Back to Journals » Substance Abuse and Rehabilitation » Volume 6
Prevalence of and factors associated with regular khat chewing among university students in Ethiopia
Authors Astatkie A ![]() , Demissie M
, Demissie M ![]() , Berhane Y
, Berhane Y ![]() , Worku A
, Worku A
Received 5 December 2014
Accepted for publication 20 January 2015
Published 26 February 2015 Volume 2015:6 Pages 41—50
DOI https://doi.org/10.2147/SAR.S78773
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Li-Tzy Wu
Ayalew Astatkie,1 Meaza Demissie,2 Yemane Berhane,2 Alemayehu Worku2,3
1School of Public and Environmental Health, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia; 2Addis Continental Institute of Public Health, Addis Ababa, Ethiopia; 3School of Public Health, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Purpose: Khat (Catha edulis) is commonly chewed for its psychostimulant and euphorigenic effects in Africa and the Arabian Peninsula. Students use it to help them study for long hours especially during the period of examination. However, how regularly khat is chewed among university students and its associated factors are not well documented. In this article we report on the prevalence of and factors associated with regular khat chewing among university students in Ethiopia.
Methods: We did a cross-sectional study from May 20, 2014 to June 23, 2014 on a sample of 1,255 regular students recruited from all campuses of Hawassa University, southern Ethiopia. The data were collected using self-administered questionnaires. We analyzed the data to identify factors associated with current regular khat chewing using complex sample adjusted logistic regression analysis.
Results: The prevalence of current regular khat chewing was 10.5% (95% confidence interval [CI]: 6.1%–14.9%). After controlling for sex, religion, year of study, having a father who chews khat, cigarette smoking and alcohol drinking in the adjusted logistic regression model, living off-campus in rented houses as compared to living in the university dormitory (adjusted odds ratio [95% CI] =8.09 [1.56–42.01]), and having friends who chew khat (adjusted odds ratio [95% CI] =4.62 [1.98–10.74]) were found to significantly increase the odds of current regular khat use.
Conclusion: Students living outside the university campus in rented houses compared to those living in dormitory and those with khat chewing peers are more likely to use khat. A multipronged prevention approach involving students, the university officials, the surrounding community, and regulatory bodies is required.
Keywords: current regular khat chewing, peer pressure, living arrangement, university students
Introduction
Chewing the fresh leaves and shoots of the ever green plant khat (Catha edulis) (Figure 1) dates back several centuries in eastern and southern Africa and the Arabian Peninsula. While khat is considered the main drug of abuse besides alcohol in Ethiopia and other countries of the region,1 planting and consumption of khat in parts of Asia (other than the Arabian Peninsula) such as Israel, Afghanistan, Sri Lanka, and India is also documented.1–4 People migrating from the traditional khat growing and chewing areas have also introduced the habit to neighboring countries and other parts of the world.1 With the ubiquity of road network and air transport in this era, khat could easily be delivered to any part of the world.5 As such, it is estimated that nowadays about ten million people worldwide chew khat daily1 to enjoy its psychostimulant and euphorigenic effects.5–7
 | Figure 1 Leaves and shoots of fresh khat. |
Associations between khat chewing and a number of physical and psychological health problems have been documented1 making it an important concern in public health and clinical medicine. To mention some, elevated blood pressure,8,9 acute myocardial infarction, hemorrhoids, constipation, duodenal ulcers, and inhibition of spermatogenesis have been reported to be associated with khat chewing.10,11 In a large prospective multicenter study of patients with acute coronary syndrome, khat chewing was associated with higher risk of in-hospital mortality and stroke.12 Higher frequency of anemia13 and low-birth-weight babies14 have been documented among pregnant women who chew khat. Khat chewing is also associated with different adverse oral health outcomes.15 Neurocognitive impairments,1 euphoria, excitability, anxiety, and insomnia,10,11 are some of the documented central nervous system effects of khat chewing. Khat chewing can also induce psychological dependency.1,16,17 Recently, criteria of the substance dependency syndrome were shown to be present among khat chewers indicating that khat chewing could also induce physical dependency.18 Khat chewing is also shown to be associated with occurrence of psychotic symptoms.19,20
In the past, several studies attempted to determine the prevalence of and factors associated with khat chewing among university/college students both in Ethiopia and elsewhere. In Ethiopia, studies conducted among students in different universities/colleges have reported lifetime prevalence values ranging from 13.4% to 41%.21–27 Similarly, 12 months prevalence values ranging from 7% to 20.3% have been reported.22,28 Past 30 days prevalence has been reported in the range of 6.3%–33.1%.21,23–26,29–31
The most frequently reported reasons for using khat by university/college students are to stay awake and be able to concentrate while reading,22,24–26 and to relieve stress.25,26,30 Other reasons include the need for enjoyment22,26 and relaxation,24,30 peer pressure,24,26 and the need to socialize.30 Most of these reasons are related to the desire for the psychostimulation and euphoria that result from khat chewing.
Several factors were shown to be associated with khat chewing among university/college students. These included male sex, being Muslim by religion, alcohol drinking, cigarette smoking, having a family history of khat chewing, and having friends who chew khat, all of which increase the odds of khat chewing.22,25,32,33
However, most studies disregard the regularity with which khat chewing is practiced which is important to assess the intensity of exposure to khat. Besides, though all the studies employed a complex sample survey design, all ignored the survey design during the analysis which could bias the studies’ findings.34,35 Previous studies also did not consider students’ living arrangement as a possible factor associated with khat chewing except two studies, one36 of which attempted to assess the association of residing off-campus with harmful khat use among khat chewers and the other27 the association of off-campus housing with khat chewing practice. Yet, evidence from the Western world indicates that living arrangement (dormitory versus [vs] other living arrangement) is an important determinant of substance use.37
Therefore, we conducted a cross-sectional study to determine the prevalence of and factors associated with current regular khat chewing among students of Hawassa University, southern Ethiopia. We defined current regular khat chewing as khat chewing at least once weekly in the past one year or more by adopting the definition used in the existing literature.38,39 We also addressed the methodological limitations of previous studies by doing a complex survey analysis and assessing living arrangement as a possible factor.
Methods
Study setting and subjects
This study was carried out in Hawassa University, which is located in Hawassa city, in the Southern Nations, Nationalities and Peoples Region of Ethiopia. The university is divided into five campuses. It has seven colleges and one institute which embody 21 schools and 15 departments. There are 59 undergraduate and 57 postgraduate training programs in the university. The university has a total student population (undergraduate and graduate) of more than 31,000 in the regular and continuing education programs. The undergraduate regular student population comprises 13,546 males and 3,951 females, in total 17,497 students.40,41
The study utilized a cross-sectional study design. It was conducted during the period from May 20, 2014 to June 23, 2014. We included only regular undergraduate students of the university in this study. Inclusion into the study was restricted only to students who were in the second year and above in order to create a buffer period for the transition from being a high school student to a university student.
Sample size and sampling
Sample size was estimated under varying assumptions using OpenEpi version 2.3.42 Then the sample sizes obtained under different assumptions were adjusted for anticipated nonresponse rate. The largest of all the sample sizes (n=1,290) which was calculated with the following single population proportion assumptions was used: 95% confidence level, 17,497 reference population size,41 27.9% expected prevalence of khat chewing in the past 30 days25 (as a proxy to current regular khat chewing) , 3% margin of error, a design effect of 1.5 for complex sampling, and a 5% anticipated nonresponse rate.
This study utilized a two-stage stratified cluster sampling scheme. In the first stage, from each college/institute of the university two undergraduate programs (primary sampling units) were selected by simple random sampling. In the second stage, one section (secondary sampling unit) was randomly selected (if number of sections was more than one) from each year of study in each selected program. All students in the selected sections were included in the study, which is a preferred method in most school surveys.43
Data collection instruments and procedures
Our data collection tool was a structured self-administered questionnaire. The questionnaire was initially prepared in English and then translated into Amharic. The questionnaire was also back-translated to English by an independent translator (language expert) to check the conceptual consistency of items. Some questions for the questionnaire were adapted from the Ethiopian Demographic and Health Survey 2011 questionnaire44 and from the World Health Organization (WHO) questionnaire for student drug-use surveys.45 The questionnaire contained items on basic background profile, khat chewing habit, other substance use behavior, and other pertinent information. Though indirect and weak, two honesty questions45 were also included in the questionnaire to check the trustworthiness of the students’ responses.
Before the actual data collection, the questionnaire was pretested on 50 university students recruited from another nearby university (Dilla University) which is located 90 kilometers south of Hawassa. After completing the pretest questionnaire, participants were also asked if they had difficulty understanding any of the questions. Subsequently, a few questions were paraphrased to make them more understandable.46
Data collection sessions were arranged by communicating with concerned bodies at all levels. Students were seated widely apart to ensure privacy in the rooms used to complete the questionnaire. Students were oriented about the objective of the study, why and how they were selected, about confidentiality of the information they provide and voluntary participation, and how to fill the questionnaire. Then the students were provided with the questionnaire to fill out and a nonreturnable pen. The English version of the questionnaire was made available for those who reported difficulty understanding Amharic. In each section, the data collection was facilitated by data collection facilitators and the principal investigator. None of the data collection facilitators were known to the students. No other person was allowed to enter the room during the data collection sessions to provide students the maximum privacy possible.
Study variables
The dependent (outcome) variable for this study was “current regular khat chewing” which we defined as khat chewing at least once weekly for the past one year or more by adopting the definition used for other substances.38,39 It was computed based on two questions regarding the duration (in years) of chewing and the number of days of chewing khat per week. Regarding the independent variables, students’ living arrangement referred to where the students were living while attending their university education. It consisted of three possible options: on-campus (dormitory), off-campus in rented house and off-campus with parents/relatives. Having a father, a mother, or a sibling who chews khat referred to whether the respondent had a father, a mother or a sibling whom he/she had ever seen/witnessed chewing khat. Response categories were “yes” or “no”. Having peers who chew khat referred to whether the respondents had any friends whom they had ever seen/witnessed chewing khat. Here also response categories were “yes” or “no”. Cigarette smoking and alcohol drinking also referred to whether the respondents had ever used these substances and responses were categorized as “yes” or “no”.
Statistical analysis
The data were double-entered using the software Epi Info version 3.5 and cleaned by comparing the two datasets using Epi Info’s “Data Compare” utility. Data were then exported to Stata version 12 (StataCorp LP, College Station, TX, USA) for further processing. All required variable recoding and transformation were done before the final data analysis.
As the sampling design used was a two-stage complex sampling involving stratification, clustering, and unequal probability of selecting study units, data analysis took explicit consideration of these design features of the study. For this purpose we created strata and cluster identifiers and computed finite population correction factors for both stages of sampling. We computed selection probabilities of sampling units at each stage of sampling and calculated the sample selection weight. We also did post-stratification by sex and determined post-stratification weight. The final analysis weight was then calculated as the product of the sample selection weight and the post-stratification weight as recommended by Heeringa et al.35 All the above stratification, clustering and weighting features of the study were declared in Stata prior to the data analysis.
The item-missing data rate of our study ranged from 0.24% to 11.71%. Cumulatively, the proportion of study units being excluded by case-wise deletion in the adjusted analysis reached more than 15%. Hence, we used multiple imputation technique to replace the missing items and to retain as much of the respondents in the analysis as possible. We accomplished the task of imputation using chained equations (also known as sequential regression)47 in Stata. We created 20 imputations (M=20) using a burn-in period of ten after checking the convergence of the imputation models using trace plots as indicated in Stata manual.48 We handled issues of perfect prediction using augmentation technique.48,49 Though we succeeded in imputing most of the important variables, we could not impute some variables due to a problem with model convergence. After accomplishing the imputation, we compared the descriptive summaries of imputed variables after imputation with those before imputation. They were all found to be comparable verifying that nothing abnormal occurred during imputation.48
To identify factors associated with current regular khat chewing, we started with unadjusted logistic regression analysis using each of the possible independent variables: sex; age; field of study; year of study; living arrangement – dormitory, off-campus rented house, off-campus with parents/relatives; religion; place of upbringing – urban vs rural; amount of monthly pocket money; having a father who chews khat; having a mother who chews khat; having a sibling who chews khat; having peers who chew khat; campus location – within town vs in the outskirts/out of town; cigarette smoking status; and alcohol drinking status. Following the unadjusted analysis, we selected for the initial adjusted model variables with P-values up to 0.25 in the unadjusted analysis and those deemed important based on literature.35,50,51 We refined the initial adjusted model by removing variables with insignificant coefficients on joint test and whose removal does not significantly affect both the Wald test for all parameters and the coefficients of the individual variables remaining in the model. Inclusion of relevant interaction terms (sex and cigarette smoking, sex and alcohol drinking, religion and alcohol drinking, and religion and cigarette smoking) and higher-order terms did not significantly improve the model. The final model was thus only a main effects model of significant factors and factors deemed important based on literature though not significant in the present study.
We used Monte Carlo error (MCE) estimates as per White et al’s47 guideline to assess the reproducibility of our multiple-imputation-based results. As recommended, the MCE for each coefficient in the adjusted model was less than or equal to 10% of its standard error. The MCEs for all t-statistics lay in the range of 0.04–0.09 (ie, less than or equal to the 0.1 cutoff) except for “having peers who chew khat” (MCE =0.23) and smoking cigarettes (MCE =0.50). Besides, all P-values had MCEs in the range 0.000–0.017 (ie, roughly less than or equal to the 0.01 cutoff) except for the “third year” category of year of study (MCE =0.026), the “off-campus with parent/relatives” category of living arrangement (MCE =0.034), and the “other” category of religion (MCE =0.044). No variable had MCEs beyond the recommended cutoff on more than one criterion. These MCE estimates were fairly acceptable suggesting the reproducibility of the results.
Ethical considerations
The study obtained ethical clearance from the Institutional Review Board of the College of Medicine and Health Sciences of Hawassa University, Hawassa, Ethiopia. No personal identifier of the study participants was taken and hence the data obtained remained anonymous. Participation in the study was only on voluntary basis. As the study entails a very minimal risk and also to ensure the anonymity of responses, respondents took part in the study after verbal informed consent.52
Results
The proposed sample size for this study was 1,290. Of this, 1,255 students participated in the study making the response rate 97.3%. The study population comprised of 74% males and 26% females. By year of study, 53% were in their second year, 36% were third year, and 11% fourth year and above. Orthodox Christians comprised 64%, Protestants 21%, and Muslims 12%. The average age of the study participants was 21.4 years (± standard deviation =1.6 years). Details of the background characteristics of the study participants are given in Table 1.
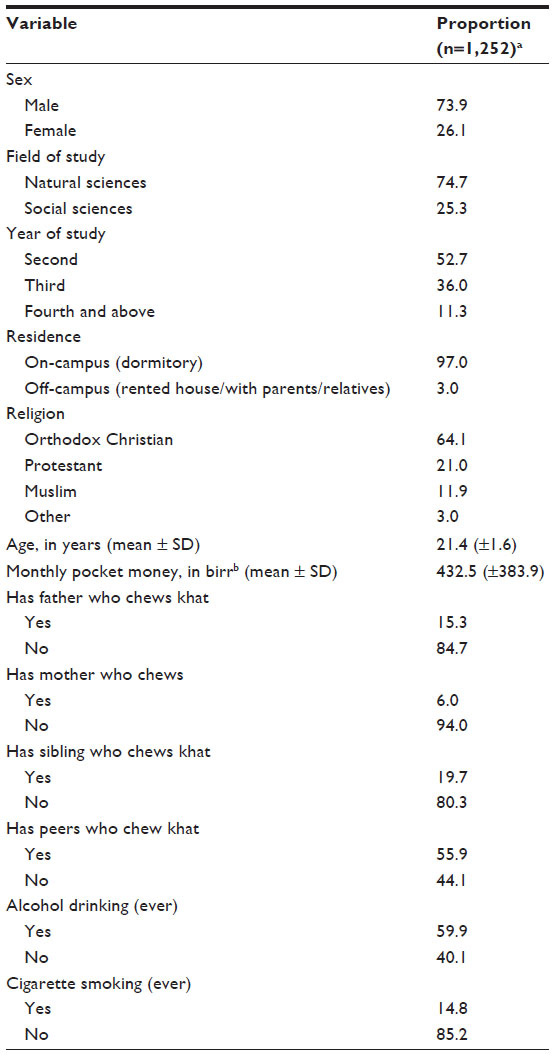 | Table 1 Background characteristics of the study participants, Hawassa University, southern Ethiopia, June 2014 |
Prevalence of khat chewing
The prevalence of current regular khat chewing was 10.5% (95% confidence interval [CI]: 6.1%–14.9%). While the lifetime prevalence was 22.8% (95% CI: 17.2%–28.4%), for the 12 months period preceding the study, the prevalence was 15.9% (95% CI: 11.3%–20.4%). For the last 30 days it was 11.1% (95% CI: 7.6%–14.7%) (Table 2). Among the khat chewers, 35.6% chewed one bundle or more khat in a session.
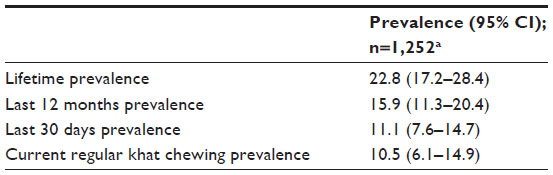 | Table 2 Prevalence of khat chewing, Hawassa University, southern Ethiopia, June 2014 |
Various reasons were reported for chewing khat by those who do. The three prominent reasons were: to be able to concentrate while reading (38.9%), to relax (37.7%), and to pass time (22.9%) (Table 3).
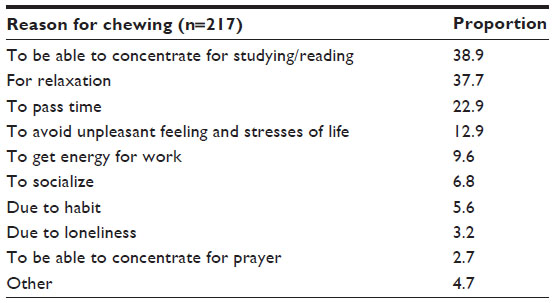 | Table 3 Reasons for khat chewing, Hawassa University, southern Ethiopia, June 2014 |
Factors associated with current regular khat chewing
Using complex sample survey logistic regression we identified different variables that were associated with current regular khat chewing. These included year of study, living arrangement, religion, having a father who chews khat, having peers who chew khat, and cigarette smoking. Compared to second year students, those in their fourth year or above had about twice higher odds of current regular khat chewing (adjusted odds ratio [AOR] [95% CI] =2.03 [1.22–3.36]). Students who live off-campus in rented houses also had about eight times higher odds of current regular khat chewing relative to those who live on-campus in a dormitory (AOR [95% CI] =8.09 [1.56–42.01]). Having a father who chews khat was also a powerful influence (AOR [95% CI] =3.68 [2.13–6.37]). Those with khat chewing peers had more than four times higher odds of being current regular khat chewers (AOR [95% CI] =4.62 [1.98–10.74]). Table 4 summarizes the results on factors associated with current regular khat chewing.
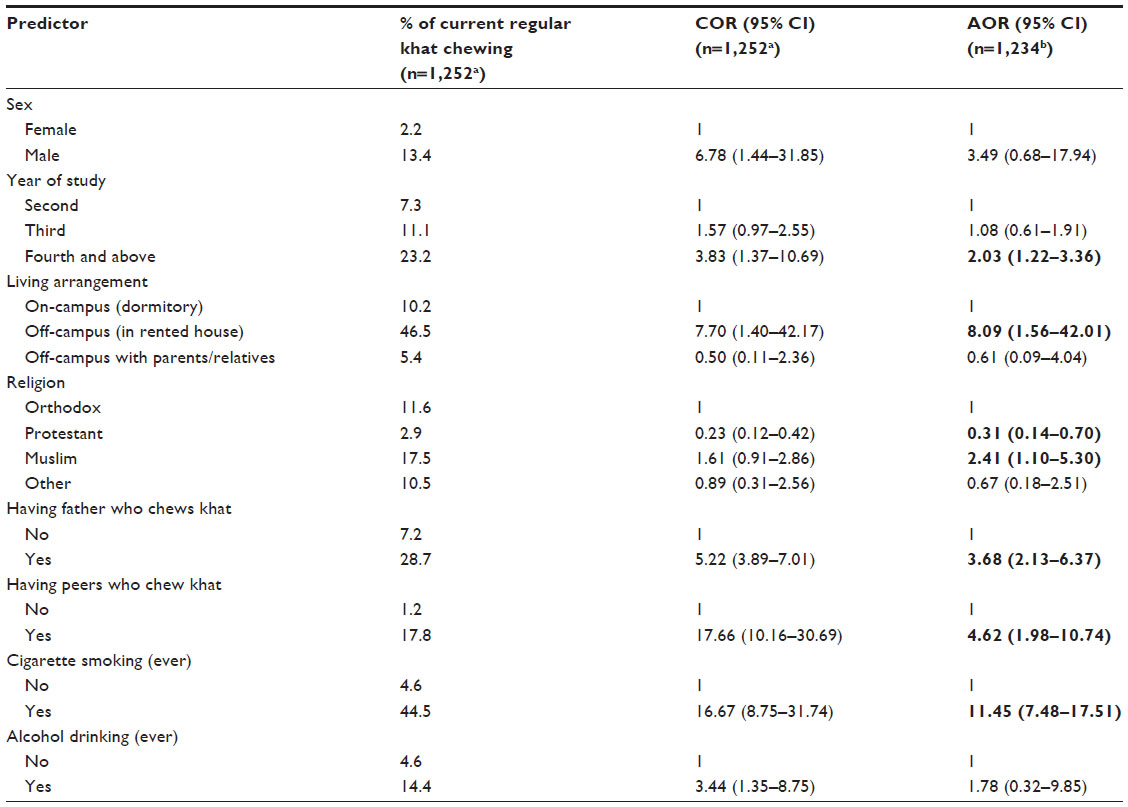 | Table 4 Factors associated with current regular khat chewing among the study participants, Hawassa University, southern Ethiopia, June 2014 |
Findings from honesty questions
When asked whether they would admit it in the questionnaire if they had ever used cannabis, about 61% said yes, 17% said not sure, and 22% said no. Similarly, when asked whether they would admit it in the questionnaire if they had ever used opium or heroin, 59% said yes, 20% said not sure, and 21% said no.
Discussion
In this study, we determined the prevalence of and factors associated with current regular khat chewing among the student population of Hawassa University, southern Ethiopia. As shown in the introduction of this article, khat chewing is associated with a range of physical and psychological health problems. Hence this study is deemed important from public health and clinical perspectives because it documents the magnitude of and factors associated with this important risk factor in a population of young university students.
The prevalence of current regular khat chewing identified by this study is nearly 11%. Being in the senior year, off-campus rented-house residence, being Muslim, having a father who chews khat, having friends who chew khat, and having ever smoked cigarettes all increase the odds of current regular khat chewing.
The lifetime prevalence of khat chewing identified by the current study generally falls within the range of lifetime prevalence values (14%–41%) among students of higher education institutions (universities and colleges) in Ethiopia reported in earlier studies.22–27 Though previous studies did not report on the magnitude of current regular use of khat among university (or college) students in Ethiopia, this study reveals that current regular use is common.
Many of the factors associated with current regular khat chewing identified by this study are consistent with factors identified by previous studies both in Ethiopia and abroad.22,25,27,32,33 However, living arrangement as an important predictor of khat chewing was not considered or not reported in previous studies except for two.27,36 In one of the studies36 it was considered as a possible predictor of harmful khat use among khat chewers and was not found to have a significant association. In the other study27 it showed a significant association with students’ khat chewing habit. Why living arrangement is overlooked in previous studies could be because in earlier times for students joining university for undergraduate study in Ethiopia, dormitory was the only option where students could reside and hence off-campus residing was not an issue. Recent studies might have overlooked the issue simply because it was not raised as an issue in most existing literature on khat.
The finding of the present study that paternal khat use is associated with higher odds of current regular khat chewing is in agreement with previous studies.32,53 Paternal substance use in general has been shown to be associated with higher odds of substance use among high school students in southeast Ethiopia54 and among adolescents elsewhere.55 Previous studies have also shown paternal alcohol abuse to be significantly associated with alcohol abuse among adolescents and young adults.56–58 It seems that children are at more odds to imitate the substance use behavior of their fathers.
The peer influence on current regular khat chewing is also consistent with previous studies which reported higher odds of khat chewing among students who had khat chewing peers.22,25,32,33,53,59 This association can be viewed from two perspectives. On the one hand, students who were not khat chewers could indulge in the habit because of their company with khat chewer friends. In the traditional khat chewing areas, chewing is mostly not a solitary practice.60–62 People chew khat in the company of friends discussing issues deemed important by the chewers.60,61 Hence, as Hansen61 noted, some chewers may attend chewing sessions mainly for socialization while not much interested in the chewing. As also shown by the present and other studies,62 socialization is one of the reasons ascribed to khat chewing. Thus, the need to socialize and be “in the mood of friends” could be how peer pressure exerts its influence. Previous studies21,28,33 have also documented “peer pressure” to be the reason for commencing the chewing habit. Peer pressure has also been found to be significantly associated with alcohol use,58 use of different substances,63 and risky sexual behavior64 among adolescents. On the other hand, being a khat chewer may be the reason for establishing friendship with khat chewing peers. Students may prefer to be friends with those who have a similar khat use status to themselves. Studies have shown the tendency of adolescents’ preference to befriend friends who are similar to them in terms of marijuana use65 and alcohol use.66
Cigarette smoking is also found to be significantly associated with current regular khat chewing. This finding is in harmony with previous studies22,25,32,33,53 which reported higher odds of khat chewing among respondents who reported cigarette smoking. Kassim et al67 have reported that khat chewing initiated tobacco smoking in 45% of simultaneous tobacco and khat users. So, as smoking could be an entry point to the khat chewing habit, the reverse could also be true.
While we found that students in the fourth year and above have about twice higher odds of engaging in current regular khat chewing, previous studies25,32 did not find a statistically significant association between khat chewing and year of study after controlling for other covariates. However, Tesfaye et al26 have found third year students (compared to first years) to be at higher odds of engaging in substance use. The higher odds of regular use of khat by senior students may be a result of cumulative exposure to khat chewing peers and khat chewing environment.
Another important factor associated with current regular use of khat is living off-campus in a rented house. It increased the odds of current regular khat chewing by about eight times relative to those living in dormitories. As only a very small fraction of students were living off-campus at the time of the study, the CI of the AOR for off-campus residence was very wide indicating inadequacy of the sample size to precisely estimate the magnitude of the association. Yet, the point estimate of the odds ratio was big (ie, 8.09) and the CI does not embrace the null value of 1 indicating a statistically significant association. Thus, the higher odds may indicate a higher risk of students residing off-campus in rented houses to engage in behaviors such as regular khat use due to absence of supervision by dormitory proctors and parents/guardians. Gebrehanna et al36 have argued that due to prohibition of khat chewing in university campuses, students may socialize with new friends in the community or go to khat selling shops to find a safer khat chewing place. In this sense, living off-campus in rented houses could also serve as a means of escape from the stricter rules against the use of substances in the university compound.
Our finding that sex is not significantly associated with current regular khat chewing is not consistent with previous studies which reported on the association between sex and khat chewing23,25,27, 32,33,59 and between sex and substance use in general21,26,54 among secondary school and university/college students. This inconsistency might have resulted mainly from differences in data analysis approaches. Whereas all the mentioned studies used a complex multistage sampling technique, none of them took the sampling design into account during the analysis. Besides, in none of the studies were study participants stratified by sex either at the design or analysis stage of the studies. However, we explicitly took account of the complex sampling design which included post-stratification weighting to attenuate possible bias due to under coverage35 of female students in the sample. However, the wide CI of the AOR for sex (0.68–17.94) indicates that the sample size was not large enough to precisely estimate the association between sex and regular khat chewing and hence the absence of association could also be due to lack of sufficient statistical power.
Alcohol drinking is also not significantly associated with current regular khat chewing. This too is not in congruence with previous findings.22,25,33 Failure of previous studies to take account of sampling design in the analysis might have resulted in a biased estimate of the association between khat chewing and alcohol drinking due to underestimation of standard errors.35
Although social desirability bias is a possibility in this study, previous studies in different countries testified that school surveys have high reliability and validity.68 Besides, we included honesty questions in our questionnaire in accordance with methodological recommendation for student drug surveys.45 As only a smaller fraction of the students did manifest a propensity of not giving honest responses, the likelihood of our findings being considerably distorted by social desirability bias is considered minimal.
In Ethiopia, drug and substance abuse prevention in schools and higher education institutes is considered a core agendum for the success of education and for peaceful accomplishment of teaching and learning activities.69 The students’ discipline guideline of Hawassa University stipulates that trying to enter the university campus with khat or being found in dormitories chewing or in possession of khat is punishable by academic suspension of one semester to one year. While such measures may help to ameliorate drug and substance abuse (including khat chewing) in the university, lessons learned from campus-based alcohol prevention programs indicate that individual-oriented approaches are not enough to ameliorate the problem and call for a multipronged approach involving the institution of higher learning (ie, the university), the surrounding community and state and federal regulatory bodies (an approach called environmental management).70 Individual-oriented interventions and environmental management could complement one another71 and lead to better results.
Conclusion
Almost one in ten university students is a current regular khat chewer. Peer influence and residing off-campus in rented houses are independently associated with the practice. A multipronged prevention approach involving students, the university, the surrounding community and regulatory bodies is recommended.
Acknowledgments
We are grateful to colleagues at the School of Public and Environmental Health of Hawassa University, and department/school heads, teachers and Students’ Council members in different campuses of Hawassa University for their kind assistance during the process of data collection. We are also indebted to the study participants for willfully taking part in the study. We gratefully acknowledge the financial and material contributions from Hawassa University and Addis Continental Institute of Public Health.
Disclosure
The authors report no conflicts of interest in this work.
References
Odenwald M, Klein A, Warfa N. Khat addiction. In: Miller PM, editor. Principles of Addiction: Comprehensive Addictive Behaviors and Disorders. Vol 1. USA: Elsevier; 2013. | |
Lemessa D. Khat (Catha edulis): Botany, Distribution, Cultivation, Usage and Economics in Ethiopia. Addis Ababa: United Nations Development Programme, Emergencies Unit for Ethiopia (UNDP-EUE); 2001. | |
Fitzgerald J, Lawrence L. Khat: A Literature Review. Melbourne: Centre for culture, ethnicity and health; 2009. | |
Ben-Shabat S, Goloubinoff P, Dudai N, Lewinsohn E. Farming amphetamines: Khat (Catha edulis Forsk.) a traditional plant with mild stimulating psychoactive and medicinal properties. In: Yaniv Z, Dudai N, editors. Medicinal and Aromatic Plants of the Middle-East. Dordrecht: Springer; 2014:181–197. | |
Kalix P, Braenden O. Pharmacological aspects of the chewing of khat leaves. Pharmacol Rev. 1985;37(2):149–164. | |
Brenneisen R, Fisch HU, Koelbing U, Geisshusler S, Kalix P. Amphetamine-like effects in humans of the khat alkaloid cathinone. Br J Clin Pharmac. 1990;30(6):825–828. | |
Widler P, Mathys K, Brenneisen R, Kalix P, Fisch HU. Pharmacodynamics and pharmacokinetics of khat: A controlled study. Clin Pharmacol Ther. 1994;55(5):556–562. | |
Getahun W, Gedif T, Tesfaye F. Regular Khat (Catha edulis) chewing is associated with elevated diastolic blood pressure among adults in Butajira, Ethiopia: A comparative study. BMC Public Health. 2010;10:390. | |
Tesfaye F, Byass P, Wall S, Berhane Y, Bonita R. Association of smoking and khat (Catha edulis Forsk) use with high blood pressure among adults in Addis Ababa, Ethiopia, 2006. Prev Chronic Dis. 2008;5(3):A89. | |
Al-Motarreb A, Al-Habori M, Broadley KJ. Khat chewing, cardiovascular diseases and other internal medical problems: The current situation and directions for future research. J Ethnopharmacol. 2010;132(3):540–548. | |
Cox G, Rampes H. Adverse effects of khat: a review. Advances in Psychiatric Treatment. 2003;9(6):456–463. | |
Ali WM, Zubaid M, Al-Motarreb A, et al. Association of khat chewing with increased risk of stroke and death in patients presenting with acute coronary syndrome. Mayo Clin Proc. 2010;85(11):974–980. | |
Kedir H, Berhane Y, Worku A. Khat chewing and restrictive dietary behaviors are associated with anemia among pregnant women in high prevalence rural communities in eastern Ethiopia. PLoS One. 2013;8(11):e78601. | |
Khatib M, Jarrar Z, Bizrah M, Checinski K. Khat: social habit or cultural burden? A survey and review. J Ethn Subst Abuse. 2013;12(2):140–153. | |
Astatkie A, Demissie M, Berhane Y. The association of khat (Catha edulis) chewing and orodental health: A systematic review and meta-analysis. S Afr Med J. 2014;104(11):773–779. | |
Kassim S, Islam S, Croucher R. Validity and reliability of a Severity of Dependence Scale for khat (SDS-khat). J Ethnopharmacol. 2010;132(3):570–577. | |
Griffiths P, Gossop M, Wickenden S, Dunworth J, Harris K, Lloyd C. A transcultural pattern of drug use: qat (khat) in the UK. Br J Psychiatry. 1997;170:281–284. | |
Kassim S, Croucher R, al’Absi M. Khat dependence syndrome: A cross sectional preliminary evaluation amongst UK-resident Yemeni khat chewers. J Ethnopharmacol. 2013;146(3):835–841. | |
Widmann M, Warsame AH, Mikulica J, et al. Khat use, PTSD and psychotic symptoms among Somali refugees in Nairobi – a pilot study. Front Public Health. 2014;2:71. | |
Odenwald M, Neuner F, Schauer M, et al. Khat use as risk factor for psychotic disorders: A cross-sectional and case-control study in Somalia. BMC Med. 2005;3:5. | |
Aklog T, Tiruneh G, Tsegay G. Assessment of substance abuse and associated factors among students of Debre Markos Poly Technique College in Debre Markos Town, East Gojjam Zone, Amhara Regional State, Ethiopia, 2013. Global Journal of Medical Research. 2013;13(4-B):5–15. | |
Deressa W, Azazh A. Substance use and its predictors among undergraduate medical students of Addis Ababa University in Ethiopia. BMC Public Health. 2011;11:660. | |
Mulugeta Y. Khat chewing and its associated factor among College students in Bahir Dar town, Ethiopia. Science Journal of Public Health. 2013;1(5):209–214. | |
Kebede Y. Cigarette smoking and Khat chewing among college students in North West Ethiopia. Ethiop J Health Dev. 2002;16(1):9–17. | |
Gebreslassie M, Feleke A, Melese T. Psychoactive substances use and associated factors among Axum University students, Axum town, north Ethiopia. BMC Public Health. 2013;13:693. | |
Tesfaye G, Derese A, Hambisa MT. Substance use and associated factors among university students in Ethiopia: A cross-sectional study. J Addict. 2014;2014:969837. | |
Gebrehanna E, Berhane Y, Worku A. Khat chewing among Ethiopian university students – a growing concern. BMC Public Health. 2014;14:1198. | |
Kassa A, Taddesse F, Yilma A. Prevalence and factors determining psychoactive substance (PAS) use among Hawassa University (HU) undergraduate students, Hawassa, Ethiopia. BMC Public Health. 2014;14:1044. | |
Nigussie T, Gobena T, Mossie A. Association between khat chewing and gastrointestinal disorders: a cross sectional study. Ethiop J Health Sci. 2013;23(2):123–130. | |
Birhanu Y, Meressa K, Mossie A, Gelaw Y. Effect of substance use on academic achievement of health officer and medical students of Jimma University, southwest Ethiopia. Ethiop J Health Sci. 2009;19(3):155–163. | |
Addis T. Substance abuse and the risk of HIV/AIDS in students attending Addis Ababa University, Ethiopia. Harar Bulletin of Health Sciences. 2012 (Special Issue: Addis Continental Institute of Public Health Research Extract Number 5):141–157. | |
Alsanosy RM, Mahfouz MS, Gaffar AM. Khat chewing among students of higher education in Jazan region, Saudi Arabia: prevalence, pattern, and related factors. Biomed Res Int. 2013;2013:487232. | |
Tsegay G, Esmael A. Psychoactive substances use (khat, alcohol and tobacco) and associated factors among Debre Markos University Students, North-West Ethiopia, 2013. J Def Manag. 2014;4(1):1000118. | |
Lohr SL. Sampling: Design and Analysis. 2nd ed. Boston: Brooks/Cole; 2010. | |
Heeringa SG, West BT, Berglund PA. Applied Survey Data Analysis. Boca Raton, FL: Chapman and Hall/CRC; 2010. | |
Gebrehanna E, Berhane Y, Worku A. Prevalence and predictors of harmful khat use among university students in Ethiopia. Subst Abuse. 2014;8:45–51. | |
Bachman GG, O’Malley PM, Schulenberg JE, Johnston LD, Bryant AL, Merline AC. The Decline of Substance use in Young Adulthood: Changes in Social Activities, Roles, and Beliefs. Mahwah, New Jersey: Lawrence Erlbaum Associates, Publishers; 2002. | |
Underwood B, Fox K. A survey of alcohol and drug use among UK based dental undergraduates. Br Dent J. 2000;189(6):314–317. | |
White HR, Jarrett N, Valencia EY, Loeber R, Wei E. Stages and sequences of initiation and regular substance use in a longitudinal cohort of black and white male adolescents. J Stud Alcohol Drugs. 2007;68(2):173–181. | |
wikipedia.org [homepage on the Internet]. Hawassa University. Available from: https://en.wikipedia.org/wiki/Hawassa_University. Accessed November 12, 2014. | |
Corporate Communication and Marketing Directorate. Hawassa University Facts and Figures. Hawassa: Hawassa University; 2013. | |
Dean AG, Sullivan KM, Soe MM. OpenEpi: Open source epidemiologic statistics for public health. Version 2.3. Available from: http://www.OpenEpi.com. Accessed January 25, 2015. | |
Bjarnason T. Sampling issues in school surveys of adolescent substance use. Conducting School Surveys on Drug Abuse. Vienna, Austria: United Nations Office on Drugs and Crime; 2003. | |
Central Statistics Agency [Ethiopia], ICF International. Ethiopia Demographic and Health Survey 2011. Addis Ababa, Ethiopia and Calverton, Maryland, USA: Central Statistics Agency and ICF International; 2012. | |
Smart RG, Hughes PH, Johnston LD, et al. A Methodology for Student Drug Survey. Geneva: World Health Organization; 1980. | |
Collins D. Pretesting survey instruments: An overview of cognitive methods. Qual Life Res. 2003;12(3):229–238. | |
White IR, Royston P, Wood AM. Multiple imputation using chained equations: Issues and guidance for practice. Stat Med. 2011;30(4):377–399. | |
StataCorp. Stata 12 Multiple-Imputation Manual. College Station, Texas: Stata Press 2011. | |
White IR, Daniel R, Royston P. Avoiding bias due to perfect prediction in multiple imputation of incomplete categorical variables. Comput Stat Data Anal. 2010;54(10):2267–2275. | |
Bursac Z, Gauss CH, Williams DK, Hosmer DW. Purposeful selection of variables in logistic regression. Source Code Biol Med. 2008;3:17. | |
Hosmer DW, Lemeshow S, Sturdivant RX. Applied Logistic Regression. 2nd ed. Hoboken, New Jersey, USA: John Wiley and Sons, Inc.; 2013. | |
Research Ethics Review Committee (WHO ERC). The Process of Obtaining Informed Consent. Geneva, Switzerland: World Health Organization. Availble from: http://www.who.int/rpc/research_ethics/Process_seeking_IF_printing.pdf. Accessed: January 1, 2015. | |
Mahfouz MS, Alsanosy RM, Gaffar AM. The role of family background on adolescent khat chewing behavior in Jazan Region. Ann Gen Psychiatry. 2013;12(1):16. | |
Dida N, Kassa Y, Sirak T, Zerga E, Dessalegn T. Substance use and associated factors among preparatory school students in Bale Zone, Oromia Regional State, Southeast Ethiopia. Harm Reduct J. 2014;11:21. | |
Johnson V, Pandina RJ. Effects of the family environment on adolescent substance use, delinquency, and coping styles. Am J Drug Alcohol Abuse. 1991;17(1):71–88. | |
Lieb R, Merikangas KR, Hofler M, Pfister H, Isensee B, Wittchen HU. Parental alcohol use disorders and alcohol use and disorders in offspring: a community study. Psychol Med. 2002;32(1):63–78. | |
Rohde P, Lewinsohn PM, Kahler CW, Seeley JR, Brown RA. Natural course of alcohol use disorders from adolescence to young adulthood. J Am Acad Child Adolesc Psychiatry. 2001;40(1):83–90. | |
Van Der Vorst H, Vermulst AA, Meeus WHJ, Dekovic M, Engels RC. Identification and prediction of drinking trajectories in early and mid-adolescence. J Clin Child Adolesc Psychol. 2009;38(3):329–341. | |
Reda AA, Moges A, Biadgilign S, Wondmagegn BY. Prevalence and determinants of khat (Catha edulis) chewing among high school students in Eastern Ethiopia: A cross-sectional study. PLoS One. 2012;7(3):e33946. | |
Ageely HM. Health and socio-economic hazards associated with khat consumption. J Family Community Med. 2008;15(1):3–11. | |
Hansen P. The ambiguity of khat in Somaliland. J Ethnopharmacol. 2010;132(3):590–599. | |
Dessie G. Is Khat a Social Ill? Ethical Arguments about a ‘Stimulant’ Among the Learned Ethiopians. Leiden, The Netherlands: African Studies Centre; 2013. | |
Needle R, McCubbin H, Wilson M, Reineck R, Lazar A, Mederer H. Interpersonal influences in adolescent drug use-The role of older siblings, parents, and peers. Int J Addict. 1986;21(7):739–766. | |
Cherie A, Berhane Y. Peer pressure is the prime driver of risky sexual behaviors among school adolescents in Addis Ababa, Ethiopia. World J AIDS. 2012;2:159–164. | |
de la Haye K, Green HD Jr, Pollard MS, Kennedy DP, Tucker JS. Befriending risky peers: Factors driving adolescents’ selection of friends with similar marijuana use. J Youth Adolesc. Epub November 4, 2014. | |
Osgood DW, Ragan DT, Wallace L, Gest SD, Feinberg ME, Moody J. Peers and the emergence of alcohol use: Influence and selection processes in adolescent friendship networks. J Res Adolesc. 2013; 23(3):doi:10.1111/jora.12059. | |
Kassim S, Rogers N, Leach K. The likelihood of khat chewing serving as a neglected and reverse ‘gateway’ to tobacco use among UK adult male khat chewers: a cross-sectional study. BMC Public Health. 2014;14:448. | |
Hibell B. Overview of methodological issues. Conducting School Surveys on Drug Abuse: Global Assessment Programme on Drug Abuse. Vienna, Australia: United Nations Office on Drugs and Crime; 2003. | |
unesco.org [homepage on the Internet]. Federal Ministry of Education Addis Ababa. Education Sector Development Program IV (ESDP IV) 2010/2011–2014/2015: Program Action Plan. Addis Ababa: FMOE; 2010. Available from: http://planipolis.iiep.unesco.org/upload/Ethiopia/Ethiopia_ESDP_IV.pdf. Accessed January 25, 2015. | |
DeJong W, Langford LM. A typology for campus-based alcohol prevention: Moving toward environmental management strategies. J Stud Alcohol. 2002;(14):140–147. | |
Larimer ME, Kilmer JR, Lee CM. College student drug prevention: A review of individually-oriented prevention strategies. J Drug Issues. 2005;35(2):431–456. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.