Back to Journals » Psychology Research and Behavior Management » Volume 13
Racial Difference in the Relationship Between Health and Happiness in the United States
Authors Cobb S, Javanbakht A, Khalifeh Soltani E, Bazargan M, Assari S ![]()
Received 6 February 2020
Accepted for publication 24 March 2020
Published 25 May 2020 Volume 2020:13 Pages 481—490
DOI https://doi.org/10.2147/PRBM.S248633
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Einar Thorsteinsson
Sharon Cobb,1 Arash Javanbakht,2 Ebrahim Khalifeh Soltani,3 Mohsen Bazargan,4,5 Shervin Assari4
1School of Nursing, Charles R Drew University of Medicine and Science, Los Angeles, CA, USA; 2Department of Psychiatry and Behavioral Neurosciences, Wayne State University, Detroit, MI, USA; 3Department of Political Science, Eastern Michigan University, Ypsilanti, MI, USA; 4Department of Family Medicine, Charles R Drew University of Medicine and Science, Los Angeles, CA, USA; 5Department of Family Medicine, UCLA, Los Angeles, CA, USA
Correspondence: Shervin Assari Email [email protected]
Background: Although health is a prerequisite for happiness, the salience of health for maintaining happiness may be diminished for Blacks when compared to Whites, a phenomenon which can be explained by the Black-White mental health paradox and minorities’ diminished returns.
Aim: To understand if Black and White adult Americans differ in the effects of self-rated health (SRH) on happiness.
Methods: This cross-sectional study used data from the General Social Survey (GSS; 1972– 2018), a nationally representative survey in the US. Our analytical sample included 42,201 Black and White adults. The independent variable was SRH. Happiness was the dependent variable. Sociodemographic factors were covariates. Race was the moderator. Logistic regression was used to analyze the data without and with interaction terms between race and SRH.
Results: Overall, good SRH was positively associated with happiness, however, there was a significant interaction between race/ethnicity and good SRH on the outcome (i.e. happiness) . This finding suggested that the boosting effect of good SRH on happiness is weaker for Black than White people.
Conclusion: In the United States, due to a weaker concordance between good health and happiness, Blacks who have poor SRH are more likely to report happiness. At the same time, Whites who are healthy report happiness, however, Blacks who are healthy do not necessarily report happiness. Disjointed link between health and happiness may be due to different racial, ethnic, and cultural perceptions of physical health and happiness as well as salience of physical health as a component of happiness. This may be an adaptive response of Blacks to sociopolitical as well as health-related adversities over centuries as a result of the combination of oppression, injustice, and poverty.
Keywords: population groups, Blacks, Whites, race/ethnicity, self-rated health, happiness
Introduction
There is abundant evidence showing happiness is influenced by both physical and mental health. Chronic physical illness as well as mood, anxiety, and other mental disorders can greatly reduce happiness.1 Happiness is recognized as being influenced by endogenic dimensions (biological, cognitive, and personality factors) and exogenic factors (health status, socio-demographics, behavioral factors, and life events).2,3 Physical health is critical in constructing and evaluating happiness,2,3 which is a major component of life satisfaction.3,4 The strong linkage between physical health and happiness is state-dependent (rather than a stable trait).5,6 For example, physical conditions such as chronic pain, arthritis, cardiovascular disease, and kidney disease may reduce happiness through causing depression and anxiety.7
The interrelationship between physical and mental health may differ across racial/ethnic groups, specifically Whites and Blacks. For example, Blacks are more likely to have co-occurring physical and mental comorbidities than Whites.8 Nobles and colleagues found the association between lifetime history of trauma and diabetes to be higher among Blacks compared to Whites.9 Blacks and Whites with better physical health have higher levels of happiness.10 However, Blacks and Whites may differ in the association between the two.
MDR Literature
According to the Minorities Diminished Status (MDRs) theory,11 the marginal utility of resources may be weaker for Blacks than Whites. For example, the return of socioeconomic status (SES) resources are systematically smaller for minority groups, such as Blacks, when compared to Whites.12 The concordance between factors that are expected to covary are weaker in Black people compared to White people. It has been established that SES is a primary determinant of adverse physical and mental health outcomes.13,14 Further, it has been found that household income is more protective for Whites against chronic medical conditions as compared to Blacks.15 Another example is that education and income show a weaker association in Blacks than Whites. Blacks are less likely to experience upward mobility based on parental and self-educational attainment.16,17 Similarly, the reciprocal association between positive and negative affect is stronger for Whites than Blacks, who endorse higher levels of negative affect.18 Similar to the marginal return of SES19,20 and coping,21 physical health may show a weaker utility for generating happiness for Blacks than Whites. In this view, due to a diminished health-happiness gradient, Blacks may show less increase in happiness even if they are healthy, however, for Whites, health would be more likely to improve happiness. This may explain the observation that highly educated and high income Black men are at an increased rather than reduced risk of depression.22–24
We may also expect a disjointed concordance between health and happiness according to the Black-White mental health paradox. The Black-White mental health paradox can be defined as better mental health of Blacks, compared to Whites, despite of higher prevalence of health problems as well as stress and adverse life conditions.25–29 Keyes found Blacks are highly resilient regardless of diminished returns, SES, and exposure to discrimination, as evidenced by their lower rates of mental illnesses.26 Assari found the association between depression and chronic medical conditions to be weaker among Blacks compared to Whites.25 Other supporting evidence has shown that mental health symptoms may be predictive of worsening health status, including mortality, for Whites but not Blacks.30 Jackson and colleagues have found that Blacks, who are more likely to live in stressful environments with multiple disparities, may reduce their mental stress symptoms though engagement in unhealthy lifestyle behaviors.31 While they can alleviate symptoms of stress, these behaviors increase the risk for higher morbidity and mortality for this group.
Another argument suggesting a disjoint between SRH and happiness is that racial differences may exist in the definition and perception of happiness in the context of SRH, and what poor SRH reflects. Many studies have documented Black-White differences in correlates of happiness32 and SRH.33–35 For Whites, SRH seems to be strongly affected by physical health as it may operate as a sponge that also absorbs social relations and promotes greater mental well-being. This may not be true for Blacks. Among Blacks, demographic and SES factors greatly impact the association between mental illness and SRH.36 For example, a study by Assari showed that the association between mental illnesses and physical SRH was explained by SES factors.33 In some other studies, SRH better reflected risk of mortality for Whites than Blacks.37 This may be because Whites may have a narrower definition of happiness and health, while for Blacks these may be different and also may be more inclusive to social factors. For example, Blacks were more likely to experience depressive symptoms if they reported mobilities issues, worse access and quality of healthcare resources, lower functional status, and limiting of social activities due to chronic health conditions.38 Further, they report high levels of self-esteem in spite of greater encounters with traumatic stress exposure.28 Another explanation is that physical illness and disability are more acceptable in the Black culture, and as a result, they may not as negatively affect their happiness, compared to Whites.
Research by Other Groups
Multiple studies have tested combined effects of race and SES on health. These studies have collectively provided evidence for the continuing significance of both race and SES in determining health status, however, in complex ways. In a study, Geronimus, Hicken, Keene, and Bound compared Black and White adults for the roles of age and SES on biological markers of health (allostatic load scores). The paper showed that Blacks experience early health deterioration, reflected in their biological indicators of repeated exposure and adaptation to stressors, however, this is not simply due to SES. Using data from the National Health and Nutrition Examination Survey data, the study showed that Blacks have higher allostatic load scores than did Whites at all ages, particularly at 35–64 years. Authors concluded that racial inequalities in health exist across a range of biological systems and are not all due to racial differences in poverty. The study proposed that combination of living in a race-conscious society and engagement in high-effort coping are likely to have physiological toll.39 Howard and Sparks also conducted a study to expand the earlier findings of racial/ethnic and education–allostatic load associations. The study investigated the persistence of racial differences in allostatic load across all levels of educational attainment. Borrowing data from four recent waves of the National Health and Nutrition Survey (NHANES), their study suggested that race/ethnicity and educational attainment affected allostatic load; however, the effect of race/ethnicity was inconsistent across education level. Analysis of interactions showed that allostatic load levels did not differ by race/ethnicity in the lowest sections of society (based on education) and largest for Mexican Americans (p < 0.01) and non-Hispanic Blacks (p < 0.001) in those with a college degree or more. This finding was attributed to differential returns to education by race/ethnicity.40 Finally, Farmer and Ferraro used the US National Health and Nutrition Examination Survey to compare racial health disparities between White and Black adults by SES. Authors found interactions between race and education/employment on health outcomes. Their study showed that the racial disparity in self-rated health was largest at the higher levels of SES, suggesting that SES generates “diminishing returns” for Black adults than White adults.41
Aims
To better understand racial differences in the association between health and happiness of American adults, we compared American Black and White adults for the effects of good SRH on happiness. Based on previous work on Blacks’ mental health paradox25,27 and diminished returns of resources for Blacks compared to Whites (i.e. MDRs),42–45 we expected a weaker association between good SRH and happiness in Blacks than Whites. To generate generalizable results, we used a nationally representative sample.
Methods
Design and Setting
The General Social Survey (GSS; 1972–2018) is a state-of-the-art social survey of American adults. The GSS is conducted annually from 1972 to 2018 by the University of Chicago to monitor the societal change and social trends of the American society over time. The GSS is mainly funded by the National Science Foundation (NSF).
Ethics
The GSS study protocol is approved by the University of Chicago Institutional Review Board (IRB). All GSS participants have provided informed consent. The current study, however, was not human subject research as all the data were public and fully deidentified.
General Social Survey (GSS)
The GSS gathers extensive data on the social aspects of the contemporary American society. This study has continued to monitor the trends of attitudes, behaviors, and beliefs of American adults for over 4 decades since 1972. The GSS helps us understand how the American individuals and society as whole have changed. It also sheds light on the changes of different demographic groups over these decades. This study provides a unique opportunity to investigate sub-population variation based on gender, race/ethnicity, and class. The data have also provided a unique opportunity to compare US subgroups over time . Some of the variables cover sociological, economical, demographic, and policy-making-related aspects of health and happiness.
Analytical Sample
The current study included all Black or White adults who had participated in the GSS from 1974 to 2018 and had data on SRH and happiness. This was a total number of 42,201 people. From all, 35,802 people were White (84.8%) and 6399 people where Black (15.2%).
Study Measures
Study variables included age, gender, race/ethnicity, educational attainment, employment status, marital status, year of the survey, as well as SRH, and happiness.
Independent Variable
SRH was measured using a 4-level categorical variable. The exact item was “Would you say your own health, in general, is excellent, good, fair, or poor?” Potential responses were excellent, good, fair, or poor. We merged excellent and good as good health (coded as 1) and fair and poor as poor SRH (coded as 0). This variable is commonly operationalized as a categorical (binary) variable to compare poor (poor/fair) and good (excellent/good) as the outcome. As shown by Idler and others, SRH is a strong and independent predictor of mortality.46
Outcome
General happiness was measured using a single item. The item reads as: “Taken all together, how would you say things are these days – would you say that you are very happy, pretty happy, or not too happy?” Responses were 1) very happy, 2) pretty happy, and 3) not too happy. This variable was operationalized as a categorical (binary) variable (1 being very happy/pretty happy, 0 not too happy).
Moderator
Self-identified race and ethnicity were measured as a three-level categorical variable: Whites 0 [the reference group], Blacks 1), and other race/ethnic groups 2.
Confounders
Age (years), race/ethnicity, and year of survey were the study covariates. Age was an interval variable, measured in years.
Gender
Gender (men 0, women 1) was a binary variable.
Year of the Survey
Year of study was operationalized as an interval variable ranging from 0 to 46 (reflecting the study years 1972 to 2018) (Table 1).
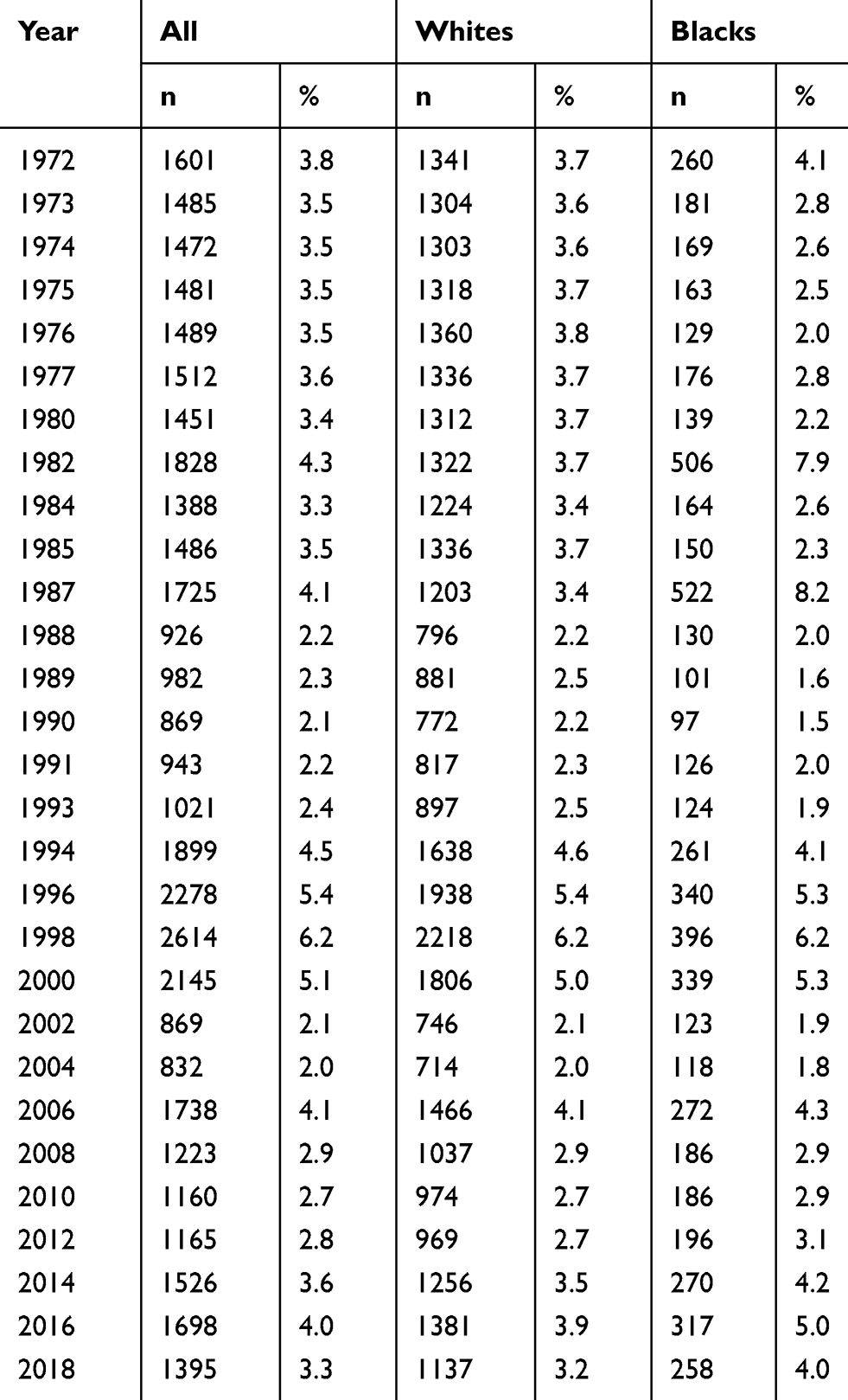 |
Table 1 Frequency of Participants Based on Year in the General Social Survey Overall and by Race |
Educational Attainment
Education attainment was measured as years of schooling, varying from 0 to 20. It was treated as an interval measure (a higher score reflecting higher education attainment/years of schooling).
Fulltime Employment
Employment was measured as an ordinal variable, with categories: “1) Working Full-time, 2) Working Part-time, 3) Temporarily Not Working, 4) Unemployed, Laid Off, 5) Retired, 6) School, 7) Keeping House, and 8) Other”. We recoded this variable as a binary variable with working full-time as 1 and other status as the reference group.
Marital Status
Marital Status was also assessed as a binary variable: Married, widowed, divorced, separated, and never married. Married was coded as 1 and other statuses were the referent category (coded as 0).
Statistical Analysis
Data were analyzed using SPSS 22.0. Although each 1. We did not apply GSS sampling weight because that is only available for 18 of 32 years (https://gssdataexplorer.norc.org/variables/5593/vshow). We reported frequency (%) and mean (standard error; SE) to describe our participants overall as well as by race/ethnicity. We used Chi-square or independent t-tests to compare race/ethnic groups for our study variables. Overall, we ran four logistic regression models for data analysis. The first two models (Model 1 and Model 2) were performed in the pooled sample that included all race/ethnic groups. Model 1 only had the main effects. Model 2, however, also included the race/ethnicity by SRH interaction term. Model 3 and Model 4 were performed in Whites and Blacks, respectively. Age, gender, educational attainment (years of education), employment status and marital status were covariates, good SRH was the primary predictor (independent variable), and year of survey were the covariates. Race/ethnicity was the moderator. Odds Ratio (OR), SE, 95% CI, and p values were reported.
Results
Descriptive Statistics
The total sample of 42,201 were drawn between 1972 and 2018. Each year about 2% to 6% of the sample was drawn (Table 1).
This study included 42,201 people. From this number, 35,802 people were White (84.8%) and 6399 people where Black (15.2%). Black and White people differed in gender, age, education, marital status, SRH, and happiness. Blacks were younger than Whites (43.56 vs 46.56; p <0.05). Blacks were more women than Whites (61.4% vs 54.7%; p <0.05). Blacks had lower education than Whites (highest education = 4.2% vs 12.5%; p <0.05). Blacks were also less likely to be married than Whites (34.7% vs 57.3%; p <0.05). Finally, Blacks were less likely than Whites to report good health (67.5% vs 76.5%; p<0.05) and high happiness (77.9% vs 88.6%; p<0.05) (Table 2).
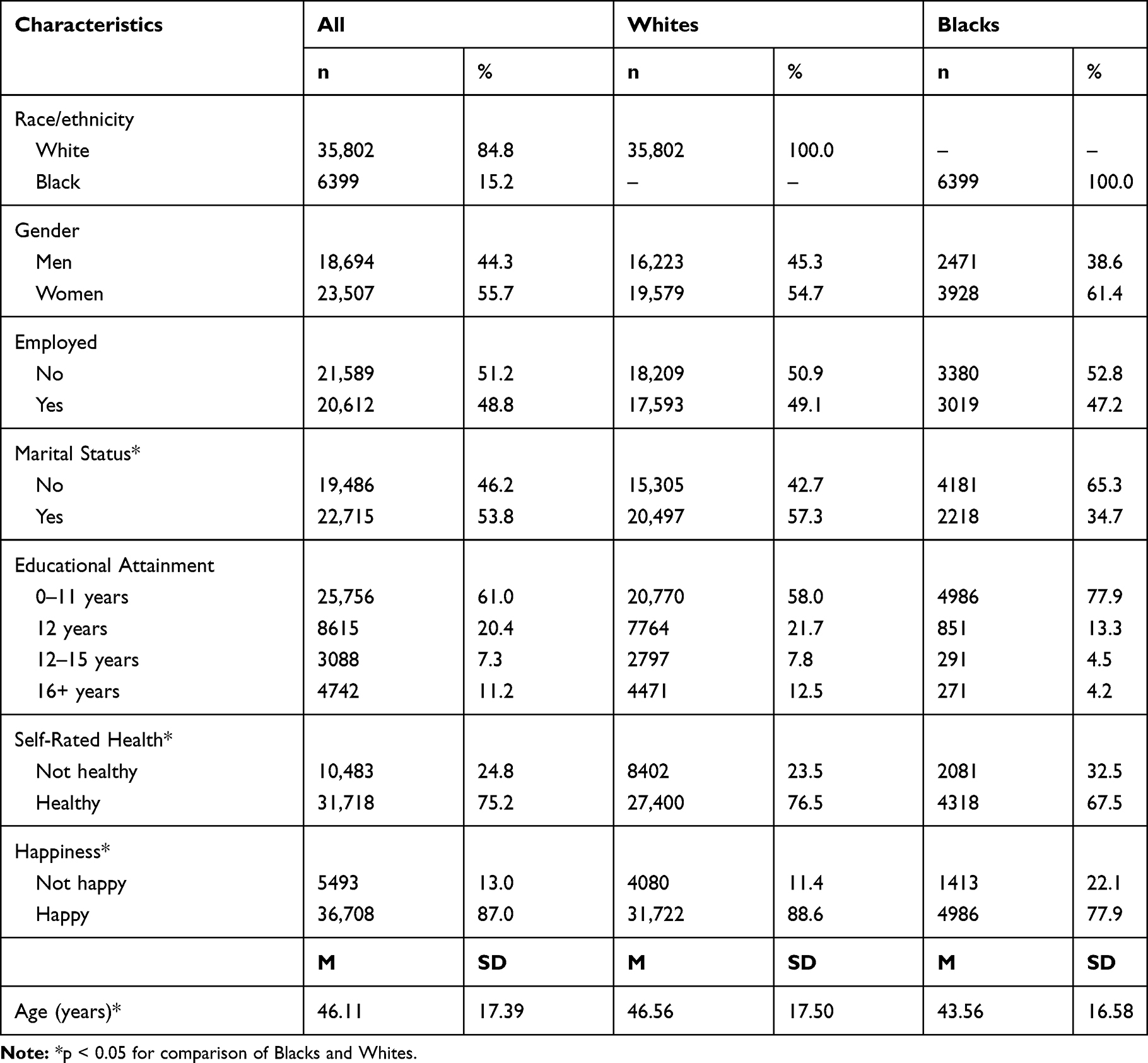 |
Table 2 Descriptive Statistics in the Overall Sample and by Race |
Multivariable Models (Pooled Sample)
Table 3 presents the summary of the results of our two logistic regression models with SRH, race, and covariates as the independent variables and happiness as the dependent variable. Both models were estimated in the overall sample. Model 1 only entered the main effects of SES indicators (educational attainment, employment, and marital status) while controlling for gender and covariates. Model 2, however, also added three interaction terms between gender and our SES indicators. Based on Model 1, good health was associated with lower odds of happiness (OR = 2.94; 95% CI = 2.76–3.14; p<0.001). Model 2, however, showed a statistically significant interaction between race/ethnicity and good SRH on odds of happiness (OR = 0.68; 95% CI = 0.59–0.79; P<0.001), suggesting that good SRH has a weaker boosting effect on the happiness of Blacks than Whites.
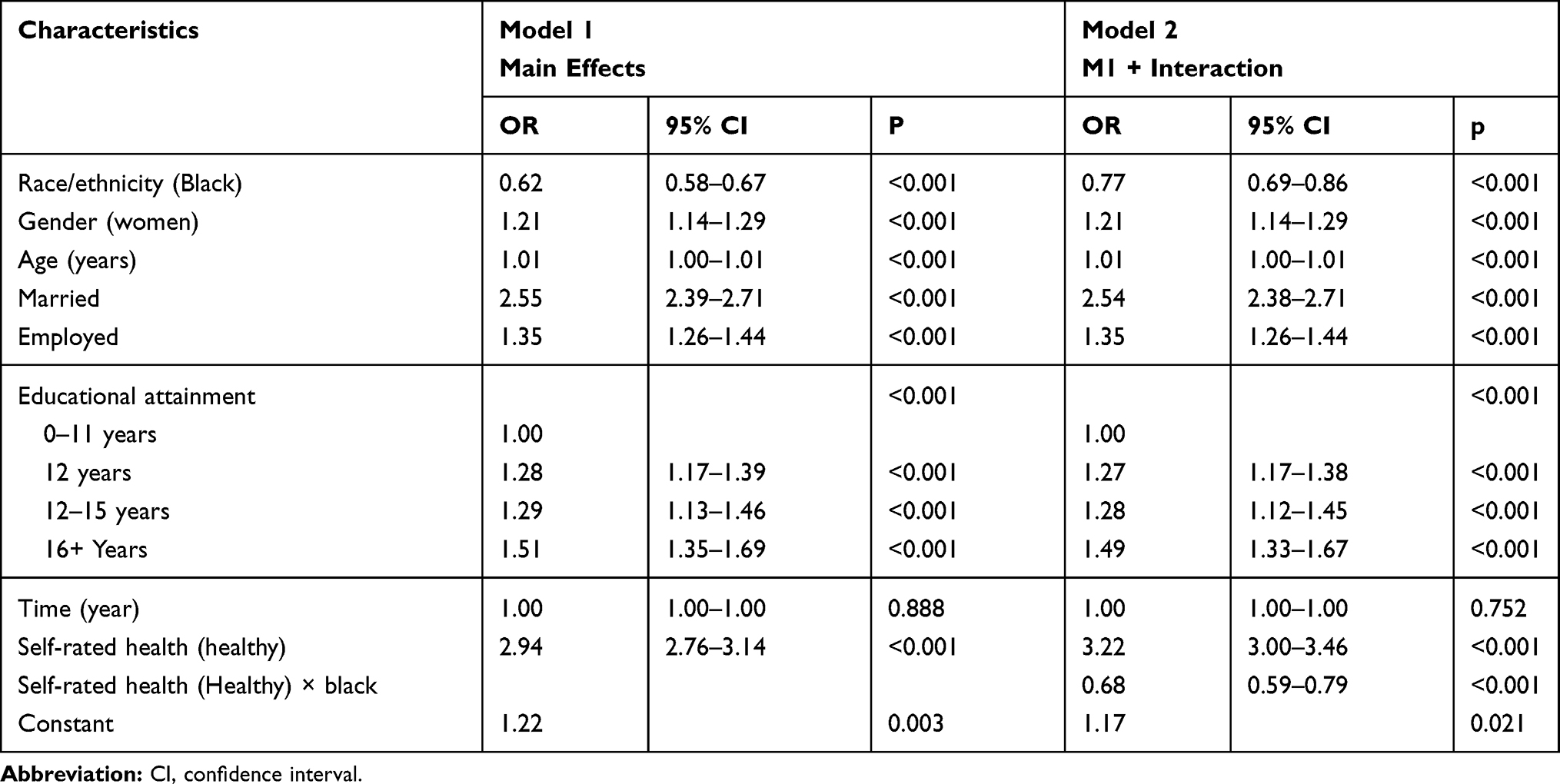 |
Table 3 Summary of Logistic Regressions on the Association Between Good Self-Rated Health and Happiness in the Pooled Sample |
Multivariable Models (Race/Ethnic-Specific Results)
Table 4 presents the summary of the results of race-stratified logistic regression models on the association between good SRH and happiness across races. Model 3 and Model 4 were performed in White and Black people, respectively. While in both races, good SRH was associated with happiness, the magnitude of this association was larger for Whites (OR = 3.18; 95% CI = 2.95–3.42 P<0.001) than Blacks (OR = 2.35; 95% CI =2.05–2.68 P<0.001). The difference in the magnitudes of these effects in terms of OR was about 20% (comparison of OR of 2.95 and 2.35 for Whites and Blacks, respectively).
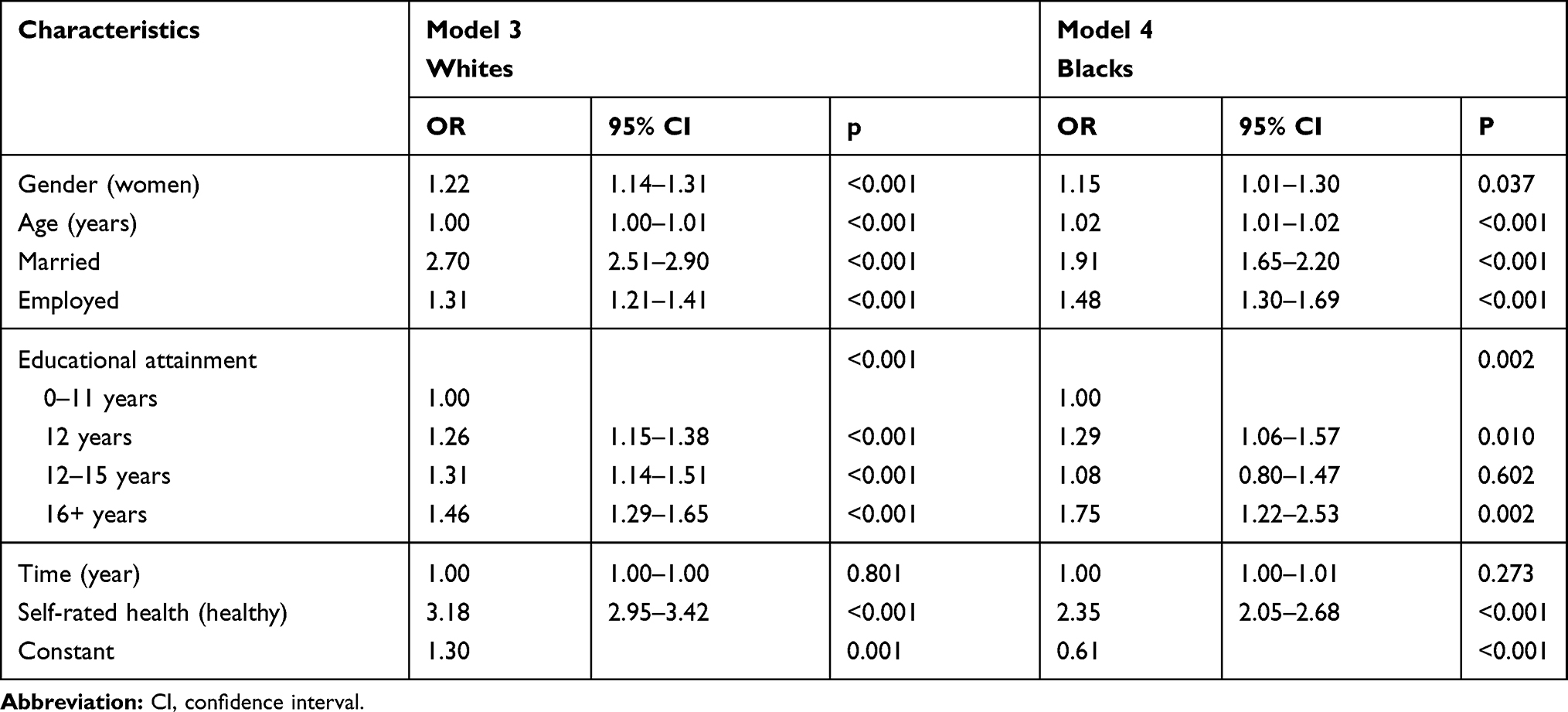 |
Table 4 Summary of Logistic Regressions on the Association Between Good Self-Rated Health and Happiness in Whites and Blacks |
Discussion
In the US, while health and happiness covary, this link differs by race/ethnicity. The concordance between health and happiness is weaker for Blacks than Whites. That means, the marginal return of health in terms of happiness is smaller for Blacks than Whites. In fact, the return of health in terms of happiness is approximately 20% less for Blacks than for Whites (OR = 2.35 vs OR = 2.95).
This study documented diminished returns of good health in generating happiness for Blacks compared to Whites. This finding is in line with the extensive literature on MDRs of SES on health of Blacks compared to Whites.19,20,47,48 Similar MDRs are shown for the health returns of positive coping.21 Finally, some studies have shown that high SES Blacks are more likely, not less likely, to be depressed.22–24,49–51 Thus, due to MDRs, a resource is less likely to generate positive outcomes for Blacks than Whites.52,53 In two independent studies, education and income generated more happiness and positive emotions for Whites than Blacks.32,45
Blacks with poor SRH can maintain happiness, while Whites with poor SRH lose more happiness. This study adds to the body of literature supporting the Black-White mental health paradox.26,28,54 Blacks have higher prevalence of chronic physical conditions, such as diabetes or hypertension, which may be influenced by racial inequalities and experiences with racism.54 However, this group remains very resilient despite having a lower SES and differential protective effects than Whites.35 Socioeconomic factors, such as higher self-rated health and perceived income, are acknowledged as being associated with happiness.55 Blacks who have been identified as happy are more likely to be married, employed and earn an annual salary of at least $30,000, which may show that there are certain social factors that influence mental well-being as opposed to health conditions.10
Interestingly, Blacks still possess higher level of happiness even when they have lower SRH. Similar to other minority groups, certain cultural factors, such as religiosity, of the Black population may increase resilience despite adverse events and discrimination.56,57 Among Blacks, the historical burden of oppression, discrimination, downward mobility, and economic hardship have resulted in high allostatic loads at birth and throughout their lifetime with protective cultural factors, such as supportive family relationships.58 Such resilience protects Blacks with high levels of psychosocial functioning in multiple domains, evidenced in this study with happiness, but leads to increased risk of infection.59
Blacks have faced high levels of racial discrimination, poorer SES, more health problems, and greater social inequities compared to other ethnic groups in the United States. Yet, this group exhibits lower rates of mental illness compared to Whites, indicating they have developed a form of hardiness.60 Hagiwara and colleagues found that perceived group level racial discrimination among Blacks was associated with better mental and physical status, but diminished with perceived personal-level racial discrimination.29 A negative association between poor health behaviors and stress has been found among Blacks, which may indicate that Blacks are protected from mental illnesses by engaging in risky behaviors.61 This may explain the stronger effect of happiness among Blacks compared to Whites but lead to concerns about their physical health status and well-being. For example, the cultural construct of the “strong Black women” (SBW) has assisted Black women to negate the direct effects of racial discrimination for centuries but has led to poor physical health effects.62,63 Some of the SBW factors include being emotionally contained, taking care of family and others, and being high achieving, which are pervasive among Blacks, regardless of SES factors.64 Another explanation can be lower level of expectation in Blacks when it comes to what they need to be happy compared to Whites. Also, Black culture (norm) may be more accepting of medical illnesses as they are more common than in the lives of White people.
These findings have important implications for healthcare practice and policy. For Whites, those who are less happy have poor SRH as well, so lower happiness may prompt providers to examine further health issues for Whites.65 However, such correlation is less meaningful in Blacks with high or low levels of happiness when it comes to clinical practice, because happiness is less informing of SRH of Blacks than Whites. Providers should be encouraged to utilize various measures when assessing the overall physical health status of Black people, using multi-item screening tools, as each one may not capture all of the data, given the lack of concordance between mental and physical health. In summary, reduced physical health seems to be more informing of possible mental health issues in Whites than Blacks. Also, there is potential evidence for less healthy coping mechanisms for stress in Black that may lead to the mismatch between happiness and medical illness.66 In this population, exploring and replacing those coping methods with more healthy ones seems to be an important preventive approach in primary care practice.
These findings underscore the importance of taking a multifaceted approach to understanding the physical health of Blacks who may express happiness despite having a poor SRH. This study calls for more attention to positive aspects of mental well-being among Blacks, such as resilience, as they maintain happiness even with diminished gains and racial discrimination compared to Whites. Studies that focus on examining different aspects of happiness should incorporate related SES factors in addition to resilience processes that are protecting this group from mental stress but leading to worsening physical health conditions. Further research needs to explore the effects of other SES factors (wealth and income) and lifestyle behaviors (spirituality) to fully account for the underlying factors of happiness among Blacks.
Limitations
This study had some methodological limitations. Similar to other studies with a cross-sectional design, our data do not allow causal inferences between race, physical health and happiness. We did not test variations of our findings based on other factors such as class, gender, and their interaction with race and ethnicity. We only tested differential effects by race/ethnicity. Future research may also include SES, class, and region. Despite these limitations, the results of the current study extend what is already known about racial differences in the well-being of American people. Last but not least, we used only one measure of happiness. Happiness can be seen and measured from multiple aspects, such as life, work, etc. Future research may test if these results replicate across domains of happiness. Finally, we did not break the sample based on age groups. The results may differ for young, middle aged, and older adults.67,68 A strength of our study was that we used data from GSS, a state-of-the-art study with results that are robust methodology, sampling, and very large sample size that increase our confidence in our results.69,70
Conclusion
In the United States, there is a relative discordance between good SRH and happiness in Black than White Americans. This discordance may allow Blacks to maintain happiness in the absence of health, which reflects mental resilience and is in line with the Black-White mental health paradox. In line with minorities’ diminished returns, physical health may have lost some of its utility in generating happiness for Blacks compared to Whites. The final possibility is that happiness and SRH have different meanings for Black and White people. All these hypotheses and explanations require additional research on the complex interplay between race/ethnicity, adversities, health problems, and mental well-being.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
Research reported in this publication was supported by the 495 following National Institutes of Health (NIH) awards: S21MD000103, U54CA229974, U54MD008149, R25 MD007610, U54MD007598, U54 TR001627, and CA201415-02.
Disclosure
The authors declare no conflict of interest in this work.
References
1. Scott KM, Lim C, Al-Hamzawi A, et al. Association of mental disorders with subsequent chronic physical conditions: world mental health surveys from 17 countries. JAMA Psychiatry. 2016;73(2):150–158. doi:10.1001/jamapsychiatry.2015.2688
2. Freeman HP. The origin, evolution, and principles of patient navigation. Cancer Epidemiol Biomarkers Prev. 2012;21(10):1614–1617. doi:10.1158/1055-9965.EPI-12-0982
3. Dfarhud D, Malmir M, Khanahmadi M. Happiness & health: the biological factors- systematic review article. Iran J Public Health. 2014;43(11):1468–1477.
4. Luchesi BM, de Oliveira NA, de Morais D, de Paula Pessoa RM, Pavarini SCI, Chagas MHN. Factors associated with happiness in the elderly persons living in the community. Arch Gerontol Geriatr. 2018;74:83–87. doi:10.1016/j.archger.2017.10.006
5. Ohrnberger J, Fichera E, Sutton M. The relationship between physical and mental health: a mediation analysis. Soc Sci Med. 2017;195:42–49. doi:10.1016/j.socscimed.2017.11.008
6. Ohrnberger J, Fichera E, Sutton M. The dynamics of physical and mental health in the older population. J Econ Ageing. 2017;9:52–62. doi:10.1016/j.jeoa.2016.07.002
7. Bayat N, Alishiri GH, Salimzadeh A, et al. Symptoms of anxiety and depression: a comparison among patients with different chronic conditions. J Res Med Sci. 2011;16(11):1441–1447.
8. Erving CL. Physical-psychiatric comorbidity: patterns and explanations for ethnic group differences. Ethn Health. 2018;23(6):583–610. doi:10.1080/13557858.2017.1290216
9. Nobles CJ, Valentine SE, Borba CPC, Gerber MW, Shtasel DL, Marques L. Black-white disparities in the association between posttraumatic stress disorder and chronic illness. J Psychosom Res. 2016;85:19–25. doi:10.1016/j.jpsychores.2016.03.126
10. Mwinnyaa G, Porch T, Bowie J, Thorpe RJ. The association between happiness and self-rated physical health of African American men: a population-based cross-sectional study. American Journal of Men’s Health. 2018;12(5):1615–1620. doi:10.1177/1557988318780844
11. Assari S. High income protects Whites but not African Americans against risk of depression. Healthcare (Basel). 2018;6(2):37. doi:10.3390/healthcare6020037
12. Assari S, Bazargan M. Unequal effects of educational attainment on workplace exposure to second-hand smoke by race and ethnicity; minorities’ diminished returns in the National Health Interview Survey (NHIS). J Med Res Innov. 2019;3(2):e000179. doi:10.32892/jmri.179
13. Bethea TN, Palmer JR, Rosenberg L, Cozier YC. Neighborhood socioeconomic status in relation to all-cause, cancer, and cardiovascular mortality in the Black Women’s Health Study. Ethn Dis. 2016;26(2):157–164. doi:10.18865/ed.26.2.157
14. Assari S, Smith J, Mistry R, Farokhnia M, Bazargan M. Substance use among economically disadvantaged African American older adults; objective and subjective socioeconomic status. Int J Environ Res Public Health. 2019;16(10):1826. doi:10.3390/ijerph16101826
15. Assari S. The benefits of higher income in protecting against chronic medical conditions are smaller for African Americans than Whites. Healthcare (Basel). 2018;6(1):2. doi:10.3390/healthcare6010002
16. Assari S. Parental education attainment and educational upward mobility; role of race and gender. Behav Sci (Basel). 2018;8(11):107. doi:10.3390/bs8110107
17. Assari S. Blacks’ diminished return of education attainment on subjective health; mediating effect of income. Brain Sci. 2018;8(9):176. doi:10.3390/brainsci8090176
18. Lankarani MM, Assari S. Positive and negative affect more concurrent among Blacks than Whites. Behav Sci (Basel). 2017;7(4):48. doi:10.3390/bs7030048
19. Assari S, Caldwell CH, Mincy R. Family socioeconomic status at birth and youth impulsivity at age 15; Blacks’ diminished return. Children (Basel). 2018;5(5):58.
20. Assari S, Thomas A, Caldwell CH, Mincy RB. Blacks’ diminished health return of family structure and socioeconomic status; 15 years of follow-up of a national urban sample of youth. J Urban Health. 2018;95(1):21–35. doi:10.1007/s11524-017-0217-3
21. Assari S. General self-efficacy and mortality in the USA; racial differences. J Racial Ethn Health Disparities. 2017;4(4):746–757. doi:10.1007/s40615-016-0278-0
22. Assari S, Caldwell CH. High risk of depression in high-income African American boys. J Racial Ethn Health Disparities. 2018;5(4):808–819. doi:10.1007/s40615-017-0426-1
23. Assari S. Does school racial composition explain why high income Black youth perceive more discrimination? A gender analysis. Brain Sci. 2018;8(8):140. doi:10.3390/brainsci8080140
24. Assari S, Lankarani MM, Caldwell CH. Does discrimination explain high risk of depression among high-income African American men? Behav Sci (Basel). 2018;8(4):40.
25. Assari S, Burgard S, Zivin K. Long-term reciprocal associations between depressive symptoms and number of chronic medical conditions: longitudinal support for Black-White health paradox. J Racial Ethn Health Disparities. 2015;2(4):589–597. doi:10.1007/s40615-015-0116-9
26. Keyes CLM. The Black-White paradox in health: flourishing in the face of social inequality and discrimination. J Pers. 2009;77(6):1677–1706. doi:10.1111/j.1467-6494.2009.00597.x
27. Assari S, Lankarani MM. Chronic medical conditions and negative affect; racial variation in reciprocal associations over time. Front Psychiatry. 2016;7:140. doi:10.3389/fpsyt.2016.00140
28. Louie P, Wheaton B. The Black-White paradox revisited: understanding the role of counterbalancing mechanisms during adolescence. J Health Soc Behav. 2019;60(2):169–187. doi:10.1177/0022146519845069
29. Hagiwara N, Alderson CJ, Mezuk B. Differential effects of personal-level vs group-level racial discrimination on health among Black Americans. Ethn Dis. 2016;26(3):453–460. doi:10.18865/ed.26.3.453
30. Assari S, Burgard S. Black-White differences in the effect of baseline depressive symptoms on deaths due to renal diseases: 25 year follow up of a nationally representative community sample. J Renal Inj Prev. 2015;4(4):127–134. doi:10.12861/jrip.2015.27
31. Jackson JS, Knight KM, Rafferty JA. Race and unhealthy behaviors: chronic stress, the HPA axis, and physical and mental health disparities over the life course. Am J Public Health. 2010;100(5):933–939. doi:10.2105/AJPH.2008.143446
32. Assari S. Race, education attainment, and happiness in the United States. Int J Epidemiol Res. 2019;6(2):76. doi:10.15171/ijer.2019.14
33. Assari S. Psychiatric disorders differently correlate with physical self-rated health across ethnic groups. J Pers Med. 2017;7(4):6. doi:10.3390/jpm7040006
34. Assari S, Lankarani MM. Demographic and socioeconomic determinants of physical and mental self-rated health across 10 ethnic groups in the United States. Int J Epidemiol Res. 2017;3(12):185–193. doi:10.15171/ijer.2017.02
35. Assari S, Lapeyrouse LM, Neighbors HW. Income and self-rated mental health: diminished returns for high income Black Americans. Behav Sci (Basel). 2018;8(5):50.
36. Assari S. Ethnic groups differ in how poor self-rated mental health reflects psychiatric disorders. J Racial Ethn Health Disparities. 2018;5(4):728–736. doi:10.1007/s40615-017-0417-2
37. Assari S, Lankarani MM, Burgard S. Black-white difference in long-term predictive power of self-rated health on all-cause mortality in United States. Ann Epidemiol. 2016;26(2):106–114. doi:10.1016/j.annepidem.2015.11.006
38. Mitchell JA, Watkins DC, Shires D, Chapman RA, Burnett J. Clues to the blues: predictors of self-reported mental and emotional health among older African American men. Am J Men’s Health. 2017;11(5):1366–1375. doi:10.1177/1557988315600064
39. Geronimus AT, Hicken M, Keene D, Bound J. “Weathering” and age patterns of allostatic load scores among blacks and whites in the United States. Am J Public Health. 2006;96(5):826–833. doi:10.2105/AJPH.2004.060749
40. Howard JT, Sparks PJ. The role of education in explaining racial/ethnic allostatic load differentials in the United States. Biodemography Soc Biol. 2015;61(1):18–39. doi:10.1080/19485565.2014.937000
41. Farmer MM, Ferraro KF. Are racial disparities in health conditional on socioeconomic status? Soc Sci Med. 2005;60(1):191–204. doi:10.1016/j.socscimed.2004.04.026
42. Assari S. Family socioeconomic position at birth and school bonding at age 15; Blacks’ diminished returns. Behav Sci (Basel). 2019;9(3)26.
43. Assari S, Bazargan M. Minorities’ diminished returns of educational attainment on hospitalization risk: national health interview survey (NHIS). Hosp Pract Res. 2019;4(3):86–91. doi:10.15171/hpr.2019.17
44. Assari S, Chalian H, Bazargan M. High education level protects European Americans but not African Americans against chronic obstructive pulmonary disease: national health interview survey. Int J Biomed Eng Clin Sci. 2019;5(2):16–23. doi:10.11648/j.ijbecs.20190502.12
45. Assari S, Preiser B, Kelly M. Education and income predict future emotional well-being of Whites but not Blacks: a ten-year cohort. Brain Sci. 2018;8(7):122. doi:10.3390/brainsci8070122
46. Idler EL, Benyamini Y. Self-rated health and mortality: a review of twenty-seven community studies. J Health Soc Behav. 1997;38(1):21–37. doi:10.2307/2955359
47. Assari S, Boyce S, Bazargan M, Mincy R, Caldwell CH. Unequal protective effects of parental educational attainment on the body mass index of Black and White youth. Int J Environ Res Public Health. 2019;16(19):3641. doi:10.3390/ijerph16193641
48. Assari S, Caldwell CH, Mincy RB. Maternal educational attainment at birth promotes future self-rated health of White but not Black youth: a 15-year cohort of a national sample. J Clin Med. 2018;7(5):93. doi:10.3390/jcm7050093
49. Assari S. Combined racial and gender differences in the long-term predictive role of education on depressive symptoms and chronic medical conditions. J Racial Ethn Health Disparities. 2017;4(3):385–396. doi:10.1007/s40615-016-0239-7
50. Assari S, Gibbons FX, Simons R. Depression among Black youth; interaction of class and place. Brain Sci. 2018;8(6):108. doi:10.3390/brainsci8060108
51. Assari S, Moghani Lankarani M. Workplace racial composition explains high perceived discrimination of high socioeconomic status African American men. Brain Sci. 2018;8(8):139. doi:10.3390/brainsci8080139
52. Assari S. Health disparities due to diminished return among Black Americans: public policy solutions. Soc Issues Policy Rev. 2018;12(1):112–145. doi:10.1111/sipr.12042
53. Assari S. Unequal gain of equal resources across racial groups. Int J Health Policy Manag. 2018;7(1):1–9. doi:10.15171/ijhpm.2017.90
54. Veenstra G, Patterson AC. Black-White health inequalities in Canada. J Immigr Minor Health. 2016;18(1):51–57. doi:10.1007/s10903-014-0140-6
55. Weech-Maldonado R, Miller MJ, Lord JC. The relationships among socio-demographics, perceived health, and happiness. Appl Res Qual Life. 2017;12(2):289–302. doi:10.1007/s11482-017-9517-8
56. Gallo LC, Penedo FJ, Espinosa de Los Monteros K, Arguelles W. Resiliency in the face of disadvantage: do Hispanic cultural characteristics protect health outcomes? J Pers. 2009;77(6):1707–1746. doi:10.1111/j.1467-6494.2009.00598.x
57. Yang I, Hall LA, Ashford K, Paul S, Polivka B, Ridner SL. Pathways from socioeconomic status to prenatal smoking: a test of the reserve capacity model. Nurs Res. 2017;66(1):2–11. doi:10.1097/NNR.0000000000000191
58. Brody GH, Yu T, Beach SRH. Resilience to adversity and the early origins of disease. Dev Psychopathol. 2016;28(4pt2):1347–1365. doi:10.1017/S0954579416000894
59. Miller GE, Cohen S, Janicki-Deverts D, Brody GH, Chen E. Viral challenge reveals further evidence of skin-deep resilience in African Americans from disadvantaged backgrounds. Health Psychol. 2016;35(11):1225–1234. doi:10.1037/hea0000398
60. Williams AM. Distress and hardiness: a comparison of African-American and white caregivers. J Natl Black Nurses Assoc. 2000;11(1):21–26.
61. Mezuk B, Rafferty JA, Kershaw KN, et al. Reconsidering the role of social disadvantage in physical and mental health: stressful life events, health behaviors, race, and depression. Am J Epidemiol. 2010;172(11):1238–1249. doi:10.1093/aje/kwq283
62. Etowa JB, Beagan BL, Eghan F, Bernard WT. “You feel you have to be made of steel”: the strong Black woman, health, and well-being in Nova Scotia. Health Care Women Int. 2017;38(4):379–393. doi:10.1080/07399332.2017.1290099
63. Watson NN, Hunter CD. “I had to be strong”: tensions in the strong Black woman schema. J Black Psychol. 2016;42(5):424–452. doi:10.1177/0095798415597093
64. Nelson T, Cardemil EV, Adeoye CT. Rethinking strength: Black women’s perceptions of the “strong Black woman” role. Psychol Women Q. 2016;40(4):551–563. doi:10.1177/0361684316646716
65. Hall WJ, Chapman MV, Lee KM, et al. Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: a systematic review. Am J Public Health. 2015;105(12):e60–e76. doi:10.2105/AJPH.2015.302903
66. Ellis KR, Griffith DM, Allen JO, Thorpe RJ, Bruce MA. “If you do nothing about stress, the next thing you know, you’re shattered”: perspectives on African American men’s stress, coping and health from African American men and key women in their lives. Soc Sci Med. 2015;139:107–114. doi:10.1016/j.socscimed.2015.06.036
67. Xu X, Huang X, Zhang X, Chen L. Family economic burden of elderly chronic diseases: evidence from China. Healthcare (Basel). 2019;7(3):99.
68. Xu X, Chen L. Influencing factors of disability among the elderly in China, 2003–2016: application of Bayesian quantile regression. J Med Econ. 2019;22(6):605–611. doi:10.1080/13696998.2019.1600525
69. Tourangeau R, Yan T, Sun H, Hyland A, Stanton CA. Population Assessment of Tobacco and Health (PATH) reliability and validity study: selected reliability and validity estimates. Tob Control. 2018;28(6):663–8.
70. Hyland A, Ambrose BK, Conway KP, et al. Design and methods of the Population Assessment of Tobacco and Health (PATH) study. Tob Control. 2017;26(4):371–378. doi:10.1136/tobaccocontrol-2016-052934
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.