Back to Journals » Clinical Ophthalmology » Volume 14
Providing a Safe and Effective Intravitreal Treatment Service: Strategies for Service Delivery
Authors Amoaku W, Bailey C, Downey L ![]() , Gale RP, Ghanchi F
, Gale RP, Ghanchi F ![]() , Hamilton R
, Hamilton R ![]() , Mahmood S, Menon G, Nosek J
, Mahmood S, Menon G, Nosek J ![]() , Pearce I, Yang Y
, Pearce I, Yang Y
Received 2 October 2019
Accepted for publication 3 April 2020
Published 15 May 2020 Volume 2020:14 Pages 1315—1328
DOI https://doi.org/10.2147/OPTH.S233061
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Winfried Amoaku,1 Clare Bailey,2 Louise Downey,3 Richard P Gale,4 Faruque Ghanchi,5 Robin Hamilton,6 Sajjad Mahmood,7 Geeta Menon,8 Jenny Nosek,9 Ian Pearce,10 Yit Yang11
1Academic Ophthalmology, Division of Clinical Neuroscience, University of Nottingham, Nottingham, UK; 2University Hospitals Bristol NHS Foundation Trust, Bristol, UK; 3Hull and East Yorkshire Eye Hospital, Hull University Teaching Hospital, Hull, UK; 4York Teaching Hospital NHS Foundation Trust, York, UK; 5Bradford Teaching Hospitals NHS Foundation Trust, Bradford, UK; 6Moorfield Eye Hospital NHS Foundation Trust, London, UK; 7Manchester Royal Eye Hospital, Manchester University NHS Foundation Trust, University of Manchester, Manchester Academic Health Science Centre, Manchester, UK; 8Frimley Health NHS Foundation Trust, Frimley, UK; 9Royal Shrewsbury Hospital, Shropshire, UK; 10St Paul’s Eye Unit, Royal Liverpool University Hospital, Liverpool, UK; 11Wolverhampton Eye Infirmary, The Royal Wolverhampton NHS Trust, Wolverhampton, UK
Correspondence: Louise Downey Email [email protected]
Abstract: An aging population leads to increasing demand for medical retina services with chronic diseases being managed in long-term care pathways. Many hospital services struggle to deliver efficient and effective MR care due, at least in part, to infrastructure that does not expand responsively enough to meet the increased demand. A steering committee of retinal specialists from a variety of UK NHS hospital ophthalmology departments with experience of leading and managing NHS retinal services in the intravitreal era came together for the generation of this document to review and compile key aspects that should be considered when optimising intravitreal treatment capacity within MR services. This article aims to provide a useful collation and signposting of key published evidence, consensus and insights on aspects of delivering an intravitreal service, including treatment regimens, virtual clinics, staff training and governance, telemedicine and information technology, and data collection and key performance indicators. The objective is to equip ophthalmologic healthcare professionals with the necessary tools to develop and adapt their local service in the face of current and projected increased demand.
Keywords: capacity, intravitreal service, nAMD, resources
Introduction
The expanding elderly population and concomitant rise in the numbers of patients with diseases of the retina have led to an increasing demand for treatment within the medical retina (MR) service.1–3 Moreover, the inclusion of efficacious anti-vascular endothelial growth factor (anti-VEGF) intravitreal agents following guidance from the National Institute for Health and Care Excellence (NICE) and the Scottish Medicine Consortium (SMC),4–7 has resulted in more than a 40% increase in outpatient attendances in the past 10 years.1,2 The required, recurrent injections for these agents necessitate frequent and substantial follow-up care, greatly contributing to the clinical workload of a service that lacks commensurate growth in resources.1,2,8,9 Many services are under pressure and are often running at maximum capacity, with some ophthalmologists feeling that the bottleneck lies directly with intravitreal injection appointments.9
When considering the barriers faced by the age-related macular disease (AMD) service, several key resource challenges have been identified by the Action on AMD and The Way Forward groups. These focus on capacity issues relating to clinic space, staffing, equipment, support and quality, and funding.1,2 Professional bodies, including The Royal College of Ophthalmologists (RCOphth), have developed guidance and frameworks based on exemplar MR service capacity models, with the unifying theme of optimising utilisation of resource while meeting the needs of patients both now and in the future.2,10,11 However, a one-size-fits-all solution does not exist, and local services will have to adapt models of working in line with their individual situations.
A working group of MR experts with experience of leading and managing NHS retinal services in the intravitreal era covering a reasonable geographic spread across England recently (Four meetings between May 2018 and November 2019) discussed the key aspects of delivering an intravitreal service and have come together to highlight the current issues faced and to support the service by sharing solutions to optimise capacity and reference the evidence for these. This article presents a collation and signposting of useful resources and should help equip ophthalmologic healthcare professionals (HCPs) with the necessary tools to develop and adapt their local service in the face of current and projected growth in demand. The intention is to provide various options that individual departments can assess and implement according to their needs for managing intravitreal services.
Treatment Regimens: Treat and Extend
Retinal service leads need to understand differences in intravitreal treatment regimens and their relative impact on service capacity. Treatment regimens should ideally optimise outcomes in terms of visual acuity (VA) and improve quality of life for patients but also minimise the burden to patients, carers, and healthcare infrastructure.
Intravitreal treatment regimens are broadly divided into reactive (treatment is given when disease activity is identified and judged as active) or “proactive” (treatment is given in a continuous manner). Reactive regimens include the pro re nata (PRN) or “as needed” treatment regimen.12 PRN protocols do not eliminate monthly review appointments or the challenge of timely injections meaning that retinal services may still be overburdened.13 Proactive regimens include fixed and Treat and Extend (T&E) regimens. Treating proactively allows injections to be predicted and hence scheduled in advance, which may be better for patients and also helps with service planning. Regimens like T&E aim to continuously control the disease, whereas PRN, by definition allows the disease to relapse before you treat.
Evidence for the efficacy and superiority of T&E is most developed for nAMD and hence will be the focus of the following section. Other diseases, including diabetic macular oedema (DMO) and retinal vein occlusion (RVO), have also been treated effectively in this way.
Clinical nAMD Trials Utilising the T&E Regimen
Several clinical trials published over the last 5 years have demonstrated comparable efficacy between T&E and fixed monthly regimens, and superiority of T&E over a PRN regimen with regards to visual outcomes in neovascular AMD (nAMD).12,14–22 Additionally, there is an emerging body of evidence reporting better visual outcomes with the T&E regimen than PRN in various real-world studies.23–25
In a meta-analysis of over 25,000 patients with nAMD the mean change in VA for patients receiving T&E was +8.8, +6.7, and +5.4 Early Treatment Diabetic Retinopathy Study (ETDRS) letters at year 1, year 2, and ≥3 years, respectively. In comparison, patients treated with PRN had +3.5, +1.3, and −1.9 ETDRS letters at the same time intervals.25 In addition, although T&E patients received on average more injections (6.9 vs 4.7) they had fewer visits (7.6 vs 9.2) in the first year.25
A T&E regimen can help individualise treatment where patients receive an injection at each visit and are assessed to determine the interval to the next visit. Such an approach avoids under- and over-treatment, thus reducing patient burden and improving cost-effectiveness, reducing the need to continuously monitor or inject patients.13,26 Clinical data has demonstrated that a T&E regimen can reduce the number of patient clinic visits in comparison with the monthly visits and diagnostic evaluations necessary for PRN treatment, coupled with better functional outcomes.12 Overall, an individualised T&E regimen has the potential to reduce clinic burden and improve patient compliance while helping to achieve a safe and effective service for the treatment of nAMD.
Delivery of T&E
Many hospitals are now adopting the implementation of a T&E regimen based on evidence from clinical trials and ongoing support of real-world evidence. All authors provide National Health Service (NHS) intravitreal services where T&E is the default pathway for patients with nAMD undergoing intravitreal therapy. The authors are also aware that there are services and instances where this is not always possible or suitable. Patients who receive a T&E regimen are typically treated with an initiation phase on a monthly basis until stable.27,28 Thereafter, injections are administered at intervals of extended length until recurrence or worsening of disease activity when the interval is shortened.
The challenges and issues associated with the implementation of the regimen are comprehensively discussed in an article from Amoaku and colleagues. This is a useful resource for understanding the T&E regimen and its role in an effective retinal service.26
Virtual Clinics
What are Virtual Clinics?
Virtual clinics have gained increasing popularity as a means of increasing the outpatient capacity of ophthalmic clinics in an era when they are often under-resourced.1,2 In 2016, The RCOphth reported that virtual AMD clinics had been implemented in over 60% of eye departments in the UK.2 One definition of a virtual clinic is a clinic in which “the face-to-face clinician consultation is removed”.29 A patient and clinician may interact in real time during a virtual clinic (synchronous model) or the interaction may occur at different times (asynchronous model). Virtual data assessment of VA and retinal images usually occurs as a secondary asynchronous event after the patient has attended the primary data acquisition clinic, where the data is often collected by HCPs.
When to Consider Virtual Clinics
Virtual clinics may be an option when staffing/clinic rooms for disease assessments are limited. In general, the clinician assessing the data virtually, can assess at least double the number of patients who would have been seen in a face-to-face clinic,30 Furthermore, by acquiring assessment data at a different time to the review, the data acquisition clinics can be planned for a time when the required equipment (eg, optical coherence tomography [OCT] scanners, LogMAR charts) is ordinarily not in use, such as at the weekends or in the evenings.
Virtual clinics can also aid quality assurance for delegation of clinic assessments to trained non-medical HCPs. For example, in services where HCPs have been trained to review OCT data and support patient throughput by providing extra clinician capacity. A virtual assessment of OCT/ultra-widefield (UWF) imaging data can be better supported by consultant quality assurance, as the asynchronous nature of the review provides time for the HCP to ask/email for a second specialist opinion. This is particularly effective when services have electronic patient records (EPRs), meaning that paper notes do not need to be available to answer queries.
What Types of Diseases Have Services Managed with Virtual Clinics?
Virtual clinics are helpful for chronic diseases when repeat follow-up diagnostic assessments are needed, including nAMD, diabetic retinopathy (DR), glaucoma, choroidal naevi, sickle cell retinopathy and, more recently, hydroxychloroquine retinopathy.1,30–33
Some services use virtual clinics as a rapid means of disease triage for new referrals for intravitreal therapy so that best use can be made of limited baseline specialist clinic slots.30,34 New patient OCT triage, such as those from fast-track nAMD referrals or M1-graded patients from DR screening exemplify the use of virtual review for VA/OCT data analysis in order to increase throughput.30 “M1” is a category of patients with maculopathy felt to have disease which merits referral from the diabetic retinopathy screening service. Patients with “M1” disease have: exudate within 1 disc diameter (DD) of the centre of the fovea OR a group of exudates within the macula OR any microaneurysm or haemorrhage within 1DD of the centre of the fovea only if associated with a best VA of 6/12.35
False-positive referrals from the community may be 50–90% for fast-track nAMD referrals.2 All the authors use virtual clinics, in some form or another, routinely for nAMD follow-up assessments and also for triage of new referrals.
Virtual Clinics for Different Treatment Regimens
Injection regimens that use fixed dosing or T&E protocols are proactive. Therefore, the opportunity can be taken to acquire virtual VA/OCT data on the day of the planned injection, and this can then be reviewed in a virtual setting shortly after the injection visit to plan ongoing treatment intervals. This enables care to be delivered as a one-stop for patients but a “two-stop” for the hospital. Injection regimens with PRN dosing require monthly assessments, which are also highly amenable to virtual clinic delivery. However, in this scenario, the patient with active disease must then return at a later date for an injection within a two-stop pathway, increasing the burden of care for patient and service.
Safety of Virtual Clinics as a Replacement for Traditional Face-to-Face Clinic Reviews
In order to safely replace a face-to-face slit-lamp clinic review, incorporating retinal imaging with a virtual review using retinal imaging data only for new and follow-up patient appointments, the data collected during a virtual assessment should ideally be as sensitive as clinical evaluation with a slit lamp alongside the appropriate imaging.36 To improve sensitivity an OCT scan accompanied by a colour photo of the macula is helpful for nAMD/DMO macular assessments to detect retinal haemorrhage. UWF is often used to assess peripheral DR status.30 Although pathways with only virtual clinic follow-up assessments struggle to deliver holistic care, supplementing a predominantly virtual pathway with occasional slit-lamp clinics is a good compromise. Regular routine MR consultant arbitration of images and decision-making within the virtual pathway for services with non-consultant level HCPs making decisions ensures ongoing safety levels.
Points to Consider to Manage Effective Virtual Clinics
There are several strategies a local service should consider in order to run an effective virtual clinic, including redesigning invitation-to-appointment letters, patient outcome letters, and information leaflets (Table 1):
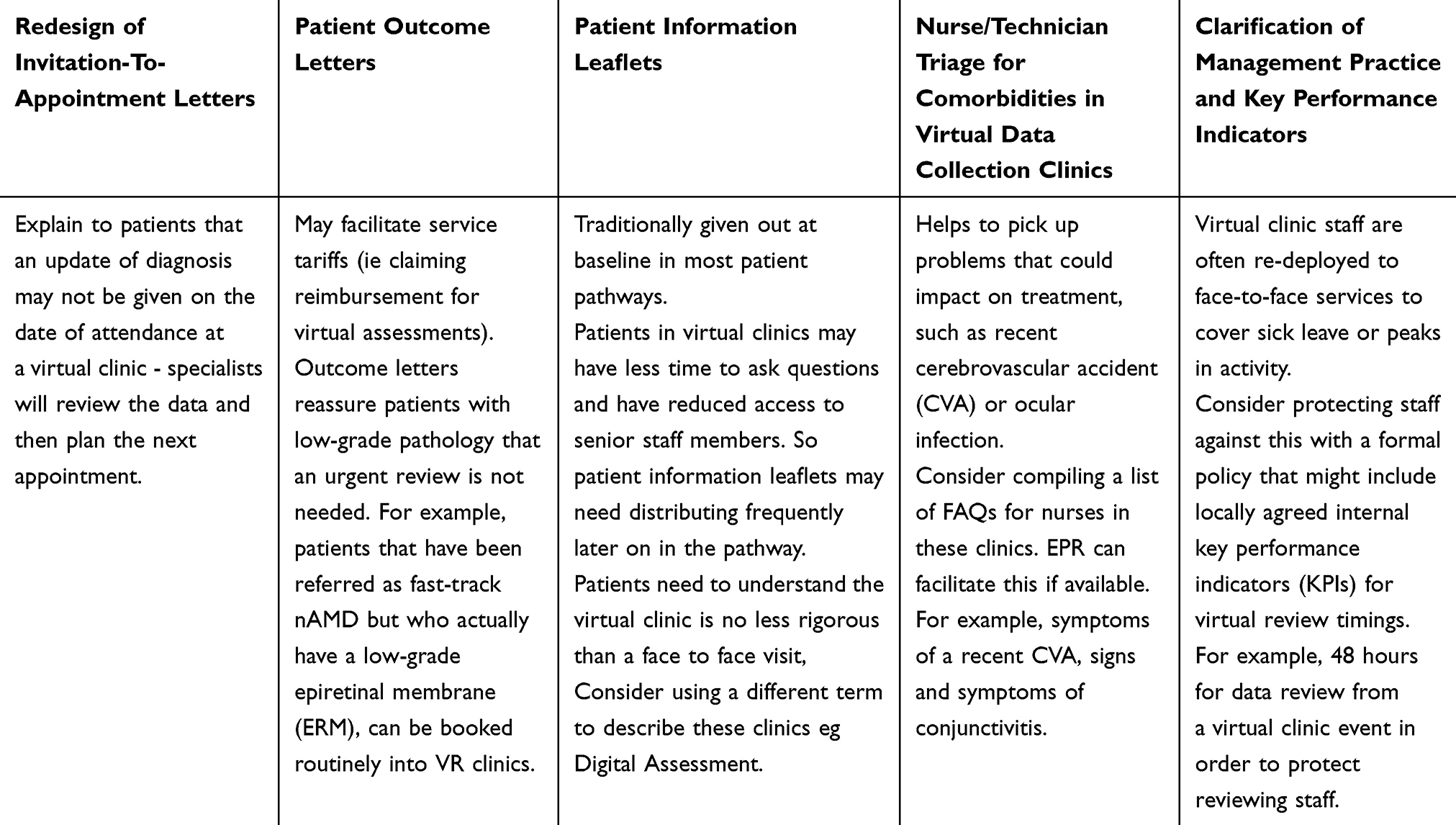 |
Table 1 Points to Consider for Effective Virtual Clinics; a Consensus View Based on the Experience of All Members of the Working Group |
OCT Imaging/OCTA: Baseline Imaging and Follow-Up
Optical coherence tomography (OCT) technology has completely revolutionised our detection, diagnostic accuracy and monitoring of retinal pathologies over the past 2 decades. During this period, OCT interpretation for different retinal and choroidal pathologies has developed significantly with a growing number of quantitative measures (eg, central retinal thickness, macular volume map, choroidal thickness) and qualitative factors (eg, vitreo-retinal interface changes, disorganization of retinal inner layers “DRIL” in diabetic maculopathy, variable patterns of drusen and drusenoid deposits in AMD, hypertrophic/dilated large choroidal vessels in pachychoroidal diseases). Each of these different parameters must be correctly recorded, classified and interpreted for accurate diagnosis and monitoring.
Recommendations for the role of OCT for baseline and monitoring visits are available in nAMD guidelines from NICE37,38 and The RCOphth have developed a comprehensive document that provides an overview of the commercially available ophthalmic imaging technologies and their clinical applications.39
It is important for units to develop and agree locally accepted pathways for frequency and mode of imaging to be undertaken at baseline and monitoring visits taking in to account existing national guidelines, evolving evidence and local factors. The pathway needs to assess not only the affected eye for management decisions but also for continued monitoring and early detection of pathology in the fellow eye.
OCT angiography (OCTA) is a more novel technology that is growing in acceptance as an alternative to traditional fluorescein angiography (FFA) in baseline assessment of many retinal pathologies including assessment of macular perfusion in DMO40 and to confirm baseline diagnosis of nAMD. Certainly, in specific circumstances such as in assessing the deep capillary plexus in diabetic maculopathy or in assessing for the presence of a vascular net in sub RPE Type I CNV (choroidal neovascularization) or small Type II CNV lesions it has distinct advantages over FFA. However, despite the obvious advantages of OCTA compared to the more invasive traditional FFA, the consensus from our steering group is that ophthalmologists must be cautious in interpreting OCTA images as there still remains significant potential for misleading image artefacts and pitfalls. Further refinements and validation studies are needed to establish its role in routine MR practice.41
For efficient and safe service delivery, our consensus is that units utilising OCTA should also have access to fluorescein angiography and when using these imaging modalities should have
- Agreed local pathways for frequency and mode of imaging to be undertaken at baseline and follow-up visits
- Appropriate training of staff and robust protocols for image acquisition (this will include fellow eye imaging protocols so early detection of disease is not missed)
- Appropriate training of staff and robust protocols for image interpretation to avoid missing appropriate signs that could impact care and early detection.
- Regular and updated continuous training for image acquisition and interpretation as the understanding and improved utility of OCT and OCTA are constantly evolving
- Networked image systems if images are collected at different sites so that appropriate comparison of previous images is available
- Appropriate IT hardware/software/network support to provide rapid access to large image files (particularly in case of OCTA) and robust storage systems for historical images
- Regular maintenance/service contracts for imaging equipment and appropriate contingency planning in event of equipment failure
Governance of Clean Rooms for Intravitreal Injections
The governance of clean rooms for IVT should be guided on best practice in order to improve the quality of services and, ultimately, prevent risk of harm to patients. There exists pertinent research evidence and policies with regards to clean room standards, in particular, the National Safety Standards for Invasive Procedures (NatSSIPs) 2015,42 which was developed following a review of never events reported across the NHS.43
Clean Room Requirements
In 2018, The RCOphth published guidance on performing all IVT as safely as possible, which included clean room requirements.44 To summarise their advice, IVT may be undertaken in theatre or in a clean room in the outpatient setting.44
|
|
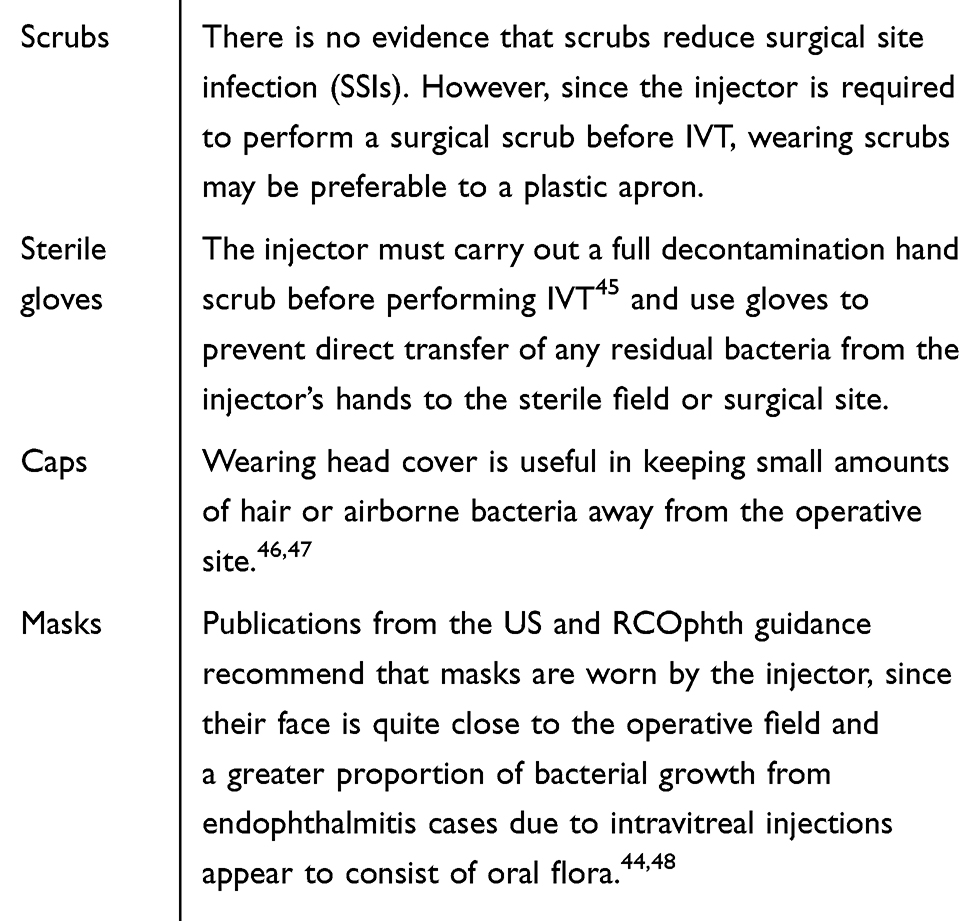
Minimum Standards for Clean Room Attire
Variations in dress code exist among units undertaking IVT. While there is evidence of surgical site infection no studies have been carried out in the clean rooms used for ophthalmology, particularly those for IVT. The advice on minimum standards should be considered alongside that of your local infection control team:
 |
|
Drug Accountability
Anti-VEGF agents require refrigeration and may be sensitive to temperature fluctuation. Therefore, these agents must be maintained between 2°C and 8°C when in storage.49 Further guidance on the safe and secure handling of medicines is given by the Royal Pharmaceutical Society of Great Britain.50
Prophylactic Use of Antibiotic Drops
Historically, the drug licence for anti-VEGF agents recommended the use of pre- and post-operative antibiotics to minimise the risk of infection.51 Similarly, the licences for newer anti-VEGF agents have included such prophylaxis recommendations. However, there is now a growing body of evidence, which strongly suggests that antibiotics do not meaningfully lower the risk of post-injection endophthalmitis,52–56 The authors of this publication adhere to RCOphth intravitreal guidelines and do not routinely prescribe topical antibiotics.57 If there are any signs of conjunctival infection or chronic blepharitis in the eye to be injected, advice must be taken from the ophthalmologist in charge as to the appropriate actions to be taken to safeguard the patient. This may involve postponing the injection until the infection is cleared or prescribing a course of topical antibiotics.
Patient Safety in the Clean Room
An intravitreal injection is an invasive procedure that meets the criteria defined by the national patient safety standards ‘Any interventional procedures performed in operating theatres or outpatient treatment areas’.42 Thus, it is important that there are agreed policies and procedures in place that define how staff working in clean rooms communicate with each other about surgical matters. Effective communication between clinical personnel before, during, and after procedures minimises the risk of adverse events.
All NHS theatres have a core set of safety checks identified for improving performance at safety critical time points within the patients intraoperative care pathway this best practice needs to be replicated in some form in the intravitreal clean room to deliver safe care for patients undergoing intravitreal injections.
Whether electronic or paper documentation it must be designed in such a way that key safety checks in the patient pathway are performed in sequence and are documented.
Checks to include:
- Patient identification
- Planned procedure
- Correct eye/eyes marked
- Correct drug and expiry date
- Sterility of the procedure pack
- Allergies
- Valid consent — ensure that the consent and the notes include, when appropriate, the side to be operated on using the words “left” or “right” in full58
It is vitality important, in light of the ageing population that receive intravitreal injections, that not only do you check that a consent is present but you need to establish that the patient still has the capacity to give consent as per the requirements of the Mental Capacity Act (2005) and document that this has taken place before each injection.59
If there is any doubt that the patient does not have the capacity you must act in your patient’s best interests as to whether to or not to proceed and, where relevant, seek consent from a person authorised with a lasting power of attorney to give consent on behalf of your patient.
Telemedicine IT
In order to facilitate continuous audit and permit paperless care across multiple locations, a MR service should have access to networked electronic patient record (EPR). Networked peripheral locations linked to the main hub could include GP practices, mobile units, or at premises in a shopping mall, all of which have already occurred at various units in the UK.
EPR systems also have other benefits: if imaging can be networked with local optometry practices, this would permit virtual review of patients’ OCT scans, such that some face to face referrals may not be necessary, and this would result in more cost-effective care for the NHS. Moreover, subject to clinical governance oversight, if community optometrists could upload information to the EPR system, or indeed have fuller access, then enhanced community shared care working with optometrists could be hugely facilitated. Many units already have shared-care optometrists working within the hospital setting, and such trained individuals, if they had access to EPR/networked imaging, could potentially work in a similar manner in their high street practices, under the auspices and clinical governance of the main hospital eye service retinal unit. In this scenario, community optometrists must be able to provide optimal images/scan protocols and ideally these would be transferrable into HES. Formal policies need to be considered to ensure confidentially is maintained. In addition, since May 2018 there has been guidance on how personal data is governed and handled. A national GDPR working group and Information Governance Alliance have created official guidance for the NHS on handing personal data and adhering to GDPR.60
The RCOphth has published a useful review of the positives of using an EPR together with potential risks/pitfalls.61 The consensus of this group is that EPRs are particularly beneficial for areas in Ophthalmology where high throughput follow-up episodes are needed such as medical retina.
It is essential that there is rapid access to appropriate IT support, so that technical issues with EPR or imaging do not cause major disruption to clinical work. Ideally, a unit should have a dedicated individual responsible for imaging or other IT queries. The availability of appropriate server space and networking capabilities should be taken into account when new pieces of imaging equipment are acquired. Having sufficient server capacity, connection speeds and appropriate clinic computer hardware/software to allow efficient clinical work are also vital.
Data Collections EPR/Audit and KPIs/Outcomes
Electronic Patient Records in Ophthalmology
Electronic Patient records (EPRs) are increasingly used by clinical teams to record clinical care in a standardised way and to measure the quality of the services they provide61,62 The RCOphth have developed a document based on published evidence and consensus expert opinion, that highlights key elements of how EPRs can best support services and the delivery of high-quality care.61
This document includes what to consider when planning an EPR, including transitioning from historic paper notes, ensuring realistic launch programme, and robust contingencies for data backup.
EPRs should allow the capture of minimum structured data in line with agreed datasets to ensure accurate audits and allow frequently asked questions to be input by non-consultant grade HCPs.
- EPRs should facilitate clinical audits, including contribution to national audit programmes and allow the assessment of the performance of a service, in addition, the EPR should facilitate research and collection of enhanced datasets.
- A survey was conducted to understand the current snapshot of EPR use across ophthalmology units in the UK.63
- A significant proportion of units were engaging with EPR or planned to do so in the future.
- A 45.3% (n=48) of the units who responded were currently using an EPR and a further 26.4% (n=28) planned to implement EPR within 2 years.
- The study concluded that EPR has the potential to address current limitations of patient information transfer and sharing in ophthalmology.
- However, differing EPR systems and lack of remote access mean further optimisation of these record systems are needed to allow data transfer between units.
- EPRs with clear and accurate data with appropriate datasets offer the ability to capture the data of large numbers of patients and assess real-life outcomes of clinical practice.64
- Regular review of safety and visual outcome audits in EPRs can accurately track the response of new treatment pathways, new treatment modalities or local delivery issues65 and potentially influence pathways on a national scale.
- EPR outcome data may affect national clinical pathways if sufficient outcome data is available.37,66
Key Performance Indicators in Retinal Service Delivery
Quality of service in relation to macular treatments may be measured according to nationally agreed standards and local service-specific metrics. Reporting against such standards can be important when planning services with commissioners who fund treatment and are also necessary for eye departments when business planning and allocating resources.
The following standards may be considered in this context.
Service Delivery–Related
Time to First Treatment: Target 100%
Many of the disease indications treated with intravitreal anti-VEGF injections require urgent treatment initiation in particular choroidal neovascularisation in patients with wet age-related macular degeneration and myopic choroidal neovascularisation. The RCOphth and NICE advise that the first treatment for a patient affected by nAMD should be within 2 weeks of referral.37,38,67
Review Intervals
The duration of anti-VEGF therapy action varies depending on the disease, drug and individual patient. Modern treatment regimens aim to customise the treatment according to the needs of patients but depend on the capacity to deliver appointments at the treatment interval required. An optimal service is able to deliver treatment according to the required management plan. A local target may be set based on overall service capacity aiming to continue to build capacity so review appointments can be within one to 2 weeks of the required date.
Outcomes-Related
Maintenance of Visual Acuity
Most clinical trials of anti-VEGF therapy have used mean vision gain over a period of time as a primary endpoint for analysis. However, such gains are often not achieved in real-world clinical practice. This may be due to a number of differences, including case mix not bound by the inclusion/exclusion of a clinical trial, service delivery, compliance with appointments. A low mean vision gain may actually reflect an exceptionally good referral pathway treating patients earlier when vision is high so that scope for improvement is limited due to a “ceiling effect”. Visual acuity decline over time can occur due to service delivery problems but may also be simply part of the natural history of the disease (atrophy) despite optimally delivered treatment. The steering committee considered the stability of mean vision change between months 6 to 12 in the first year and months 12 to 24 as metrics aiming for stability to be defined as within 5 letters change during this period.
Adverse Events
The most serious adverse event related to intravitreal injection therapy is endophthalmitis. As clinical practice and experience has developed over the years this has declined. There is no current nationally reported standard, but the British Ophthalmological Surveillance Unit set up by The RCOphth most recently reviewed this and estimated a rate of 0.025% which may be used as a current benchmark. Real-world data and RCT data report incidences of between 0.02% and 0.09%.19,20,25,68–74
Patient Experience–Related
It is important for eye departments to have feedback from patients in relation to their overall satisfaction with the service. This may be questionnaire-based asking patients for their overall opinion and comments on the service. A common standard used in NHS across specialties is the “friends and family test.” This is defined as the likelihood that patients would recommend the service they have experienced to their family and friends. This should be benchmarked across the hospital service as a whole but a target of 90%+ of patients likely or highly likely to recommend the service is desirable. In addition, ICHOM have developed the Standard Set for Macular Degeneration, a recommendation of the outcomes that have an impact on patients including disutility of care, visual functioning and HRQoL, which is available as leaflets and reference guides.75 From an international perspective, several patient-reported outcome measures assessing the vision-related quality of life have also been developed and implemented.76
Miscellaneous Standards
Other generic standards may be used across hospital services and may be of value to record and report in relation to macular service delivery. This may include:
- Patient retention/drop-out from the service over defined timescales. This can help with service planning.
- The number of patients failing to attend an appointment, often called “DNA” which stands for “Did not attend” and also the number of appointments cancelled as the patient was “unable to attend” often termed “UTA” rates. These can affect service efficiency and measures to keep these low should be considered at the individual department level.
- Complaints and response to complaints within hospital-expected timescales.
- Duty of candour events. This can be a reflection of clinical incidents occurring within a department.
- Incidence of blindness and visual impairment within the service secondary to AMD.77 This can be a reflection on the ability of the service to deliver a timely and safe pathway.
All departments may vary in terms of which specific metrics they feel require the greatest focus and the frequency of reporting. However, working according to recognised key performance indicators can allow benchmarking and standardisation and encourage greater dialogue with commissioners to enable support for the continuation of services to a high standard.
Staff Training and Governance
Demand and Resource in the Medical Retina Service
According to the Action on AMD and The Way Forward publications, clinical capacity issues are, in part, a result of shortages in the numbers of key staff and/or inadequacies in skills and training.1,2 Improved efficiency through sustainable service adaptations could counteract the growing disparity between demand and resource,1,2 including expanded roles for non-medical ophthalmic HCPs.1,11 By ensuring that orthoptists, optometrists and ophthalmic nurses have the appropriate knowledge, skills and support, and are trained to perform functions of medical staff, consultant ophthalmologists can be freed up to take on advanced roles in the clinical care pathway.1,2
However, the safe delegation of tasks from consultants to non-medical HCPs necessitates recognised and identifiable levels of competence, supported by education and training.10,57 As such, a nationally agreed competency framework outlining standardised training has been published to help develop an upskilled, multidisciplinary workforce that is able to facilitate service capacity for the MR service.10
The Ophthalmology Common Clinical Competency Framework
The Ophthalmology Common Clinical Competency Framework (the Framework), developed in 2016 by The RCOphth, The Royal College of Nursing (RCN), The British & Irish Orthoptic Society (BIOS) and the College of Optometrists, sets out guidance regarding the knowledge and skills (competences) that non-medical ophthalmic HCPs in secondary care must possess in order to safely and successfully undertake expanded roles.10 The Framework is written for use across the UK and covers four clinical areas, including medical retina.10,11 There are three levels of competences for each clinical area which are set out in a hierarchical fashion (Levels 1 to 3).10 An HCP must possess a basic set of generic skills before undertaking further training for a Level 1-expanded role (and beyond).10,11
A curriculum is currently being mapped to the Advanced Clinical Practice (ACP) framework at Level 3 to coordinate with the Apprenticeship programme, which will help services train HCPs.57,78–80 Training can be arranged locally and should include a range of topics.67,81–83
Intravitreal Injection Therapy
As per the Framework, delegated HCPs in a Level 3-expanded MR role should be capable of dealing with certain needs of ophthalmic patients, including the administration of pharmacological interventions such as intravitreal injection therapy (IVT).10 The training and accreditation of such HCPs must be fully approved locally by a trust governance committee.57 Training for IVT should include wetlab sessions and, only after basic competency is achieved in wetlab, can a delegated HCP be introduced to IVT on patients (Box 1).83–86 Thereafter, a set number of injection procedures must be performed under supervision before independent injections are permissible.11,12,14–16,82–86
The supervising consultant ophthalmologist of the delegated HCP has the responsibility of ensuring that they are suitably trained, competent and sufficiently experienced, as per General Medical Council (GMC 2013) guidance on Good Medical Practice (GMP).17 The care afforded by the delegated HCP should be supported by local policy or protocols, and a regular clinical audit of processes and outcomes should be conducted to ensure good patient care is being provided.67,78,79
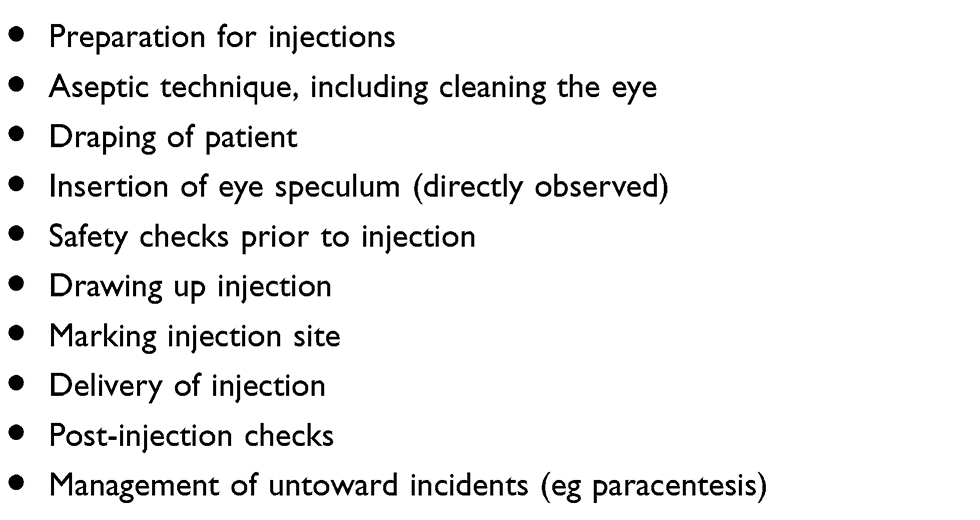 |
Box 1 A Delegated HCP Should Be Provided with Practical Training on |
The RCOphth has published an Ophthalmic Service Guidance regarding IVT (2018). The guidance is designed for easy reference and provides advice about performing IVT as safely as possible, with its recommendations based on published high-quality evidence and expert consensus.39,81
Sufficient clinical capacity to counterbalance ever-growing demand presents an unmet need across many UK MR services. The implementation of a nationwide framework of standardised and recognised training will allow non-medical ophthalmic HCPs to take on expanded roles, helping to manage demand for nAMD treatment within the MR service while continuing to meet minimum standards and delivering safe and efficient patient care.
Summary
Providing services for patients with nAMD continues to challenge HCPs in the secondary care sector after more than a decade since the intravitreal therapy era began. During this time we have seen the development of a range of multidisciplinary strategies that help us to provide a safe and effective service. In this article, we have collated the evidence and signposts to necessary guidelines from a group of experienced lead clinicians which should provide the core essentials in the toolkit for providing an AMD service. This resource should be useful for us to align our infrastructures and clinical governance mechanisms across the secondary care departments within our national service.
Abbreviations
AMD, age-related macular degeneration; DMO, diabetic macular oedema; DR, diabetic retinopathy; EPR, electronic patient record; HCP, healthcare professional; IOP, intraocular pressure; IVT, intravitreal injection therapy; KPI, key performance indicator; MR, medical retina; nAMD, neovascular (wet) age-related macular degeneration; NatSSIPs, National Safety Standards for Invasive Procedures; NICE, The National Institute for Health and Care Excellence; OCT, optical coherence tomography; PRN, pro re nata; RCOphth, The Royal College of Ophthalmologists; SMC, Scottish Medicines Consortium; SOP, standard operating procedure; SSI, surgical site infection; T&E, Treat and Extend; UWF, ultra-widefield; VA, visual acuity; VEGF, vascular endothelial growth factor.
Acknowledgments
The views and opinions of the authors are not necessarily those of Novartis or the publisher. This supplement and the group that developed it were sponsored by Novartis Pharmaceuticals UK Ltd. All authors received honoraria, contributed to the development of the manuscript, and retained final control of the content and editorial decisions. Medical writing assistance was provided by Daniel Webber, Rock Unlimited. Four meetings were held between May 2018 and November 2019 to discuss the consensus for the article. Novartis has checked that the content was factually accurate, balanced, and compliant with the Association of the British Pharmaceutical Industry Code of Practice.
Disclosure
Winfried Amoaku has received research grants from Allergan, Bayer, CentreVue, Boehringer Ingelheim, Novartis; Educational travel grants from Alimera, Allergan, Bayer, Novartis and honoraria for Advisory Board Memberships from Abbvie, Alimera, Allergan, Bayer, Novartis, and Roche. Clare Bailey has received grant funding for advisory board work/travel support from Novartis, Bayer, Roche, Bristol Eye Hospital, Alimera Sciences, and has received research funding from Bayer, Novartis, Allergan, Boehringer Ingelheim, and Roche. Louise Downey has received research funding from Allergan, Bayer, Heidelburg, Novartis, Alimera, Roche, educational travel grants from Allergan, Bayer, Novartis and Honoraria for Advisory Boards/speakers fees from Alimera, Bayer, Novartis, Bausch and Lomb. Richard Gale has conducted consultancy advisory boards for Novartis, Bayer and Allergan, Alimera, Santen, received educational travel grants from Novartis, Bayer, Allergan, Heidelberg and departmental research from Allergan, Bayer, Novartis, and Roche. Faruque Ghanchi has received honorarium for consultancy-advisory boards from Alimera, Allergan, Bayer, Novartis, Oxford BioElectronics, Roche; educational travel grants from Allergan, Bayer, Novartis and departmental research grants from Allergan, Bayer, Boehringer Ingelheim, Chengdu Pharma, Novartis, PanOptica, Roche. Robin Hamilton has received non-financial assistance, personal fees, and been advisor to Novartis, Bayer, Allergan, Roche, and Ellex. Sajjad Mahmood has received lecture fees from Bayer and Novartis, consultancy fees from Alimera, Bayer, Novartis, Travel fees from Bayer and Novartis and Research funding from Bayer, Novartis and Roche. Geeta Menon has conducted consultancy advisory boards for Novartis, Bayer and Allergan, received educational travel grants from Novartis, Bayer, Allergan; and departmental research from Allergan, Bayer, Boehringer Ingelheim, Chengdu Pharma, Novartis, PanOptica, and Roche. Jenny Nosek has received honorarium from Novartis, Bayer and Zeiss. Yit Yang has received personal fees and non-financial assistance from Novartis, Bayer, Allergan, and Roche. Ian Pearce has received lecture fees from Allergan, Bayer, Heidelberg and Novartis, consultancy fees from Allergan, Alimera, Bayer and Novartis and travel fees from Allergan, Bayer and Novartis. The authors report no other conflicts of interest in this work.
References
1. Amoaku W, Blakeney S, Freeman M, et al. Action on AMD. Optimising patient management: act now to ensure current and continual delivery of best possible patient care. Eye (Lond). 2012;26(Suppl 1):S2–S21. doi:10.1038/eye.2011.343
2. The Royal College of Ophthalmologists (RCOphth). The Way Forward. Options to Help Meet Demand for the Current and Future Care of Patients with Eye Disease —age-Related Macular Degeneration and Diabetic Retinopathy. London: RCOphth; 2017. Available from: https://www.rcophth.ac.uk/wp-content/uploads/2015/10/RCOphth-The-Way-Forward-AMD-300117.pdf.
3. Foot B, MacEwen C. Surveillance of sight loss due to delay in ophthalmic treatment or review: frequency, cause and outcome. Eye (Lond). 2017;31(5):771–775. doi:10.1038/eye.2017.1
4. National Institute of Health and Clinical Excellence (NICE). Ranibizumab and Pegaptanib for the Treatment of Age-Related Macular Degeneration. NICE Technology Appraisal Guidance TA155. London: NICE; 2008. Available from: www.nice.org.uk/guidance/ta155/resources/ranibizumab-and-pegaptanib-for-the-treatment-of-agerelated-macular-degeneration-pdf-82598316423109.
5. Scottish Medicines Consortium (SMC). Ranibizumab 10mg/Ml Solution for Intravitreal Injection (Lucentis®). SMC No. (381/07). Glasgow: SMC; 2007. Available from: www.scottishmedicines.org.uk/media/2217/ranibizumab_10mgmlsolution_intravitrealinjection_lucentis_38107.pdf.
6. National Institute of Health and Clinical Excellence (NICE). Aflibercept Solution for Injection for Treating Wet Age-Related Macular Degeneration. NICE Technology Appraisal Guidance TA294. London: NICE; 2013. Available from: https://www.nice.org.uk/guidance/ta294/resources/aflibercept-solution-for-injection-for-treating-wet-agerelated-macular-degeneration-pdf-82600733390533.
7. Aflibercept 40mg/mL solution for injection (Elyea®). SMC No. (1074/15). Glasgow: SMC; 2005. Available from: https://www.scottishmedicines.org.uk/media/1215/aflibercept__eylea__final_august_2015amend020915_for_website.pdf2005.
8. Ghazala F, Hovan M, Mahmood S. Improving treatment provision of Wet AMD with intravitreal ranibizumab. BMJ Qual Improv Rep. 2013;2(1):1–5.
9. The Royal College of Ophthalmologists (RCOphth). Maximising Capacity in AMD Services. London: RCOphth; 2013. Available from: www.rcophth.ac.uk/wp-content/uploads/2014/12/2013-sci-302-maximising-capacity-in-amd-services-july-2013.pdf.
10. The Royal College of Ophthalmologists (RCOphth). The Common Clinical Competency Framework for Non-Medical Ophthalmic Healthcare Professionals in Secondary Care — Setting Out Guidance and Benefits. London: RCOphth; 2016. Available from: www.rcophth.ac.uk/wp-content/uploads/2017/01/CCCF-HCPs.pdf.
11. The Royal College of Ophthalmologists (RCOphth). The Common Clinical Competency Framework for Non-Medical Ophthalmic Healthcare Professionals in Secondary Care — Medical Retina. London: RCOphth; 2016. Available from: www.rcophth.ac.uk/wp-content/uploads/2017/01/cccf-medical-retina.pdf.
12. Hatz K, Prunte C. Treat and extend versus pro re nata regimens of ranibizumab in neovascular age-related macular degeneration: a comparative 12 Month study. Acta Ophthalmol. 2017;95(1):e67–e72. doi:10.1111/aos.13031
13. Gale RPG. What is the best neovascular age-related macular degeneration treatment regime for 2016? European Ophthalmic Review. 2015;9(2):157–158.
14. Wykoff CC, Croft DE, Brown DM, et al. Prospective trial of treat-and-extend versus monthly dosing for neovascular age-related macular degeneration: TREX-AMD 1-year results. Ophthalmology. 2015;122(12):2514–2522. doi:10.1016/j.ophtha.2015.08.009
15. Wykoff CC, Ou WC, Croft DE, et al. Neovascular age-related macular degeneration management in the third year: final results from the TREX-AMD randomised trial. Br J Ophthalmol. 2018;102(4):460–464. doi:10.1136/bjophthalmol-2017-310822
16. Berg K, Pedersen TR, Sandvik L, Bragadottir R. Comparison of ranibizumab and bevacizumab for neovascular age-related macular degeneration according to LUCAS treat-and-extend protocol. Ophthalmology. 2015;122(1):146–152. doi:10.1016/j.ophtha.2014.07.041
17. Silva R, Berta A, Larsen M, et al. Treat-and-Extend versus monthly regimen in neovascular age-related macular degeneration: results with ranibizumab from the TREND study. Ophthalmology. 2018;125(1):57–65. doi:10.1016/j.ophtha.2017.07.014
18. Kertes PJ, Galic IJ, Greve M, et al. Canadian treat-and-extend analysis trial with ranibizumab in patients with neovascular age-related macular disease: one-year results of the randomized Canadian treat-and-extend analysis trial with ranibizumab study. Ophthalmology. 2019;126(6):841–848. doi:10.1016/j.ophtha.2019.01.013
19. Brown DM, Michels M, Kaiser PK, et al. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: two-year results of the ANCHOR study. Ophthalmology. 2009;116(1):57–65.e55. doi:10.1016/j.ophtha.2008.10.018
20. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419–1431. doi:10.1056/NEJMoa054481
21. Heier JS, Brown DM, Chong V, et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012;119(12):2537–2548. doi:10.1016/j.ophtha.2012.09.006
22. Regillo CD, Brown DM, Abraham P, et al. Randomized, double-masked, sham-controlled trial of ranibizumab for neovascular age-related macular degeneration: PIER Study year 1. Am J Ophthalmol. 2008;145(2):239–248. doi:10.1016/j.ajo.2007.10.004
23. Gillies MC, Campain A, Barthelmes D, et al. Long-term outcomes of treatment of neovascular age-related macular degeneration: data from an observational study. Ophthalmology. 2015;122(9):1837–1845. doi:10.1016/j.ophtha.2015.05.010
24. Vardarinos A, Gupta N, Janjua R, Iron A, Empeslidis T, Tsaousis KT. 24-month clinical outcomes of a treat-and-extend regimen with ranibizumab for wet age-related macular degeneration in a real life setting. BMC Ophthalmol. 2017;17(1):58. doi:10.1186/s12886-017-0451-1
25. Kim LN, Mehta H, Barthelmes D, Nguyen V, Gillies MC. Metaanalysis of real-world outcomes of intravitreal ranibizumab for the treatment of neovascular age-related macular degeneration. Retina. 2016;36(8):1418–1431. doi:10.1097/IAE.0000000000001142
26. Amoaku W, Balaskas K, Cudrnak Tet al,. Initiation and maintenance of a Treat-and-Extend regimen for ranibizumab therapy in wet age-related macular degeneration: Recommendations from the UK Retinal Outcomes Group. Clin Ophthalmol. 2018;12:1731–1740. doi:10.2147/OPTH.S174560.
27. Gupta OP, Shienbaum G, Patel AH, Fecarotta C, Kaiser RS, Regillo CD. A treat and extend regimen using ranibizumab for neovascular age-related macular degeneration clinical and economic impact. Ophthalmology. 2010;117(11):2134–2140. doi:10.1016/j.ophtha.2010.02.032
28. Engelbert M, Zweifel SA, Freund KB. “Treat and extend” dosing of intravitreal antivascular endothelial growth factor therapy for type 3 neovascularization/retinal angiomatous proliferation. Retina. 2009;29(10):1424–1431. doi:10.1097/IAE.0b013e3181bfbd46
29. The Royal College of Ophthalmologists (RCOphth). Ophthalmic Services Guidance — Standards for Virtual Clinics in Glaucoma Care in the NHS Hospital Eye Service. London: RCOphth. Available from: www.rcophth.ac.uk/wp-content/uploads/2017/03/virtual-glaucoma-clinics.pdf.
30. Lee JX, Manjunath V, Talks SJ. Expanding the role of medical retina virtual clinics using multimodal ultra-widefield and optical coherence tomography imaging. Clin Ophthalmol. 2018;12:2337–2345. doi:10.2147/OPTH.S181108
31. Balaskas K, Gray J, Blows P, et al. Management of choroidal naevomelanocytic lesions: feasibility and safety of a virtual clinic model. Br J Ophthalmol. 2016;100(5):665–670. doi:10.1136/bjophthalmol-2015-307168
32. Clarke J, Puertas R, Kotecha A, Foster PJ, Barton K. Virtual clinics in glaucoma care: face-to-face versus remote decision-making. Br J Ophthalmol. 2017;101(7):892–895. doi:10.1136/bjophthalmol-2016-308993
33. Tsaousis KT, Empeslidis T, Konidaris VE, et al. The concept of virtual clinics in monitoring patients with age-related macular degeneration. Acta Ophthalmol. 2016;94(5):e353–e355. doi:10.1111/aos.12832
34. Kelly SP, Wallwork I, Haider D, Qureshi K. Teleophthalmology with optical coherence tomography imaging in community optometry. Evaluation of a quality improvement for macular patients. Clin Ophthalmol. 2011;5:1673–1678. doi:10.2147/OPTH.S26753
35. England PH. Diabetic eye screening: retinal image grading criteria. 2017; Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/582710/Grading_definitions_for_referrable_disease_2017_new_110117.pdf.
36. Manjunath V, Papastavrou V, Steel DH, et al. Wide-field imaging and OCT vs clinical evaluation of patients referred from diabetic retinopathy screening. Eye (Lond). 2015;29(3):416–423. doi:10.1038/eye.2014.320
37. National Institute of Health and Clinical Excellence (NICE). Age-Related Macular Degeneration. NICE Guideline NG82. London: NICE; 2018. Available from: www.nice.org.uk/guidance/ng82/resources/agerelated-macular-degeneration-pdf-1837691334853.
38. National Institute of Health and Clinical Excellence (NICE). Serious Eye Disorders. Quality Standard QS180. London: NICE; 2019. Available from: https://www.nice.org.uk/guidance/qs180/resources/serious-eye-disorders-pdf-75545714656213.
39. The Royal College of Ophthalmologists. Ophthalmic IMAGING - OPHTHALMIC SERVICES GUIDANCE: 2016. Available from: https://www.rcophth.ac.uk/wp-content/uploads/2014/12/Ophthalmic-Imaging-November-2016.pdf.
40. Rodriguez FJ, Staurenghi G, Gale R. Vision Academy Steering C. The role of OCT-A in retinal disease management. Graefes Arch Clin Exp Ophthalmol. 2018;256(11):2019–2026. doi:10.1007/s00417-018-4109-3
41. The Royal College of Ophthalmologists. Update on retinal imaging: OCT angiography: 2016. Available from: https://www.rcophth.ac.uk/wp-content/uploads/2015/02/College-News-Focus-July-2016-FINAL.pdf.
42. National Health Service (NHS) England. National Safety Standards for Invasive Procedures (Natssips). London: NHS England; 2015. Available from: www.improvement.nhs.uk/documents/923/natssips-safety-standards.pdf.
43. National Health Service (NHS) England. Surgical Never Events Taskforce Report. London: NHS England; 2014. Available from: www.improvement.nhs.uk/documents/922/sur-nev-ev-tf.pdf.
44. The Royal College of Ophthalmologists (RCOphth). Intravitreal Injection Therapy. London: RCOphth; 2018. Available from: www.rcophth.ac.uk/wp-content/uploads/2018/02/intravitreal-injection-therapy-august-2018-2.pdf.
45. Tanner J, Swarbrook S, Stuart J. Surgical hand antisepsis to reduce surgical site infection. Cochrane Database Syst Rev. 2008;(1):CD004288.
46. Mastro TD, Farley TA, Elliott JA, et al. An outbreak of surgical-wound infections due to group A streptococcus carried on the scalp. N Engl J Med. 1990;323(14):968–972. doi:10.1056/NEJM199010043231406
47. Friberg B, Friberg S, Ostensson R, Burman LG. Surgical area contamination–comparable bacterial counts using disposable head and mask and helmet aspirator system, but dramatic increase upon omission of head-gear: an experimental study in horizontal laminar air-flow. J Hosp Infect. 2001;47(2):110–115. doi:10.1053/jhin.2000.0909
48. Pilli S, Kotsolis A, Spaide RF, et al. Endophthalmitis associated with intravitreal anti-vascular endothelial growth factor therapy injections in an office setting. Am J Ophthalmol. 2008;145(5):879–882. doi:10.1016/j.ajo.2007.12.036
49. Kelly SP, Barua A. A review of safety incidents in England and Wales for vascular endothelial growth factor inhibitor medications. Eye (Lond). 2011;25(6):710–716. doi:10.1038/eye.2011.89
50. Royal Pharmaceutical Society of Great Britain (RPSGB). The Safe and Secure Handling of Medicines: A Team Approach. London: RPSGB; 2018. Available from: www.rpharms.com/portals/0/rps%20document%20library/open%20access/publications/safe%20and%20secure%20handling%20of%20medicines%202005.pdf.
51. Lucentis® 10 mg/mL solution for injection summary of product characteristics. 2018. Available from: www.medicines.org.uk/emc/product/307/smpc.
52. Kim SJ, Toma HS. Antimicrobial resistance and ophthalmic antibiotics: 1-year results of a longitudinal controlled study of patients undergoing intravitreal injections. Arch Ophthalmol. 2011;129(9):1180–1188. doi:10.1001/archophthalmol.2011.213
53. Cheung CS, Wong AW, Lui A, Kertes PJ, Devenyi RG, Lam WC. Incidence of endophthalmitis and use of antibiotic prophylaxis after intravitreal injections. Ophthalmology. 2012;119(8):1609–1614. doi:10.1016/j.ophtha.2012.02.014
54. Bhatt SS, Stepien KE, Joshi K. Prophylactic antibiotic use after intravitreal injection: effect on endophthalmitis rate. Retina. 2011;31(10):2032–2036. doi:10.1097/IAE.0b013e31820f4b4f
55. Storey P, Dollin M, Pitcher J, et al. The role of topical antibiotic prophylaxis to prevent endophthalmitis after intravitreal injection. Ophthalmology. 2014;121(1):283–289. doi:10.1016/j.ophtha.2013.08.037
56. Minims® Povidone Iodine 5% w/v eye drops, solution summary of product characteristics. 2017. Available from: www.medicines.org.uk/emc/product/3018/smpc.
57. The Royal College of Ophthalmologists. Ophthalmic Service Guidance. Intravitreal injection therapy London: rCOphth: 2018. Available from: https://www.rcophth.ac.uk/wp-content/uploads/2018/02/Intravitreal-Injection-Therapy-August-2018-2.pdf.
58. NHS. Consent to treatment 2019. Available from: https://www.nhs.uk/conditions/consent-to-treatment/.
59. NHS. Mental Capacity Act. 2005. Available from: https://www.nhs.uk/conditions/social-care-and-support-guide/making-decisions-for-someone-else/mental-capacity-act/.
60. National Health Service (NHS) Digital. General Data Protection Regulation (GDPR) guidance: NHS Digital 2018. Available from: https://digital.nhs.uk/data-and-information/looking-after-information/data-security-and-information-governance/information-governance-alliance-iga/general-data-protection-regulation-gdpr-guidance.
61. The Royal College of Ophthalmologists. Electronic medical records - Standards for UK ophthalmology services: 2018. Available from: https://www.rcophth.ac.uk/wp-content/uploads/2018/06/Electronic-Medical-Records-Standards-for-UK-Ophthalmology-Services.pdf.
62. Elliott AF, Davidson A, Lum F, et al. Use of electronic health records and administrative data for public health surveillance of eye health and vision-related conditions in the United States. Am J Ophthalmol. 2012;154(6 Suppl):S63–70. doi:10.1016/j.ajo.2011.10.002
63. Lim SB, Shahid H. Distribution and extent of electronic medical record utilisation in eye units across the United Kingdom: a cross-sectional study of the current landscape. BMJ Open. 2017;7(5):e012682. doi:10.1136/bmjopen-2016-012682
64. Writing Committee for the UKA-RMDEMRUG. The neovascular age-related macular degeneration database: multicenter study of 92 976 ranibizumab injections: report 1: visual acuity. Ophthalmology. 2014;121(5):1092–1101. doi:10.1016/j.ophtha.2013.11.031
65. Lee AY, Lee CS, Egan CA, et al. UK AMD/DR EMR REPORT IX: comparative effectiveness of predominantly as needed (PRN) ranibizumab versus continuous aflibercept in UK clinical practice. Br J Ophthalmol. 2017;101(12):1683–1688. doi:10.1136/bjophthalmol-2016-309818
66. Lee AY, Lee CS, Butt T, et al. UK AMD EMR USERS GROUP REPORT V: benefits of initiating ranibizumab therapy for neovascular AMD in eyes with vision better than 6/12. Br J Ophthalmol. 2015;99(8):1045–1050. doi:10.1136/bjophthalmol-2014-306229
67. The Royal College of Ophthalmologists. Age-related macular degeneration: guidelines for management: 2013. Available from: http://www.rcophth.ac.uk/wp-content/uploads/2014/12/2013-SCI-318-RCOphth-AMD-Guidelines-Sept-2013-FINAL-2.pdf.
68. Fintak DR, Shah GK, Blinder KJ, et al. Incidence of endophthalmitis related to intravitreal injection of bevacizumab and ranibizumab. Retina. 2008;28(10):1395–1399. doi:10.1097/IAE.0b013e3181884fd2
69. Cavalcante LL, Cavalcante ML, Murray TG, et al. Intravitreal injection analysis at the Bascom Palmer Eye Institute: evaluation of clinical indications for the treatment and incidence rates of endophthalmitis. Clin Ophthalmol. 2010;4(519–524).
70. Klein KS, Walsh MK, Hassan TS, et al. Endophthalmitis after anti-VEGF injections. Ophthalmology. 2009;116(6):1225 e1221. doi:10.1016/j.ophtha.2009.02.031
71. Chang TS, Bressler NM, Fine JT, et al. Improved vision-related function after ranibizumab treatment of neovascular age-related macular degeneration: results of a randomized clinical trial. Arch Ophthalmol. 2007;125(11):1460–1469. doi:10.1001/archopht.125.11.1460
72. Boyer DS, Heier JS, Brown DM, Francom SF, Ianchulev T, Rubio RG. A Phase IIIb study to evaluate the safety of ranibizumab in subjects with neovascular age-related macular degeneration. Ophthalmology. 2009;116(9):1731–1739. doi:10.1016/j.ophtha.2009.05.024.
73. Bhavsar AR, Stockdale CR, Ferris FL
74. Storey PP, Tauqeer Z, Yonekawa Y, et al. The impact of prefilled syringes on endophthalmitis following intravitreal injection of ranibizumab. Am J Ophthalmol. 2019;199:200–208.
75. ICHOM. The standard set for macular degeneration. Available from: https://www.ichom.org/portfolio/macular-degeneration/.
76. Centre for Eye Research Australia. Patient-reported outcome questionnaires. Available from: https://www.cera.org.au/pro-questionnaires/. 2018.
77. Johnston RL, Lee AY, Buckle M, et al. UK age-related macular degeneration electronic medical record system (AMD EMR) users group Report IV: incidence of blindness and sight impairment in ranibizumab-treated patients. Ophthalmology. 2016;123(11):2386–2392. doi:10.1016/j.ophtha.2016.07.037
78. General Medical Council (GMC). Delegation and Referral. London: GMC; 2013. Available from: www.gmc-uk.org/-/media/documents/delegation-and-referral_pdf-58834134.pdf.
79. The Royal College of Ophthalmologists (RCOphth). Clinical Audit and Clinical Effectiveness in ophthalmology. London: RCOphth; 2018. Available from: www.rcophth.ac.uk/wp-content/uploads/2016/12/clinical-audit-and-clinical-effectiveness-in-ophthalmology.pdf.
80. (HEE) HEE. Multi-Professional Framework for Advanced Clinical Practice in England. London: HEE; 2017. Available from: www.hee.nhs.uk/sites/default/files/documents/multi-professionalframework foradvanced clinical practice in England.pdf.
81. Centre BM. Checklist for intravitreal injections Bradford: bradford Macular Service 2014. Available from: https://www.rcophth.ac.uk/wp-content/uploads/2015/08/BradfordTeaching-Hospitals-NHS-Trust-Macula-Service-Theatre-Checklist-October-2014.pdf.
82. Varma D, Lunt D, Johnson P, Stanley S. A novel approach to expanding the role of nurses to deliver intravitreal injections for patients with age-related macular degeneration. Int J Ophthalmic Prac. 2013;6(1):68–72.
83. Nago J. Intravitreal injections for nurse practitioners: a guide to good practice. Int J Ophthalmic Prac. 2015;6(2):1–7. doi:10.12968/ijop.2015.6.1.1
84. Austeng D, Morken TS, Bolme S, Follestad T, Halsteinli V. Nurse-administered intravitreal injections of anti-VEGF: study protocol for noninferiority randomized controlled trial of safety, cost and patient satisfaction. BMC Ophthalmol. 2016;16(1):169. doi:10.1186/s12886-016-0348-4
85. DaCosta J, Hamilton R, Nago J, et al. Implementation of a nurse-delivered intravitreal injection service. Eye (Lond). 2014;28(6):734–740. doi:10.1038/eye.2014.69
86. Michelotti MM, Abugreen S, Kelly SP, et al. Transformational change: nurses substituting for ophthalmologists for intravitreal injections – a quality-improvement report. Clin Ophthalmol. 2014;8:755–761.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.