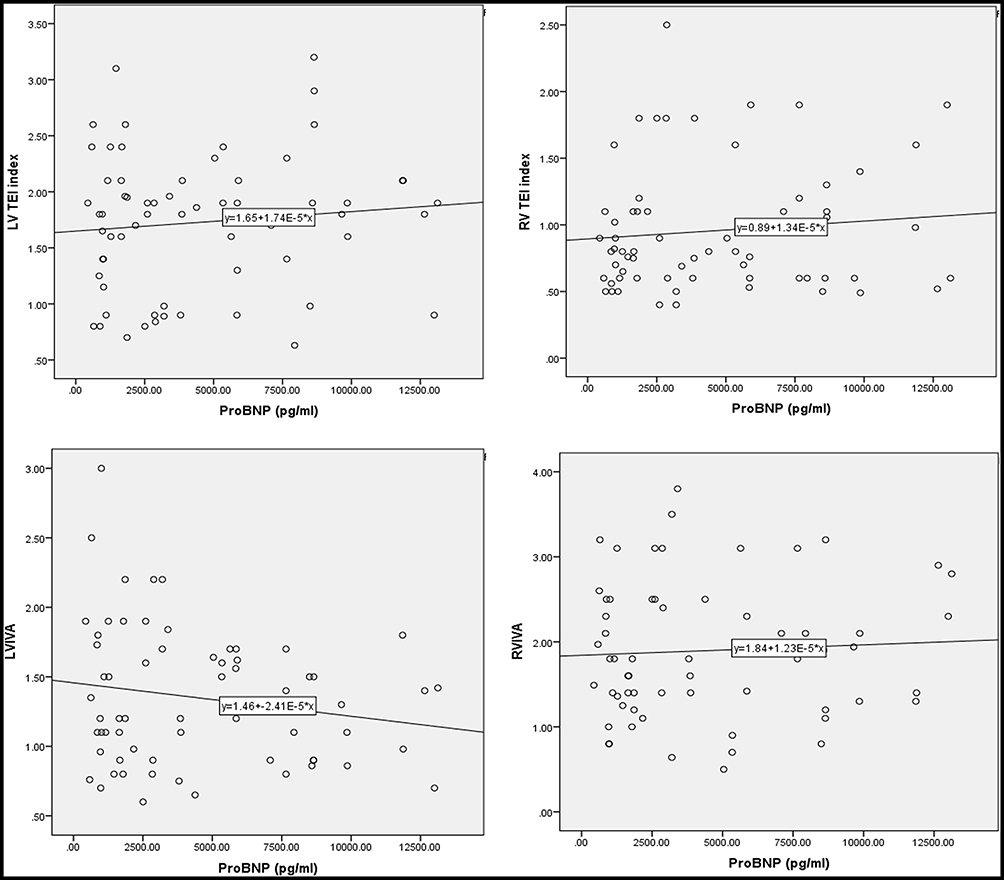 |
Figure 2 The correlation between Pro-BNP and RVIVA, LVIVA, RV TEI index and LV TEI index. |
 |
Figure 3 The correlation between Pro-BNP and RV TEI index in patients with EF<20%. |
In our study population, there was no in-hospital mortality and during 6-month follow-up, only one patient died. The multiple logistic regression analysis in systolic heart failure patients showed the LV TEI index could significantly predict mortality (β=−0.329, T=−2.643, P=0.011).
Discussion
There are limited studies evaluating the relationship between Pro-BNP and Doppler echocardiographic parameters in subjects with systolic HF. Here, we evaluated this relation between the level of Pro-BNP and TEI and IVA indexes. The main outcome of our investigation demonstrates that there was no marked correlation between Pro-BNP level and RV TEI index, LV TEI index, RVIVA and LVIVA in all participants.
In patients with less than 20% EF, a positive relationship was found between RV TEI index and Pro-BNP. This issue in our population study can show the TEI index is related with Pro-BNP level in lower EF HF patients. We also showed that the LV TEI index could significantly predict the 6-month mortality in our population.
NHYA classification and Pro-BNP level had no considerable relation in this study. In line with our result, Mikkelsen et al21 showed that Pro-BNP concentrations were decreased after treatment and change in Pro-BNP was poorly correlated with NYHA classification. In contrast, in Lee et al's study, there was a strong relationship between Pro-BNP and NYHA classification in the beginning of the research but the changes of Pro-BNP and NYHA classification had poor correlation.22 Jourdain et al showed that by increasing NYHA classification, BNP concentration rose.23
In this study, RVIVA and LVIVA had directly marked correlation with LVEF.
However, there was no considerable correlation between RV and LVIVA and Pro-BNP concentration in systolic HF patients. RVIVA calculation might be a more sensitive method in predicting contractility.18,24 Previously, IVA was an indicator of early right ventricular dysfunction in obstructive sleep apnoea and systemic sclerosis subjects.25–27 In Yang et al's study, they first validated the accuracy of IVA in RV systolic function in patients with pulmonary hypertension and found it can be an independent indicator of right ventricular function.28
A novel, non-invasive Doppler indicator that covers both systolic and diastolic myocardial function was introduced as the TEI index.29 The TEI index was determined by the summation of ICT and IRT divided by ET. In our study, despite a linear correlation with lower r2 value between Pro-BNP and RV and LV TEI indexes, the relationship was not significant. The LV dysfunction is leading to prolongation of both ICT and IRT and lower ejection time.30 Therefore, the TEI index increases in subjects with LV dysfunction and is an indicator of global LV performance. The normal value of the TEI index is mentioned as 0.39±0.05 in adults. A TEI index of 0.45 can markedly associate with elevated BNP levels in comparison with TEI index <0.45, independent of LV systolic function.31 One study showed that, after first myocardial infarction, elevated TEI index could be a predictor of early in-hospital heart failure.32 Lang found that BNP levels were elevated in patients with isolated diastolic dysfunction.33 The extent of systolic dysfunction is not always associated with deterioration in functional status in HF patients. Moreover, diastolic dysfunction is generally related to primary systolic dysfunction. Therefore, the index merging both systolic and diastolic function might present a best overall LV function rather than separately ejection or relaxation.34
Our study had some limitations. First, we had few participants. We could not check the Pro-BNP in the last follow-up. Our last follow-up only described the mortality rate and not the change in echocardiographic and laboratory data. Another limitation was the short-term follow-up in our study, which was only 6 months. It is recommended to do a large-scale study with long-term follow-up concluded measuring all echocardiographic and laboratory characteristics between follow-up times.
Conclusions
We showed that the IVA index is correlated to both LV and RVEF and can differ in large-scale in a population study. We also showed that the RV TEI index is significantly correlated with Pro-BNP in patients with EF<20%. Another finding of this study was the predictor role of the LV TEI index in 6-month mortality rate. Our results suggested that these indexes are new and important indexes which need to be more evaluated in large-scale populations.
Acknowledgments
The authors all thank Ghaem Hospital catheterization laboratory for their cooperation in doing this study. This study was supported by Mashhad University of Medical Sciences.
Funding
There was no funding support.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Savarese G, Lund LH. Global public health burden of heart failure. Card Fail Rev. 2017;3(1):7–11. doi:10.15420/cfr.2016:25:2
2. Ziaeian B, Fonarow GC. Epidemiology and aetiology of heart failure. Nat Rev Cardiol. 2016;13(6):368–378.
3. Goldberg LR, Jessup M. Stage B heart failure: management of asymptomatic left ventricular systolic dysfunction. Circulation. 2006;113(24):2851–2860. doi:10.1161/CIRCULATIONAHA.105.600437
4. McMurray JJ, Ezekowitz JA, Lewis BS, et al. Left ventricular systolic dysfunction, heart failure, and the risk of stroke and systemic embolism in patients with atrial fibrillation: insights from the ARISTOTLE trial. Circ Heart Fail. 2013;6(3):451–460.
5. Rigolli M, Whalley GA. Heart failure with preserved ejection fraction. J Geriatr Cardiol. 2013;10(4):369.
6. Gong H, Wang X, Shi Y-J, et al. Correlation between brain natriuretic peptide levels and the prognosis of patients with left ventricular diastolic dysfunction. Exp Ther Med. 2016;11(6):2583–2589. doi:10.3892/etm.2016.3203
7. Ritchie RH, Rosenkranz AC, Kaye DM. B-type natriuretic peptide: endogenous regulator of myocardial structure, biomarker and therapeutic target. Curr Mol Med. 2009;9(7):814–825. doi:10.2174/156652409789105499
8. Talwar S, Siebenhofer A, Williams B, Ng L. Influence of hypertension, left ventricular hypertrophy, and left ventricular systolic dysfunction on plasma N terminal proBNP. Heart. 2000;83(3):278–282. doi:10.1136/heart.83.3.278
9. Pfister R, Scholz M, Wielckens K, Erdmann E, Schneider C. Use of NT‐proBNP in routine testing and comparison to BNP. Eur J Heart Fail. 2004;6(3):289–293.
10. Kim WS, Park S-H. Correlation between N-terminal pro-brain natriuretic peptide and Doppler echocardiographic parameters of left ventricular filling pressure in atrial fibrillation. J Cardiovasc Ultrasound. 2011;19(1):26–31. doi:10.4250/jcu.2011.19.1.26
11. Tei C. New non-invasive index for combined systolic and diastolic ventricular function. J Cardiol. 1995;26(2):135–136.
12. Eidem BW, Tei C, O’Leary PW, Cetta F, Seward JB. Nongeometric quantitative assessment of right and left ventricular function: myocardial performance index in normal children and patients with Ebstein anomaly. J Am Soc Echocardiogr. 1998;11(9):849–856. doi:10.1016/S0894-7317(98)70004-5
13. Yeo TC, Dujardin KS, Tei C, Mahoney DW, McGoon MD, Seward JB. Value of a Doppler-derived index combining systolic and diastolic time intervals in predicting outcome in primary pulmonary hypertension. Am J Cardiol. 1998;81(9):1157–1161. doi:10.1016/S0002-9149(98)00140-4
14. Tei C, Dujardin KS, Hodge DO, Kyle RA, Tajik AJ, Seward JB. Doppler index combining systolic and diastolic myocardial performance: clinical value in cardiac amyloidosis. J Am Coll Cardiol. 1996;28(3):658–664. doi:10.1016/0735-1097(96)00202-1
15. Dujardin KS, Tei C, Yeo TC, Hodge DO, Rossi A, Seward JB. Prognostic value of a Doppler index combining systolic and diastolic performance in idiopathic-dilated cardiomyopathy. Am J Cardiol. 1998;82(9):1071–1076.
16. Tei C, Dujardin KS, Hodge DO, et al. Doppler echocardiographic index for assessment of global right ventricular function. J Am Soc Echocardiogr. 1996;9(6):838–847. doi:10.1016/S0894-7317(96)90476-9
17. Vogel M, Cheung MM, Li J, et al. Noninvasive assessment of left ventricular force-frequency relationships using tissue Doppler–derived isovolumic acceleration: validation in an animal model. Circulation. 2003;107(12):1647–1652. doi:10.1161/01.CIR.0000058171.62847.90
18. Turhan S, Tulunay C, Ozduman Cin M, et al. Effects of thyroxine therapy on right ventricular systolic and diastolic function in patients with subclinical hypothyroidism: a study by pulsed wave tissue Doppler imaging. J Clin Endocrinol Metab. 2006;91(9):3490–3493. doi:10.1210/jc.2006-0810
19. Tayyareci Y, Nisanci Y, Umman B, et al. Early detection of right ventricular systolic dysfunction by using myocardial acceleration during isovolumic contraction in patients with mitral stenosis. Eur J Echocardiogr. 2007;9(4):516–521.
20. Schiller N, Shah PM, Crawford M. American society of echocardiography committee on standards, subcommittee on quantitation of two-dimensional echocardiograms: recommendations for quantitation of the left ventricle by two-dimensional echocardiography. J Am Soc Echocardiogr. 1989;2(5):358–367. doi:10.1016/S0894-7317(89)80014-8
21. Mikkelsen KV, Møller JE, Bie P, Ryde H, Videbæk L, Haghfelt T. Tei index and neurohormonal activation in patients with incident heart failure: serial changes and prognostic value. Eur J Heart Fail. 2006;8(6):599–608. doi:10.1016/j.ejheart.2005.11.015
22. Lee S-C, Stevens TL, Sandberg SM, et al. The potential of brain natriuretic peptide as a biomarker for New York Heart Association class during the outpatient treatment of heart failure. J Card Fail. 2002;8(3):149–154. doi:10.1054/jcaf.2002.125368
23. Jourdain P, Funck F, Bellorini M, et al. Bedside B‐type natriuretic peptide and functional capacity in chronic heart failure. Eur J Heart Fail. 2003;5(2):155–160. doi:10.1016/S1388-9842(02)00247-7
24. Pauliks LB, Chan K-C, Chang D, et al. Regional myocardial velocities and isovolumic contraction acceleration before and after device closure of atrial septal defects: a color tissue Doppler study. Am Heart J. 2005;150(2):294–301. doi:10.1016/j.ahj.2004.09.052
25. Schattke S, Knebel F, Grohmann A, et al. Early right ventricular systolic dysfunction in patients with systemic sclerosis without pulmonary hypertension: a Doppler tissue and speckle tracking echocardiography study. Cardiovasc Ultrasound. 2010;8:3. doi:10.1186/1476-7120-8-3
26. Tugcu A, Yildirimturk O, Tayyareci Y, Demiroglu C, Aytekin S. Evaluation of subclinical right ventricular dysfunction in obstructive sleep apnea patients using velocity vector imaging. Circ J. 2010;74(2):312–319. doi:10.1253/circj.CJ-09-0562
27. Sciatti E, Vizzardi E, Bonadei I, Curnis A, D’Aloia A, Metra M. Prognostic value of RV isovolumic acceleration and tissue strain in moderate HF r EF. Eur J Clin Invest. 2015;45(10):1052–1059. doi:10.1111/eci.12505
28. Yang T, Liang Y, Zhang Y, et al. Echocardiographic parameters in patients with pulmonary arterial hypertension: correlations with right ventricular ejection fraction derived from cardiac magnetic resonance and hemodynamics. PLoS One. 2013;8(8):e71276. doi:10.1371/journal.pone.0071276
29. Tei C, Ling L, Hodge D, et al. New index of combined systolic and diastolic myocardial performance: a simple and reproducible measure of cardiac function–a study in normals and dilated cardiomyopathy. J Cardiol. 1995;26(6):357–366.
30. Weissler AM, Harris WS, Schoenfeld CD. Systolic time intervals in heart failure in man. Circulation. 1968;37(2):149–159. doi:10.1161/01.CIR.37.2.149
31. Ono M, Tanabe K, Asanuma T, et al. Doppler echocardiography-derived index of myocardial performance (Tei index). Jpn Circ J. 2001;65(7):637–642. doi:10.1253/jcj.65.637
32. AlsayedAbuomara HZ, MohamedHassan O, Rashid T, Baraka M. Myocardial performance index as an echocardiographic predictor of early in-hospital heart failure during first acute anterior ST-elevation myocardial infarction. Egypt Heart J. 2018;70:71–75. doi:10.1016/j.ehj.2017.12.001
33. Lang CC. Increased plasma levels of brain natriuretic peptide in patients with isolated diastolic dysfunction. Am Heart J. 1994;127:1635–1636.
34. Cao Z, Jia Y, Zhu B. BNP and NT-proBNP as diagnostic biomarkers for cardiac dysfunction in both clinical and forensic medicine. Int J Mol Sci. 2019;20(8):1820. doi:10.3390/ijms20081820
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.