Back to Journals » Open Access Emergency Medicine » Volume 12
Prevalence, Clinical Characteristics, and Risk Among Patients with Ischemic Heart Disease in the Young Jordanian Population
Authors Raffee LA ![]() , Alawneh KZ
, Alawneh KZ ![]() , Ibdah RK
, Ibdah RK ![]() , Rawashdeh SI
, Rawashdeh SI ![]() , Zoghoul S
, Zoghoul S ![]() , Ewais AS
, Ewais AS ![]() , Al-Mistarehi AH
, Al-Mistarehi AH
Received 29 July 2020
Accepted for publication 27 October 2020
Published 16 November 2020 Volume 2020:12 Pages 389—397
DOI https://doi.org/10.2147/OAEM.S272961
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hans-Christoph Pape
Liqaa A Raffee,1 Khaled Z Alawneh,2 Rashid K Ibdah,3 Sukaina I Rawashdeh,3 Sohaib Zoghoul,4 Abdel Salam Ewais,1 Abdel-Hameed Al-Mistarehi5
1Department of Accident and Emergency Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 2Department of Diagnostic Radiology and Nuclear Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 3Division of Cardiology, Department of Internal Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 4Medical Education Department, Hamad Medical Corporation (HMC), Doha, Qatar; 5Department of Public Health and Family Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan
Correspondence: Liqaa A Raffee Department of Accident and Emergency Medicine, Faculty of Medicine
Jordan University of Science and Technology, Irbid, Jordan
Email [email protected]
Purpose: This study aims to evaluate the prevalence of ischemic heart disease (IHD) among the young population in Jordan. We examined the risk factors that might be involved in disease incidence. Clinical characteristics, patients’ living standards, and various other risk factors were considered to conduct the study.
Methods: A retrospective study was conducted at King Abdullah University Hospital. Data were collected from patients who visited this hospital between January 2013 and December 2017. Only young Jordanian adults of age < 50 years were included in this study. The data of 358 patients were purposively collected and analyzed (as per the determined inclusion criteria), where information related to their baseline characteristics, clinical characteristics, and related biochemical assays was reviewed.
Results: This study showed a high prevalence of IHD among young males in Jordan. It also revealed that increased age, smoking, hypertension, unfavorable lipid profile, and obesity were the major possible risk factors for the occurrence of disease. These patients were initially diagnosed with either unstable angina or acute myocardial infarction. Initial WBCs count, particularly monocytes differential, was high in about one-third of patients, besides cardiac biomarkers.
Conclusion: The high incidence of IHD was noticed among young individuals. We suggest that more efforts should be instigated for reducing the high prevalence of IHD by adopting a healthy lifestyle, preventive attitude, and nutritious food intake.
Keywords: family history, ischemic heart disease, myocardial infarction, risk factors, young, Jordan
Introduction
Globally, there is an increase in the occurrence of coronary artery disease (CAD),1 which is also a major cause of mortality.2 The burden of cardiovascular disease is a significant public concern.3 According to Nowbar et al4 ischemic heart disease (IHD) is the prime cause of death as it caused around 9 million deaths in 2016.5 A report issued by the American Heart Association mentioned that approximately 17.9 million people die from heart disease that represents 31% of the total deaths in the Western countries.6 Among these, 6.7 million deaths are due to stroke; while 7.4 million deaths are because of IHD. It is expected that the prevalence of IHD will spike up to 43.9% by 2030.6 The factors leading to the development of IHD include; high blood pressure, a family history of coronary heart disease, physical inactivity, economic transition, sociodemographic, poor nutrition, and diabetes.7 Various pieces of research have observed the increased prevalence of IHD and risk factors among patients suffering from cardiovascular diseases.8–10 The major causes of cardiovascular disease are smoking, reperfusion therapy, and left ventricular ejection fraction.3
The Institute for Health Metrics and Evaluation (IHME)11 stated that the prevalence of IHD in Jordan accounts for 54.7 of the annual deaths. Eshah12 has reported a substantial lacking public awareness about IHD lead towards increased IHD related mortality. One of the previous studies has shown that it is possible to modify and reduce the IHD related risk factors and enable people to pursue quality life.13 However, there is an upward trend observed concerning the high prevalence of IHD among the young population. A study revealed that 6% of the overall hospital population were aged less than 50 years, which was comparatively lower than adults.14 Moreover, the re-admissions of these patients are substantially more as compared with patients aged above 50 years.14 Leifheit-Limson et al15 documented that 93% of all the IHD patients possess high-risk factors as compared to others. Also, the previous researches indicate risk factors for IHD are also the major stimulator for behavior change among such patients.16–18 Barbero19 emphasizes that there is an increase in IHD prevalence among younger patients having different coronary artery anomalies.
The analysis of its risk factors, prevalence, and outcomes remains an understudied area. The prevalence of the disease varies in each population because of their lifestyle change. The prevalence of IHD among young adults in Jordan is a widely studied area. Further, statistical yearbook20 highlighted that Jordan’s population at present constitutes 86.74% of the young adults. Hence, considering the increase in the young adult population and continual episodes of IHD, it is integral to determine the IHD risk factors among young adults. The findings are likely to assist in mitigating the prevalence of IHD among the young population, identifying the clinical characteristics as well as the IHD manifestation among the young adults. However various studies have been conducted to identify the IHD prevalence, the findings are expected to assist in establishing a medical precautionary foundation for disease detection at various phases as well as presentation. Conclusively, it will help in reducing the morbidity and mortality rate and will advance the health prospects of the young adults in Jordan.
Materials and Methods
Study Design
A descriptive, retrospective study design, along with a quantitative approach was used. The reason for selecting this study design is based on its relevance to the study nature, and its efficacy to draw conclusive findings. Accordingly, the research design has been employed in previous studies and is deemed appropriate for concluding effective findings.21 Though, these studies differ from the present one based on their study scope, population, and sample.
Study Population and Sample
The study population constitutes of the medical records of young ischemic heart patients who visited King Abdullah University Hospital from 1st January 2013 to 31st December 2017. A total of 358 patients were recruited to conduct the current study. All the details from their medical records were collected. Inclusion criteria: Medical records of all the patients of confirmed ischemic heart disease who visited cardiology and emergency departments of KAUH were thoroughly studied. Among these, only Jordanian patients with age <50 years were selected for the study. Informed consent was obtained from each patient participated in this study.
Data Collection
This study was approved by the Institutional Review Board (IRB) of Jordan University of Science and Technology and King Abdullah University Hospital before conducting data collection. The medical records of the patients were reviewed for collecting the relevant data with specific consideration on the prevalence of IHD, its clinical characteristics along with the associated risk factors among young patients. After it, a follow-up using a questionnaire was held for identifying the risk factors other than those that were recorded. This follow-up was held via phone for the confirmed IHD patients. The information collected includes symptoms and signs, past cardiovascular history, and risk factors (hypertension, cigarette smoking, diabetes mellitus, and family history). The other details noted include the LDL (Low-density lipoprotein), HDL (High-density lipoprotein), triglycerides, total serum cholesterol, body mass index (BMI), random blood glucose. The initial changes in ECG (electrocardiogram) were also recorded in these patients. The cut-off values for all the biochemical data in this study have been illustrated in Table 1.
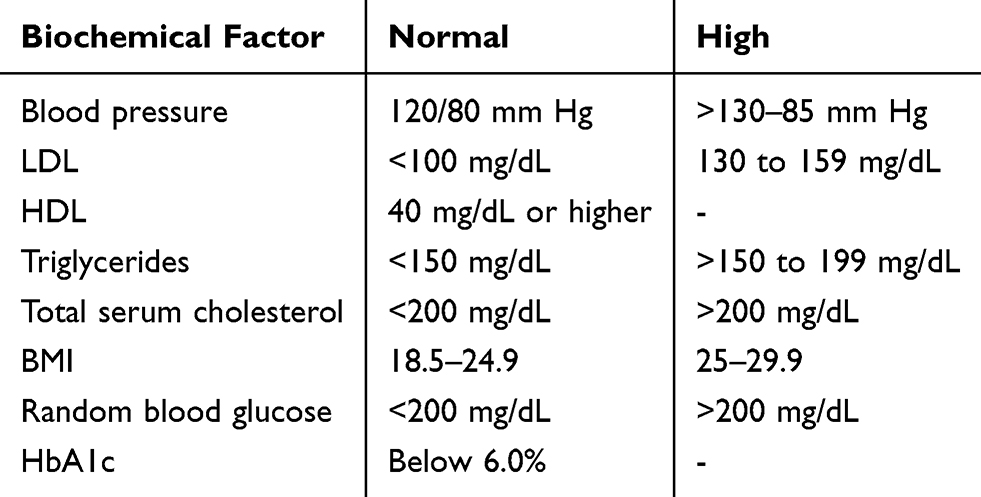 |
Table 1 Cut-off Values of Biochemical Factors |
Data Analysis
IBM SPSS (Statistical Package for Social Sciences) Version 23.0 was used to analyze the collected data. Mean, and the standard deviation was computed for the continuous variables, whereas frequency was used for computing the qualitative data. The statistical significance of the p-value was determined as <0.05.
Results
Table 2 indicates the demographic details of the participants. The findings of this study indicated that most of the respondents (91.3%) were males, while a few (8.7%) of them were females. Most of the participants belonged to the age group from 36 to 47 years, in which 44.7% were 36 to 41 years old while 40% belonged to the age group, 42 to 49 years. Only 3% of the patients had <30 years of age.
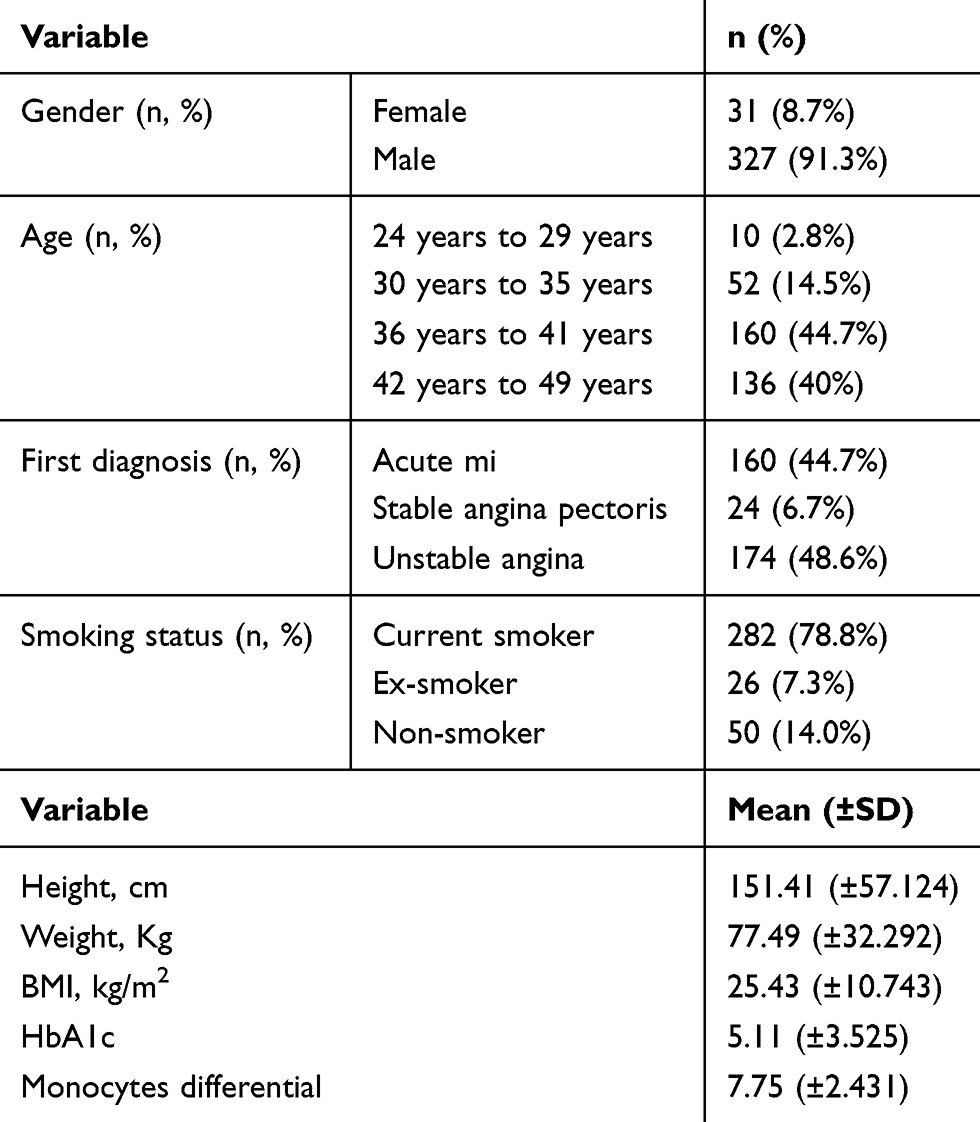 |
Table 2 Demographic Details |
The initial diagnosis of the participants indicated that 174 participants had unstable angina. Besides, 160 were suffering from acute myocardial infarction (MI) and 24 participants had stable angina pectoris. The smoking status of these patients was also identified. Findings indicated that 282 (78.8%) participants were current smokers, 50 (14.0%) of them were nonsmokers while the remaining 26 (7.3%) participants fall into the category of ex-smoker.
Table 2 also indicates the findings regarding the mean values of each patient’s height, weight, BMI, HbAlc, and differential monocytes. The average height of the participants was 151.41±57 cm, and the average weight of these participants was 77.49±32.292 Kg. On the estimation of the Basal Metabolic Index (BMI), we found that most of the IHD patients had higher BMI than normal. The mean value of BMI is indicated as 25.43±10.743. Estimation of HbA1c was also done to observe if diabetic or pre-diabetic individuals are at higher risk for the onset of ischemic heart disease. Findings revealed the mean value of HbA1c is 5.11±3.52. Also, an increase in monocytes was noted in the differential CBC in positive cardiac catheterization (Cath) patients in comparison to the control group with normal Cath, the mean of which was found to be 7.75±2.43.
Table 3 highlights the effects of gender discrimination on clinical characteristics, associated risk factors of IHD, and the effects of beta-blockers on the prevalence of the disease. The records showed that white blood cells (WBC) count was normal among most of the patients (68.2% in males, and 60% in females). However, 31.8% of males and 36.7% of females had high WBC count which indicates that these patients are at higher risk of IHD and mortality. Platelets count among the male and female patients was found normal ie 88.6% and 83.3% respectively. Few patients, including males and females (8.0% and 13.3%) had slightly higher platelet count while its difference between males and females was insignificant (p=0.630).
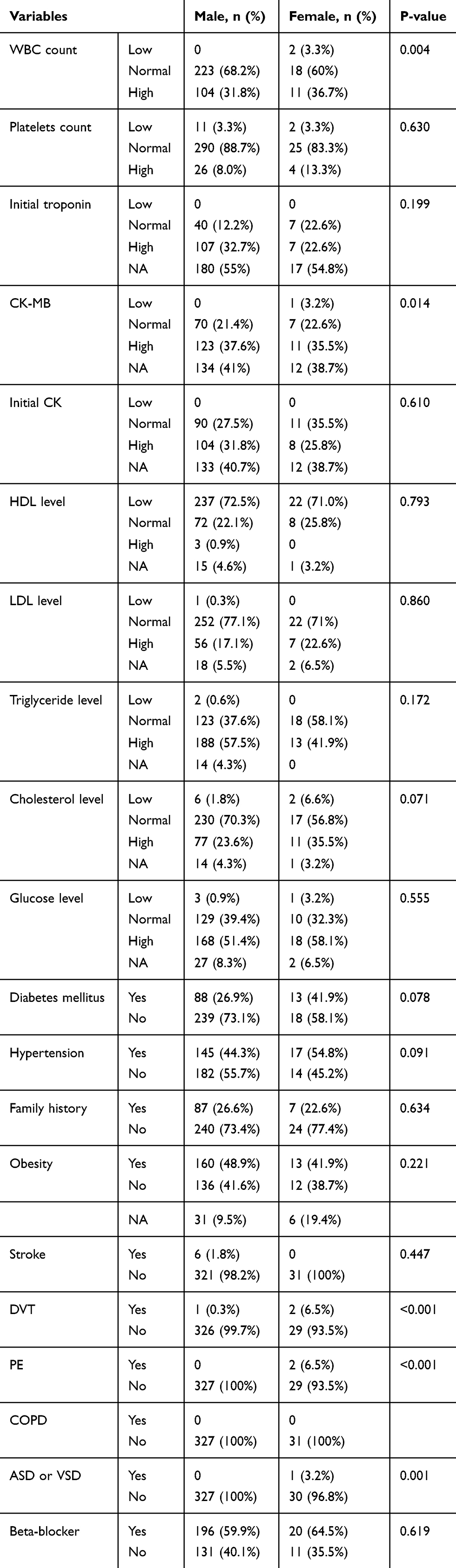 |
Table 3 Gender Effects on Biochemical Factors, Associated Risk Factors and Beta-Blocker Intake in Patients with IHD |
The initial troponin levels were higher among most of the males than females (32.7% in males and 22.6% in females) which indicates that the majority of the males had experienced a heart attack. However, troponin data of many participants was not available.
The creatine kinase (CK-MB) among the Jordanian population is found higher among both males (37.6%) and females (35.5%). It shares a high association with IHD cases (p-value 0.014) and confirms the troponin findings. Also, the records showed that initial CK was high among males (31.8%) than females (25.8%). However, 27.5% of males and 35.5% of females had normal levels of initial CK. We also check the lipid profile of our participants; and found that most of the patients, including males and females (72.5% and 71.0%) had lower levels of HDL and few of them had normal HDL levels. Unlike HDL, LDL levels were found normal among both males and females (77.1% and 71%). Triglycerides (TG) levels were found high in males (57.5%) than females (41.9%). Interestingly, approximately one-third of females (35.5%) had elevated levels of cholesterol as compared to males (23.6%). However, the remaining IHD patients had normal or low cholesterol levels. We also investigated if these patients had other related comorbidities that might worsen conditions related to IHD. We found that majority of the females (41.9%) were already suffering from diabetes mellitus and their number was higher than males (26.9%). Prevalence rates of hypertension were significantly higher in females (54.8%) than males (44.3%). If compared regardless the gender, approximately half of the patients (males and females) had hypertension. The family history of these patients revealed that neither males nor females (73.4%, 77.4%) had a family history of IHD. Obesity can be the major factor that is involved in the prevalence of this disease, as 48.9% of males and 41.9% of females with IHD were obese. We also found that almost none of the males and females (98.2%, 100%) had experienced a stroke.
We also investigated the patients if they had deep vein thrombosis (DVT), Pulmonary embolism (PE), chronic obstructive pulmonary disease (COPD), atrial septal defect (ASD), or ventricular septal defect (VSD) at any time in their life. Results reveal that most of the patients, including males and females, did not have any of these diseases. However, few of the females (3.2%) had septum defects and their values were significantly (0.001) higher than males.
We evaluated the intake of beta-blockers by these IHD patients and found that 59.9% of males and 64.5% of females consume beta-blockers to manage their diseased condition. However, the remaining 40.1% males and 35.5% females used other drugs like calcium channel blocker, PI (Protease inhibitor), Angiotensin Receptor Blocker (ARBs), Angiotensin Converting Enzyme (ACE) inhibitors to manage their ailment.
We evaluated all the above-mentioned factors based on the smoking status of these patients and the results are mention in Table 4. We found that WBC count was significantly (0.007) higher in smokers (33%) than ex-smokers (23.1%) and non-smokers (30.0%). Platelet count was found normal among the majority of the patients with no significant differences among different categories of smoking status. Initial Troponin levels were found higher among current smokers (33.3%) and ex-smokers (28.9%) than non-smokers (26%) without significant difference (p=0.266). Initial CK-MB levels were also found higher among current smokers and ex-smokers (39%, and 34.6%) than non-smokers (30%). Initial CK was raised in 32.6%, and 34.6% of current smokers and ex-smokers than non-smokers (22%).
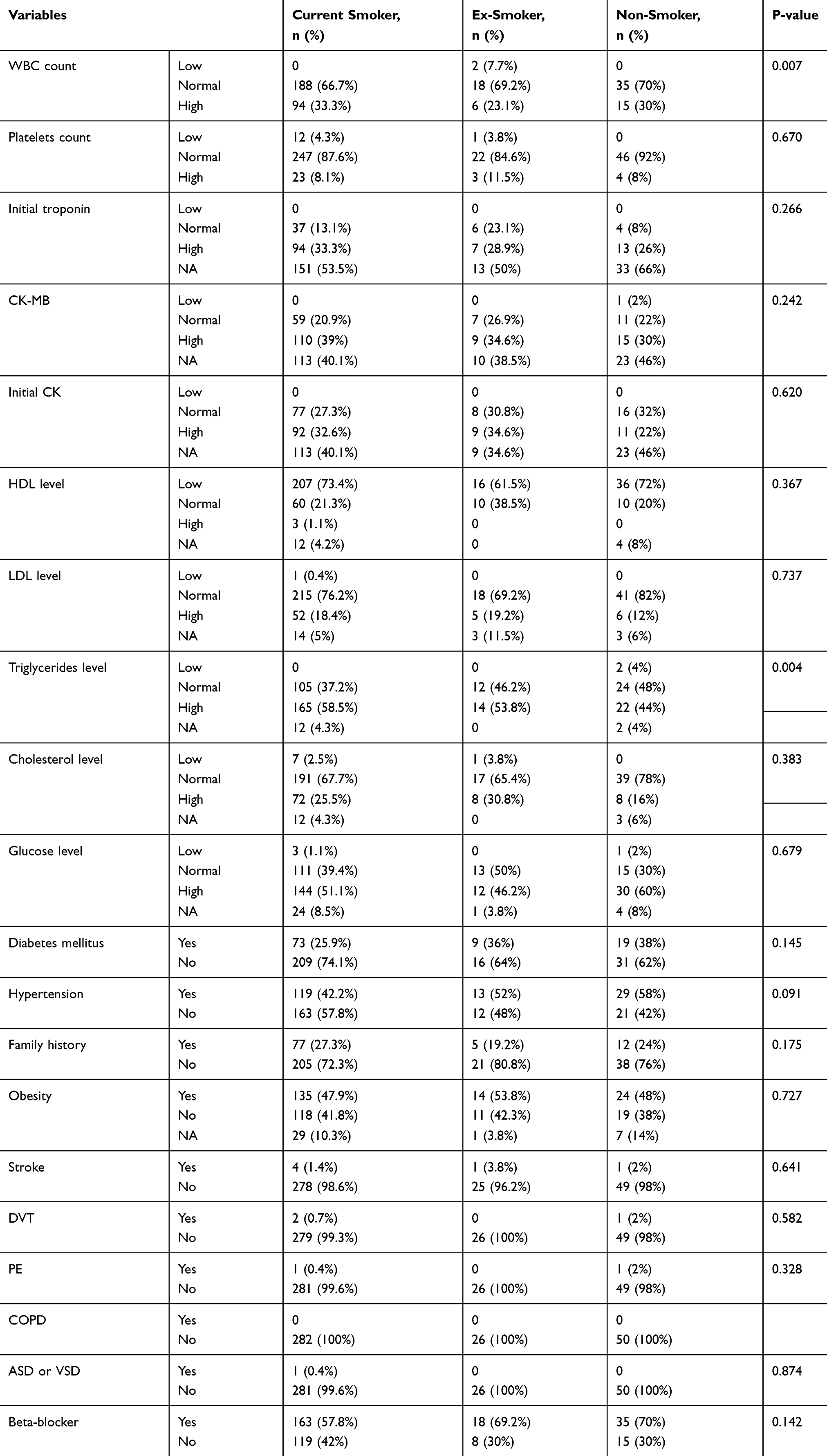 |
Table 4 Effects of Smoking on Biochemical Factors, Associated Risk Factors and Beta-Blocker Intake in Patients with IHD |
Lipid profile analysis of these patients showed that there were no significant effects of smoking on serum HDL levels. However, LDL levels were higher in current smokers and ex-smokers (18.4% and 19.2%) than non-smokers (12%). Serum triglyceride (TG) levels were significantly (p=0.004) affected by smoking. TG levels were found 58.5% higher among current smokers and 53.8% in ex-smokers than non-smokers 44%. Total Cholesterol levels were also found elevated in current smokers and ex-smokers (25.5% and 30.8%) compared to non-smokers (16%) without significant differences (p=0.383). There were no significant effects of smoking on glucose levels and patients’ diabetic or hypertensive status. There was no impact of smoking on the family history of IHD among these patients. Smoking also did not affect obesity, stroke, DVT, COPD, ASD, and VSD. On the evaluation of beta-blocker intake, we found that non-smokers (70%) consume it more than current smokers and ex-smokers (57.8% and 69.2%).
Discussion
This retrospective analysis showed that the prevalence of IHD was majorly in males and at an increasing age. The initial diagnosis revealed unstable angina or acute MI among patients. It showed that IHD and its relevant complications were higher among patients who currently smoke as compared to the ex-smokers or non-smokers. Also, the clinical diagnosis showed that the WBC count of the patients was normal among males and females however it was higher among smokers compared to the ex-smokers and non-smokers.
The platelet count was normal among most of the patients and had not been affected by the smoking status of these individuals. We observed that serum levels of troponin, CK-MB, and initial CK were not affected by smoking status, while initial CK levels were significantly increased in males than in females. Our findings showed that males were at higher risk of IHD and smoking increased the chances of IHD, and its related complications. Abnormal HDL levels, hypertriglyceridemia, hypertension, high glucose levels, and obesity were possible risk factors among the young Jordanian population for IHD. This is in contrast with the results found in another study conducted in Jordan which found hypercholesterolemia as the major risk factor.22 The noted high prevalence of IHD is consistent with the earlier Jordanian studies, where increased cardiac-related risk is documented.12,23 The increase in the IHD risk might also account for environmental and psychological circumstances in Jordan. EUGenMed et al24 had also stated that the prevalence of IHD varies among gender, which is similar to the reporting of the present study. Such as the study explains that the difference may be due to the sociocultural processes and behavior, along with their specific environmental exposure and a different attitude towards prevention and treatments.24
Similarly, male gender and older age were revealed as the significant predictors in IHD, which is corroborated by recent studies.24–26 The increasing use of beta-blockers was high among the current study population, which was found to be effective for IHD patients, and is found consistent with the earlier research of Hwa et al.27 The current study also found that IHD increases with the increase in the number of monocytes. This is consistent with the findings of Madjid and Fatemi,28 which found an increased heart disease risk in patients with high monocyte counts. The prevalence and high risk of IHD among the young patients in the region may also account for the resource availability, health-care oriented behavior, and inadequate attention of the healthcare. The Jordanian research of Eshah et al29 also emphasizes that healthcare providers must improve and prioritize cardiac treatment and must establish its importance, healthy behavior, and early treatment among the patients to reduce the mortality rate and improve patient’s quality of life.
The findings of the study recommend that different interventions should be instigated for controlling the risk factor and reducing the high prevalence of IHD among the young Jordanian population. Yandrapalli et al reported some of the modifiable risk factors in young adults that are also mentioned in this study.30 Our study confirms that these risk factors were consistent in the Jordanian population. They could also be modified using the same strategy. It could begin at a clinical level, where patients can be exposed to different content and practices for controlling the risk factors as per the state of the patient. Such as targeted interventions could be introduced by the behavioral change of the patient and by the setting of the realist goals. For instance, behavioral changes for smoking, healthy eating, and exercise could be used as interventional strategies.
This study has certain limitations, which include its retrospective study design, the inclusion of the young population as study participants with a comparable control group, non-randomized collection of data was restricted to Jordan only. The study fails to address the patients presented with normal coronary angiography. Moreover, the outcome of the high prevalence of IHD among the young Jordanian population has not been explained in this study. Therefore, future studies are required to address these limitations. Future studies can adopt the same objective while using a different study design and study population to improve the research scope and significance.
Conclusion
IHD has a major prevalence among the young Jordanian population. This study shows that IHD was high among males, and people with increasing age, hypertension, smoking, unfavorable lipid profile, and obesity. The increased intake of beta-blockers was also found among patients for prevention against IHD. Initial WBCs count, particularly monocytes differential, was high in about one-third of patients, besides cardiac biomarkers. This study showed that young adults were at a high risk of IHD, where prevention measures are necessary. Additionally, consideration of the environment, as well as psychological circumstances is also important for enhancing the prevention and treatment outcomes. Finally, the study recommends the use of various effective interventional strategies along with primary preventive practices against IHD and effective disease screening to improve the quality of life among young patients with IHD.
Data Sharing Statement
The datasets generated and analyzed during the current study are available with the corresponding author.
Compliance with Ethical Standards
All procedures performed in this study involving human participants were reviewed and ethically approved by the Institutional Review Board (IRB) of Jordan University of Science and Technology and King Abdullah University Hospital. This study was conducted following the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study on phone.
Acknowledgments
The author is very thankful to all the associated personnel in any reference that contributed in/for the purpose of this research.
Funding
There is no Funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Benjamin EJ, Virani SS, Callaway CW. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. 2018;137:67–492.
2. Choi AR, Jeong MH, Hong YJ. Clinical characteristics and outcomes in acute myocardial infarction patients with versus without any cardiovascular risk factors. Korean J Intern Med. 2019;34:1040. doi:10.3904/kjim.2018.056
3. Liu Y, Han T, Gao M, et al. Clinical characteristics and prognosis of acute myocardial infarction in young smokers and non-smokers (≤ 45 years): a systematic review and meta-analysis. Oncotarget. 2017;8:81195. doi:10.18632/oncotarget.21092
4. Nowbar AN, Gitto M, Howard JP, et al. Mortality from ischemic heart disease: analysis of data from the world health organization and coronary artery disease risk factors from NCD risk factor collaboration. Circ Cardiovasc Qual Outcomes. 2019;12:e005375. doi:10.1161/circoutcomes.118.005375
5. Global Health Estimates. 2016: deaths by cause, age, sex, by country and by region, 2000–2016. Geneva, Switzerland: World Health Organization; 2018. Available from: http://www.who.int/healthinfo/global_burden_disease/estimates/en/.
6. Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart disease and stroke statistics—2017 update. 2017
7. Hata J, Nagai A, Hirata M, et al. Risk prediction models for mortality in patients with cardiovascular disease: the BioBank Japan project. J Epidemiol. 2017;27:71–76. doi:10.1016/j.je.2016.10.007
8. Masana L, Ros E, Sudano I, et al. Is there a role for lifestyle changes in cardiovascular prevention? What, when, and how? Atheroscler Suppl. 2017;26:2–15. doi:10.1016/s1567-5688(17)30020-x
9. Micha R, Peñalvo JL, Cudhea F, et al. Association between dietary factors and mortality from heart disease, stroke, and type 2 diabetes in the United States. JAMA. 2017;317:912–924. doi:10.1001/jama.2017.0947
10. Wolever RQ, Webber DM, Meunier JP, et al. Modifiable disease risk, readiness to change and psychosocial functioning improve with integrative medicine immersion model. Altern Ther Health Med. 2011;17:38.
11. IHME. What causes the most deaths? 2017. Available from: http://www.healthdata.org/jordan.
12. Eshah NF. Ischemic heart diseases: the unrecognized killer in the Jordanian community. J Behav Health. 2014;3:58–64. doi:10.5455/jbh.20131226115903
13. Chiou AF, Hsu SP, Hung HF. Predictors of health-promoting behaviors in Taiwanese patients with coronary artery disease. Appl Nurs Res. 2016;30:1–6. doi:10.1016/j.apnr.2015.08.008
14. Andrés E, Cordero A, Magán P, et al. Mortalidad a largo plazo y reingreso hospitalario tras infarto agudo de miocardio: un estudio de seguimiento de ocho años. Rev Esp Cardiol. 2012;65:414–420. doi:10.1016/j.recesp.2011.09.009
15. Leifheit-Limson EC, Spertus JA, Reid KJ, et al. Prevalence of traditional cardiac risk factors and secondary prevention among patients hospitalized for acute myocardial infarction (AMI): variation by age, sex, and race. J Womens Health. 2013;22:659–666. doi:10.1089/jwh.2012.3962
16. Larson N, Chen Y, Wall M, et al. Personal, behavioral, and environmental predictors of healthy weight maintenance during the transition to adulthood. Prev Med. 2018;113:80–90. doi:10.1016/j.ypmed.2018.04.027
17. Morris AA, Ko YA, Hutcheson SH, et al. Race/ethnic and sex differences in the association of atherosclerotic cardiovascular disease risk and healthy lifestyle behaviors. J Am Heart Assoc. 2018;7:8250. doi:10.1161/jaha.117.008250
18. Noureddine S, Massouh A. Factors associated with continued smoking in lebanese patients with acute coronary syndrome. J Cardiovasc Nurs. 2019;34:94–98. doi:10.1097/jcn.0000000000000514
19. Barbero U, Scacciatella P, Iannaccone M, et al. Culprit plaque characteristics in younger versus older patients with acute coronary syndromes: an optical coherence tomography study from the FORMIDABLE registry. Catheter Cardiovasc Interv. 2018;92:1–8. doi:10.1002/ccd.27172
20. Statistical Yearbook. Table 2.5 estimated population of the kingdom by sex and age group, at end-year 2012. Department of statistics. 2012. Available from: http://www.dos.gov.jo/dos_home_e/main/Demograghy/2012/2-5.pdf.
21. Wang X, Gao M, Zhou S, et al. Trend in young coronary artery disease in China from 2010 to 2014: a retrospective study of young patients ≤ 45. BMC Cardiovasc Disord. 2017;17:18. doi:10.1186/s12872-016-0458-1
22. Jarrah MI, Alrabadi N, Alzoubi KH. Applying DESyne coronary stent system in patients with ischemic heart disease: experience from Jordan. Med Devices. 2018;11:405.
23. Haddad NE, Saleh MN, Eshah NF. Cardiac catheterisation and patients’ anxiety levels. Br J Card Nurs. 2017;12:353–358. doi:10.12968/bjca.2017.12.7.353
24. Regitz-Zagrosek V, Oertelt-Prigione S, Prescott E; EUGenMed, Cardiovascular Clinical Study Group, et al. Gender in cardiovascular diseases: impact on clinical manifestations, management, and outcomes. Eur Heart J. 2015;37:24–34. doi:10.1093/eurheartj/ehv598
25. Aggarwal A, Srivastava S, Velmurugan M. Newer perspectives of coronary artery disease in young. World J Cardiol. 2016;8:728. doi:10.4330/wjc.v8.i12.728
26. Raffee LA, Alawneh KZ, Al Suleiman MK, Ibdah RK, Rawashdeh SI, Al-Mistarehi A-HW. An observational study of the occurrence of acute coronary syndrome (ACS) among jordanian patients: identifying the influence of Ramadan Fasting. Ann Med Surg. 2020;59:171–175. doi:10.1016/j.amsu.2020.09.042
27. Hwa YL, Shi Q, Kumar SK, et al. Beta-blockers improve survival outcomes in patients with multiple myeloma: a retrospective evaluation. Am J Hematol. 2017;92:50–55. doi:10.1002/ajh.24582
28. Madjid M, Fatemi O. Components of the complete blood count as risk predictors for coronary heart disease: in-depth review and update. Tex Heart Inst J. 2013;40:17.
29. Eshah NF. Readiness for behavior change in patients living with ischemic heart disease. J Nurs Res. 2019;27:57. doi:10.1097/jnr.0000000000000336
30. Yandrapalli S, Nabors C, Goyal A, et al. Modifiable risk factors in young adults with first myocardial Infarction. J Am Coll Cardiol. 2019;73;573–584.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.