Back to Journals » Clinical Ophthalmology » Volume 14
Refractive and Visual Outcomes After Implantation of a Secondary Toric Sulcus Intraocular Lenses
Authors Gundersen KG ![]() , Potvin R
, Potvin R ![]()
Received 27 March 2020
Accepted for publication 6 May 2020
Published 18 May 2020 Volume 2020:14 Pages 1337—1342
DOI https://doi.org/10.2147/OPTH.S255725
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kjell Gunnar Gundersen,1 Rick Potvin2
1IFocus Øyeklinikk AS, Haugesund, Norway; 2Science in Vision, Akron, NY, USA
Correspondence: Kjell Gunnar Gundersen Email [email protected]
Purpose: To evaluate the rotational stability, visual acuity and refractive error after sulcus implantation of a secondary toric IOL.
Setting: One clinical practice in Haugesund, Norway.
Design: Non-interventional single-arm diagnostic study.
Methods: Eligible subjects who had previous successful primary cataract or refractive lens exchange surgery in one or both eyes and the AddOn® secondary toric IOL implanted in the sulcus were evaluated at a single postoperative diagnostic visit to measure visual outcomes. Subjects with surgical complications (either primary or secondary) or pathology that would affect best-corrected visual acuity (eg, amblyopia) were excluded. Clinical evaluations at the diagnostic visit included measurement of visual acuity, manifest refraction and IOL orientation.
Results: Eighteen eyes were evaluated. After secondary IOL implantation, mean residual refractive astigmatism was significantly reduced (1.66 ± 0.92 to 0.32 ± 0.25 D). There was no appreciable change in the spherical equivalent refraction. Sixteen of 18 eyes (89%) had residual refractive astigmatism ≤ 0.50D, and no eye had more than 0.75D after secondary IOL implantation. Mean UCVA was 0.00 ± 0.03 logMAR, with no eyes worse than 0.10. Mean BCVA was − 0.05 ± 0.03 logMAR (20/20+2), with all eyes having BCVA of 0.00 logMAR. The mean change in orientation was near zero, with a mean absolute change of 4.9 ± 3.7 degrees. Sixteen of 18 eyes (89%) had a lens orientation ≤ 10 degrees from intended, with no eye oriented more than 13 degrees from intended.
Conclusion: The AddOn® toric sulcus IOL significantly reduced postoperative refractive astigmatism in patients with high astigmatism after their primary cataract or RLE surgery, providing very good uncorrected distance vision.
Keywords: sulcus IOL, secondary IOL, AddOn toric, toric IOL
Plain Language Summary
With modern cataract surgery, patients are interested in having their dependence on spectacles reduced, either for distance or (when patients choose a presbyopia-correcting IOL) for all viewing distances. In both cases, clear distance vision is the most important predictor of satisfaction. Astigmatism, an optical condition that blurs vision at any distance, can negatively affect results after surgery. While glasses and contact lenses may be used to correct astigmatism after surgery many patients would rather have the situation corrected surgically. One option is a second lens implanted in their eye, on top of the first, to reduce their astigmatism. The challenge is that such lenses must be sufficiently stable in the eye that they do not rotate, because rotation would change the effect the lens had on astigmatism. We designed this study to determine if a secondary lens used for correcting astigmatism after the original cataract surgery was sufficiently stable to provide improved vision.
Our results showed that the secondary lenses implanted were very effective in reducing astigmatism in the 18 eyes in which they were implanted. There were only minor differences between the orientation planned for the lenses and their final position. All subjects had 20/25 or better distance vision without glasses after secondary surgery.
Introduction
Modern cataract surgery is a refractive procedure, with patient expectations of significantly reduced dependence on spectacles after cataract surgery and intraocular lens (IOL) implantation, at least for distance vision. However, unanticipated residual astigmatism can occur, which produces suboptimal visual outcomes in some patients. A 1.5 line decrease in uncorrected distance visual acuity (UDVA) can occur with each diopter of residual astigmatism.1
Residual refractive astigmatism can be managed with spectacles or contact lenses, but many patients prefer not to have to rely on these for clear distance vision.2 Surgical alternatives to correct residual refractive astigmatism include corneal refractive surgery, arcuate partial-depth incisions, IOL exchange or secondary lens implantation.3–7 Corneal refractive surgery, such as photo-refractive keratectomy (PRK) and laser in situ keratomileusis (LASIK), may worsen dry eye and negatively affect visual outcomes in some patients.8 Relaxing incisions may only be appropriate for reducing small amounts of corneal astigmatism.9 Performing an IOL exchange can result in good refractive outcomes for patients,10 but there are risks of zonular damage and capsular rupture. Secondary lens implantation is a less-invasive procedure than an IOL exchange.
Secondary lens implantation began with the “two-in-the-bag” technique, which placed two IOLs in the capsular bag.11 This technique led to interlenticular opacification;12 as a result, secondary lenses are now generally targeted for implantation in the ciliary sulcus. However, these secondary IOLs need to be specifically designed for implantation in the sulcus, as the sharp edges of IOLs designed for the capsular bag can lead to iris chafing and pigmentary glaucoma. 13 Secondary IOLs are typically designed with round optic edges (to prevent iris chafing) and a concave posterior surface to reduce the potential for interlenticular opacification. Secondary lens implantation has been demonstrated to provide good visual outcomes and safety for patients,7,14,15 including when implanted to correct residual astigmatism.16–18
The AddOn® IOL (1stQ GmbH, Mannheim, Germany) is one secondary IOL option, available in monofocal, multifocal, toric and multifocal toric designs. It has an overall diameter of 13.0 mm and an optic diameter of 6.0 mm. The optic is convex on the anterior and concave on the posterior. Attached to the optic are four soft flexible haptics. Two previous studies have been published evaluating this secondary IOL. Reiter et al19 used human cadaver eyes to investigate alignment and spacing between the secondary and primary IOLs. The results suggested that both the alignment and spacing were adequate, though tilt was observed in a few cases. Gundersen and Potvin7 investigated the visual outcomes in 46 eyes implanted with the non-toric and toric models of this secondary IOL to correct residual refractive error. The authors reported a mean increase of almost 2 lines in uncorrected visual acuity (UCVA) for the 46 subjects evaluated. In the 10 eyes treated with a toric version of the IOL, there was a significant reduction in refractive astigmatism. The purpose of the present study was to evaluate the clinical and visual performance of the toric version of this secondary IOL after sulcus implantation to correct residual astigmatism.
Methods
This study was a non-interventional single-arm study of visual outcomes after successful cataract or refractive lens exchange (RLE) surgery that was followed by sulcus implantation of a secondary toric IOL to correct residual astigmatism. There was no masking and no control group. The study was approved by an institutional review board (REK, Norway) and all subjects signed an appropriate informed consent. The study was conducted in a manner consistent with the tenets of the Declaration of Helsinki. The study involved only a single postoperative diagnostic evaluation, with no intervention, so there was no requirement to register with any clinical trial registry.
Eligible subjects were those who had previous successful primary cataract or RLE surgery in one or both eyes and a secondary toric IOL implanted in the sulcus at a later date. Subjects with surgical complications (either primary or secondary) or pathology that would affect best-corrected visual acuity (eg, amblyopia) were excluded. Subjects were assessed during a single visit 1 month or more after their secondary IOL implantation surgery. Their prior surgery history was recorded, including the IOL originally implanted, the residual refractive error after primary implantation and the secondary IOL implanted. All secondary IOLs were implanted by the same surgeon (KGG) at one site. The online AddOn toric calculator was used to plan the orientation of the sulcus IOL.
Clinical evaluations at the diagnostic visit included measurement of visual acuity, manifest refraction and IOL orientation. The primary measure of interest was the change in orientation of the IOL. This was measured using images from the Casia SS-1000 swept source optical coherence tomography (OCT) scanner (Tomey Corporation, Aichi, Japan). Other measures of interest included distance visual acuity (uncorrected and best-corrected) and the manifest refraction. IOP before sulcus IOL implantation and at the diagnostic visit were recorded where available. Refractive and visual acuity changes were based on by-subject differences, evaluated with a repeated-measures analysis of variance (ANOVA). IOL orientation analysis was limited to descriptive statistics, as there was no comparison group. In addition, a slit lamp examination was conducted to determine if any intralenticular opacification or pigment dispersion due to iris chafing had occurred.
Results
Twenty eyes for possible inclusion in the study were identified from clinical records. One eye was amblyopic and another eye had a surgical complication unrelated to the secondary IOL, leaving 18 eyes for analysis. Secondary IOL implantation occurred from 5/15 to 11/19. Primary lenses included trifocal, EDOF and monofocal IOLs, both sphere and toric. There were insufficient lenses in any group for reliable subgroup analysis. Follow up times after secondary IOL surgery ranged from 43 days to 4.5 years, though the majority of eyes were evaluated 1 to 2 years after surgery. Seven eyes (39%) were examined more than 3 years after secondary IOL implantation. Surgical records showed the mean sphere power of the sulcus toric IOL was 0.03 ± 1.23 D, and ranged from −2.50D to 1.75D. The majority of the IOLs (13/18, 72%) had a cylinder power of 1.5 (7) or 2.25 (6).
Table 1 shows the mean spherical equivalent refraction and the refractive cylinder before and after IOL implantation. After secondary IOL implantation, mean residual refractive astigmatism was significantly reduced (p < 0.001), though there was no appreciable change in the spherical equivalent refraction (p = 0.83). The residual cylinder was not correlated to the cylinder power of the sulcus IOL (p > 0.05). Figure 1 shows the distribution of residual refractive astigmatism at that latter visit. Sixteen of 18 eyes (89%) had residual refractive astigmatism ≤0.50D, and no eye had more than 0.75D after secondary IOL implantation.
 |
Table 1 Spherical Equivalent Refraction and Refractive Cylinder Before and After Secondary IOL Implantation |
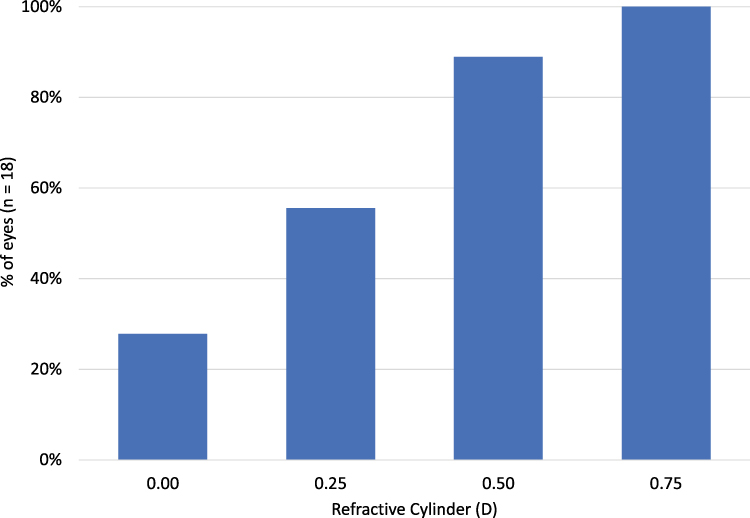 |
Figure 1 Cumulative dstribution of refractive astigmatism after secondary IOL implantation in the sulcus.Abbreviations: IOL, intraocular lens; D, diopter. |
After secondary IOL implantation, mean UCVA was 0.00 ± 0.03 logMAR (20/20 Snellen) for the 17 eyes that had a target of plano (one eye was targeted for monovision). No eye had UCVA worse than 0.1 logMAR (20/25) and 13/17 (76%) had a UCVA of plano (0.0) or better. Mean BCVA was −0.05 ± 0.03 logMAR (20/20+2), with all eyes having BCVA of 0.00 logMAR (20/20). Sixteen of 18 eyes had UCVA within 1 line of their BCVA.
Figure 2 shows the distribution of the difference in lens orientation from the intended orientation. The mean difference was −0.1 ± 6.3 degrees, which was not statistically significantly different from zero (p = 0.94). The mean absolute lens orientation was 4.9 ± 3.7 degrees from intended. Sixteen of 18 eyes (89%) had a lens orientation ≤10 degrees from intended, and no eye had a lens orientation of more than 13 degrees from intended. There was no correlation between the time between secondary IOL implantation and the difference in IOL orientation from intended (p = 0.45).
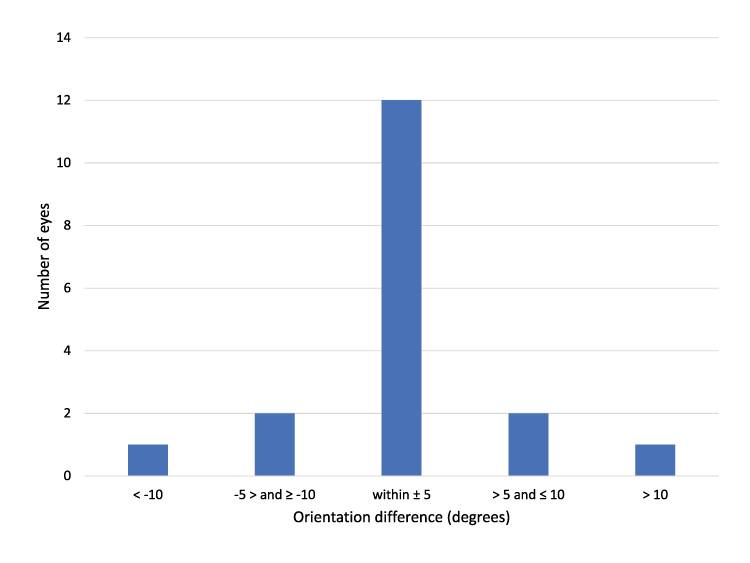 |
Figure 2 Distribution of difference in lens orientation from intended. |
Intraocular pressure readings just before sulcus IOL implantation and at the diagnostic visit were available for 16 eyes. A repeated-measures analysis of variance showed no statistically significant difference in the IOP before and after the secondary IOL implantation (12.6 ± 2.6 mmHg before and 12.9 ± 2.4 mmHg after, p = 0.54). The mean change for all eyes was 0.4 mmHg, with a range of −6.0 to +4.0 mmHg. No eye had an IOP higher than 20 mmHg at the diagnostic visit.
There was no evidence of any interlenticular opacification in any of the eyes. There was also no evidence of any pigment dispersion.
Discussion
To the best of our knowledge, this is one of the largest published data sets to evaluate the clinical performance of the 1stQ AddOn toric secondary IOL after implantation in the sulcus, and one of the largest for any toric sulcus IOL.
The results of this study demonstrate that the 1stQ IOL can provide visual and refractive outcomes similar to or better than those obtained with other currently available secondary toric IOLs or LASIK to correct residual astigmatism.5,7,16-18,20–23 Other toric secondary IOLs include the HumanOptics add-on toric IOL (HumanOptics, Erlangen, Germany) the Sulcoflex toric IOL (Rayner Intraocular Lenses, East Essex, United Kingdom) and the toric Implantable Collamer Lens (ICL, STAAR Surgical). Several older case studies of the HumanOptics IOL can be found in the literature,20,21 though the lens is no longer commercially available. The case study presented by Rabsilber et al21 reported binocular UDVA of 20/20 and high patient satisfaction following bilateral implantation; however, more studies are needed to corroborate this result. Thomas et al18 used the HumanOptics add-on toric secondary IOL in cases with high astigmatism and observed good results, which included a spherical equivalent of ±1.00 D in 65% of eyes. Results here appear as good or better than these, and in a larger sample. The Sulcoflex toric IOL has been used to correct residual astigmatism in patients with and without prior corneal transplantation.16,22,23 McLintock et al16 reported that the visual outcomes in patients with no prior corneal transplantation were acceptable, with 61% of eyes achieving a UDVA of 20/20; the results with the IOL in the current study (76%) appear better than this. The mean UDVA for the toric ICL was reported to be around 0.2 logMAR, almost 2 lines lower than the results achieved in the current study.
The mean residual refractive cylinder was significantly reduced in the current study, with a residual cylinder of 0.50 D or less in 89% of eyes. This appears better than the results reported by Gundersen and Potvin7 for the same lens (but with only 10 eyes); they reported residual cylinder of 0.50D or less in 70% of eyes. The results for the current study also appear better than the 73% reported for the Sulcoflex lens, and 62.5% reported for the toric ICL in prior studies.16,17
Rotational stability is of critical importance for toric IOLs. Excessive lens misorientation can significantly decrease the effectiveness of the IOL.24 The 1stQ lens studied here had very good rotational stability, with a mean absolute lens rotation <5°. This is much lower than has been reported for the Sulcoflex IOL. In a large sample, the mean rotation was 8.2° at 1 day and 17° at the last subject visit (at least 3 months postoperative).16 No 1stQ IOLs in the current study needed repositioning, compared to 62% for the Sulcoflex lens in a previous study16 and 25% for the Humanoptics IOLs.16 Despite the fact that the lens is positioned in the ciliary sulcus, the rotational stability achieved with the IOL in the present study appears similar to that observed with primary toric IOLs into the capsular bag.25 The unique haptic design of the IOL studied here may be a contributing factor to this observed stability.
Almost 40% of eyes evaluated were seen more than 3 years after their secondary implant surgery. The absence of intralenticular opacification and pigment dispersion in any of the eyes examined indicates that the IOL design is well suited for sulcus implantation. There was also no material change in the IOP in any eye.
This study has several limitations. The study was based on a post-operative diagnostic evaluation of previously implanted eyes, which is retrospective in nature, as there is no ethical rationale to justify conducting a prospective study. The number of subjects is larger than many comparable studies of secondary IOLs but is still fairly low. Finally, the diagnostic testing was primarily limited to visual acuity and refractive error, though eyes were also examined for interlenticular opacification and pigment dispersion. There may be other measures of interest related to ocular health and/or patient satisfaction that would be useful to quantify.
In summary, the secondary toric IOL investigated in the current study, when implanted in the sulcus, significantly reduced residual refractive astigmatism and provided very good uncorrected distance vision for subjects. Lens rotation was minimal.
Acknowledgments
Brad Hall, PhD of Sengi, aided in the preparation of this manuscript.
Disclosure
This research was conducted with an unrestricted grant from 1stQ Deutschland GmbH. Dr Rick Potvin reports personal fees from Alcon and Carl Zeiss Meditec, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Lehmann RP, Houtman DM. Visual performance in cataract patients with low levels of postoperative astigmatism: full correction versus spherical equivalent correction. Clin Ophthalmol. 2012;6:333–338. doi:10.2147/OPTH.S28241
2. Wilkins MR, Allan B, Rubin G, Moorfields IOLSG. Spectacle use after routine cataract surgery. Br J Ophthalmol. 2009;93(10):1307–1312. doi:10.1136/bjo.2008.151829
3. Thornton SP. Astigmatic keratotomy: a review of basic concepts with case reports. J Cataract Refract Surg. 1990;16(4):430–435. doi:10.1016/S0886-3350(13)80795-X
4. Budak K, Friedman NJ, Koch DD. Limbal relaxing incisions with cataract surgery. J Cataract Refract Surg. 1998;24(4):503–508. doi:10.1016/S0886-3350(98)80292-7
5. Norouzi H, Rahmati-Kamel M. Laser in situ keratomileusis for correction of induced astigmatism from cataract surgery. J Refract Surg. 2003;19(4):416–424.
6. Mozayan E, Lee JK. Update on astigmatism management. Curr Opin Ophthalmol. 2014;25(4):286–290. doi:10.1097/ICU.0000000000000068
7. Gundersen KG, Potvin R. A review of results after implantation of a secondary intraocular lens to correct residual refractive error after cataract surgery. Clin Ophthalmol. 2017;11:1791–1796. doi:10.2147/OPTH.S144675
8. Szakats I, Sebestyen M, Toth E, Purebl G. Dry eye symptoms, patient-reported visual functioning, and health anxiety influencing patient satisfaction after cataract surgery. Curr Eye Res. 2017;42(6):832–836. doi:10.1080/02713683.2016.1262429
9. Hirnschall N, Gangwani V, Crnej A, Koshy J, Maurino V, Findl O. Correction of moderate corneal astigmatism during cataract surgery: toric intraocular lens versus peripheral corneal relaxing incisions. J Cataract Refract Surg. 2014;40(3):354–361. doi:10.1016/j.jcrs.2013.08.049
10. El Awady HE, Ghanem AA. Secondary piggyback implantation versus IOL exchange for symptomatic pseudophakic residual ametropia. Graefes Arch Clin Exp Ophthalmol. 2013;251(7):1861–1866. doi:10.1007/s00417-013-2283-x
11. Gayton JL, Sanders VN. Implanting two posterior chamber intraocular lenses in a case of microphthalmos. J Cataract Refract Surg. 1993;19(6):776–777. doi:10.1016/S0886-3350(13)80349-5
12. Gayton JL, Apple DJ, Peng Q, et al. Interlenticular opacification: clinicopathological correlation of a complication of posterior chamber piggyback intraocular lenses. J Cataract Refract Surg. 2000;26(3):330–336. doi:10.1016/S0886-3350(99)00433-2
13. Iwase T, Tanaka N. Elevated intraocular pressure in secondary piggyback intraocular lens implantation. J Cataract Refract Surg. 2005;31(9):1821–1823. doi:10.1016/j.jcrs.2005.06.034
14. Gerten G, Kermani O, Schmiedt K, Farvili E, Foerster A, Oberheide U. Dual intraocular lens implantation: monofocal lens in the bag and additional diffractive multifocal lens in the sulcus. J Cataract Refract Surg. 2009;35(12):2136–2143. doi:10.1016/j.jcrs.2009.07.014
15. Falzon K, Stewart OG. Correction of undesirable pseudophakic refractive error with the Sulcoflex intraocular lens. J Refract Surg. 2012;28(9):614–619. doi:10.3928/1081597X-20120809-01
16. McLintock CA, McKelvie J, Gatzioufas Z, Wilson JJ, Stephensen DC, Apel AJG. Outcomes of toric supplementary intraocular lenses for residual astigmatic refractive error in pseudophakic eyes. Int Ophthalmol. 2019;39(9):1965–1972. doi:10.1007/s10792-018-1027-7
17. Kojima T, Horai R, Hara S, et al. Correction of residual refractive error in pseudophakic eyes with the use of a secondary piggyback toric implantable collamer lens. J Refract Surg. 2010;26(10):766–769. doi:10.3928/1081597X-20100512-02
18. Thomas BC, Auffarth GU, Reiter J, Holzer MP, Rabsilber TM. Implantation of three-piece silicone toric additive IOLs in challenging clinical cases with high astigmatism. J Refract Surg. 2013;29(3):187–193. doi:10.3928/1081597X-20130212-01
19. Reiter N, Werner L, Guan J, et al. Assessment of a new hydrophilic acrylic supplementary IOL for sulcus fixation in pseudophakic cadaver eyes. Eye (Lond). 2017;31(5):802–809. doi:10.1038/eye.2016.310
20. Jin H, Limberger IJ, Borkenstein AF, Ehmer A, Guo H, Auffarth GU. Pseudophakic eye with obliquely crossed piggyback toric intraocular lenses. J Cataract Refract Surg. 2010;36(3):497–502. doi:10.1016/j.jcrs.2009.07.054
21. Rabsilber TM, Kretz FT, Holzer MP, Fitting A, Sanchez MJ, Auffarth GU. Bilateral implantation of toric multifocal additive intraocular lenses in pseudophakic eyes. J Cataract Refract Surg. 2012;38(8):1495–1498. doi:10.1016/j.jcrs.2012.06.014
22. Srinivasan S, Ting DS, Lyall DA. Implantation of a customized toric intraocular lens for correction of post-keratoplasty astigmatism. Eye (Lond). 2013;27(4):531–537. doi:10.1038/eye.2012.300
23. Ferreira TB, Pinheiro J. Clinical results with a supplementary toric intraocular lens for the correction of astigmatism in pseudophakic patients. Eur J Ophthalmol. 2015;25(4):302–308. doi:10.5301/ejo.5000564
24. Tognetto D, Perrotta AA, Bauci F, et al. Quality of images with toric intraocular lenses [published correction appears in J Cataract Refract Surg. 2018 Jun;44(6):794]. J Cataract Refract Surg. 2018;44(3):376–381. doi:10.1016/j.jcrs.2017.10.053
25. Lee BS, Chang DF. Comparison of the rotational stability of two toric intraocular lenses in 1273 consecutive eyes. Ophthalmology. 2018;125(9):1325–1331. doi:10.1016/j.ophtha.2018.02.012
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.