Back to Journals » Therapeutics and Clinical Risk Management » Volume 11
Pulmonary hypertension: diagnostic and therapeutic challenges
Received 18 April 2015
Accepted for publication 16 June 2015
Published 17 August 2015 Volume 2015:11 Pages 1221—1233
DOI https://doi.org/10.2147/TCRM.S74881
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Isabel S Bazan, Wassim H Fares
Department of Internal Medicine, Section of Pulmonary, Critical Care and Sleep Medicine, Yale University, New Haven, CT, USA
Abstract: Pulmonary hypertension (PH) is a hemodynamic and pathophysiologic state that can be found in multiple conditions with associated symptoms of dyspnea, decreased exercise tolerance, and progression to right heart failure. The World Health Organization has classified PH into five groups. The first group is pulmonary arterial hypertension (PAH), which can be idiopathic, heritable, due to drugs and toxins, or associated with conditions such as connective tissue diseases, congenital heart disease, portal hypertension, and others. The development of PAH is believed to result from smooth muscle cells and endothelial dysfunction that impairs production of vasodilators, including nitric oxide and prostacyclin. The importance of distinguishing this group from the other groups of PH is that there are PAH-specific drugs that target the molecular pathways that are pathogenic in the vascular derangements, leading to arterial hypertension, which should not be used in the other forms of PH. Other groups of PH include PH due to left heart disease, lung disease, chronic thromboembolic disease, as well as a miscellaneous category. Echocardiography is used to screen for PH and has varying sensitivity and specificity in detecting PH. Additionally, the right heart pressures estimated during echocardiogram often differ from those obtained during confirmatory testing with right heart catheterization. The most challenging PH diagnosis is in a case that does not fit one group of PH, but meets criteria that overlap between several groups. This also makes the treatment challenging because each group of PH is managed differently. This review provides an overview of the five groups of PH and discusses the diagnostic and therapeutic challenges of each.
Keywords: pulmonary hypertension, pulmonary arterial hypertension, right heart failure, diagnosis, management
Introduction
Pulmonary hypertension (PH) is a hemodynamic and pathophysiologic state that can be found in multiple clinical conditions. It is defined as a mean pulmonary artery pressure (mPAP) of 25 mm Hg or greater at rest. Symptoms typically include shortness of breath, decreased exercise tolerance, and eventually heart failure. The World Health Organization (WHO) has classified PH into five categories based on etiologic and pathophysiologic groupings (Table 1).1 The most common cause of PH is left heart dysfunction,2 causing WHO group 2 PH. Lung disease associated PH is also a common cause, classified as WHO group 3 PH. Chronic thromboembolic PH, classified as WHO group 4 PH, is an important cause of PH as it is potentially curable. All other causes of PH, which do not clearly fit any of the first four WHO groups of PH, are lumped together into WHO group 5 PH.
 | Table 1 WHO groups of pulmonary hypertension |
Pulmonary arterial hypertension (PAH) is a clinical condition that falls under WHO group 1 and can be idiopathic (IPAH), heritable (HPAH) due to drugs and toxins, or associated PAH (APAH). APAH occurs in the setting of a variety of conditions such as connective tissue disease (CTD), congenital heart disease (CHD), portal hypertension, or HIV infection. PAH leads to progressive increase in pulmonary vascular resistance (PVR) and eventually a decrease in cardiac output, leading to right heart failure and death.
The pathophysiology of PAH is complex but it involves molecular mechanisms of endothelial dysfunction that impair production of vasodilators including nitric oxide (NO) and prostacyclin. In addition, there is an overexpression of vasoconstrictors such as endothelin. These molecular derangements affect vascular tone and promote pathological vascular remodeling, which leads to pulmonary arterial vasoconstriction, medial hypertrophy, intimal proliferation and fibrosis, in-situ thrombosis, and occasionally complex plexiform lesions.3 As the disease progresses, vascular remodeling and fibrosis eventually cause right ventricular dilation and failure.4
WHO group 1 PH: PAH
This PH group includes IPAH, HPAH, PH due to drugs and toxins, and APAH. These were all grouped together because they share similar clinical and histopathologic characteristics.1 The hemodynamic characterization of this group is a mPAP of ≥25 mm Hg at rest, a pulmonary artery wedge pressure (PAWP) of ≤15 mm Hg, and a PVR of ≥3 Wood units. Pathologic lesions of PAH affect the whole pulmonary circulation, particularly the distal pulmonary arteries, although PAH has also been associated with the systemic circulation.1 The pulmonary vasculature in PAH is characterized by medial hypertrophy, intimal proliferative/fibrotic changes, adventitial thickening with moderate perivascular inflammatory infiltrates, in situ thrombotic lesions, and occasionally plexiform lesions.5
Diagnosis
The diagnostic approach to PAH is the same for all PH etiologies, and it is suspected to be based on the patient’s history and physical exam, screened by an echocardiogram, and confirmed by a right heart catheterization (RHC), which is the gold standard. Echocardiography provides a noninvasive screening method for PH; however, it has been demonstrated that there is frequently limited agreement between pulmonary artery systolic pressure (PASP) as estimated by echocardiography and RHC measurements. The accuracy of echocardiography in estimating PASP is 50%.6,7
In patients whose clinical picture is highly suggestive of PAH, echocardiography may not be sufficient to rule out PAH. Spectral Doppler is used to determine the peak velocity of the tricuspid regurgitant (TR) jet, which can be entered into modified Bernoulli equation to estimate the PASP. This estimate may be unreliable if the peak TR velocity cannot be determined because there is minimal tricuspid regurgitation, an eccentric jet, a very large jet, or if the TR jet “envelope” on Doppler is incomplete because of technical reasons. A low PASP on echo is not adequate enough to exclude the diagnosis of PAH. Other echo findings such as right ventricular enlargement, hypertrophy, or systolic dysfunction, right atrial enlargement, characteristic pulmonic valve motion, interventricular septal wall motion in systole, and certain spectral Doppler characteristics should be considered.8
The gold standard for hemodynamic evaluation remains the RHC, and it is mandatory before the initiation of any PAH-specific therapy. Maneuvers to exclude occult left-sided diastolic dysfunction, such as fluid challenge or exercise, may be performed in patients with risk factors like older age, left atrial enlargement, left ventricular hypertrophy, diabetes, or hypertension. Unless contraindicated (eg, because of systemic hypotension or decreased cardiac output), an acute vasodilator challenge should be performed during the RHC for all PAH patients, both to assess prognosis and to identify the rare patients who may respond to calcium channel blockers (CCBs). A suggestive algorithm for the diagnosis of PH is shown in Figure 1.
 | Figure 1 Diagnostic approach to pulmonary hypertension. |
Treatment
The goals for treating PAH are to improve patient symptoms, enhance functional capacity, and, if possible, reverse or slow the progression of the disease and prolong life. Treatment options for PAH have evolved considerably in the past decade, given the increasing knowledge of the pathophysiology of the disease. The management incorporates supportive therapy, specific drug therapy, and psychosocial support.
Supportive therapy for PAH includes several therapies that have limited controlled trial data, but nevertheless have been found to be beneficial.9 Hypoxemia can worsen pulmonary vasoconstriction, and oxygen supplementation has been shown to reduce PVR. Many PAH patients present with or progress to right heart failure with subsequent fluid retention, hepatic congestion, ascites, and peripheral edema. Understandably, there is symptomatic benefit of using diuretics to manage volume overload. Adding spironolactone may have a long-term beneficial effect in PAH.10,11 Digoxin may also be considered in patients with acute right heart failure and for chronic management to reduce symptoms of heart failure.12 Some observational studies suggested an improved survival with warfarin. Current guidelines recommend the use of anticoagulation in PAH patients with advanced disease, with a titration to an international normalized ratio of 1.5–2.5.12 However, the bleeding risk is prohibitive in patients with liver disease, CTD, and CHD.
Specific drug therapy
PAH patients who exhibit an acute vasodilator response during the diagnostic RHC have a very good overall prognosis.13 However, very few patients exhibit this response. Those who do respond should be managed with CCBs and careful long-term monitoring for signs of worsening PAH. If worsening PAH ensues, which is not uncommon in “responders”, other PAH-specific therapies should be considered. A summary of treatment options for all groups of PH is shown in Table 2.
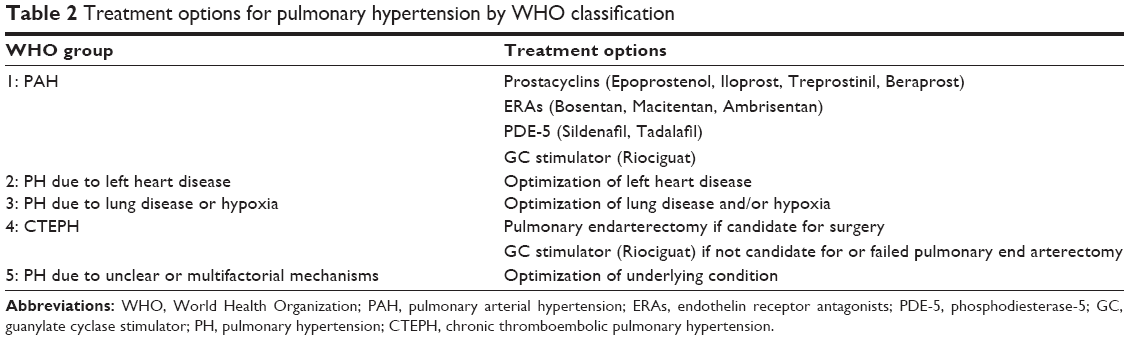 | Table 2 Treatment options for pulmonary hypertension by WHO classification |
PAH-specific treatment options target three main molecular pathways that are pathogenic in PAH vascular derangements.14
Prostanoids work via a cyclic AMP-mediated relaxation of vascular smooth muscle, leading to pulmonary artery vasodilation.15 Epoprostenol is a synthetic prostacyclin that is administered intravenously and continuously via infusion pump because of its short half-life. Epoprostenol has been shown to improve symptoms, exercise capacity, and hemodynamics in IPAH and scleroderma APAH16–18 and is also efficacious for other APAH subtypes. Epoprostenol has even been shown to have a survival benefit.17 Treprostinil has a longer half-life and is available in infused (both intravenous and subcutaneous routes), inhaled, and oral formulations.19–21 Iloprost is also an available inhaled prostanoid analog, but requires six to nine times daily dosing that is not convenient to some patients.
The success of infused prostanoid analogs comes with challenges: Pump failure, local catheter site infection or pain (especially for the subcutaneous route), catheter-related venous thrombosis (for the intravenous route), and sepsis. Abrupt cessation of prostanoid analogs infusion is potentially fatal as it leads to rebound PH.5 This is especially a challenge if patients underestimate the effect of missing some doses of an oral prostanoid.22
Endothelin receptor antagonists (ERAs) work by inhibiting endothelin-1, which is a potent vasoconstrictor and pro-inflammatory molecule, typically overexpressed in PAH. The three FDA approved ERAs are Bosentan, Ambrisentan, and Macitentan.23 These oral therapies have been shown to improve hemodynamics, exercise tolerance, and prevent clinical worsening, with varying levels of evidence and study designs.24–26 Liver function tests must be monitored indefinitely for Bosentan on a monthly basis due to the risk of hepatotoxicity.12 Monthly pregnancy tests are required for all PAH female patients with childbearing potential taking ERAs.
Phosphodiesterase (PDE-5) inhibitors work by preventing PDE-5 from impairing the cyclic GMP-mediated vasodilatory function of NO.27 Sildenafil, also used for the treatment of erectile dysfunction, has been shown to improve exercise tolerance and improve functional class in PAH.12 Tadalafil improves exercise tolerance and time to clinical worsening.28 Side effects of these medications include headache, flushing, dyspepsia, and epistaxis.12
A relatively new class of drug, guanylate cyclase stimulators (GCs), works in synergy with endogenous NO, while directly stimulating guanylate cyclase, and thus increasing cyclic-GMP, theoretically working in the absence of NO. Riociguat significantly improved exercise capacity, hemodynamics, WHO functional class, and time to clinical worsening in PAH patients. This was tested in patients simultaneously receiving other PAH-specific therapy, as well as those not on PAH treatment.29 Overall, GCs are another oral option for the treatment of PAH that can be used in conjunction with ERAs, but are contraindicated with PDE-5 inhibitors because of the concern about systemic hypotension.
In general, patients with advanced PAH (eg, those with functional class III or IV heart failure have pericardial effusion, syncope or presyncope, or with elevated Registry to Evaluate Early And Long-term PAH disease management (REVEAL) risk score30) should be initiated on parenteral therapy (prostanoids), while patients with less severe PAH may start with the oral options (ERAs and/or PDE-5 inhibitors/GCs). There is also data supporting the use of both sequential and upfront combination therapy.31,32
One major challenge in the management of PAH is the limited number of RCTs that study all PAH etiologies. Most trials are primarily done with IPAH and CTD-PAH, and to a lesser extent anorexigen-induced PAH. As exemplified in the PATENT-1 trial, few are done with HIV and CHD patients. Another challenge is that the RCT-documented degree of clinical benefit of these medications is limited. There is no human evidence that these medications reverse the vascular remodeling that is characteristic of PAH, and many patients remain symptomatic with a suboptimal quality of life.
Of note, the PAH-specific drugs that have been mentioned are currently approved for the treatment of PAH, not for patients with other causes of PH (ie, WHO groups 2–5). In some cases, these medications may cause harm.33 For this reason, their use in treating non-PAH PH is not supported.34 One exception is Riociguat, which is also approved for treatment of chronic thromboembolic pulmonary hypertension (CTEPH) patients (WHO group 4 PH) who are not surgical candidates, or failed pulmonary endarterectomy.
Despite advances in medical therapy for PAH, many patients have progressive disease and referral for transplant should be considered. Lung transplant or heart/lung transplant has shown to improve outcomes; however, the major limitation is chronic rejection,35 as well as the limited availability of organs.
Specific PAH subgroups
Idiopathic PAH
There are no comparative epidemiological data on the prevalence of PH. Recent registries estimated the prevalence of IPAH at 30%–50% of all PAH, or 15 cases per million of the general population.36 In the French registry, 39% of PAH patients had IPAH and 3.9% with PAH family history.37 IPAH corresponds to sporadic disease, without any family history or clearly identified hereditary or triggering factor of PAH.
Heritable PAH
The previously termed familial PAH was changed to HPAH because specific gene mutations have been identified in sporadic cases with no family history. Heritable forms of PAH include clinically sporadic IPAH with germ line mutations and clinical familial cases with or without identified germ line mutations. If genetic testing is to be done, appropriate genetic counseling is mandatory prior to testing. Most HPAH (75%) is caused by a mutation in the bone-morphogenetic protein receptor-2 (BMPR2) gene.38 Mutations in other genes, such as BMPR1B, CAV1, ENG, SMAD9, are less common.39,40 Mutations are identified in upto 25% of individuals without a contributory family history.40 HPAH has identical symptoms, signs and histology, as IPAH. The time from the onset of symptoms to diagnosis may be shorter in individuals with familial PAH because of familial awareness of the disease. Some studies suggest that BMPR2 mutation exhibits more severe disease. BMPR2-associated HPAH is inherited in an autosomal dominant manner, but the average penetrance is approximately 20%,41 which makes genetic counseling complex.
The diagnosis of HPAH is made in the presence of two or more family members with PAH for the identification of a genetic mutation known to cause PAH, such as BMPR2.
Drug and toxin induced PAH
Several drugs and toxins have been identified as risk factors for PAH, with varying degrees of strength in their association. There is a definite association between appetite suppressants (aminorex, fenfluramine derivatives) and PAH,1 and many have been withdrawn from the market. These medications may act through interactions with the serotonin transporter located on pulmonary artery smooth muscle cells, increasing serotonin levels and stimulating smooth muscle cell growth, or altering the expression of the transporter.42
Amphetamines, phentermine, and mazindol were also implicated but still considered likely risk factors. Dasatinib, a dual Src/Abl kinase inhibitor, that is used in the treatment of chronic myelogenous leukemia has been associated with severe PAH, but is at least partially reversible if the offending agent is stopped. Recent observational (with potentially confounding biases) studies have raised concerns about endothelial dysfunction that could be induced by interferon. Possible associations have been implicated for cocaine, selective serotonin reuptake inhibitors, and other drugs with limited data.5,43
CTD-associated PAH
PAH has a clear association with CTD. The most commonly affected CTD is systemic sclerosis (SSc, or scleroderma), although most other CTD are also associated with PAH. The prevalence of PAH in scleroderma is ~10%–12%.12,44 There seems to be an increased risk of developing PAH in older SSc patients44 or those with the limited form of SSc as opposed to those with diffuse skin disease; however, all subsets can be affected.
The reported prevalence of PAH in systemic lupus erythematous (SLE) is also estimated at ~11%, but with very wide range depending on the study.45,46 The incidence of PAH in other CTDs is elevated but still fairly rare.44 There is also significantly less literature on these subgroups. REVEAL is a multicenter, observational, US-based registry study of PAH that was designed to characterize the PAH population. Results from the REVEAL registry found that 25% of patients with WHO group 1 PH had CTD-PAH.46,47
In addition to an increased prevalence of PAH, those with CTD-PAH also have a greater degree of morbidity and mortality than those with other forms of PAH. According to the REVEAL study, the 1-year survival rate of patients with CTD-PAH compared with IPAH was worse (86% vs 93%), with scleroderma-PAH faring worse at 82%.48 This worse prognosis in CTD-PAH persists beyond the first year.
The antibody profile of CTD patients may be helpful in predicting PAH development. In scleroderma, the presence of U3RNP/fibrillarin antibodies or anticentromere antibodies is associated with an increased risk of developing PAH, whereas anti-topoisomerase (Scl-70) antibodies seem to be protective.49 For SLE, increased anti-endothelial cell antibodies, anti-cardiolipin antibody, and anti-ribonucleoprotein antibody have all shown positive correlation with PAH diagnosis.50 Whether or not any of these antibodies has a direct correlation to PAH development is unclear.51
There are many diagnostic challenges associated with CTD-PAH, including the number of comorbidities associated with these rheumatologic conditions. For example, those with scleroderma often have coexisting interstitial lung disease (ILD), left heart disease with preserved ejection fraction (diastolic dysfunction), pulmonary veno-occlusive disease, musculoskeletal abnormalities, and kidney disease, which can all have overlapping signs and symptoms of PAH.44 Another challenge is eliciting PAH symptoms. An early symptom of PAH is exertional dyspnea; however, many patients with CTD have also decreased activity levels secondary to musculoskeletal manifestations of CTD. Due to the relatively high PAH incidence in scleroderma and the difficulty in eliciting typical symptoms, it is recommended to screen scleroderma patients regularly for PAH, at least annually. Screening tools include echocardiogram, pulmonary function tests, and 6-minute walk test. Chest computed tomography may be done if ILD is suspected.44
Treatment options for CTD-PAH are the same as those for IPAH. The major difference between these two groups is that those with scleroderma-PAH have a more blunted response to treatment. Scleroderma-PAH is rarely vasoreactive and often do not respond to CCBs. Otherwise the same PAH-specific therapies are used. Immunosuppression does not have role for scleroderma-PAH, but may for other CTD-PAH including SLE and mixed CTD.44
HIV-associated PAH
PAH occurs in 0.5% of patients with HIV. HIV-associated PAH can be severe.52 The pathogenesis is not well known, but it is suspected to include the effects of HIV viral proteins, or risk factors that are common in HIV. HIV infection also induces a chronic inflammatory state characterized by persistent immune activation and dysregulation that could indirectly induce the release of proinflammatory cytokines and growth factors that could cause PAH.52
As in other PAH-subgroups, echocardiography has a low diagnostic yield in HIV patients. In a study of Doppler echocardiography, HIV-associated PAH was missed in more than one-third of the patients.53
Studies have shown that antiretroviral treatment (ART) has reduced the incidence of HIV-associated PAH, improved exercise tolerance as assessed by 6-minute walk distance; and in animal models, protease inhibitors have been shown to reverse hypoxia-induced PH.54–56 Current guidelines recommend that all HIV-infected patients be treated with antiretrovirals regardless of CD4 T-cell count and viral load.57 When choosing the ART regimen, clinicians should take into consideration the likely need for PAH-specific therapies and relevant drug interactions.
Few studies have specifically addressed the treatment of HIV-associated PAH, so the approach to treatment is the same as those for IPAH. Studies have shown that although there are drug interactions between ART and PAH-specific therapy, such as PDE-5 inhibitors, successful coadministration has been reported.58,59 With regard to specific challenges in management, few patients with HIV-associated PAH have positive acute vasodilator response during RHC, and therefore do not have long-term responses to CCBs.60
Congenital heart disease
PAH-associated with CHD (PAH-CHD) occurs due to pulmonary “overcirculation” but given advances in cardiac care, many patients undergo repair before PAH develops. PAH may still develop even many years if not decades after surgical repair. However, PAH-CHD remains a problem mainly for those whom the left-to-right shunt is not detected until childhood or adulthood, or in patients with limited access to surgical management.61 One pediatric registry reports that 40% of included patients have CHD, 35% of which previously had surgical repair.62
The prevalence of PAH-CHD in Western countries has been estimated at 1.6–12.5 cases per million adults. Eisenmenger’s syndrome is the most common and most advanced form of PAH-CHD. The histopathological findings seen in CHD-PAH are the same as those with IPAH. Clinically, CHD-PAH presents the same way as IPAH except for the case of Eisenmenger’s syndrome, where cyanosis is a key feature. Survival of patients with Eisenmenger’s syndrome is understandably less than that of the general population, but appears to be better than those with IPAH. However, survival bias may be one contributory factor to this perceived improved survival rate.
Management options are the same as those for IPAH, with additional options being phlebotomy for those with hyperviscosity due to prolonged cyanosis, and surgical repair of cardiac defect prior to shunt reversal.63 Some PAH-CHD improves or resolves after repair of the defect, while in others, the PAH is irreversible and surgery can worsen the prognosis. Patients with persistent or recurrent PAH after surgery have been shown to have worse outcomes.61
Portopulmonary hypertension
The incidence of portopulmonary hypertension (PoPH) varies from 0.7% in autopsy studies to 16% in selected patients with advanced liver disease.64 Despite a higher incidence in studies, with more advanced liver disease, there has been no clear relationship between severity of hepatic dysfunction or portal hypertension and severity of PH. The pathogenesis of PoPH is incompletely understood. A hyperdynamic circulation is present in almost all patients with early stages of PoPH. High cardiac output increases stress on the pulmonary circulation. In the setting of portal hypertension, the pulmonary vasculature may dilate leading to hepatopulmonary syndrome, or it may increase the vascular resistance and vasoconstricts leading to pulmonary vascular remodeling and PH. It is unclear what factors determine the direction of vascular response. Histologically, the proliferative pulmonary arteriopathy with the formation of plexiform lesions is indistinguishable from that of IPAH.5
PoPH most commonly presents with progressive dyspnea on exertion. However, one diagnostic challenge is that the signs and symptoms of right heart failure, for example, peripheral edema and ascite, may overlap with those of liver cirrhosis. Otherwise, PoPH is screened with echocardiography and diagnosed with RHC, just as other types of PH.
Patients with mild PoPH (ie, mPAP <30–35 mm Hg) may have no suspicious symptoms. Those with moderate PoPH have a much higher perioperative risk. PoPH is frequently reversible after liver transplantation. In cases of severe PoPH, mortality after liver transplantation is significantly increased due to PAH risk as well as compromised perfusion of the liver graft. There is also concern of hepatic congestion posttransplant from decreased right ventricular function that can lead to primary graft dysfunction. In some patients, specific pulmonary vasodilator treatment can be used prior to transplantation in an attempt to improve outcome.65
Other management limitations include the safety of PAH treatments in PoPH. For example, in some patients with PAH, anticoagulation has been shown to slow the disease progression.66 However, patients with advanced liver disease have a higher risk of hemorrhagic complications such as bleeding varices and therefore are typically not candidates for anticoagulation.
Another therapeutic limitation is the use of infused prostanoid analogs. Epoprostenol is the best-studied drug in patients with PoPH.67,68 As previously discussed, the major drawback is that it requires permanent central venous access and uninterrupted drug infusion. This delivery system is prone to infection, thromboembolic disease, and/or pump failure and requires strict cooperation from patients. Infused prostanoids should not be used in patients with continued excessive alcohol intake or illicit drug use. The other oral and inhaled medications for PAH are not as well studied in this population, but remain a viable option.
Schistosomiasis
Though rare in develop countries, more than 200 million people are infected with schistosomiasis worldwide, which is the third most common parasitic disease, and ~1% of those who are chronically infected develop PAH. Schistosomiasis is still one of the most common causes of PAH worldwide. It is presumed that the acute cutaneous infection with Schistosoma causes inflammation at the site of parasite penetration, followed by a subacute immune complex-mediated hypersensitivity response as the parasite migrates through the liver and the lungs. Chronic infection induced a granulomatous inflammation around ova deposited in tissue. Schistosoma enter to portal venous system and cause preportal fibrosis in a subset of individuals. Fibrosis results in progressive portal venous system destruction, leading to portal hypertension. Portal hypertension appears to be an important contributor to the pathogenesis of PH, as most cases of schistosomiasis-associated PAH develop in the setting of portal fibrosis. The pulmonary vascular remodeling is likely due to the direct consequence of the host inflammatory response, and PoPH may be a significant contributor.69 The biggest diagnostic and treatment obstacle for schistosomiasis-associated PAH is that most patients are from resource-poor areas, often are diagnosed at late stages, and PAH-specific therapies may not be available to them.
WHO group 2 PH
WHO group 2 is PH due to left heart disease. The prevalence of PH in chronic heart failure patients increases with functional class impairment. Up to 60% of patients with severe left ventricular systolic dysfunction and 70% of those with isolated diastolic dysfunction may have PH.70 Left-sided valvular disease can also cause PH, and the prevalence increases with the severity of the defect.71 Group 2 PH is distinguished from the other types by the presence of pulmonary venous hypertension. Pathological changes in this group are characterized by enlarged and thickened pulmonary veins, pulmonary capillary dilatation, interstitial edema, potentially alveolar hemorrhage, and lymphatic vessels and lymph nodes enlargement. Distal pulmonary arteries may be affected by medical hypertrophy and intimal fibrosis.5
Diagnosis
The diagnosis is made when the PAWP or left ventricular end-diastolic pressure is ≥15 mm Hg, in addition to the elevated mPAP that is required for any PH diagnosis. However, the PAWP or left ventricular end-diastolic pressure can be misleadingly normal if the patient is being managed with diuretics or is intravascularly depleted at the time of the RHC (eg, after a prolonged fasting state for the procedure). A fluid or exercise challenge can be done to elucidate left ventricular dysfunction, but this process has not been standardized. In some patients with mildly elevated PAWP values (15–18 mm Hg), it may be difficult to distinguish PAH from group 2 PH, as the increased right ventricular pressure restricts the compliance of the left ventricle (inter-ventricular dependence).5 If the PAWP is elevated long enough, it causes pathologic remodeling in the pulmonary circulation that even after the PAWP is decreased, these patients may have elevated PVR and hemodynamics that are identical to PAH hemodynamics.
Treatment
Currently, there are no WHO group 2 PH-specific therapies, and so the management of this group is aimed at optimizing the treatment of left heart disease. Some PAH-specific therapies have been studied for left heart failure, but the results were disappointing.72 Thus, these therapies are not recommended. Patients with PH that is subjectively deemed to be inconsistent with the severity of left heart disease could be enrolled in clinical trials targeting PAH-specific drugs.5
WHO group 3 PH
WHO group 3 PH are those owing to chronic lung diseases and/or hypoxemia. This group includes, among other lung diseases, chronic obstructive pulmonary disease (COPD), ILD, and sleep disordered breathing. An important clinical distinction between these patients as compared to those with lung disease alone is that exertional dyspnea is disproportionate to the ventilatory pathology noted on pulmonary function tests or chest imaging, and it is more related to a limited circulatory reserve.73 In general, this group of PH is thought to be mediated by hypoxic vasoconstriction, mechanical stress of hyperinflated lungs, loss of capillaries, and/or inflammation. Pathological changes for this group include medial hypertrophy and intimal obstructive proliferation of the distal pulmonary arteries. A variable degree of destruction of the vascular bed in emphysematous or fibrotic areas may also be present.5
The prevalence of PH in COPD is dependent on the severity of the disease. In advanced COPD, >50% of patients have PH, though most of only mild severity. However, severity of COPD does not predict the severity of PH. The National Emphysema Treatment Trial found that only 5% of patients with severe COPD had an mPAP ≥35 mm Hg.74 A serotonin gene polymorphism appears to determine the severity of PH in hypoxemic patients with COPD.75 A retrospective study in patients with COPD and severe PH found that these patients had a distinctive pattern of hypocapnia, very low DLCO (diffusing capacity or transfer factor of the lung for carbon monoxide), and increased right atrial pressures with a reduced cardiac index. These distinctions were made in comparison to the control group, patients with COPD, and mild-to-moderate PH. Another finding in this study was that 16 of the 27 patients with COPD and severe PH were found to have another possible cause of PH, such as left heart disease, CTEPH, obstructive sleep apnea, or CTD. Therefore, patients with COPD and an mPAP ≥35 mm Hg should undergo thorough workup to look for other causes of PH. Survival was significantly shorter in patients with severe PH.76 A 5-year survival rate of only 36% was reported for COPD patients with mPAP values ≥25 mm Hg, with pulmonary hemodynamics being a far stronger predictor of survival than the forced expiratory volume in 1 second – FEV1 or gas exchange variables.77
ILD such as idiopathic pulmonary fibrosis (IPF) and other diffuse parenchymal diseases also cause WHO group 3 PH. The prevalence of PH in ILD is estimated to be between 32% and 39%.78 For IPF, mPAP values of ≥25 mm Hg were reported between 8.1% and 14.9% of patients,79,80 with higher prevalence in advanced- and end-stage IPF (>60% of cases).81 A smaller percentage of patients have an mPAP ≥40 mm Hg. Just as in COPD patients, there is a poor correlation between PH severity and lung function impairment. PH worsens the prognosis of IPF patients, with mPAP and forced vital capacity being independent predictors of survival.80 Patients with combined pulmonary fibrosis and emphysema are more likely to develop PH with prevalence estimates between 30% and 50%.73
Other lung diseases in this group include sleep-disordered breathing such as obstructive sleep apnea,82 alveolar hypoventilation disorders, and other lung diseases that result in hypoxemia.
Diagnosis
A clinical diagnosis of PH is more difficult in this group because of respiratory compromise associated with these conditions. Echocardiography is the best screening tool, however, and it is still limited by the reliability of PA pressures. Another adjunctive test is the plasma level of B-type natriuretic protein (BNP), which is elevated in PH, but not in isolated lung diseases. However, this value is quite variable and lacks sensitivity in moderate PH and can also be confounded with any left heart abnormalities, which is often present in these patients.73 Despite this, BNP levels have been found to be predictive of mortality in patients with ILD.83 Indications for RHC include evaluation for lung transplantation, clinical worsening, or exercise limitation “disproportionate” to ventilatory impairment, suspicion for right heart failure, or inconclusive echocardiographic study in those with a high clinical suspicion for PH.5 One diagnostic limitation is the subjectivity of the “out of proportion” determination in these patients, so more objective definitions are currently recommended.73
Treatment
Just as in WHO group 2 PH patients, the first step in the treatment of PH due to lung disease is optimizing the management of the underlying lung disease. An important aspect of this management is the use of supplemental oxygen to avoid hypoxemia, which can worsen PH. Long-term oxygen supplementation has been shown to partially reduce the progression of PH in COPD patients.5
With regard to PAH-specific drugs, the data for their use in group 3 patients are mixed. Theoretically, the vasodilation of pulmonary vessels could actually worsen gas exchange in patients with lung disease because of the interference with “regional” hypoxic vasoconstriction, thus inadvertently perfusing poorly ventilated lung areas. However, because of their mode of distribution, inhaled Iloprost, Treprostinil, or NO could provide vasodilation to areas that are better ventilated and oxygenated, which would be beneficial. Objective data are needed for the use of inhaled prostanoids in these patients, especially since even when given via inhalation, they still have high enough levels in the systemic circulation, and thus also act as systemic prostanoid analogs.
PDE-5 inhibitors may enhance normoxic vasodilation and could also be beneficial. There have been some trials that suggested improvement in exercise tolerance and oxygenation in a subgroup of IPF patients,84,85 though more studies are needed. Another study found that PDE-5 inhibitors improved the hemodynamics in COPD patients, but worsened the gas exchange.86 However, definite harm has been documented in other RCTs, and the use of some pulmonary vasodilators is contraindicated in ILD, for example.33,87 Overall, it is currently not recommended to use these pulmonary vasodilator drugs in WHO group 3 PH patients, and more investigation is needed.
WHO group 4 PH
WHO group 4 PH results from chronic thromboembolic disease. After an acute pulmonary embolism (PE), it is estimated that 1%–4% of patients develop CTEPH.88 It is proposed that the acute embolus does not completely resolve, and subsequently undergoes fibrosis, which initially leads to a mechanical obstruction of the pulmonary arteries. Obstruction causes inflammatory and vasculotrophic mediators to be released, resulting in vascular remodeling. This can occur regardless of the cause of clot formation. For example, there have been a few causes identified in patients with CTEPH, with thoracic outlet syndrome in which chronic compression of the subclavian vein can cause a deep vein thrombosis and a subsequent PE.
CTEPH can also occur without a previously known history of acute PE. A suspected mechanism of this is that thrombotic and/or inflammatory lesions exist in the pulmonary vasculature, and they result in vascular remodeling without clinically manifesting acute thromboembolic events. Certain conditions have been associated with the development of CTEPH, likely due to their chronic inflammatory states. These include postsplenectomy, myeloproliferative disorders, and inflammatory bowel diseases.5
Diagnosis
Any patient with unexplained PH and all patients with PAH should be evaluated for CTEPH. Patients with an acute PE and signs of PH or RV dysfunction at the time of presentation should have a follow-up echocardiogram at 3–6 months to determine whether PH has resolved. The workup for CTEPH should include a ventilation–perfusion scan. Computed tomography of the chest with arteriography has a lower sensitivity than the ventilation–perfusion scan for chronic pulmonary emboli.89 A final diagnosis is made when there is hemodynamic evidence of precapillary PH (mPAP ≥25, PAWP ≤15) plus multiple chronic occlusive thrombi or emboli in the pulmonary arteries.
Treatment
All patients with CTEPH should receive life-long anticoagulation. The first-line treatment option for CTEPH is a pulmonary endarterectomy (PEA), which is potentially curative. Considerations for surgery include extent and location of organized thrombi (proximal being more ideal for PEA), degree of PH, age, and comorbidities.5 Best outcomes following PEA occur at expert centers. However, only 63% of patients are eligible for surgery,90 and PH persists or recurs after surgery in 5%–35% of patients.91,92 Routine placement of an inferior vena cava filter in CTEPH patients is controversial.
Unlike WHO groups 2 and 3, PAH-specific drugs can be considered for CTEPH patients. These drugs are used for those patients who are not candidates for surgery, who require preoperative treatment to improve hemodynamics or for those who have residual or recurrent symptoms of PH following PEA.5 Prostanoids, ERAs, and PDE-5 inhibitors all have suggested evidence in uncontrolled trials to improve hemodynamics and have clinical benefits. One randomized controlled trial evaluated Bosentan for inoperable CTEPH patients and found a significant drop in PVR. Unfortunately, no change was seen in exercise tolerance, functional class, or time to clinical worsening.93 Currently, none of these medications (except Riociguat; see below) is FDA-approved for the use in CTEPH.
The only approved class for medical treatment of CTEPH is Riociguat, a GCs. As discussed earlier, the PATENT-1 study found that Riociguat showed significant benefit in PAH patients.29 The CHEST-1 trial studied Riociguat in CTEPH patients and found that it improved exercise capacity, PVR, and WHO functional class in patients with inoperable or persistent/recurrent CTEPH.94
WHO group 5 PH
This final group encompasses PH due to unclear reasons. Conditions included in this group include sarcoidosis, myeloproliferative disorders, Langerhans cell histiocytosis, chronic renal failure, and many other rare disorders.5 The pathogenic mechanisms for the development of PH in this group are uncertain, and given its heterogeneity, the epidemiology of this group is unknown. There are evolving recommendations for screening for PH in these conditions, as well as ongoing research for the use of PAH-specific medications, however, there are currently no approved medications for this group of PH. The only recommended treatment is optimizing the management of each condition.
Conclusion
Overall, the prevalence in the general population of these five groups of PH is unknown but has been estimated at >10%, with group 2 being the most common.2 The diagnostic challenges in each group of PH have been described earlier. Additionally, the diagnosis of PH in patients with more than one risk factor is also problematic. For example, a patient with scleroderma, obstructive sleep apnea, and mild diastolic dysfunction could have a severely elevated mPAP, with a mildly elevated PAWP, not strictly satisfying the diagnostic criteria of PAH, and having features of both WHO groups 2 and 3. These patients with mixed clinical pictures present not only a diagnostic challenge, but also a therapeutic challenge, since most medications have been shown to be helpful in PAH patients alone, and potentially harmful in non-PAH patients. Using the same example, one could argue that PAH-specific therapy could greatly benefit this patient because scleroderma could be driving the PH, while others could argue that because these drugs could in fact be harmful to those in groups 2 and 3 PH, that they should instead be avoided. Despite the advances in diagnostic and therapeutics for PH, there is still uncertainty in managing these patients with non-PAH PH, and there is no standardization in their care.
Disclosure
The authors report no conflicts of interest in this work.
References
Simonneau G, Gatzoulis MA, Adatia I, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2013;62(25_S):D34–D41. | ||
Mozaffarian D, Benjamin EJ, Go AS, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics – 2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29–e322. | ||
Tuder RM, Archer SL, Dorfmüller P, et al. Relevant issues in the pathology and pathobiology of pulmonary hypertension. J Am Coll Cardiol. 2013;62(25):D4–D12. | ||
Humbert M, Morrell NW, Archer SL, et al. Cellular and molecular pathobiology of pulmonary arterial hypertension. J Am Coll Cardiol. 2004;43(12 suppl):S13–S24. | ||
Galiè N, Hoeper MM, Humbert M, et al; Task Force for Diagnosis and Treatment of Pulmonary Hypertension of European Society of Cardiology (ESC); European Respiratory Society (ERS); International Society of Heart and Lung Transplantation (ISHLT). Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J. 2009;34(6):1219–1263. | ||
Fisher MR, Forfia PR, Chamera E, et al. Accuracy of Doppler echocardiography in the hemodynamic assessment of pulmonary hypertension. Am J Respir Crit Care Med. 2009;179:615–621. | ||
Janda S, Shahidi N, Gin K, Swiston J. Diagnostic accuracy of echocardiography for pulmonary hypertension: a systematic review and meta-analysis. Heart. 2011;97:612–622. | ||
Raymond RJ, Hinderliter AL, Willis PW, et al. Echocardiographic predictors of adverse outcomes in primary pulmonary hypertension. J Am Coll Cardiol. 2002;39(7):1214–1219. | ||
Sauler M, Fares WH, Trow TK. Standard nonspecific therapies in the management of pulmonary arterial hypertension. Clin Chest Med. 2013;34(4):799–810. | ||
Maron BA, Waxman AB, Opotowsky AR, et al. Effectiveness of spironolactone plus ambrisentan for treatment of pulmonary arterial hypertension (from the [ARIES] study 1 and 2 trials). Am J Cardiol. 2013;112(5):720–725. | ||
Maron BA, Leopold JA. The role of the renin-angiotensin-aldosterone system in the pathobiology of pulmonary arterial hypertension (2013 Grover Conference series). Pulm Circ. 2014;4:200–210. | ||
McLaughlin VV, Archer SL, Badesch DB, et al; American College of Cardiology Foundation Task Force on Expert Consensus Documents; American Heart Association; American College of Chest Physicians; American Thoracic Society, Inc; Pulmonary Hypertension Association. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association developed in collaboration with the American College of Chest Physicians; American Thoracic Society, Inc.; and the Pulmonary Hypertension Association. J Am Coll Cardiol. 2009;53(17):1573–1619. | ||
Rich S, Kaufmann E, Levy PS. The effect of high doses of calcium-channel blockers on survival in primary pulmonary hypertension. N Engl J Med. 1992;327(2):76–81. | ||
Fares WH, Trow TK. Targeted approaches to the treatment of pulmonary hypertension. Ther Adv Respir Dis. 2012;6:147–159. | ||
Ruan CH, Dixon RA, Willerson JT, Ruan KH. Prostacyclin therapy for pulmonary arterial hypertension. Tex Heart Inst J. 2010;37(4):391–399. | ||
Rubin LJ, Mendoza J, Hood M, et al. Treatment of primary pulmonary hypertension with continuous intravenous prostacyclin (epoprostenol). Results of a randomized trial. Ann Intern Med. 1990;112(7):485–491. | ||
Barst RJ, Rubin LJ, Long WA, et al; Primary Pulmonary Hypertension Study Group. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. N Engl J Med. 1996;334(5):296–301. | ||
Badesch DB, Tapson VF, McGoon MD, et al. Continuous intravenous epoprostenol for pulmonary hypertension due to the scleroderma spectrum of disease. A randomized, controlled trial. Ann Intern Med. 2000;132:425–434. | ||
Benza RL, Tapson VF, Gomberg-Maitland M, Poms A, Barst RJ, McLaughlin VV. One-year experience with intravenous treprostinil for pulmonary arterial hypertension. J Heart Lung Transplant. 2013;32(9):889–896. | ||
Jing ZC, Parikh K, Pulido T, et al. Efficacy and safety of oral treprostinil monotherapy for the treatment of pulmonary arterial hypertension: a randomized, controlled trial. Circulation. 2013;127(5):624–633. | ||
Krishnan U, Takatsuki S, Ivy DD, et al. Effectiveness and safety of inhaled treprostinil for the treatment of pulmonary arterial hypertension in children. Am J Cardiol. 2012;110(11):1704–1709. | ||
Fares WH. Orenitram…. not verified. Am J Respir Crit Care Med. 2015;191(6):713–714. | ||
Kholdani CA, Fares WH, Trow TK. Macitentan for the treatment of pulmonary arterial hypertension. Vasc Health Risk Manag. 2014;10:665–673. | ||
Badesch DB, Feldman J, Keogh A, et al; ARIES-3 Study Group. ARIES-3: ambrisentan therapy in a diverse population of patients with pulmonary hypertension. Cardiovasc Ther. 2012;30(2):93–99. | ||
Galie N, Olschewski H, Oudiz RJ, et al; Ambrisentan in Pulmonary Arterial Hypertension, Randomized, Double-Blind, Placebo-Controlled, Multicenter, Efficacy Studies (ARIES) Group. Ambrisentan for the treatment of pulmonary arterial hypertension: results of the ambrisentan in pulmonary arterial hypertension, randomized, double-blind, placebo-controlled, multicenter, efficacy (ARIES) study 1 and 2. Circulation. 2008;117:3010–3019. | ||
Pulido T, Adzerikho I, Channick RN, et al; SERAPHIN Investigators. Macitentan and morbidity and mortality in pulmonary arterial hypertension. N Engl J Med. 2013;369(9):809–818. | ||
Fan YF, Zhang R, Jiang X, et al. The phosphodiesterase-5 inhibitor vardenafil reduces oxidative stress while reversing pulmonary arterial hypertension. Cardiovasc Res. 2013;99:395–403. | ||
Galiè N, Brundage BH, Ghofrani HA, et al; Pulmonary Arterial Hypertension and Response to Tadalafil (PHIRST) Study Group. Tadalafil therapy for pulmonary arterial hypertension. Circulation. 2009;119(22):2894–2903. | ||
Ghofrani HA, Galiè N, Grimminger F, et al; PATENT-1 Study Group. Riociguat for the treatment of pulmonary arterial hypertension. N Engl J Med. 2013;369(4):330–340. | ||
Benza RL, Gomberg-Maitland M, Miller DP, et al. The REVEAL Registry risk score calculator in patients newly diagnosed with pulmonary arterial hypertension. Chest. 2012;141:354–362. | ||
Galiè N, Corris PA, Frost A, et al. Updated treatment algorithm of pulmonary arterial hypertension. J Am Coll Cardiol. 2013;62(25 suppl):D60–D72. | ||
Rubin L, Barbera J, Frost A, et al. Upfront combination therapy with ambrisentan and tadalafiliin treatment naive patients with Pulmonary Arterial Hypertension (PAH): subgroup analyses by Functional Class (FC), etiology, and region from the AMBITION Study. Chest. 2014;146:339A–339A. 4_MeetingAbstracts. | ||
Raghu G, Behr J, Brown KK, et al; ARTEMIS-IPF Investigators. Treatment of idiopathic pulmonary fibrosis with ambrisentan: a parallel, randomized trial. Ann Intern Med. 2013;158:641–649. | ||
Taichman DB, Ornelas J, Chung L, et al. Pharmacologic therapy for pulmonary arterial hypertension in adults: CHEST guideline and expert panel report. Chest. 2014;146:449–475. | ||
Doyle RL, McCrory D, Channick RN, Simonneau G, Conte J. Surgical treatments/interventions for pulmonary arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest. 2004;126:63S–71S. | ||
Peacock AJ, Murphy NF, McMurray JJV, Caballero L, Stewart S. An epidemiological study of pulmonary arterial hypertension. Eur Respir J. 2007;30(1):104–109. | ||
Humbert M, Sitbon O, Chaouat A, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006;173:1023–1030. | ||
Cogan JD, Pauciulo MW, Batchman AP, et al. High frequency of BMPR2 exonic deletions/duplications in familial pulmonary arterial hypertension. Am J Respir Crit Care Med. 2006;174:590–598. | ||
Chida A, Shintani M, Nakayama T, et al. Missense mutations of the BMPR1B (ALK6) gene in childhood idiopathic pulmonary arterial hypertension. Circ J. 2012;76:1501–1508. | ||
Thomson JR, Machado RD, Pauciulo MW, et al. Sporadic primary pulmonary hypertension is associated with germline mutations of the gene encoding BMPR-II, a receptor member of the TGF-beta family. J Med Genet. 2000;37(10):741–745. | ||
Austin ED, Loyd JE, Phillips JA. Heritable pulmonary arterial hypertension. GeneReviews(R). Seattle WA: University of Washington, Seattle; 2015. | ||
Eddahibi S, Adnot S. Anorexigen-induced pulmonary hypertension and the serotonin (5-HT) hypothesis: lessons for the future in pathogenesis. Respir Res. 2002;3:9. | ||
Montani D, Seferian A, Savale L, Simonneau G, Humbert M. Drug-induced pulmonary arterial hypertension: a recent outbreak. Eur Respir Rev. 2013;22:244–250. | ||
Goldberg A. Pulmonary arterial hypertension in connective tissue diseases. Cardiol Rev. 2010;18:85–88. | ||
Kamel SR, Omar GM, Darwish AF, Asklany HT, Ellabban AS. Asymptomatic pulmonary hypertension in systemic lupus erythematosus. Clin Med Insights Arthritis Musculoskelet Disord. 2011;4:77–86. | ||
Badesch DB, Raskob GE, Elliott CG, et al. Pulmonary arterial hypertension: baseline characteristics from the REVEAL registry. Chest. 2010;137:376–387. | ||
McGoon MD, Miller DP. REVEAL: a contemporary US pulmonary arterial hypertension registry. European Respiratory Review. 2012;21(123):8–18. | ||
Chung L, Liu J, Parsons L, et al. Characterization of connective tissue disease-associated pulmonary arterial hypertension from REVEAL: identifying systemic sclerosis as a unique phenotype. Chest. 2010;138:1383–1394. | ||
Steen V, Medsger TA Jr. Predictors of isolated pulmonary hypertension in patients with systemic sclerosis and limited cutaneous involvement. Arthritis Rheum. 2003;48(2):516–522. | ||
Xia YK, Tu SH, Hu YH, et al. Pulmonary hypertension in systemic lupus erythematosus: a systematic review and analysis of 642 cases in Chinese population. Rheumatol Int. 2013;33(5):1211–1217. | ||
Dhala A. Pulmonary arterial hypertension in systemic lupus erythematosus: current status and future direction. Clin Dev Immunol. 2012;2012:854941. | ||
Barnett CF, Hsue PY. Human immunodeficiency virus-associated pulmonary arterial hypertension. Clin Chest Med. 2013;34(2):283–292. | ||
Selby VN, Scherzer R, Barnett CF, et al. Doppler echocardiography does not accurately estimate pulmonary artery systolic pressure in HIV-infected patients. AIDS. 2012;26(15):1967–1969. | ||
Pugliese A, Isnardi D, Saini A, Scarabelli T, Raddino R, Torre D. Impact of highly active antiretroviral therapy in HIV-positive patients with cardiac involvement. J Infect. 2000;40(3):282–284. | ||
Degano B, Guillaume M, Savale L, et al. HIV-associated pulmonary arterial hypertension: survival and prognostic factors in the modern therapeutic era. AIDS. 2010;24(1):67–75. | ||
Gary-Bobo G, Houssaini A, Amsellem V, et al. Effects of HIV protease inhibitors on progression of monocrotaline- and hypoxia-induced pulmonary hypertension in rats. Circulation. 2010;122(19):1937–1947. | ||
Thompson MA, Aberg JA, Hoy JF, et al. Antiretroviral treatment of adult HIV infection: 2012 Recommendations of the International Antiviral Society-USA panel. JAMA. 2012;308(4):387–402. | ||
Ieong MH, Farber HW. Noninfectious pulmonary complications of HIV. Clin Pulm Med. 2006;13(3):194–202. | ||
Schumacher YO, Zdebik A, Huonker M, Kreisel W. Sildenafil in HIV-related pulmonary hypertensin [3]. AIDS. 2001;15(13):1747–1748. | ||
Aguilar RV, Farber HW. Epoprostenol (Prostacyclin) therapy in HIV-associated pulmonary hypertension. Am J Respir Crit Care Med. 2000;162(5):1846–1850. | ||
Myers PO, Tissot C, Beghetti M. Assessment of operability of patients with pulmonary arterial hypertension associated with congenital heart disease. Circ J. 2014;78:4–11. | ||
Berger RM, Beghetti M, Humpl T, et al. Clinical features of paediatric pulmonary hypertension: a registry study. Lancet. 2012;379(9815):537–546. | ||
Galie N, Manes A, Palazzini M, et al. Management of pulmonary arterial hypertension associated with congenital systemic-to-pulmonary shunts and Eisenmenger’s syndrome. Drugs. 2008;68:1049–1066. | ||
McDonnell PJ, Toye PA, Hutchins GM. Primary pulmonary hypertension and cirrhosis: are they related? Am Rev Respir Dis. 1983;127(4):437–441. | ||
Hoeper MM, Krowka MJ, Strassburg CP. Portopulmonary hypertension and hepatopulmonary syndrome. Lancet. 2004;363:1461–1468. | ||
Fuster V, Steele PM, Edwards WD, Gersh BJ, McGoon MD, Frye RL. Primary pulmonary hypertension: natural history and the importance of thrombosis. Circulation. 1984;70(4):580–587. | ||
Kuo PC, Johnson LB, Plotkin JS, Howell CD, Bartlett ST, Rubin LJ. Continuous intravenous infusion of epoprostenol for the treatment of portopulmonary hypertension. Transplantation. 1997;63(4):604–606. | ||
Plotkin JS, Kuo PC, Rubin LJ, et al. Successful use of chronic epoprostenol as a bridge to liver transplantation in severe portopulmonary hypertension. Transplantation. 1998;65(4):457–459. | ||
Graham BB, Bandeira AP, Morrell NW, Butrous G, Tuder RM. Schistosomiasis-associated pulmonary hypertension: pulmonary vascular disease: the global perspective. Chest. 2010;137:20S–29S. | ||
Ghio S, Gavazzi A, Campana C, et al. Independent and additive prognostic value of right ventricular systolic function and pulmonary artery pressure in patients with chronic heart failure. J Am Coll Cardiol. 2001;37:183–188. | ||
Vahanian A, Baumgartner H, Bax J, et al. Guidelines on the management of valvular heart disease. Eur Heart J. 2007;28(2):230–268. | ||
Redfield MM, Chen HH, Borlaug BA, et al; RELAX Trial. Effect of phosphodiesterase-5 inhibition on exercise capacity and clinical status in heart failure with preserved ejection fraction: a randomized clinical trial. JAMA. 2013;309(12):1268–1277. | ||
Seeger W, Adir Y, Barberà JA, et al. Pulmonary hypertension in chronic lung diseases. J Am Coll Cardiol. 2013;62(25, suppl):D109–D116. | ||
Scharf SM, Iqbal M, Keller C, Criner G, Lee S, Fessler HE. Hemodynamic characterization of patients with severe emphysema. Am J Respir Crit Care Med. 2002;166(3):314–322. | ||
Eddahibi S, Chaouat A, Morrell N, et al. Polymorphism of the serotonin transporter gene and pulmonary hypertension in chronic obstructive pulmonary disease. Circulation. 2003;108(15):1839–1844. | ||
Chaouat A, Bugnet AS, Kadaoui N, et al. Severe pulmonary hypertension and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;172:189–194. | ||
Oswald-Mammosser M, Weitzenblum E, Quoix E, et al. Prognostic factors in COPD patients receiving long-term oxygen therapy. Importance of pulmonary artery pressure. Chest. 1995;107(5):1193–1198. | ||
Lettieri CJ, Nathan SD, Barnett SD, Ahmad S, Shorr AF. Prevalence and outcomes of pulmonary arterial hypertension in advanced idiopathic pulmonary fibrosis. Chest. 2006;129:746–752. | ||
Hamada K, Nagai S, Tanaka S, et al. Significance of pulmonary arterial pressure and diffusion capacity of the lung as prognosticator in patients with idiopathic pulmonary fibrosis. Chest. 2007;131(3):650–656. | ||
Kimura M, Taniguchi H, Kondoh Y, et al. Pulmonary hypertension as a prognostic indicator at the initial evaluation in idiopathic pulmonary fibrosis. Respiration. 2013;85(6):456–463. | ||
Nathan SD, Shlobin OA, Ahmad S, et al. Serial development of pulmonary hypertension in patients with idiopathic pulmonary fibrosis. Respiration. 2008;76(3):288–294. | ||
Kholdani C, Fares WH, Mohsenin V. Pulmonary hypertension in obstructive sleep apnea: is it clinically significant? A critical analysis of the association and pathophysiology. Pulm Circ. 2015;5(2):220–227. | ||
Corte TJ, Wort SJ, Gatzoulis MA, et al. Elevated brain natriuretic peptide predicts mortality in interstitial lung disease. Eur Respir J. 2010;36(4):819–825. | ||
Collard HR, Anstrom KJ, Schwarz MI, Zisman DA. Sildenafil improves walk distance in idiopathic pulmonary fibrosis. Chest. 2007;131(3):897–899. | ||
Zisman DA, Schwarz M, Anstrom KJ, Collard HR, Flaherty KR, Hunninghake GW. A controlled trial of sildenafil in advanced idiopathic pulmonary fibrosis. N Engl J Med. 2010;363(7):620–628. | ||
Blanco I, Gimeno E, Munoz PA, et al. Hemodynamic and gas exchange effects of sildenafil in patients with chronic obstructive pulmonary disease and pulmonary hypertension. Am J Respir Crit Care Med. 2010;181(3):270–278. | ||
Raghu G, Million-Rousseau R, Morganti A, Perchenet L, Behr J. Macitentan for the treatment of idiopathic pulmonary fibrosis: the randomised controlled MUSIC trial. Eur Respir J. 2013;42:1622–1632. | ||
Pengo V, Lensing AW, Prins MH, et al; Thromboembolic Pulmonary Hypertension Study Group. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med. 2004;350:2257–2264. [Massachusetts Medical Society]. | ||
Tunariu N, Gibbs SJ, Win Z, et al. Ventilation-perfusion scintigraphy is more sensitive than multidetector CTPA in detecting chronic thromboembolic pulmonary disease as a treatable cause of pulmonary hypertension. J Nucl Med. 2007;48:680–684. | ||
Mayer E, Jenkins D, Lindner J, et al. Surgical management and outcome of patients with chronic thromboembolic pulmonary hypertension: results from an international prospective registry. J Thorac Cardiovasc Surg. 2011;141:702–710. | ||
Freed DH, Thomson BM, Berman M, et al. Survival after pulmonary thromboendarterectomy: effect of residual pulmonary hypertension. J Thorac Cardiovasc Surg. 2011;141:383–387. [United States: A 2011 The American Association for Thoracic Surgery. Published by Mosby, Inc.]. | ||
Bonderman D, Skoro-Sajer N, Jakowitsch J, et al. Predictors of outcome in chronic thromboembolic pulmonary hypertension. Circulation. 2007;115:2153–2158. | ||
Jaïs X, D’Armini AM, Jansa P, et al; Bosentan Effects in iNopErable Forms of chronIc Thromboembolic pulmonary hypertension Study Group. Bosentan for treatment of inoperable chronic thromboembolic pulmonary hypertension: BENEFiT (Bosentan effects in iNopErable forms of chronIc thromboembolic pulmonary hypertension), a randomized, placebo-controlled trial. J Am Coll Cardiol. 2008;52:2127–2134. | ||
Ghofrani H-A, D’Armini AM, Grimminger F, et al. Riociguat for the treatment of chronic thromboembolic pulmonary hypertension. N Engl J Med. 2013;369(4):319–329. | ||
Hoeper MM, Bogaard HJ, Condliffe R, et al. Definitions and diagnosis of pulmonary hypertension. J Am Coll Cardiol. 2013;62(25_S):D42–D50. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.