Back to Journals » Clinical Ophthalmology » Volume 11
Prolongation of injection interval after switching therapy from ranibizumab to aflibercept in Japanese patients with macular edema secondary to branch retinal vein occlusion
Authors Tagami M, Sai R, Fukuda M, Azumi A
Received 24 November 2016
Accepted for publication 23 December 2016
Published 22 February 2017 Volume 2017:11 Pages 403—408
DOI https://doi.org/10.2147/OPTH.S128651
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Mizuki Tagami, Ryuto Sai, Masahide Fukuda, Atsushi Azumi
Ophthalmology Department, Eye Center, Kobe Kaisei Hospital, Kobe, Hyogo, Japan
Purpose: This study was conducted to investigate the outcome of switching therapy from ranibizumab to aflibercept in Japanese patients with macular edema (ME) secondary to branch retinal vein occlusion (BRVO) in daily practice.
Materials and methods: This retrospective study enrolled 15 eyes in 15 Japanese patients with ME secondary to BRVO who had been receiving a pro re nata regimen of ranibizumab and had provided written informed consent to switch to aflibercept therapy. The intravitreal injection interval, central retinal thickness, and visual acuity were evaluated before and after switching.
Results: The mean period of ranibizumab treatment was 11.8±4.2 months. The mean observation period after switching to aflibercept was 10.6±3.4 months, and seven patients were observed for more than 12 months after switching. The mean intravitreal injection interval was prolonged by 23.6 days with aflibercept (68.2±26.4 days with ranibizumab vs 91.8±33.2 days with aflibercept; P=0.0011). The mean intravitreal injection interval just before the switch was 81.3±35.6 days and was significantly prolonged to 100.8±34.2 days just after the switch to aflibercept (P=0.0309). The mean central retinal thickness did not change before or after the switch to aflibercept (295±55 µm with ranibizumab vs 276±25 µm with aflibercept; P=0.12). The mean visual acuity also remained at an improved level after the switch. No systemic or ocular side effects were evident during the study period.
Conclusion: Switching therapy from ranibizumab to aflibercept in Japanese patients with ME secondary to BRVO prolonged the intravitreal injection interval without anatomical or functional degradation.
Keywords: branch retinal vein occlusion, macular edema, ranibizumab, aflibercept
Corrigendum for this paper has been published
Introduction
The most common cause of visual loss in patients with branch retinal vein occlusion (BRVO) is macular edema (ME). One of the main triggers of ME is overproduction of vascular endothelial growth factor (VEGF) caused by venous occlusion, and therefore, blocking the action of VEGF is expected to facilitate the management of ME secondary to BRVO. The development of VEGF inhibitors has brought new hope for improving visual acuity (VA) in patients with ME secondary to BRVO. However, intravitreal injection of anti-VEGF agents can be associated with a risk of endophthalmitis, fear for endoophthalmitis by medical managing side and patients, issues resulting from the invasive procedure, and economic burden. Additionally, because BRVO often occurs in working-age populations, frequent hospital visits for injection or examination may well be burdensome for patients.1 Ophthalmologists should attempt to alleviate these problems, and in this era in which we have several alternative treatment strategies, anti-VEGF agents, and regimens, treatment plans that are not burdensome should be considered as the optimal treatments of choice.
Aflibercept is a new anti-VEGF agent, and there are few reports on its use in ME secondary to BRVO. Wang et al2,3 demonstrated that intravitreal injection of aflibercept was useful in the treatment of Chinese BRVO patients and that aflibercept had equivalent efficacy with bevacizumab to ME secondary to BRVO. Even in the treatment of ME secondary to central retinal vein occlusion (CRVO), which is often more serious than BRVO, aflibercept was more effective than ranibizumab in reducing central retinal thickness (CRT) and suppressing the levels of aqueous VEGF.4 The effects of switching from bevacizumab or ranibizumab to aflibercept have been studied both in patients with ME secondary to BRVO and in those with ME secondary to CRVO.5–10 These studies targeted patients without sufficient response to bevacizumab or ranibizumab. In these reports, visual improvement and reduction of CRT were demonstrated in CRVO patients, and prolongation of the intravitreal injection interval was reported in both BRVO and CRVO patients. The latter finding offers hope for further prolongation of intravitreal injection intervals even in patients with sufficient response to bevacizumab or ranibizumab.
In this study, we evaluated the change in the intravitreal injection interval as well as anatomical and functional changes after switching therapy from ranibizumab to aflibercept in Japanese patients with ME secondary to BRVO in our hospital.
Materials and methods
This retrospective study was approved by the ethics committee of Kobe Kaisei Hospital, and written informed consent was obtained from all study participants.
In our hospital, switching therapy from ranibizumab to aflibercept was strongly recommended to all patients with ME secondary to BRVO and who had been receiving a pro re nata (PRN) regimen of ranibizumab since December 2013. This retrospective study enrolled 15 eyes in 15 patients who had provided informed consent to switch to therapy with aflibercept from September 2015 and been observed for more than 6 months after switching.
The participants were examined for exacerbation every month, they all kept their appointments, and if any sign of exacerbation was detected, they were treated with intravitreal injection of ranibizumab or aflibercept later the same day if possible or within a week at most. We defined the signs of exacerbation as any decrease in VA from a previous examination and CRT >300 μm.
Intravitreal aflibercept injection was performed as described previously.11 Topical anesthesia was induced using 4% lidocaine eye drops, and then the eyelid, eyelashes, and periorbital area were thoroughly cleaned with povidone–iodine. A lid speculum was inserted, and additional topical anesthetic eye drops were administered and 2 mg (0.05 mL) of aflibercept (Eylea®; Bayer Schweiz AG, Zurich, Switzerland) was injected into the vitreous cavity with a 30-gauge needle through the pars plana. Thereafter, ofloxacin ointment was applied, and the eye was covered with a patch. Moxifloxacin eye drops were self-administered three times a day for 3 days after injection.
The primary outcome measure was change in the injection interval during the ranibizumab treatment period and the aflibercept treatment period. Secondary outcome measures were CRT, transition of best-corrected VA (BCVA), and safety. Mean intervals and CRT values were calculated using all the data from every administration or examination during each test drug phase. Optical coherence tomography (OCT) images were obtained using spectral domain OCT (Heidelberg Engineering, Heidelberg, Germany). Mean retinal thickness of the area corresponding to the central retinal subfield in the Early Treatment of Diabetic Retinopathy Study areas, automatically generated by the OCT software, was defined as CRT in this study. Decimal VA was measured using a Landolt ring chart, which is widely used in Japan, and converted to the logarithm of the minimum angle of resolution (logMAR).
For statistical analysis, the Wilcoxon signed-rank test was used for comparison of paired values and the Mann–Whitney U-test was used for comparison of the repeated measured values including intravitreal injection interval and CRT.
Results
A total of 15 eyes in 6 male and 9 female patients who consented to switch therapy from ranibizumab to aflibercept were included in this study; all patients were observed for more than 6 months after the switch (Table 1). Because none of the patients declined the switch, this study became an all-comer study without selection. The mean age of patients at baseline (before starting ranibizumab treatment) was 71.5 years (standard deviation [SD]: 12.6 years). The mean period of ranibizumab treatment was 11.8 months (SD: 4.2 months). The mean observation period after switching was 10.6 months (SD: 3.4 months), and four male and three female patients were observed for more than 12 months after the switch. VA during the ranibizumab treatment period was well controlled. There was no complete nonresponder to ranibizumab among the participants, although the patients with diabetes showed a tendency toward quick exacerbation of ME. Fluorescein angiography images were obtained from 14 patients, of whom 11 were perfusion type and 3 were nonperfusion type. Neovascularization was not observed.
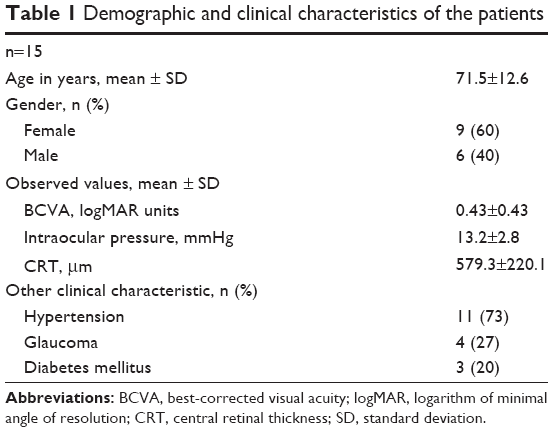 | Table 1 Demographic and clinical characteristics of the patients |
Comparison of injection intervals
The mean intravitreal injection interval increased from 68.2 days (SD: 26.4, median: 62, range: 28–168 days) during the ranibizumab treatment period to 91.8 days (SD: 33.2, median: 87, range: 49–168 days) after switching to aflibercept, indicating a statistically significant increase (P=0.0011, Mann–Whitney U-test; Figure 1). We also compared the intervals between the last and the second-to the-last intravitreal injection of ranibizumab and the first and the second intravitreal injection of aflibercept. The mean intravitreal injection interval just before switching was 81.3 days (SD: 35.6, median: 72, range: 45–168 days), and this significantly increased to 100.8 days (SD: 34.2, median: 90, range: 49–168 days) just after the switch to aflibercept (P=0.0309, Wilcoxon signed-rank test; Figure 2).
 | Figure 1 Intravitreal injection intervals before and after the switch from ranibizumab to aflibercept. |
 | Figure 2 Intravitreal injection intervals just before and after the switch from ranibizumab to aflibercept. |
Comparison of CRT
The mean CRT just before the start of ranibizumab therapy was 580 μm (SD: 211, median: 511, range: 358–1,239 μm), and this decreased significantly to 295 μm (SD: 55, median: 279, range: 228–590 μm) before therapy was switched (P<0.001). The mean CRT after the switch was 276 μm (SD: 25, median: 270, range 233–333 μm), and there was no significant difference from that before the switch (P=0.12, Mann–Whitney U-test; Figure 3).
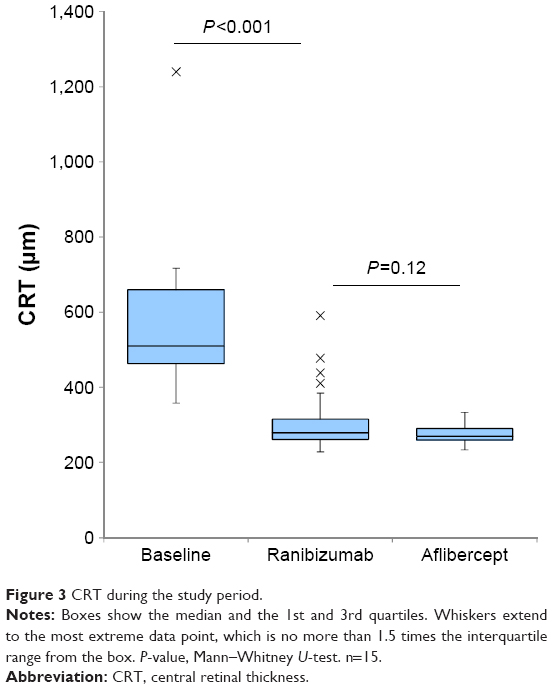 | Figure 3 CRT during the study period. |
Transition of BCVA
The mean BCVA just before the start of ranibizumab therapy was 0.43 logMAR (SD: 0.43). During treatment with aflibercept, no significant change in BCVA was observed (Figure 4).
 | Figure 4 BCVA after the switch to aflibercept. |
Safety
After switching to aflibercept, neither systemic nor ophthalmic complications were observed. Aflibercept therapy was well tolerated by all patients without discontinuation.
Discussion
In Japan, two anti-VEGF agents, ranibizumab and aflibercept, are approved for the management of ME secondary to RVO. Ranibizumab showed superior efficacy to improve vision and reduce CRT compared with sham injection in patients with ME secondary to BRVO in the BRAVO study and secondary to CRVO in the CRUISE study.12,13 In the second year, these studies continued in the HORIZON study, which suggested that the appropriate long-term management strategies of CRVO and BRVO should be different.14
The VIBRANT study showed superior efficacy of aflibercept injection compared with macular grid laser photocoagulation for the treatment of ME secondary to BRVO.15 Likewise, the COPERNICUS and GALILEO studies demonstrated that aflibercept produced significant improvements in VA and CRT compared with sham injection in patients with ME secondary to CRVO, although the disease state of CRVO is often more severe than that of BRVO.16,17
These clinical studies yielded excellent outcomes, but it is difficult to adopt the same regimen of six consecutive monthly doses in clinical settings. Therefore, there is a strong need to report and accumulate experience with the use of anti-VEGF agents in real-life therapy. It is also difficult to compare our study on switching agents with these earlier studies. A comparative test of these agents and observation after switching from one agent to another is necessary to provide the best treatment option for patients with ME secondary to BRVO.
In our hospital, all patients with ME secondary to BRVO who received ranibizumab intravitreal injections showed a certain degree of response to the agent. However, we switched the treatment of all these patients to aflibercept because we expected a prolonged injection interval under the same PRN regimen. Our results did show significant prolongation of the intravitreal injection interval following the switch: an increase from 68.2 days during the ranibizumab treatment period to 91.8 days during the aflibercept treatment period. Additionally, the results of this comparison show that the mean intravitreal injection interval just after the switch was significantly longer than that just before the switch; this eliminated the possibility that the prolonged interval might be caused by spontaneous remission of the disease and suggests that the prolongation is due to the effect of treatment with aflibercept, although the absence of a control group was one of the limitations of this study. Taken together, our results suggest that the benefit of aflibercept reported previously might also be obtainable in Japanese patients with ME secondary to BRVO.2–10 In the most relevant study, Wirth et al5 reported that a significant extension of the injection interval as well as decreased central retinal volume resulted from changing treatment to aflibercept by a proactive treat-and-extend regimen in patients with ME secondary to BRVO insufficiently responding to ranibizumab and/or bevacizumab. The principal difference between this report and our study is the patients’ response to previous treatments; the participants in our study all responded to ranibizumab. Our results also suggest the further benefit of aflibercept to ranibizumab responders, without giving a clear conclusion because our study was not controlled.
Dexamethasone intravitreal implant (DEX implant) is another treatment option for treating ME secondary to RVO.18 Especially, the combination of DEX implant and macular grid laser showed significant effect in increasing BCVA and prolonging the intravitreal injection interval in patients with ME secondary to BRVO compared with DEX implant monotherapy.19 This report is helpful, but DEX implant is not approved for treating ME in Japan.
The reasons for the prolonged intravitreal injection interval might be the greater affinity of aflibercept for the target molecule and its longer half-life compared with ranibizumab.20–22 Based on the intravitreal half-life and binding affinity, mathematical simulation has indicated that aflibercept retains binding activity for longer than ranibizumab in the vitreous body.23 Moreover, the longer duration of VEGF suppression of aflibercept than that of ranibizumab has also been confirmed in human age-related macular degeneration eyes and in macaque eyes.24,25 Given that aflibercept and ranibizumab showed similar half-lives in macaque eyes, the difference in the affinity of these agents for the target molecule could explain the difference in the duration of VEGF suppression. Specifically, the strong binding affinity of aflibercept could enhance its potency even after the concentration in the vitreous body is reduced. Additionally, because aflibercept suppresses not only VEGF-A but also placental growth factor, the difference in the target molecules of the agents might affect prolongation of the injection interval.20
Although prolongation of the intravitreal injection interval raises concerns about visual and anatomical exacerbation, our study showed a stable course of BCVA and no significant change in CRT after switching. These results suggest that, regarding ME secondary to BRVO, intravitreal administration of aflibercept under a PRN regimen should reduce the burden associated with intravitreal injection of patients and ophthalmologists without functional and anatomical degradation. However, it should be noted that patients need to visit hospital for monthly examination, and that PRN dosing enables reduction of the number of intravitreal injections but not the frequency of visits. Furthermore, when exacerbation is observed, reinjection should be performed on the same day as the examination if possible, to prevent further exacerbation of the clinical condition.
Conclusion
In this study, for the first time, we clinically investigated the switch of therapy from ranibizumab to aflibercept under a PRN regimen in Japanese patients with ME secondary to BRVO. Although this study is retrospective with a single-arm design and small sample size, the results suggest that switching therapy from ranibizumab to aflibercept might prolong the intravitreal injection interval without functional and anatomical exacerbation. Large-scale studies are warranted.
Limitations
Our study has limitations, including small sample size, the absence of a control group, and the single-center clinical trial design. A randomized comparison with a continuous ranibizumab administration group and a larger number of cases are needed to discuss the effect of switching accurately. Additionally, the period after switching is too short. A longer follow-up period might reveal other effects and yield information on switching of therapy.
Acknowledgment
Medical writing and editing were supported by Havas Worldwide Japan K.K., for which funding was received from Bayer Yakuhin, Ltd.
Disclosure
The authors report no conflicts of interest in this work and did not receive any honorarium for the preparation of this manuscript. Bayer Yakuhin, Ltd. was not involved in this study including data collection and analysis.
References
Yasuda M, Kiyohara Y, Arakawa S, et al. Prevalence and systemic risk factors for retinal vein occlusion in a general Japanese population: the Hisayama study. Invest Ophthalmol Vis Sci. 2010;51(6):3205–3209. | ||
Wang JK, Huang TL, Su PY, Chang PY, Tseng YY. Intravitreal aflibercept for macular edema secondary to branch retinal vein occlusion in Chinese patients. Eye Sci. 2015;30(2):63–66. | ||
Wang JK, Su PY, Hsu YR, Chen YJ, Chen FT, Tseng YY. Comparison of the efficacy of intravitreal aflibercept and bevacizumab for macular edema secondary to branch retinal vein occlusion. J Ophthalmol. 2016;2016:8421940. | ||
Saishin Y, Ito Y, Fujikawa M, Sawada T, Ohji M. Comparison between ranibizumab and aflibercept for macular edema associated with central retinal vein occlusion. Jpn J Ophthalmol. Epub 2016 Sep 22. | ||
Wirth MA, Becker MD, Graf N, Michels S. Aflibercept in branch retinal vein occlusion as second line therapy: clinical outcome 12 months after changing treatment from bevacizumab/ranibizumab – a pilot study. Int J Retin Vitr. 2016;2:20. | ||
Lehmann-Clarke L, Dirani A, Mantel I, Ambresin A. The effect of switching ranibizumab to aflibercept in refractory cases of macular edema secondary to ischemic central vein occlusion. Klin Monbl Augenheilkd. 2015;232(4):552–555. | ||
Eadie JA, Ip MS, Kulkarni AD. Response to aflibercept as secondary therapy in patients with persistent retinal edema due to central retinal vein occlusion initially treated with bevacizumab or ranibizumab. Retina. 2014;34(12):2439–2443. | ||
Cohen MN, Houston SK, Juhn A, et al. Effect of aflibercept on refractory macular edema associated with central retinal vein occlusion. Can J Ophthalmol. 2016;51(5):342–347. | ||
Pfau M, Fassnacht-Riederle H, Becker MD, Graf N, Michels S. Clinical outcome after switching therapy from ranibizumab and/or bevacizumab to aflibercept in central retinal vein occlusion. Ophthalmic Res. 2015;54(3):150–156. | ||
Papakostas TD, Lim L, van Zyl T, et al. Intravitreal aflibercept for macular oedema secondary to central retinal vein occlusion in patients with prior treatment with bevacizumab or ranibizumab. Eye (Lond). 2016;30(1):79–84. | ||
Tagami M, Kusuhara S, Imai H, Honda S, Tsukahara Y, Negi A. Impact of intravitreal injection of tissue plasminogen activator on full-field electroretinogram in patients with macular oedema secondary to retinal vein occlusion. Ophthalmologica. 2011;226(2):81–86. | ||
Campochiaro PA, Heier JS, Feiner L, et al. Ranibizumab for macular edema following branch retinal vein occlusion: six-month primary end point results of a phase III study. Ophthalmology. 2010;117(6):1102–1112. | ||
Brown DM, Campochiaro PA, Singh RP, et al. Ranibizumab for macular edema following central retinal vein occlusion: six-month primary end point results of a phase III study. Ophthalmology. 2010;117(6):1124–1133. | ||
Heier JS, Campochiaro PA, Yau L, et al. Ranibizumab for macular edema due to retinal vein occlusions: long-term follow-up in the HORIZON trial. Ophthalmology. 2012;119(4):802–809. | ||
Campochiaro PA, Clark WL, Boyer DS, et al. Intravitreal aflibercept for macular edema following branch retinal vein occlusion: the 24-week results of the VIBRANT study. Ophthalmology. 2015;122(3):538–544. | ||
Boyer D, Heier J, Brown DM, et al. Vascular endothelial growth factor Trap-Eye for macular edema secondary to central retinal vein occlusion: six-month results of the phase 3 COPERNICUS study. Ophthalmology. 2012;119(5):1024–1032. | ||
Holz FG, Roider J, Ogura Y, et al. VEGF Trap-Eye for macular oedema secondary to central retinal vein occlusion: 6-month results of the phase III GALILEO study. Br J Ophthalmol. 2013;97(3):278–284. | ||
Capone A Jr, Singer MA, Dodwell DG, et al. Efficacy and safety of two or more dexamethasone intravitreal implant injections for treatment of macular edema related to retinal vein occlusion (Shasta study). Retina. 2014;34(2):342–351. | ||
Pichi F, Specchia C, Vitale L, et al. Combination therapy with dexamethasone intravitreal implant and macular grid laser in patients with branch retinal vein occlusion. Am J Ophthalmol. 2014;157(3):607–615. | ||
Papadopoulos N, Martin J, Ruan Q, et al. Binding and neutralization of vascular endothelial growth factor (VEGF) and related ligands by VEGF trap, ranibizumab and bevacizumab. Angiogenesis. 2012;15(2):171–185. | ||
Park SJ, Choi Y, Na YM, et al. Intraocular pharmacokinetics of intravitreal aflibercept (Eylea) in a rabbit model. Invest Ophthalmol Vis Sci. 2016;57(6):2612–2617. | ||
Stewart MW. What are the half-lives of ranibizumab and aflibercept (VEGF Trap-eye) in human eyes? Calculations with a mathematical model. Eye Reports. 2011;1:e5. | ||
Stewart MW, Rosenfeld PJ. Predicted biological activity of intravitreal VEGF Trap. Br J Ophthalmol. 2008;92(5):667–668. | ||
Fauser S, Muether PS. Clinical correlation to differences in ranibizumab and aflibercept vascular endothelial growth factor suppression times. Br J Ophthalmol. Epub 2016 Feb 17. | ||
Niwa Y, Kakinoki M, Sawada T, Wang X, Ohji M. Ranibizumab and aflibercept: intraocular pharmacokinetics and their effects on aqueous VEGF level in vitrectomized and nonvitrectomized macaque eyes. Invest Ophthalmol Vis Sci. 2015;56(11):6501–6505. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.