Back to Journals » Patient Preference and Adherence » Volume 9
Profile of paliperidone palmitate once-monthly long-acting injectable in the management of schizophrenia: long-term safety, efficacy, and patient acceptability – a review
Authors González-Rodríguez A, Catalán R, Penadés R, Garcia-Rizo C, Bioque M, Parellada E, Bernardo M ![]()
Received 19 February 2015
Accepted for publication 8 April 2015
Published 27 May 2015 Volume 2015:9 Pages 695—706
DOI https://doi.org/10.2147/PPA.S63948
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Alexandre González-Rodríguez,1 Rosa Catalán,1–4 Rafael Penadés,1–4 Clemente Garcia-Rizo,1,3,4 Miquel Bioque,1,4 Eduard Parellada,1,3–5 Miquel Bernardo1–4
1Barcelona Clinic Schizophrenia Unit (BCSU), Neuroscience Institute, Hospital Clinic of Barcelona, 2Department of Psychiatry and Clinical Psychobiology, University of Barcelona, 3Institut d’Investigacions Biomèdiques August Pi I Sunyer (IDIBAPS), Barcelona, Spain; 4Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM), Madrid, Spain; 5Department of Pharmacology, University of Barcelona, Barcelona, Spain
Background and objectives: Short-term studies focused on once-monthly paliperidone palmitate (PP) at doses of 25 mg eq, 50 mg eq, 75 mg eq, 100 mg eq, or 150 mg eq have shown its efficacy and tolerability in the treatment of schizophrenia patients. However, few open-label and long-term studies are available regarding this new pharmacological formulation. Thus, our main aim was to review the scientific evidence on efficacy, safety, tolerability, and preference of PP in these populations.
Method: Electronic searches were conducted by using PubMed and ISI Web of Knowledge databases. All relevant studies published from 2009 until January 2015 were included without any language restriction if patients met diagnostic criteria for schizophrenia, and adequate information on efficacy, safety, and tolerability of once-monthly PP was available.
Results: Nineteen studies were identified irrespective of the study design and duration of the follow-up period. Randomized, double-blind, placebo-controlled trials found that schizophrenia patients receiving PP showed a significant improvement in psychotic symptoms and similar adverse events compared to placebo and suggested that all doses of PP were efficacious and well tolerated. Other studies demonstrated noninferiority of PP compared to risperidone long-acting injectable in recently diagnosed schizophrenia patients, chronically ill patients, as well as in acute and nonacute symptomatic schizophrenia patients, and a similar proportion of treatment-emergent adverse events between both groups were also noted.
Conclusion: Several studies have demonstrated that schizophrenia patients treated with PP show higher rates of improvement of psychotic symptoms compared to placebo, and similar efficacy and tolerability outcomes were noted when comparing PP to risperidone long-acting injectable or oral, paliperidone extended release.
Keywords: once-monthly paliperidone palmitate, long-acting antipsychotics, psychosis, schizophrenia, safety, efficacy, relapses
Introduction
Antipsychotics (understood as dopamine-receptor regulators, antagonists and partial agonists of dopamine and serotonin receptors) represent the cornerstone of the current pharmacological treatment of schizophrenia.1 Since the initial stages of antipsychotics (chlorpromazine was released in 1953), it was observed that treatment compliance was difficult to achieve and it was directly related with psychotic relapse and readmission. Although the first formulations were for oral administration, the specific characteristics of the disease allowed the development of the concept of long-acting injectables (LAIs) in order to ensure treatment adherence and management of these populations.2
Initial studies comparing long-acting injectable antipsychotics (LAIAs) with oral formulations showed that the relapse risk ratio in patients treated with long-term formulations was much lower.3 A systematic review underlined the inconclusive results but highlighted that mirror-image studies would be better designed and LAIAs might have improved long-term outcome in schizophrenia patients.4
Since the introduction of second-generation antipsychotics (SGAs), its oral formulations took over the research in schizophrenia, leaving behind first-generation antipsychotics (FGAs). Its initial promising effects in positive, negative, and cognitive symptoms did not end up with the previous difficulties in improving the final outcomes. Although there is still debate and controversy over efficacy differences between SGA and FGA, overall relapse risk ratio has been described to be lower with SGA compared to FGA, which would imply relevant and beneficial consequences in patient’s performance.5,6
Again, the introduction of long-acting risperidone came after the persistent need in treating patients with schizophrenia and psychotic symptoms, treatment adherence, and the still unresolved problem of treatment-resistance symptoms. Although patient’s difficulties to be compliant to treatments is frequent in general medical practice, its relevance in schizophrenia seems extreme as consequences range from psychotic relapse, hospitalization, disruptive behavior, reduced capacity to recovery, and worse outcome and prognosis.7 Nevertheless, social and familiar environment also play a role in the adherence, so a multidisciplinary approach is required to improve patient’s adherence and functioning.8
LAIA formulations have traditionally been used at latter stages of the disorder, for those patients with schizophrenia with most severe symptoms, poorest adherence, higher rates for relapses, and generally poorest outcomes.9,10 However, several authors support the notion that patients in early phases may gain from LAIAs, at a time when their disorder is most treatable, in order to avoid recurrences and rehospitalizations and decrease complications associated with noncompliance such as substance abuse, violence, legal conflicts, and treatment resistance.9–11
A group of authors have tried to clarify whether LAIAs are more effective to prevent relapses in schizophrenia patients in comparison to oral formulations. In a recent meta-analysis of randomized controlled trials, LAIAs did not show to be more effective in reducing relapses compared with oral antipsychotics in schizophrenia patients. But this finding was vulnerable to a cohort bias, as populations included were less representative of real-world patients than naturalistic studies.12 For instance, population in mirror-image studies better reflect clinical practice for patients receiving LAIAs than randomized controlled trials.13 Results from mirror-image studies in patients eligible for clinical use of LAIAs showed strong superiority of LAIs compared to oral antipsychotics in preventing hospitalizations.13
Paliperidone is a metabolite of risperidone that was previously introduced commercially in an oral formulation.14,15 Like risperidone, paliperidone blocks both 5HT2A and dopamine 2 receptors, alpha 1 and alpha 2 adrenoceptors, and histamine 1 receptors, but not beta adrenoceptors, muscarinic cholinoceptors, or peptidergic receptors.16
In pharmacokinetic trials sponsored by the manufacturer, the maximum paliperidone plasma concentrations were 28% higher when starting treatment in the deltoid muscle, rather than in the gluteal muscle.16 This difference may be related to the different distribution of muscle and adipose tissue between the two sites. Accordingly, the manufacturer recommends deltoid injections on the first (150 mg) and eighth days ±4 (100 mg) of treatment, to rapidly achieve appropriate plasma concentrations, followed by monthly administration into either the deltoid or gluteal muscles.16 The manufacturer does not recommend oral supplementation of paliperidone palmitate (PP).16 The manufacturer reports that oral paliperidone is roughly equivalent to PP on the following doses: 3 mg oral to 50 mg of palmitate, 6 mg to 75 mg, 9 mg to 100–150 mg. In its injectable formulation, PP is combined with inactive substances, so doses of PP can be expressed in terms of milligram equivalents (mg eq) of the active substance, PP, so that the 234 mg dose has 150 mg eq of PP, the 156-mg dose has 100 mg eq, the 117-mg dose has 75 mg eq, the 78-mg dose has 50 mg eq, and the 39-mg dose has 25 mg eq.16
In short-term studies, PP is an antipsychotic drug that was shown to be more efficacious than placebo.14,15 Related adverse events are similar to those of its related compounds, paliperidone and risperidone, with extrapyramidal movement disorders, weight gain, substantial increases in serum prolactin, and tachycardia all more common with PP than placebo.14,15
We therefore aimed to review the scientific evidence regarding the efficacy, safety, and tolerability of PP in the treatment of schizophrenia patients. As a particular mention, we provide a subsection focused on recently diagnosed schizophrenia patients, as this topic has been of interest in the last years for many clinical reasons.
Methods
We performed electronic searches by using PubMed and ISI Web of Knowledge database. All relevant studies published from 2009 until 2015 were included without any language restriction if patients fulfilled schizophrenia diagnostic criteria according to Diagnostic and Statistic Manual of Mental Disorders and International Classification of Diseases (ICD-10). The following key words were used: “once-monthly paliperidone palmitate and schizophrenia”, “paliperidone palmitate and safety”, “paliperidone palmitate and tolerability”, and “paliperidone palmitate and efficacy”. References of selected articles were carefully searched to identify potential further relevant articles. Psychopathological assessment as efficacy measures was considered when validated scales were used in the reported studies, and adverse events were taken into account when self-reported or measured by specific scales on safety and tolerability. Studies including data on pharmacoeconomics or cost-effectiveness of PP were excluded, as this was not the aim of the present review.
Results
Nineteen studies were identified regarding the efficacy, safety, and tolerability of PP on the treatment of schizophrenia patients. Studies were included irrespective of the study design and follow-up period, as we considered of special interest to summarize all the scientific evidence focused on the aforementioned new pharmacological LAI formulation.
A specific subsection on recent-onset schizophrenia patients has been implemented due to the increasing body of evidence in the pharmacological treatment of these patients.
From the 19 selected studies, we found several articles reporting outcomes by using different study designs, as follows: one randomized, cross-over trial;17 six randomized, double-blind, placebo-controlled trials;18–23 one open-label, noninferiority study comparing PP with risperidone long-acting injectable (RLAI);24 five randomized, double-blind, noninferiority clinical trials, four of them comparing PP with RLAI25–28 and one comparing PP with oral paliperidone extended release.29 Further, six open-label prospective studies were detected: one long-term, 1-year prospective study;30 one open-label, double-blind trial comparing PP in recently diagnosed patients versus chronically ill schizophrenia;31 one flexible-dose, interventional, single-arm study with 6-month follow-up;32 one open-label, 15-month, active-controlled trial;33 one open-label, 6-month, prospective study;34 and a 18-month, open-label, Phase IIIb study.35
Characteristics, study design, and main findings on efficacy, safety, and tolerability of the reviewed studies can be found in Tables 1 and 2.
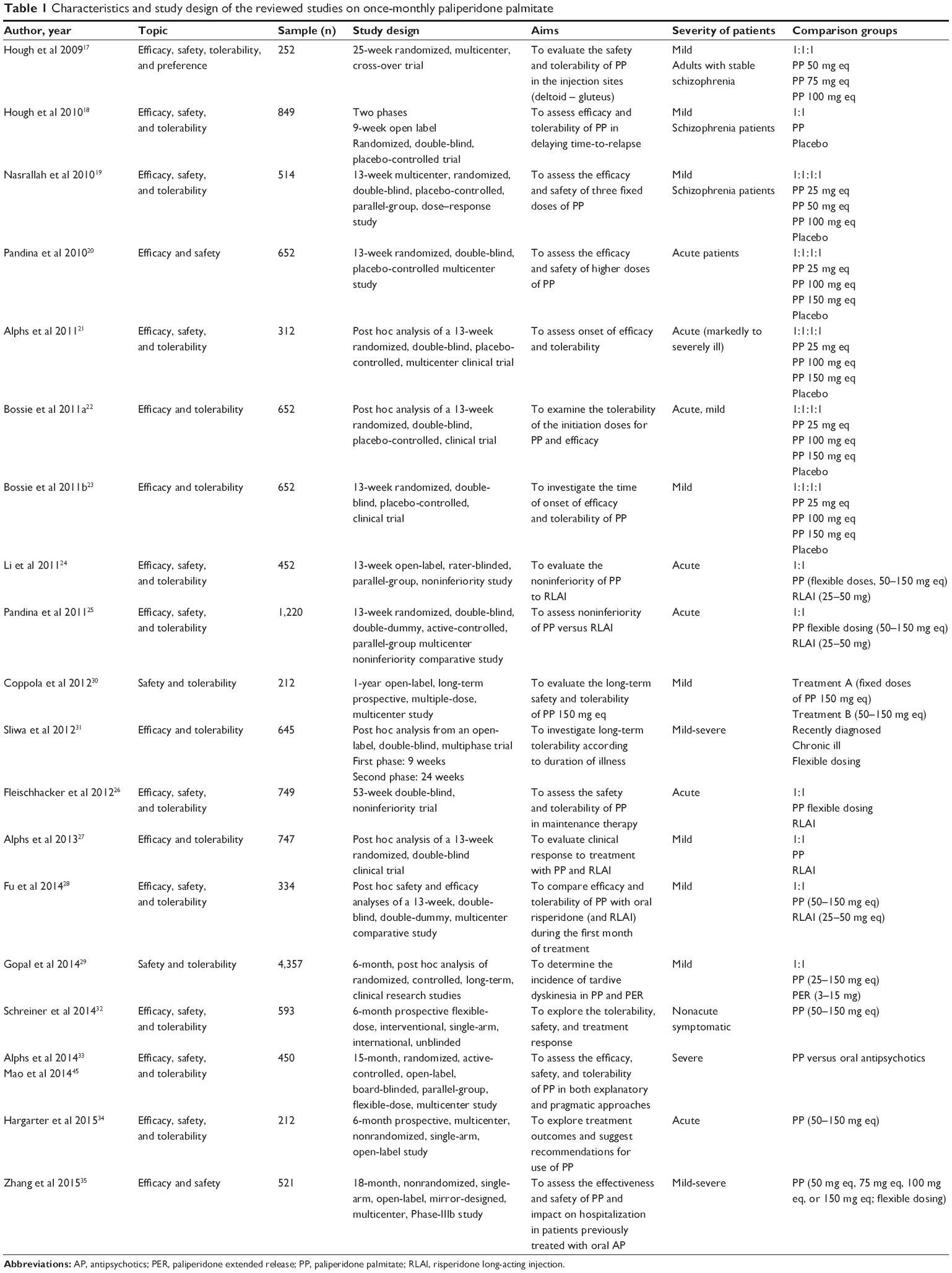 | Table 1 Characteristics and study design of the reviewed studies on once-monthly paliperidone palmitate |
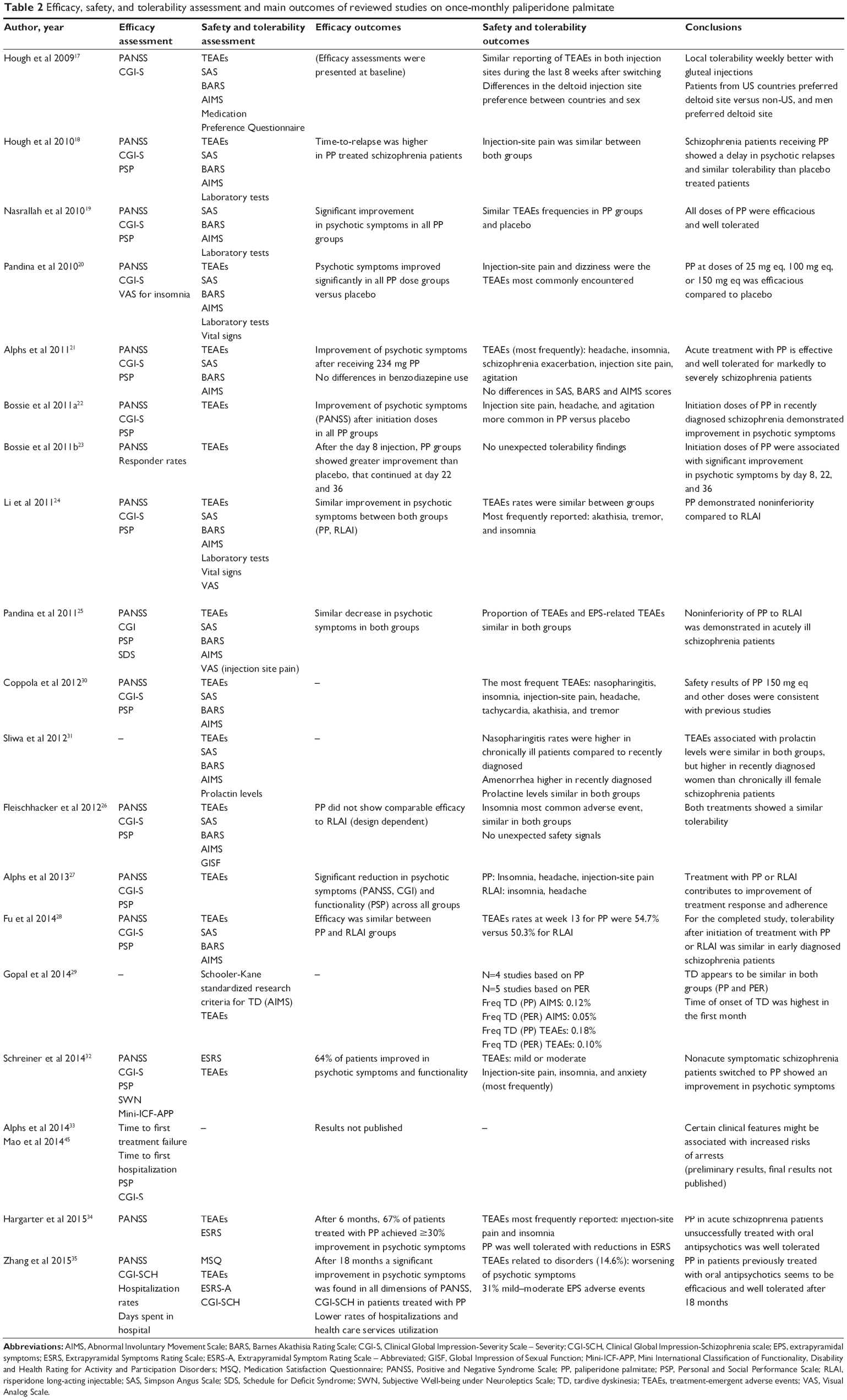 | Table 2 Efficacy, safety, and tolerability assessment and main outcomes of reviewed studies on once-monthly paliperidone palmitate |
Specific studies on recent-onset schizophrenia patients
Poor adherence to oral antipsychotics and high relapse and rehospitalization rates have been extensively found in first episode of psychosis or recent-onset schizophrenia patients. LAIAs may improve adherence to treatment and reduce the rate of relapse and rehospitalization in first-episode or recent-onset schizophrenia.36–44 For this reason, we have included a specific section regarding this issue.
Bossie and colleagues investigated the efficacy and tolerability of PP by comparing different PP doses with placebo in recently diagnosed schizophrenia patients (≤5 years).22 The authors found significant improvement in Positive and Negative Syndrome Scale (PANSS) total scores, but not an improvement in Clinical Global Impression-Severity Scale (CGI-S) and Personal and Social Performance Scale (PSP), in those patients receiving PP compared to those treated with placebo. In this subgroup of patients, PP initiation doses (150 mg eq on day 1, 100 mg eq on day 8) were well tolerated with no unexpected findings.
Long-term tolerability of PP was compared between recently diagnosed schizophrenia patients (≤5 years) and chronically ill patients as a post hoc analysis from an open-label multicenter trial.31 Regarding main findings, nasopharyngitis was more common in chronically ill patients compared to recently diagnosed schizophrenia patients, and amenorrhea in recently diagnosed patients. Further, the authors found that prolactin levels were higher in women recently diagnosed when compared to chronically ill female schizophrenia patients.
On the other hand, Fu et al compared the efficacy and tolerability of PP to RLAI in a sample formed by recently diagnosed schizophrenia patients; and over the entire sample, efficacy was found to be similar between both groups as measured by mean PANSS score changes, CGI-S and score changes in functionality, as measured by the PSP, and responder rates to treatment.28 Further, rates for adverse events were found to be similar between both LAI groups.
The most recent study evaluating the efficacy and safety of PP in recent-onset schizophrenia patients was carried out by Zhang and colleagues.35 This 18-month open-label Phase IIIb study found that patients unsuccessfully treated with oral antipsychotics and switch to PP showed a significant improvement in psychotic symptoms (measured by PANSS scale and CGI-S), and satisfaction with medications also improved after 18 months of follow-up. The authors concluded that PP treatment was efficacious and well tolerated, in particular in terms of number of psychiatric admissions and duration of hospitalizations.
Studies on chronic schizophrenia patients
Safety and tolerability of deltoid and gluteal injections of PP were investigated in stable schizophrenia patients by Hough et al by means of adverse event rates and scores of the main rating scales for extrapyramidal symptoms (Tables 1 and 2).17 The authors highlighted that at initiation doses of PP, both injection sites had a similar reporting of adverse events, as well as during the last 8 weeks after switching from site. However, several findings should be taken into consideration. Differences in the injection site differ between US and non-US countries and men preferred deltoid site in contrast with women who reported the preference of gluteus site. Further, local tolerability was better with gluteal injections than deltoid sites.
The efficacy and tolerability of three fixed doses of PP versus placebo were investigated by Nasrallah et al.19 The authors found that patients treated with all PP groups showed a significant improvement in psychotic symptoms, but no differences in functionality were detected compared to placebo. Regarding safety and tolerability, it should be taken into consideration that prolactin levels were higher in PP groups than placebo, and this increase was dose-dependent.
On the other hand, Hough et al confirmed the efficacy of PP in delaying time-to-relapse in adult schizophrenia patients.18 The authors also found that injection-site pain was similar in those treated with PP, as well as those receiving placebo.
In the same line of the study aforementioned, Pandina et al confirmed the efficacy and tolerability of lower doses of PP (25 mg eq, 100 mg eq) and observed positive results at higher doses of PP (150 mg eq) in acutely exacerbated schizophrenia patients.20
The same authors evaluated the noninferiority of PP flexible dosing versus RLAI.25 After 13 weeks of treatment, changes in psychotic symptoms showed a similar decrease in both groups, and similar frequency of adverse events.
Alphs et al carried out a randomized placebo-controlled trial in acutely schizophrenic patients by comparing efficacy and tolerability of PP dosing to placebo.21 The study included markedly to severely ill schizophrenia patients defined as 5 or more scores of the CGI-S at baseline, and the authors concluded that acute treatment with PP was an effective and well-tolerated treatment in this kind of clinical populations when compared to placebo.
In this line, Bossie and colleagues investigated the onset of efficacy and tolerability of PP by comparing different doses with placebo in schizophrenia patients.22,23 The authors found that PP was associated with higher psychopathological improvement by days 8, 22, and 36 when compared to placebo and found no unexpected tolerability findings.
An open-label, parallel-group noninferiority study evaluating the efficacy and safety of PP versus RLAI was conducted by Li and colleagues.24 The authors found both treatment groups to be similar in terms of adverse events and improvement in psychotic symptoms, as measured by the CGI-S and the PANSS Scale, suggesting that PP demonstrated noninferiority compared to RLAI.
The first long-term, open-label, prospective study in schizophrenia patients treated with PP was conducted by Coppola and collaborators, who aimed to assess the long-term safety of PP at 150 mg eq.30 In this study, all patients did not receive injectable antipsychotic formulations previously, and the authors concluded that safety results of this PP dosing were consistent with previous results recently published.
In a similar study design, long-term tolerability of PP was investigated in an open-label, double-blind, multicenter trial in recently diagnosed schizophrenia.31 Main findings of this study are mentioned in Specific Studies on recent Schizophrenia patients subsection.
The noninferiority of PP to RLAI was assessed in a sample of acutely symptomatic schizophrenia patients in a 53-week, double-blind study.26 The authors concluded that insomnia was the adverse event most commonly encountered, and tolerability of PP and RLAI was found to be similar in both groups. However, probably due to the initial dosing strategy, PP did not show less efficacy when compared to RLAI. In agreement with the previous study, a recent one reporting response to treatment with two, long-acting, injectable atypical antipsychotics (PP, RLAI) also indicated that individuals diagnosed with schizophrenia previously treated with oral antipsychotics showed a significant reduction of psychotic symptoms.27
When focusing on safety and tolerability profile of PP, it should be highlighted that Gopal et al focused their investigations in schizophrenia patients receiving PP or oral paliperidone extended release by comparing rates of tardive dyskinesia measured by two well-established methods: the Schooler–Kane standardized research criteria, based on the Abnormal Involuntary Movement Scale, and the spontaneous reporting of this particular adverse event.29 Frequency and incidence of tardive dyskinesia were similar in both treatment groups being low the observed risk (<0.2%) in the entire sample. In this study, dyskinesia rate was higher within the first month of treatment and clearly decreased over time.
A prospective, flexible-dose, interventional, 6-month study was carried out by Schreiner and colleagues in nonacute but symptomatic adult schizophrenia patients who were unsuccessfully treated with oral antipsychotics.32 This pragmatic study found that more than two-thirds of the nonacute patients switched to PP showed an improvement in psychotic symptoms and functionality after 6 months of treatment. Furthermore, satisfaction with medication and sleep quality, as measured by the Treatment Satisfaction Questionnaire for Medication Scale, showed a relevant and significant improvement in patients receiving PP.
Recently, Alphs et al published the study design and rationale of the Paliperidone Palmitate Research in Demonstrating Effectiveness study, a 15-month, open-label, and prospective study carried out between 2010 and 2013.33 The study aimed to compare PP and oral antipsychotics in schizophrenia patients in a pragmatic and explanatory approach. Preliminary results in a sample of schizophrenia patients with history of arrests or incarceration were presented at the 167th Annual Meeting of the American Psychiatric Association.45
Hargarter et al carried out an open-label, prospective study with a 6-month follow-up in acutely schizophrenia patients and suggested several recommendations for the use of PP.34 The authors found that the vast majority of the sample receiving PP showed improvement in psychotic symptoms, and PP was well tolerated, with the treatment-emergent adverse event most commonly found being injection-site pain.
Discussion
LAIAs have demonstrated to be useful regarding patients’ tolerability and adherence either in FGA or SGA formulations.46 Although symptom recognition or treatment resistance still underlie the difficulties expressed by many patients, the evaluation of LAIAs in clinical practice and the possibility of discussing the formulation with patients and family reflects a new paradigm in treatment management.8
The current state of knowledge favors the introduction of LAIAs at different stages of the illness reflecting a change of paradigm toward new treatment options not only from the patient’s personal view but also and most important from the mental health care providers themselves.47
LAIA formulations have traditionally been used at latter stages, but some authors defend that early-phase patients may have the most to gain from them.9,39–42 Some clinical guidelines, like the Canadian one, are beginning to include the recommendation to use LAIAs in patients in early stages of the disorder.44,48 This proportion could also be increased with the recent appearance of new second-generation LAIAs, such as olanzapine pamoate, PP, and aripiprazole depot.49
Results from naturalistic studies, such as mirror-image studies, showed strong superiority of LAIs compared to oral antipsychotics in preventing hospitalizations.13
Thus, our main goal was to review the available scientific literature focused on the efficacy, safety, and tolerability of once-monthly PP in schizophrenia patients.
We identified 19 studies reporting data on efficacy, safety, tolerability, or preference of PP in the treatment of schizophrenia patients. From those selected, several study designs can be identified.
In a first step, it should be noted that gluteal injections have demonstrated better local tolerability than deltoid administrations in a randomized cross-over trial.17 However, this is the unique study specifically investigating tolerability in both types of administration, so results should not be generalizable.
Regarding the efficacy and safety of different doses of PP, six randomized, double-blind, placebo-controlled trials found that schizophrenia patients receiving PP showed a significant improvement in psychotic symptoms and similar adverse events compared to placebo,18–23 suggesting that all doses of PP were efficacious and well tolerated. Further, time-to-relapse was higher in those patients treated with PP.18
In spite of the evidence previously mentioned, several noninferiority studies have compared PP with other LAI formulations or oral paliperidone.24–29 These studies demonstrated noninferiority of PP compared to RLAI in early diagnosed schizophrenia patients and chronic schizophrenia patients independent of severity of illness. Further, a similar proportion of treatment-emergent adverse events was noted between both the groups. On the other hand, nonacute symptomatic schizophrenia patients, PP has also demonstrated its efficacy in terms of psychotic improvement, and lower rates of mild to moderate adverse events compared to RLAI.
The most recent studies investigating this field were conducted by Hargarter et al and Zhang et al34,35 who found that PP in acute schizophrenia was well tolerated and associated with improvement in psychotic symptoms. On the other hand, it should be mentioned that Sliwa et al found higher prolactin levels in those women suffering from an acute recent-onset schizophrenia in comparison with chronically ill female schizophrenia patients.31
Conclusion
Short-term studies based on PP at doses of 25 mg eq, 50 mg eq, 75 mg eq, 100 mg eq, or 150 mg eq have shown its efficacy and tolerability in the treatment of schizophrenia.
Several studies have demonstrated that schizophrenia patients treated with PP show higher rates of improvement of psychotic symptoms compared to placebo and similar efficacy and tolerability outcomes when comparing PP to RLAI or oral paliperidone extended release.
However, in the present review, several limitations should be taken into consideration. To date, no studies have compared the efficacy and tolerability of PP with other LAI formulations, except for RLAI. It would be of interest, and further research is needed, to compare PP with typical antipsychotics and other formulations to date not studied.
Acknowledgments
This study was supported by the Ministerio de Economía y Competitividad. Instituto de Salud Carlos III- Fondo Europeo de Desarrollo Regional, Unión Europea, Un manera de hacer Europa, Centro de Investigación Biomédica en Red de salud Mental, CIBERSAM, by the Government of Catalonia, and Secretaria d’Universitats i Recerca del Departament d’Economia i Coneixement (2014SGR441). This work was developed (in part) at the Centro Esther Koplowitz (Barcelona).
Disclosure
Miquel Bernardo has been a consultant for, received grant/research support and honoraria from, and been on the speakers/advisory board of ABBiotics, Adamed, AMGEN, Eli Lilly, Ferrer, Forum Pharmaceuticals, Gedeon, Hersill, Janssen-Cilag, Lundbeck, Otsuka, Pfizer, Roche, and Servier. Alexandre González-Rodríguez has received honoraria or been paid for travels from Pfizer, Janssen, and Ferrer. Rosa Catalán has received honoraria or has been paid for travels from Lilly, Lundbeck, Janssen, Ferrer, Pfizer, and Bristol. Rafael Penadés has received honoraria or been paid for travels from Otsuka-Lundbeck. Clemente Garcia-Rizo has been a consultant for, received grant/research support, awards, honoraria from, and been on the speakers/advisory board of Bristol-Myers Squibb, Eli-Lilly, Ferrer, Janssen-Cilag, and Pfizer. Miquel Bioque has been a consultant for, received grant/research support, awards, honoraria from, and been on the speakers/advisory board of Ferrer, Janssen-Cilag, Lundbeck, Otsuka, and Pfizer. Eduard Parellada has received honoraria and/or research grants from Janssen-Cilag, GlaxoSmith Kline, and Ferrer. The authors report no other conflicts of interest in this work.
References
Miyamoto S, Duncan GE, Marx CE, Lieberman JA. Treatments for schizophrenia: a critical review of pharmacology and mechanisms of action of antipsychotic drugs. Mol Psychiatry. 2005;10(1):79–104. | ||
Simpson GM. A brief history of depot neuroleptics. J Clin Psychiatry. 1984;45(5 pt 2):3–4. | ||
Hogarty GE, Schooler NR, Ulrich R, Mussare F, Ferro P, Herron E. Fluphenazine and social therapy in the aftercare of schizophrenic patients. Relapse analyses of a two-year controlled study of fluphenazine decanoate and fluphenazine hydrochloride. Arch Gen Psychiatry. 1979; 36(12):1283–1294. | ||
Haddad PM, Taylor M, Niaz OS. First-generation antipsychotic long-acting injections v oral antipsychotics in schizophrenia: systematic review of randomised controlled trials and observational studies. Br J Psychiatry Suppl. 2009;52:S20–S28. | ||
Leucht S, Corves C, Arbter D, Engel RR, Li C, Davis JM. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet. 2009;373(9657):31–41. | ||
Kishimoto T, Agarwal V, Kishi T, Leucht S, Kane JM, Correll CU. Relapse prevention in schizophrenia: a systematic review and meta-analysis of second-generation antipsychotics versus first-generation antipsychotics. Mol Psychiatry. 2013;18(1):53–66. | ||
Llorca PM. Partial compliance in schizophrenia and the impact on patient outcomes. Psychiatry Res. 2008;161(2):235–247. | ||
Shuler KM. Approaches to improve adherence to pharmacotherapy in patients with schizophrenia. Patient Prefer Adherence. 2014;8:701–714. | ||
Tiihonen J, Haukka J, Taylor M, Haddad PM, Patel MX, Korhonen P. A nationwide cohort study of oral and depot antipsychotics after first hospitalization for schizophrenia. Am J Psychiatry. 2011;168(6): 603–609. | ||
Stahl SM. Long-acting injectable antipsychotics: shall the last be first? CNS Spectr. 2014;19(01):3–5. | ||
Zhornitsky S, Stip E. Oral versus long-acting injectable antipsychotics in the treatment of schizophrenia and special populations at risk for treatment nonadherence: a systematic review. Schizophr Res Treatment. 2012;2012:407171. | ||
Kishimoto T, Robenzadeh A, Leucht C, et al. Long-acting injectable vs oral antipsychotics for relapse prevention in schizophrenia: a meta-analysis of randomized trials. Schizophr Bull. 2014;40(1): 192–213. | ||
Kishimoto T, Nitta M, Borenstein M, Kane JM, Correll CU. Long-acting injectable versus oral antipsychotics in schizophrenia: a systematic review and meta-analysis of mirror-image studies. J Clin Psychiatry. 2013;74(10):957–965. | ||
Nussbaum AM, Stroup TS. Paliperidone palmitate for schizophrenia. Schizophr Bull. 2012;38(6):1124–1127. | ||
Nussbaum M, Stroup TS. Paliperidone palmitate for schizophrenia. Cochrane Database Syst Rev. 2012;6:CD008296. doi:10.1002/ 14651858.CD008296.pub2. | ||
Janssen. Invega Sustenna (Paliperidone Palmitate) Extended-Release Injectable Suspension Prescribing Information. Titusville, NJ: Orth-McNeil-Janssen Pharmaceuticals, Inc; 2009. | ||
Hough D, Lindenmayer JP, Gopal S, et al. Safety and tolerability of deltoid and gluteal injections of paliperidone palmitate in schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2009;33(6):1022–1031. | ||
Hough D, Gopal S, Vijapurkar U, Lim P, Morozova M, Eerdekens M. Paliperidone palmitate maintenance treatment in delaying the time-to-relapse in patients with schizophrenia: a randomized, double-blind, placebo-controlled study. Schizophr Res. 2010;116(2–3):107–117. | ||
Nasrallah HA, Gopal S, Gassmann-Mayer C, et al. A controlled, evidence-based trial of paliperidone palmitate, a long-acting injectable antipsychotic, in schizophrenia. Neuropsychopharmacology. 2010; 35(10):2072–2082. | ||
Pandina GJ, Lindenmayer JP, Lull J, et al. A randomized, placebo-controlled study to assess the efficacy and safety of 3 doses of paliperidone palmitate in adults with acutely exacerbated schizophrenia. J Clin Psychopharmacol. 2010;30(3):235–244. | ||
Alphs L, Bossie CA, Sliwa JK, Ma YW, Turner N. Onset of efficacy with acute long-acting injectable paliperidone palmitate treatment in markedly to severely ill patients with schizophrenia: post hoc analysis of a randomized, double-blind clinical trial. Ann Gen Psychiatry. 2011;10(1):12. | ||
Bossie CA, Fu DJ, Sliwa JK, Ma YW, Alphs L. Tolerability of initiation doses of once-monthly paliperidone palmitate in patients with recently diagnosed schizophrenia in an acute treatment trial. Ther Adv Psychopharmacol. 2011;1(4):111–124. | ||
Bossie CA, Sliwa JK, Ma YW, Fu DJ, Alphs L. Onset of efficacy and tolerability following the initiation dosing of long-acting paliperidone palmitate: post-hoc analyses of a randomized, double-blind clinical trial. BMC Psychiatry. 2011;10(11):79. | ||
Li H, Rui Q, Ning X, Xu H, Gu N. A comparative study of paliperidone palmitate and risperidone long-acting injectable therapy in schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2011; 35(4):1002–1008. | ||
Pandina G, Lane R, Gopal S, et al. A double-blind study of paliperidone palmitate and risperidone long-acting injectable in adults with schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2011; 35(1):218–226. | ||
Fleischhacker WW, Gopal S, Lane R, et al. A randomized trial of paliperidone palmitate and risperidone long-acting injectable in schizophrenia. Int J Neuropsychopharmacol. 2012;15(1):107–118. | ||
Alphs L, Bossie CA, Sliwa JK, Fu DJ, Ma YW, Hulihan J. Paliperidone palmitate and risperidone long-acting injectable in subjects with schizophrenia recently treated with oral risperidone or other oral antipsychotics. Neuropsychiatr Dis Treat. 2013;9:341–350. | ||
Fu DJ, Bossie CA, Kern Sliwa J, Ma YW, Alphs L. Paliperidone palmitate versus risperidone long-acting injection in markedly-to-severely ill schizophrenia subjects: onset of efficacy with recommended initiation regimens. Clin Schizophr Relat Psychoses. 2014;8(2):101–109. | ||
Gopal S, Xu H, Bossie C, et al. Incidence of tardive dyskinesia: a comparison of long-acting injectable and oral paliperidone clinical trial databases. Int J Clin Pract. 2014;68(12):1514–1522. | ||
Coppola D, Liu Y, Gopal S, et al. A one-year prospective study of the safety, tolerability and pharmacokinetics of the highest available dose of paliperidone palmitate in patients with schizophrenia. BMC Psychiatry. 2012;28:12–26. | ||
Sliwa JK, Bossie CA, Fu DJ, Turkoz I, Alphs L. Long-term tolerability of once-monthly injectable paliperidone palmitate in subjects with recently diagnosed schizophrenia. Neuropsychiatr Dis Treat. 2012;8: 375–385. | ||
Schreiner A, Bergmans P, Cherubin P, et al. A prospective flexible-dose study of paliperidone palmitate in nonacute but symptomatic patients with schizophrenia previously unsuccessfully treated with oral antipsychotic agents. Clin Ther. 2014;36(10):1372–1388. | ||
Alphs L, Mao L, Rodriguez SC, Hulihan J, Starr HL. Design and rationale of the paliperidone palmitate research in demonstrating effectiveness (PRIDE) study: a novel comparative trial of once-monthly paliperidone palmitate versus daily oral antipsychotic treatment for delaying time to treatment failure in persons with schizophrenia. J Clin Psychiatry. 2014;75(12):1388–1393. | ||
Hargarter L, Cherubin P, Bergmans P, et al. Intramuscular long-acting paliperidone palmitate in acute patients with schizophrenia unsuccessfully treated with oral antipsychotics. Prog Neuropsychopharmacol Biol Psychiatry. 2014;58C:1–7. | ||
Zhang F, Si T, Chiou CF, et al. Efficacy, safety, and impact on hospitalizations of paliperidone palmitate in recent-onset schizophrenia. Neuropsychiatr Dis Treat. 2015;11:657–668. | ||
Kane JM, Garcia-Ribera C. Clinical guideline recommendations for antipsychotic long-acting injections. Br J Psychiatry Suppl. 2009;52:63–67. | ||
Heres S, Reichhart T, Hamann J, Mendel R, Leucht S, Kissling W. Psychiatrists’ attitude to antipsychotic depot treatment in patients with first-episode schizophrenia. Eur Psychiatry. 2011;33:297–301. | ||
Kirschner M, Theodoridou A, Fusar-Poli P, Kaiser S, Jäger M. Patients’ and clinicians’ attitude towards long-acting depot antipsychotics in subjects with a first episode of psychosis. Ther Adv Psychopharmacol. 2013;3(2):89–99. | ||
Parellada E, Velligan DI, Emsley R, Kissling W. Long-acting injectable antipsychotics in first-episode schizophrenia. Schizophr Res Treatment. 2012;2012:318535. | ||
Taylor M, Ng KY. Should long-acting (depot) antipsychotics be used in early schizophrenia? A systematic review. Aust N Z J Psychiatry. 2013;47(7):624–630. | ||
Emsley R, Chiliza B, Asmal L, Mashile M, Fusar-Poli P. Long-acting injectable antipsychotics in early psychosis: a literature review. Early Interv Psychiatry. 2013;7(3):247–254. | ||
Heres S, Lambert M, Vauth R. Treatment of early episode in patients with schizophrenia: the role of long acting antipsychotics. Eur Psychiatry. 2014;29(suppl 2):1409–1413. | ||
Kim B, Lee SH, Yang YK, Park JI, Chung YC. Long-acting injectable antipsychotics for first-episode schizophrenia: the pros and cons. Schizophr Res Treatment. 2012;2012:560836. | ||
Malla A, Tibbo P, Chue P, et al. Long-acting injectable antipsychotics: recommendations for clinicians. Can J Psychiatry. 2013;58(5 suppl 1): 30S–35S. | ||
Mao L, Alphs L, Benson C, Fastenau J, Lynn Starr H. Correlates of repeat arrests/incarcerations in adult subjects diagnosed with schizophrenia with history of criminal justice system (CJS) involvement. Poster presented at: APA 167th Meeting; May 3–7, 2014; New York, USA. | ||
Cañas F, Möller HJ. Long-acting atypical injectable antipsychotics in the treatment of schizophrenia: safety and tolerability review. Expert Opin Drug Saf. 2010;9(5):683–697. | ||
Geerts P, Martinez G, Schreiner A. Attitudes towards the administration of long-acting antipsychotics: a survey of physicians and nurses. BMC Psychiatry. 2013;13:58. | ||
Manchanda R, Chue P, Malla A, et al. Long-acting injectable antipsychotics: evidence of effectiveness and use. Can J Psychiatry. 2013;58(5 suppl 1):5S–13S. | ||
Patel M, Haddad P, Chaudhry I, McLoughlin S, David A. Psychiatrists’ use, knowledge and attitudes to first- and second-generation antipsychotic long-acting injections: comparisons over 5 years. J Psychopharmacol. 2010;24(10):1473–1482. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.