Back to Journals » Journal of Blood Medicine » Volume 10
Prevalence, Morphological Classification, And Factors Associated With Anemia Among Pregnant Women Accessing Antenatal Clinic At Itojo Hospital, South Western Uganda
Authors Okia CC, Aine B, Kiiza R, Omuba P, Wagubi R ![]() , Muwanguzi E, Apecu RO, Okongo B
, Muwanguzi E, Apecu RO, Okongo B ![]() , Oyet C
, Oyet C
Received 21 May 2019
Accepted for publication 18 September 2019
Published 22 October 2019 Volume 2019:10 Pages 351—357
DOI https://doi.org/10.2147/JBM.S216613
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin Bluth
Claire Catherine Okia,1 Boaz Aine,1 Ronald Kiiza,1 Patrick Omuba,1 Robert Wagubi,1 Enoch Muwanguzi,1 Richard Onyuthi Apecu,1 Benson Okongo,1 Caesar Oyet2
1Department of Medical Laboratory Science, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda; 2Department of Clinical Chemistry, School of Medical Laboratory Sciences, Institute of Allied Health, Clarke International University, Kampala, Uganda
Correspondence: Benson Okongo
Department of Medical Laboratory Science, Faculty of Medicine, Mbarara University of Science and Technology, P.O.BOX 1410, Mbarara, Uganda
Tel +256-7785 57867
Fax +256 4854 20782
Email [email protected]
Purpose: The study aimed to determine the prevalence, morphological classification, and risk factors of anemia among pregnant mothers attending antenatal clinic at Itojo hospital, Ntungamo district, southwestern Uganda.
Patients and methods: After obtaining an informed consent, 5mL of blood was collected from the vein of each participant for complete blood count (CBC) and peripheral film report. The CBC was performed using HumaCount 80 hematology analyzer (HUMAN Gesellschaft für Biochemica und Diagnostica mbH Max-Planck-Ring 21 65,205 Wiesbaden Germany). Peripheral blood smears were made and stained using Wright’s Romanowsky stain and examined under ×1000 magnification for morphological classification of anemia. Structured questionnaires were administered to each participant to collect information on patients’ demography and risk factors of anaemia in pregnancy. The data generated were prepared in EXCEL and later transferred to SPSS version 20 for analysis. Univariate logistic regression and multivariate logistic regression were used to evaluate the association of socio-demographic characteristics of the participants with anemia. A 95% confidence level was used and statistical significance was reached at p<0.05.
Results: One hundred and sixty-three participants (n=163) were recruited for the study with the median age of 25 years and range of (17 to 40 years). The overall prevalence of anemia was 12 (7.4%), the morphological classification was 1 (8.3%) normocytic normochromic anemia, 6 (50%) microcytic hypochromic anemia, and 5 (41.7%) macrocytic anemia. Spouse occupation (p=0.03), household income (p=0.04), use of insecticide-treated mosquito nets (p=0.001), history of urinary tract infection (p=0.002), use of haematinics (p≤0.001), and history of postpartum hemorrhage (p=0.03) were significantly associated with anemia in pregnancy.
Conclusion: Despite the reported high prevalence of anemia in pregnancy in other areas within the country, anemia prevalence was low in this study. Routine screening for anemia at all antenatal care clinics countrywide is recommended.
Keywords: anemia, prevalence, risk factors, pregnancy
Introduction
Anemia in pregnancy is a worldwide health challenge affecting low-, middle-, and high-income countries with several impacts on health and socio-economic progress. It was approximated that nearly 40.1% of pregnant mothers develop anaemia globally.1 As defined WHO, anemia in pregnancy develops when hemoglobin (Hb) concentration reduces to <11g/dL with haematocrit of <0.33/L.2 Anaemia in pregnancy present similarly like anaemia in other categories with signs and symptoms which includes easy development of fatigue, general weakness, reduced cognition, and attention/concentration span and when not managed the affected mothers experience preterm birth with low birth weight babies.3
Global data now show that anaemia in pregnancy in low- and middle-income countries can be as high as 56%4 with continental variations; sub-Saharan Africa shows 57% prevalence, South-East Asia 48%, and South America at 24.1%.5 According to WHO, during pregnancy, anemia is identified by hemoglobin levels less than 11.0g/dL and may be divided into three levels of severity: mild anemia (Hb levels 9 to 10.9g/dL), moderate anemia (Hb levels 7 to 8.9g/dL), and severe anemia (Hb levels less than 7g/dL).13
There are several contributors to the development of anaemia in pregnancy in low-income countries which may include nutritional deficiencies of iron, folate, vitamins A and B12; parasitic infections or chronic infections with tuberculosisand HIV.6,7 These factors contribute to varying degrees in the development and progress of anaemia in pregnancy but in sub-Saharan Africa, low iron intake is seen as the leading cause of anemia in pregnancy.7,8
Several maternal anaemia control programs target antenatal care (ANC) services to deliver dewormers, iron/folate complements, malaria prophylaxis, and distribution of insecticide-treated nets (ITN). In Uganda, there has been poor utilization of (ITN) in rural areas9 and poor adherence to iron supplementation10 which thwarted the efforts to reduce anaemia in pregnancy.
According to Uganda Demographic and Health Surveys report, the prevalence of anemia among pregnant women was 38% in 201611 but with regional variations from 32.9% in Gulu, northern Uganda, i 12.1% in Hoima,12 and 32.5% in Mpigi.7 In Itojo district hospital, very few data exist about the prevalence of anemia among pregnant women accessing antenatal clinic.
The aim of the study was to determine the prevalence of anemia and identify risk factors associated with anaemia among pregnant women receiving ANC at Itojo hospital, Ntungamo district, southwestern Uganda.
Methods
This cross-sectional study was carried out at Itojo hospital, Ntungamo district, southwestern Uganda from September to December 2018. Pregnant women visiting Itojo district hospital for ANC were formally consented and enrolled in the study. The required sample size for enrolment was estimated using the formula for a single population proportion, with the following assumptions: anemia prevalence of 12.1%, 95% confidence level, and 5% marginal error. According to the study by Obai, Odongo, and Wanyama (2016), the prevalence of anemia in pregnancy in southwestern Uganda was estimated at 12.1%. Using the formula for sample size calculation for the proportion

where: n=the desired sample size.
Z=critical values of normal distribution at 95%, which corresponds to 1.96
P=the proportion of the target population estimated to have pre-diabetes.
d=estimated margin of error 5%
n = 163
Adjusting for design errors and non-response, the sample size was increased by 5% to 171%. Therefore, the minimum number of pregnant mothers required for the study was 171. However, due to low turn up of the ANC mothers at the facility, the number of 171 was not achieved.
The pregnant women were subjected to ultrasound scan to ascertain the state of the pregnancy and checked for multiple fetuses. Questionnaire was administered to collect information on socio-demographic, nutritional, obstetric and gynecological data, and clinical conditions. This was followed by a physical examination. Five milliliters of blood specimen was collected from each participant using the routine local blood collection guideline in Uganda by a laboratory technician.
Complete blood count was determined using HumaCount 80 hematology analyzer (Germany). Peripheral blood smears were made and stained using Wright’s Romanowsky stain and examined under ×1000 magnification for morphological classification of anemia.
The data generated were prepared in EXCEL and later transferred to SPSS version 20 for analysis. Univariate logistic regression and multivariate logistic regression were used to evaluate the association of socio-demographic characteristics of the participants with anemia. A 95% confidence level was used with a cut off p<0.05.
Ethical Consideration
The study was approved by the faculty research committee of Mbarara University of Science and Technology and Itojo district hospital director (approval number MUST/MLS/023). Written Informed consent was obtained from each participant included in the study and the study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki (1964). Privacy and confidentiality was ensured all through the study process and abnormal findings were shared with physicians from where the participants were managed.
Results
Demographic Characteristics Of The Study Participants
The median age of the participants was 25 years with interquartile range of 17, 40 years. Most of the women were formally married (95.7%), had primary education (61.9%), peasants (68.2%),19.6% in the first trimester, 36.8% in the second trimester, and (43.6%) were in their third trimester (43.6%) as shown in Table 1.
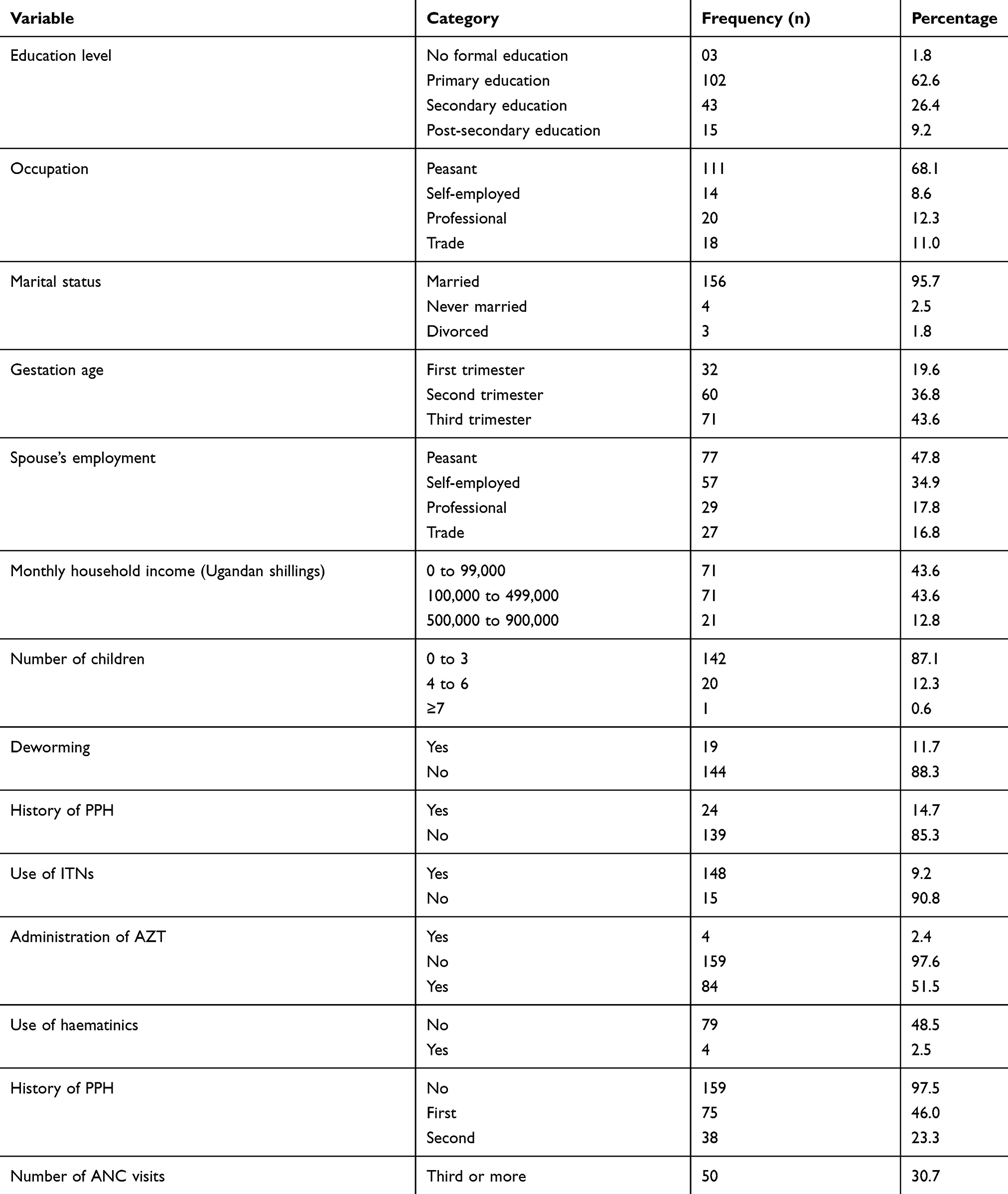 |
Table 1 Demographic Characteristics Of The Study Participants |
Prevalence Of Anemia
The general prevalence of anemia was 7.4% (Figure 1) with the mean Hb of 12.5g/dL, the minimum Hb 6.9g/dL, and maximum 15.3g/dL. 8.3% had severe anemia (Hb<7.0g/dL, WHO, 2017) and the rest had mild anemia. 92.6% of the participants had a normal Hb level and 7.4% had Hb below 11.0 g/dL. Of the anaemic participants, 91.7% had mild anaemia and 8.3% had severe anaemia. No participant had moderate anaemia.
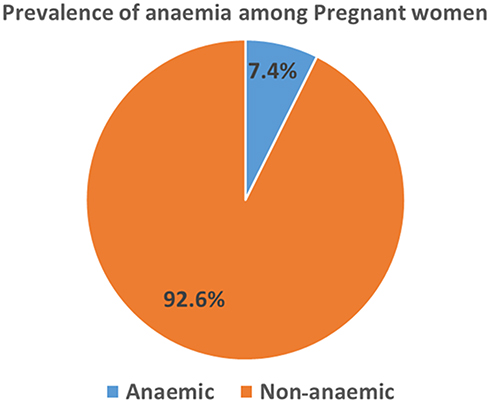 |
Figure 1 Pie chart showing the Overall Prevalence of Anemia among Pregnant Women at Itojo Hospital. |
Morphological Characterization Of Anemia
Based on the film reports, the majority of our participants with anemia had microcytic hypochromic blood picture 6 (50%), macrocytic normochromic were 5 (41.7%), and normocytic normochromic blood picture 1 (8.3%) (Figure 2).
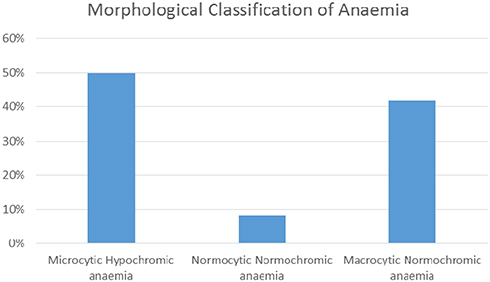 |
Figure 2 Morphological classification of anemia based on peripheral blood smear. |
Risk Factors Associated With Anemia
Several factors thought to be associated with anemia in pregnancy were studied. This included gestation age, marital status, number of children, occupation, education level, number of ANC visits, previous pregnancy outcomes and complications including PPH and preeclampsia among others. Multinomial logistic modeling was conducted to detect the association between these factors and anemia and the model was adjusted for the age of the participants. The results are as shown in Table 2.
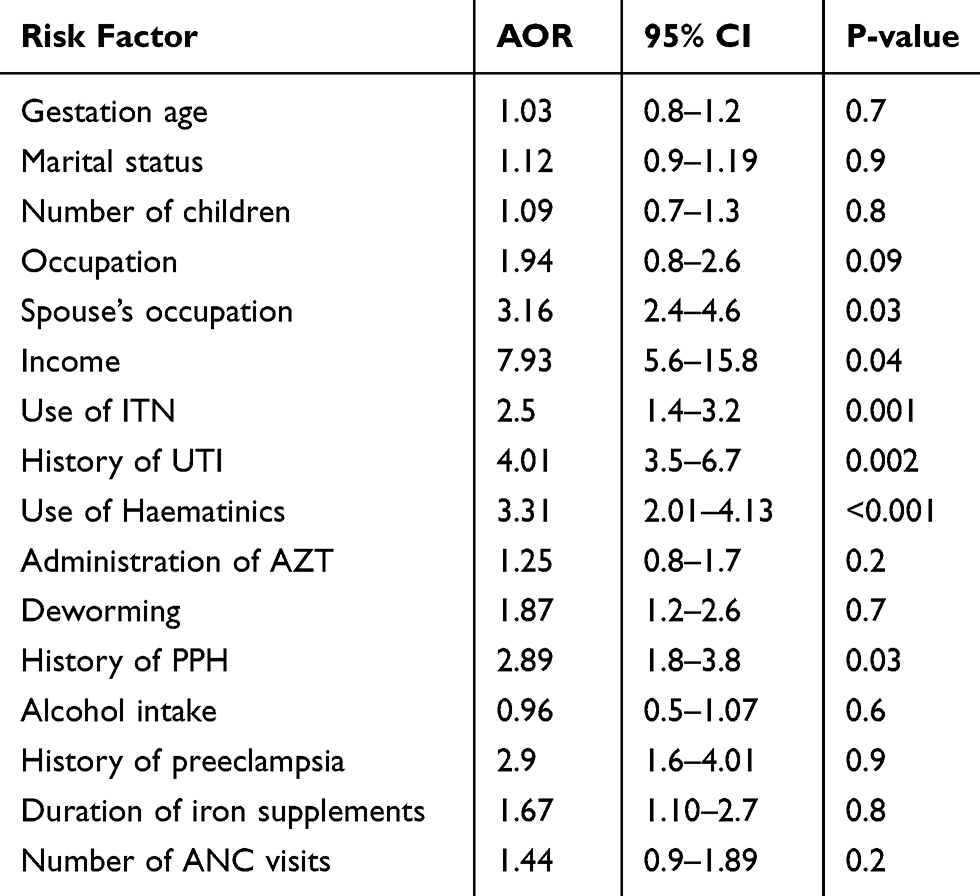 |
Table 2 Multinomial Modelling Describing The Risk Factors For Anemia (Adjusted For The Age Of The Participants) |
Discussion
Prevalence Of Anemia
Pregnancy-related anaemia is a worldwide health issue affecting low-, middle-, and high-income countries increasing the risk of pregnancy complications and deaths. The commonest cause of anaemia in pregnancy is the result of low iron intake that does not match the high demands during pregnancy. If not treated or managed, low blood iron level may increase the risk of reduced gestation age, low birth weights, restricted fetal growth, development of sepsis soon after birth with high chances of maternal and infant deaths.14,15
In this study, there were 7.4% cases of anaemia which is closely comparable with studies in Ethiopia 9.7%,16 Sudan 10%,17 and Ethiopia 11.6%.18 The prevalence is lower than the worldwide prevalence of anemia in pregnancy that has been estimated at 40.1%.1 Our prevalence, however, is lower than the national prevalence of Uganda (30.4%)19 showing spatial distribution of anaemia from region to region and relying on the study methods employed. Our prevalence was also lower compared to other studies within other regions of Uganda, a study in southwestern Uganda with 62.8% prevalence, Hoima 12.1%, and Gulu 32.9%.12 The low prevalence in this study could be due to improved services in Itojo hospital being supported by USAID funded project, through a $64.8 million, 5-year award from the US Agency for International Development, IntraHealth International is helping the government of Uganda improve the availability of improved health services in selected hospitals. Through this project, there is routine screening for anemia during antenatal clinic visits and those mothers found to be anemic are managed accordingly as opposed to other hospitals where routine screening for anemia is not carried out.
The prevalence of anaemia in the current study is also lower than those conducted outside Uganda such as in Kisangani DRC 76.2%,20 in southwest Ethiopia 23.5%,21 a study by Kwabena Acheampong et al (50.1%).22 The differences in the findings could be attributed to larger sample sizes, techniques used in HB estimation and geographical locations in these studies compared to our study. However, our finding is higher than the study in Ethiopia 2.8%.23
Morphological Classification Of Anemia
According to our study, the majority of our participants with anemia had a microcytic hypochromic blood picture (50%), followed by macrocytic normochromic (41.7%) and normocytic normochromic blood picture (8.3%). Other similar studies also showed that microcytic hypochromic anemia was the predominant morphological classification of anemia in pregnant women and these include; the study done at Mbarara regional referral hospital where microcytic hypochromic anemia was 76.68%,24and in Mulago Uganda, the common type of anemia was microcytic hypochromic anemia 34.1%,25 our findings disagreed with a study in Ethiopia, which found normocytic normochromic anemia being the commonest morphological type of anemia 76%.26 This variation could be closely associated with socio-economic differences and dietary variations.
Associated Risk Factors Of Anemia
Several factors are known to increase the risk of developing anaemia in pregnancy. These factors can range from modifiable socio-economic factors to non-modifiable demographic factors. In the current study, UTI was positively associated with anaemia in pregnancy (p=0.002 and CI of 3.5 to 6.7). This is in agreement with a study done at Mbarara regional referral hospital.24 The same was found in a cross-sectional study done in Kisangani DRC. There is increased incidence of UTI in pregnancy27 and it was suggested that some of the organisms known to cause UTI induce hemolysis when they release endotoxin in blood.28
Spouse occupation and low income were also significant factors associated with anemia in pregnancy with p=0.03 and 0.04, respectively. According to the data collected, the predominant spouse’s occupation was peasantry (47.8%) and the predominant household income being below Ugandan shillings 99,000 per month. This was in agreement with other studies conducted at Mbarara regional referral hospital24 and Kisangani in DRC.20 This may be due to the fact that these mothers cannot afford a balanced diet and live in unhealthy environments. These may predispose them to dietary deficiencies such as iron that is essential for blood formation.
Use of hematinics is protective against developing anemia in pregnancy as displayed by our finding with a p-value of <0.001 and (CI 0.71 to 0.99). This is in agreement with different studies conducted in Ethiopia,29 Uganda,7 that showed similar findings. This may be owing to the fact that those who complied and took the hematinics had a chance to increase a hemoglobin level thus were protected against developing anemia. Our study also agrees with the finding in a study done to assess the effect of routine iron supplementation on anemia in pregnancy where it was found out that daily iron supplementation reduced the risk of developing anemia by 73%.30
Use of insecticide-treated bed nets was also significantly protective against anemia, according to our study with a p=0.001. This is in an agreement with other studies that showed that not using ITN was associated with anemia, such as the study in Mbarara Uganda.24 This may be due to the fact that the use of ITN minimizes the risk of the pregnant mother being bitten by mosquitoes while sleeping, which can result into malaria being one of the risk factors to developing anemia as shown in other studies such as at Gilgel Gibe dam area, southwest Ethiopia.31 History of postpartum hemorrhage was also significantly associated with anemia among pregnant women, according to our findings with a p=0.03. Postpartum hemorrhage leads to increasing blood loss of greater than or equal to 1000 mL of blood loss following delivery32 and this results in loss of large amounts of iron in the body leading to less iron being available for erythropoiesis.33
Conclusion
Despite the reported high prevalence of anemia among pregnant women in other regions within the country, anemia prevalence was low in this study. Routine screening for anemia at all ANC clinics countrywide is recommended. The associated risk factors, according to our study were spouse occupation, household income, and history of urinary tract infections, use of hematinics and use of insecticide-treated mosquito nets.
Limitation Of The Study
The study did not collect risk factors that can predispose pregnant women to anemia. eg. malaria infections, hookworm infections.
Acknowledgments
The authors express their thanks to the administration of Itojo hospital for their support, guidance, and materials for the study and to the staffs of medical side laboratory, who provided them with the Wright’s stain for staining peripheral blood films. They also extend their special thanks and appreciation to the study participants, who voluntarily participated in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO G. WHO Methods and Data Sources for Global Burden of Disease Estimates 2000-2011. Geneva: Department of Health Statistics and Information Systems; 2016.
2. Sharma JB. Anaemia in pregnancy. Differ Diagn Obstetr Gynaecol. 2008;19.
3. Breymann C, Bian X-M, Blanco-Capito LR, Chong C, Mahmud G, Rehman R. Expert recommendations for the diagnosis and treatment of iron-deficiency anemia during pregnancy and the postpartum period in the Asia-Pacific region. J Perinat Med. 2011;39(2):113–121.
4. Black RE, Victora CG, Walker SP, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. lancet. 2013;382(9890):427–451.
5. De Benoist B, Cogswell M, Egli I, McLean E. Worldwide Prevalence of Anaemia 1993–2005; WHO Global Database of Anaemia. WHO Press. 2008.
6. Msuya SE, Hussein TH, Uriyo J, Sam NE, Stray-Pedersen B. Anaemia among pregnant women in northern Tanzania: prevalence, risk factors and effect on perinatal outcomes. Tanzan J Health Res. 2011;13(1):33–39.
7. Ononge S, Campbell O, Mirembe F. Haemoglobin status and predictors of anaemia among pregnant women in Mpigi, Uganda. BMC Res Notes. 2014;7(1):712.
8. McClure EM, Meshnick SR, Mungai P, et al. The association of parasitic infections in pregnancy and maternal and fetal anemia: a cohort study in coastal Kenya. PLoS Negl Trop Dis. 2014;8(2):e2724.
9. Taremwa IM, Ashaba S, Adrama HO, et al. Knowledge, attitude and behaviour towards the use of insecticide treated mosquito nets among pregnant women and children in rural Southwestern Uganda. BMC Public Health. 2017;17(1):794.
10. Ugwu E, Olibe A, Obi S, Ugwu A. Determinants of compliance to iron supplementation among pregnant women in Enugu, Southeastern Nigeria. Niger J Clin Pract. 2014;17(5):608–612.
11. UDHS. Uganda Bureau of Statistics (UBOS) and ICF. 2016. Uganda Demographic and Health Survey 2016. Kampala, Uganda and Rockville, Maryland, USA: UBOS and ICF; 2016.
12. Obai G, Odongo P, Wanyama R. Prevalence of anaemia and associated risk factors among pregnant women attending antenatal care in Gulu and Hoima Regional Hospitals in Uganda: A cross sectional study. BMC Pregnancy Childbirth. 2016;16(1):76.
13. Goonewardene M, Shehata M, Hamad A. Anaemia in pregnancy. Best Pract Res Clin Obstetri Gynaecol. 2012;26(1):3–24.
14. Da Costa AG, Vargas S, Clode N, Graça LM. Prevalence and risk factors for iron deficiency anemia and iron depletion during pregnancy: A prospective study. Acta Med Port. 2016;29(9):514–518.
15. Rahmati S, Delpisheh A, Parizad N, Sayehmiri K. Maternal anemia and pregnancy outcomes: A systematic review and meta-analysis. Int J Pediatr. 2016;4(8):3323–3342.
16. Ayenew F, Abere Y, Timerga G. Pregnancy anaemia prevalence and associated factors among women attending ante Natal Care in north Shoa zone, Ethiopia. Reprod Syst Sexual Disord. 2014;3(135):1–7.
17. Abdelgader EA, Diab TA, Kordofani AA, Abdalla SE. Hemoglobin level, RBCs Indices, and iron status in pregnant females in Sudan. Basic Res J Med Clin Sci. 2014;3(2):8–13.
18. Gebreweld A, Tsegaye A. Prevalence and factors associated with anemia among pregnant women attending antenatal clinic at St. Paul’s hospital millennium medical college, Addis Ababa, Ethiopia. Adv Hematol. 2018;2018.
19. Stevens GA, Finucane MM, De-Regil LM, et al. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: a systematic analysis of population-representative data. Lancet Global Health. 2013;1(1):e16–e25.
20. Likilo Osundja Jeremy AO, Agasa B, Bosunga K, Likwekwe K. Risk factors associated with anemia among pregnant women in Kisangani in D.R.Congo. Int J Recent Sci Res. International Journal of Recent Scientific Research. 2018;9(4(G)):26015–26021.
21. Zekarias B, Meleko A, Hayder A, Nigatu A, Yetagessu T. Prevalence of anemia and its associated factors among pregnant women Attending Antenatal Care (ANC) in Mizan Tepi University teaching hospital, South West Ethiopia. Health Sci J. 2017;11(5):529.
22. Acheampong K, Appiah S, Baffour-Awuah D, Arhin YS. Prevalence of anemia among pregnant women attending antenatal clinic of a selected hospital in Accra, Ghana. Int J Health Sci Res. 2018;8(1):p186–93.
23. Shitie D, Zewde T, Molla Y. Anemia and other hematological profiles of pregnant women attending antenatal care in Debre Berhan Referral Hospital, North Shoa, Ethiopia. BMC Res Notes. 2018;11(1):704.
24. Kanyesigye Hamson JN, Julius M, Emmanuel B, Ronald M. Prevalence, morphological types and factors associated with anemia among mothers attending antenatal clinic at mbarara regional referral hospital, South Western Uganda. J Health Med Nurs. 2016;25.
25. Mukaya JE, Ddungu H, Ssali F, O’Shea T, Crowther MA. Prevalence and morphological types of anaemia and hookworm infestation in the medical emergency ward, Mulago Hospital, Uganda. S Afr Med J. 2009;99(12).
26. Melku M, Addis Z, Alem M, Enawgaw B. Prevalence and predictors of maternal anemia during pregnancy in Gondar, Northwest Ethiopia: an institutional based cross-sectional study. Anemia. 2014;2014.
27. Lee M, Bozzo P, Einarson A, Koren G. Urinary tract infections in pregnancy. Can Fam Physician. 2008;54(6):853–854.
28. Jabbar -A-A. The association between anemia and urinary tract infection among the pregnant women in Baghdad. J Faculty Med. 2006;48(3):267–270.
29. Bereka S, Gudeta A, Reta M, Ayana L. Prevalence and associated risk factors of anemia among pregnant women in rural part of JigJiga City, Eastern Ethiopia: a cross sectional study. J Preg Child Health. 2017;4(337):2.
30. Yakoob MY, Bhutta ZA. Effect of routine iron supplementation with or without folic acid on anemia during pregnancy. BMC Public Health. 2011;11(3):S21.
31. Getachew M, Yewhalaw D, Tafess K, Getachew Y, Zeynudin A. Anaemia and associated risk factors among pregnant women in Gilgel Gibe dam area, Southwest Ethiopia. Parasit Vectors. 2012;5(1):296.
32. ACOG. ACOG practice bulletin: clinical management guidelines for obstetrician-gynecologists number 76, October 2006: postpartum hemorrhage. Obstet Gynecol. 2006;108(4):1039.
33. Milman N. Postpartum anemia I: definition, prevalence, causes, and consequences. Ann Hematol. 2011;90(11):1247.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.