Back to Journals » Research and Reports in Tropical Medicine » Volume 11
Prevalence and Predictors of CD4+ T-Lymphocytopenia Among HIV-Negative Tuberculosis Patients in Uganda
Authors Baluku JB ![]() , Musaazi J, Mulwana R, Mugabo AR, Bongomin F, Katagira W
, Musaazi J, Mulwana R, Mugabo AR, Bongomin F, Katagira W ![]()
Received 5 March 2020
Accepted for publication 15 June 2020
Published 25 June 2020 Volume 2020:11 Pages 45—51
DOI https://doi.org/10.2147/RRTM.S252550
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mario Rodríguez-Pérez
Joseph Baruch Baluku,1– 3 Joseph Musaazi,4 Rose Mulwana,1 Araali Robert Mugabo,1 Felix Bongomin,5 Winceslaus Katagira3
1Mulago National Referral Hospital, Pulmonology Division, Kampala, Uganda; 2Mildmay Uganda, Kampala, Uganda; 3Makerere University Lung Institute, Kampala, Uganda; 4Makerere University Infectious Disease Institute, Kampala, Uganda; 5Department of Medical Microbiology & Immunology, Faculty of Medicine, Gulu University, Gulu, Uganda
Correspondence: Joseph Baruch Baluku
Mulago National Referral Hospital, Pulmonology Division, P.O. Box 7051, Kampala, Uganda
Tel +256706327972
Email [email protected]
Purpose: CD4+ T-lymphocytopenia is a risk for tuberculosis (TB) infection, reactivation and severe disease. We sought to determine the prevalence and predictors of CD4 T-lymphocytopenia among HIV-negative patients with bacteriologically confirmed TB in Uganda.
Patients and Methods: Eligible participants were adult HIV-negative patients with bacteriologically confirmed TB at the National TB Treatment Centre in Uganda. CD4+ and CD8+ T-lymphocyte counts were determined by flow cytometry. We defined CD4+ T-lymphocytopenia as a CD4+ T-lymphocyte count of < 418 cells/mm3 as per the population estimate for Ugandans. We performed logistic regression analysis to determine predictors of CD4+ T-lymphocytopenia.
Results: We enrolled 216 participants whose mean age (standard deviation (±SD)) was 32.5 (± 12.1) years, of whom 146 (67.6%) were males. The prevalence of CD4+ T-lymphocytopenia was 25% (54/216) (95% confidence interval (CI): 19.6– 31.2%). Patients with anaemia (adjusted odds ratio (aOR): 3.83, 95% CI: 1.59– 9.23, p = 0.003), weight loss (aOR: 3.61, 95% CI: 1.07– 12.23, p = 0.039) and a low CD8+ T-cell count (aOR: 6.10, 95% CI: 2.68– 13.89, p < 0.001) were more likely to have CD4+ T-lymphocytopenia while those with monocytosis (aOR: 0.35, 95% CI: 0.14– 0.89, p = 0.028) were less likely to have CD4+ T-lymphocytopenia.
Conclusion: There was a high prevalence of CD4+ T-lymphocytopenia among HIV-negative TB patients. Patients with weight loss, anaemia and a low CD8+ count were more likely to have CD4+ T-lymphocytopenia while those with monocytosis were less likely to have CD4+ lymphocytopenia. The findings suggest that CD4+ lymphocytopenia is indicative of severe disease and globally impaired cell-mediated immune responses against TB.
Keywords: HIV negative, tuberculosis, CD4+, CD8+, lymphoctyopenia, monocytosis, weight loss, anaemia
Plain Language Summary
CD4+ T-cells are a crucial component of the immune response against tuberculosis (TB). Individuals with low CD4+ T-cell counts are at risk of TB infection and more likely to have severe forms of TB. We determined the prevalence and predictors of low CD4+ T-cell counts among HIV-negative TB patients at a national TB treatment centre in Uganda. We found that a quarter of HIV-negative TB patients in this setting have a low CD4+ T-cell count (less than 418 cells per mm3). Patients with anaemia, weight loss, and low CD8+ T-cell counts were more likely to have low CD4+ T-cell counts while those with high monocyte counts were less likely to have low CD4+ T-cell counts. The results indicate that HIV-negative TB patients with low CD4+ T-cell counts also have impairment in the function of other cells of the immune system and severe TB disease.
Background
Globally, tuberculosis (TB) contributed 1.2 million deaths among HIV-negative individuals in 2018.1 The control of TB infection depends on intact innate and adaptive immune responses that are mainly effected by monocytes (as macrophages) and cluster of differentiation (CD) 4+ T-lymphocytes, respectively.2 CD4+ T-lymphocytes produce interferon gamma (IFNɣ) that contributes to the recruitment and activation of innate immune cells that ultimately clear TB infection by phagocytosis and autophagy.3,4 IFNɣ derived from CD4+ T-lymphocytes is particularly important for the control of mycobacterial burden, abating intracellular multiplication of Mycobacterium tuberculosis (Mtb), preventing dissemination from pulmonary infection and promoting long-term survival of the infected host.5,6
Among HIV-positive individuals, it has been unequivocally demonstrated that CD4+ T-lymphocytopenia increases the risk for TB infection and mortality among TB/HIV co-infected individuals.7,8 Although lower CD4+ T-lymphocyte counts are reported among HIV-negative TB patients than controls, the prevalence and predictors of the CD4+ T-lymphocytopenia are not well characterised.9,10 The few studies that have evaluated the prevalence of CD4+ T-lymphocytopenia among HIV-negative TB patients report it to be 14.4–83%.11–14 However, these studies are limited by the heterogeneity of the study population whereby participants without bacteriological confirmation of TB were included. Further, predictors of CD4+ T-lymphocytopenia among HIV-negative TB patients are not widely reported. We aimed to determine the prevalence and predictors of CD4+ T-lymphocytopenia among HIV-negative bacteriologically confirmed TB patients at a national tuberculosis treatment centre in Uganda.
Patients and Methods
Study Measurements
We analysed data from a cross-sectional study that enrolled adult bacteriologically confirmed TB patients at the National Tuberculosis Treatment Centre (NTTC) in Uganda between August 2017 and March 2018.15 Demographic data, clinical symptoms and signs, full hemogram parameters, CD4+ and CD8+ T-lymphocyte counts were extracted from the master dataset. A full description of methods employed in determination of these variables is provided elsewhere.15 CD4+ and CD8+ T-lymphocyte counts were determined by flow cytometry using a flow cytometer (BD FACSCalibur™). We defined CD4+ T-lymphocytopenia as a CD4+ count of <418 cells/mm3 considering a normal range estimate of 418–2105 cells/mm3 for Ugandans.16 Full hemogram parameters were determined by a hemoanalyser (Sysmex® Automated haematology analyser XN series – XN 1000) at Mulago Hospital Haematology laboratory. The HIV status was determined by immunochromatographic rapid tests according to the Uganda national HIV testing guidelines.17
Study Setting and Population
The NTTC is a unit of Mulago National Referral Hospital and is a tertiary referral centre for diagnosis and treatment of drug susceptible and drug resistant TB. The centre is located in Kampala city, the capital city of Uganda, and treats 25% of the country’s TB cases. In this analysis, we included bacteriologically confirmed adult (≥18 years) TB patients who were HIV negative and had a CD4+ T-lymphocyte count result. There were no exclusion criteria. In the primary study, participants were consecutively sampled from the outpatient and inpatient facilities of the NTTC until the desired sample size was obtained.15
Statistical Analysis and Sample Size Estimation
Considering a prevalence of CD4+ T-lymphocytopenia of 14.4%13 reported in Senegal, a sample size of at least 211 is sufficient to determine the prevalence of CD4+ T-lymphocytopenia at the 95% confidence interval (CI) and a possible 10% occurrence of missing data. Data were analysed using STATA 15.1 (StataCorp, College Station, TX, USA). Categorical data were summarised as frequencies and percentages while continuous variables were summarised as means with the corresponding standard deviations (SD). The prevalence of CD4+ T-lymphocytopenia was calculated as a proportion of participants with a CD4+ count of <418 cells/mm3 to the total number of study participants. To determine factors that are independently associated with CD4+ T-lymphocytopenia, we performed bi-variable logistic regression analysis and fitted factors that had a p≤ 0.2 into a multivariable logistic regression model. A p ≤ 0.05 was considered statistically significant considering a 95% CI. Missing data on monocyte counts were imputed using multiple imputations with chained equations (MICE) using age, gender and platelet count, with 30 imputations. Since modelling involved haematological parameters, multi-collinearity would be expected. Prior to fitting statistical models, we checked for multi-collinearity between covariates to determine if there existed substantial correlation (Pearson’s correlation coefficient > 0.3). The haematocrit, mean corpuscular haemoglobin (MCH), and red cell count were highly correlated with the haemoglobin level and adding them in the adjusted model induced multi-collinearity. Thus, these were dropped from the final model in favour of the haemoglobin level.
Ethical Approvals and Consent to Participate
Study participants provided written informed consent prior to study enrolment. The study was approved by the School of Medicine Research and Ethics Committee of Makerere University College of Health Sciences (REC REF 2017–087).
Results
The analysis was performed on 216 HIV-negative adult patients with bacteriologically confirmed TB.
Baseline Characteristics of Study Participants
The mean age (±SD) of the study participants was 32.54 (±12.08) years and 146 (67.6%) were males. Other baseline characteristics are shown in Table 1. The frequencies of the parameters of the full hemogram, CD8+ and CD4/CD8 ratio of the study participants are shown in Table 2.
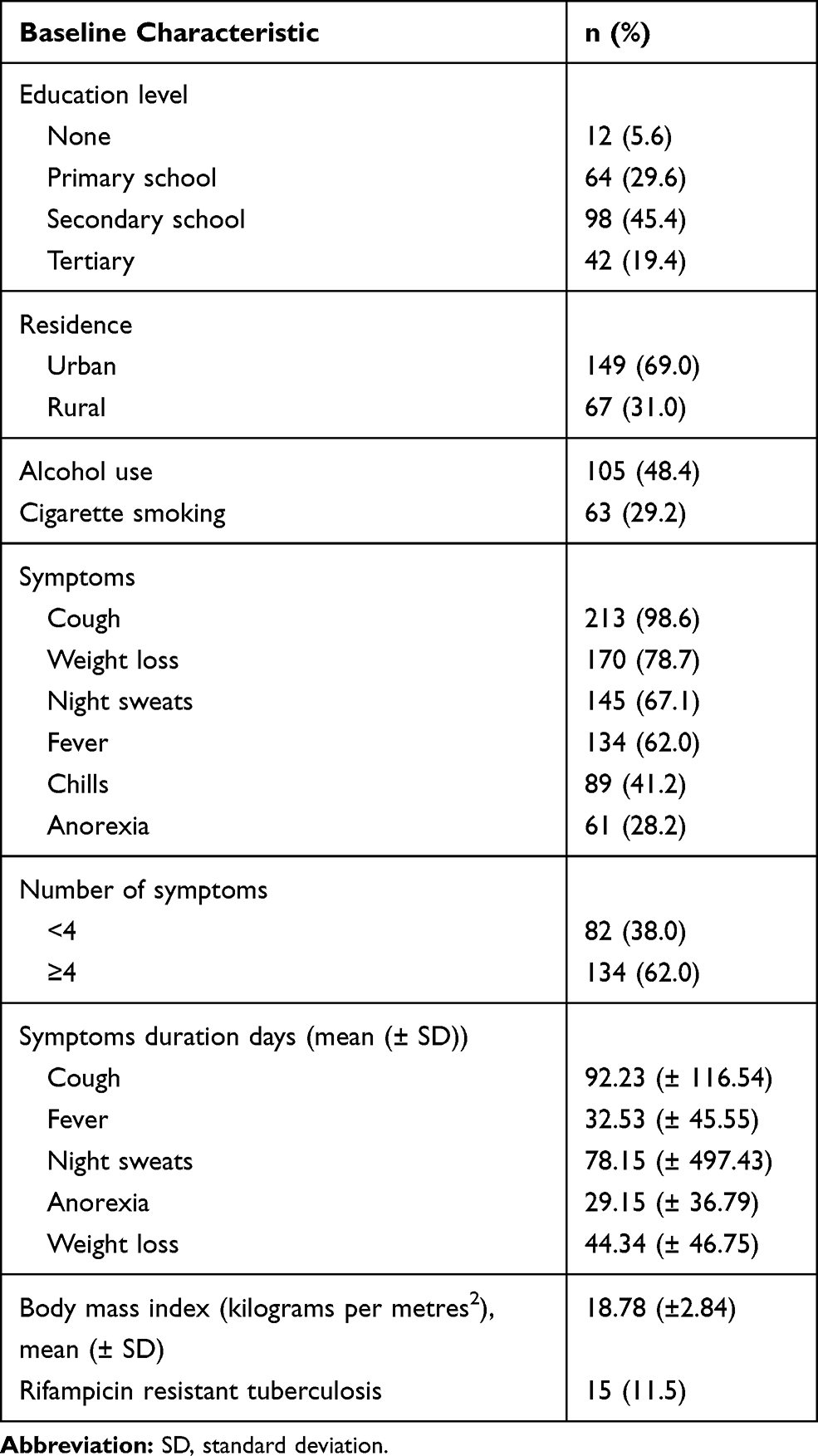 |
Table 1 Baseline Characteristics of Study Participants |
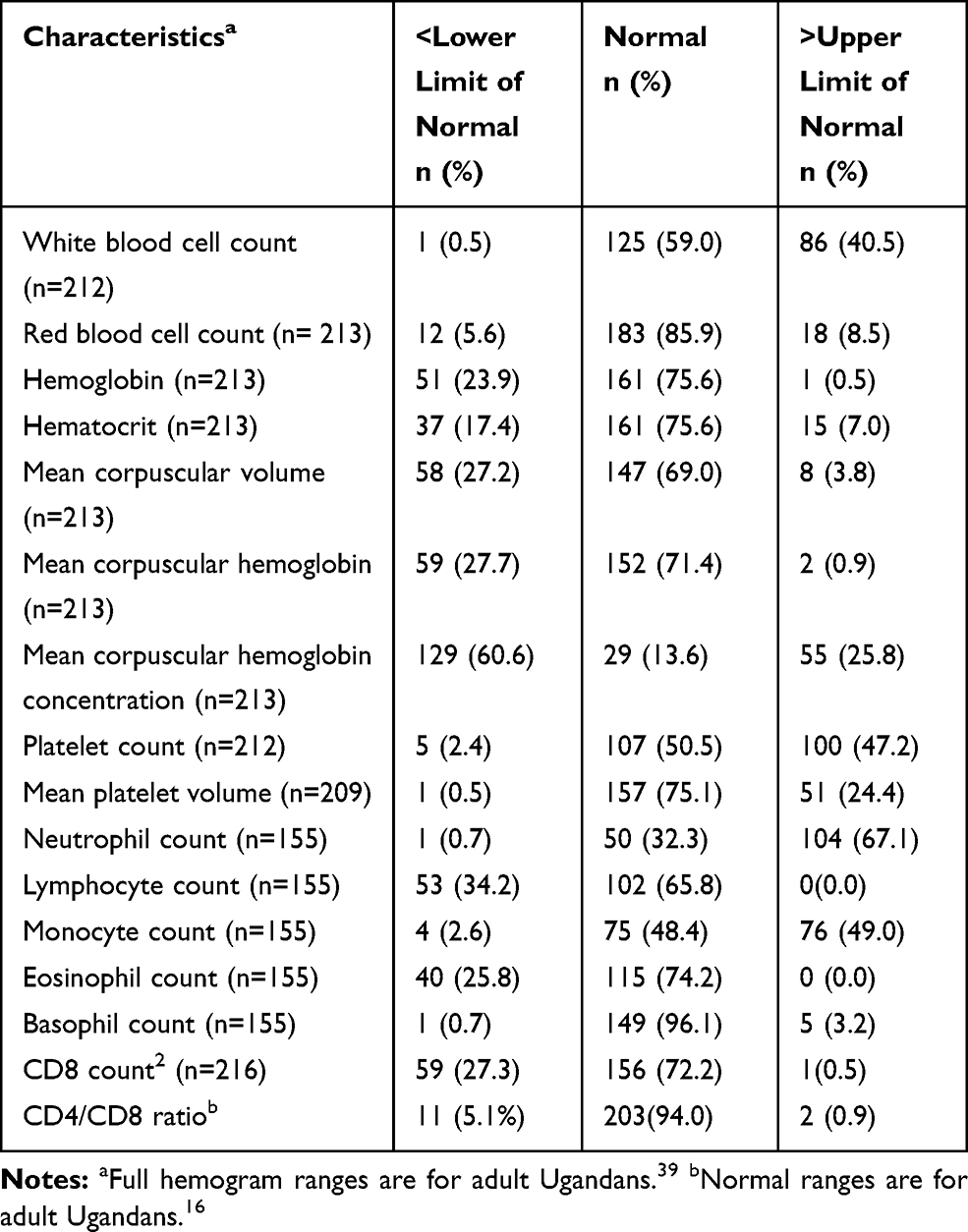 |
Table 2 Haematological and Immunological Characteristics of the Study Participants |
Prevalence of CD4+ T-Lymphocytopenia Among HIV-Negative TB Patients
The prevalence of CD4+ T-lymphocytopenia was 25% (54/216) (95% CI: 19.6% - 31.2%). For the entire study population, the mean (±SD) CD4+, CD8+ T-cell counts and CD4+/CD8+ ratio were 636.62 (±304.91) cells/mm3, 429.88 (±264.74) cells/mm3 and 1.77 (±0.89) respectively.
Predictors of CD4+ T-Lymphocytopenia Among HIV-Negative Pulmonary TB Patients
At multivariable logistic regression analysis, HIV-negative TB patients with anaemia (adjusted odds ratio (aOR): 3.83, 95% CI: 1.59–9.23, p = 0.003), weight loss (aOR: 3.61, 95% CI: 1.07–12.23, p = 0.039) and a low CD8+ T-cell count (aOR: 6.10, 95% CI: 2.68–13.89, p < 0.001) were more likely to have CD4+ T-lymphocytopenia while those with monocytosis (aOR: 0.35, 95% CI: 0.14–0.89, p = 0.028) were less likely to have CD4+ T-lymphocytopenia. The multivariable logistic regression model is shown in Table 3.
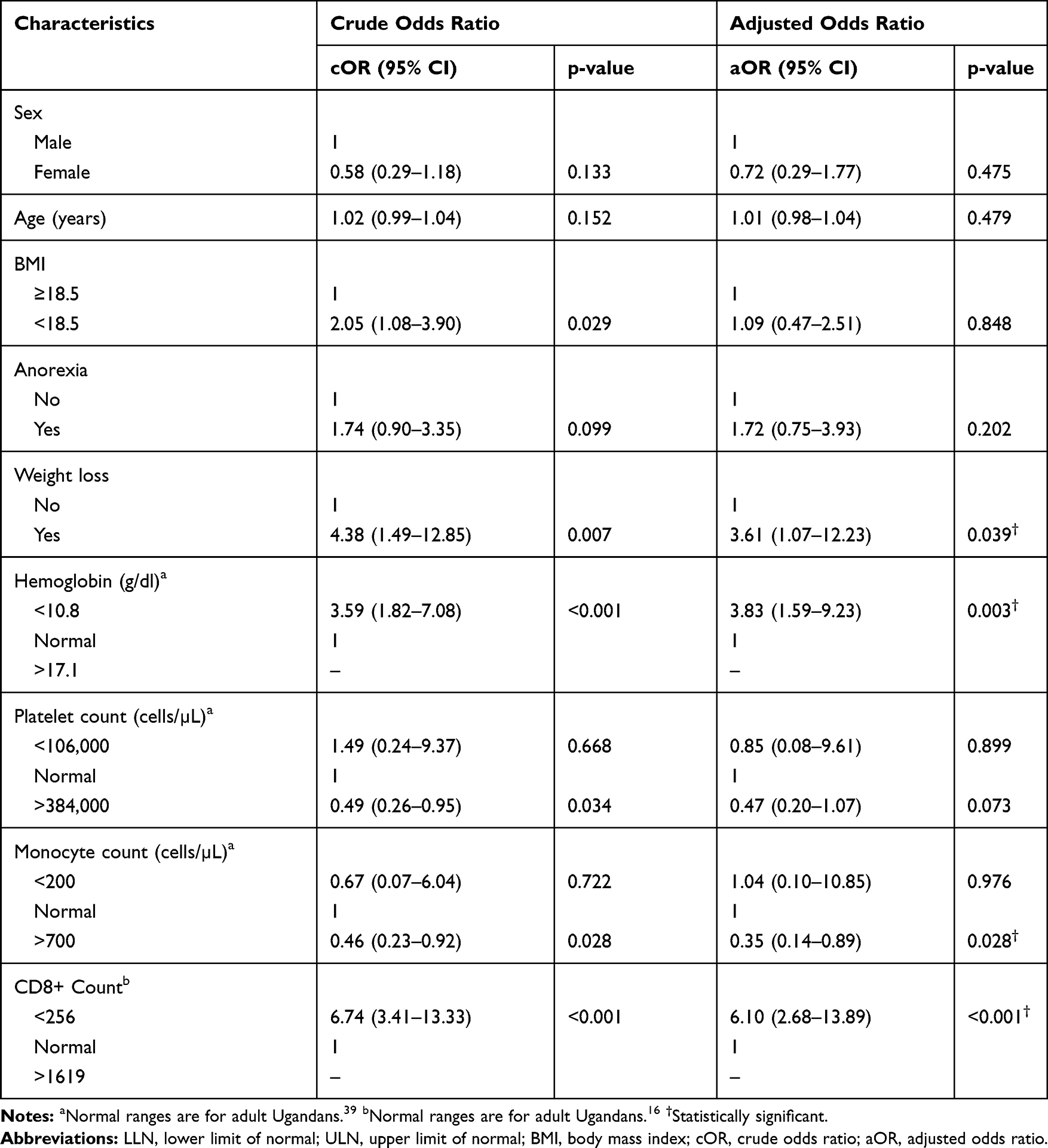 |
Table 3 Predictors of CD4+ T-Lymphocytopenia Among HIV-Negative TB Patients |
Discussion
In this study, we evaluated the prevalence and predictors of CD4+ T-lymphocytopenia among HIV-negative TB patients at a national tuberculosis treatment centre in Uganda. We found a high prevalence of CD4+ T-lymphocytopenia of 25%. Patients with anaemia, weight loss and low CD8+ T-cell counts were more likely to have CD4+ T-lymphocytopenia while those with monocytosis were less likely to have CD4+ T-lymphocytopenia.
The high prevalence of CD4+ T-lymphocytopenia indicates that a high proportion of HIV-negative TB patients in this setting may have impaired immune responses to Mtb infection. The consequences are higher rates of disseminated disease, absence of smear positivity and characteristic imaging findings that could delay diagnosis and superimposed opportunistic infections, all of which could potentially influence treatment outcomes.13 CD4+ T-lymphocytopenia among patients with tuberculosis could be explained by homing of T- lymphocytes in peripheral blood to heavily infected sites in the lung parenchyma and lung vasculature.18 It follows that response to TB treatment would correlate with improvement of the CD4+ T-lymphocyte counts in peripheral blood. Resolution of CD4+ T-lymphocytopenia upon treatment of TB has been reported.9,12 This suggests that TB is the cause of the T-lymphocytopenia as opposed to the CD4+ T-lymphocytopenia being a risk factor for TB. On the contrary, Zonios et al have shown that an idiopathic form of CD4+ T-lymphocytopenia is a risk factor for mycobacterial infections through a prospective study design.19 The cross-sectional nature of our study does not establish whether CD4+ T-lymphocytopenia was caused by TB or was a risk factor for TB among HIV-negative individuals in our study population.
CD4+ T-lymphocytopenia was associated with low CD8+ T-lymphocyte counts which would otherwise have enhanced TB immune responses.20 CD4+ T-lymphocytes are required for proliferation of CD8+ T-lymphocytes that modulate cytotoxic effects on Mtb infected macrophages and participate in memory immune responses against TB.21–23 Interestingly, the majority of the participants had a normal CD4/CD8 ratio, although the clinical utility of the CD4/CD8 ratio is not well established among HIV-negative TB patients. One meta-analysis indicates that the CD4/CD8 ratio in peripheral blood is significantly decreased among newly diagnosed patients with TB, although the bronchoalveolar CD4/CD8 ratio was increased on the contrary.27
The central role of the CD4+ T-lymphocytes in Mtb immune responses is further supported by our finding of lower odds of CD4+ T-lymphocytopenia among patients with monocytosis. Mtb-specific-CD4+ Th1 cell responses induce monocytosis by production of IFN-γ or tumour necrotic factor alpha (TNF-α) that recruits monocytes/macrophages to effect TB phagocytosis.24,25 Further, there is cell to cell communication between CD4+ T-lymphocytes and monocytes that could influence the cytokine repertoire for TB containment.26 Therefore, CD4+ T-lymphocytopenia could be indicative of global impairment of cell-mediated immune responses against TB.
We also found that anaemia and weight loss were independently associated with CD4+ T-lymphocytopenia. Anaemia and weight loss are prognostic of delayed sputum conversion and mortality in TB disease and the association with CD4+ T-lymphocytopenia may be indicative of severe TB disease.28–31 Therefore, CD4+ T-lymphocytopenia is likely to have prognostic importance even among HIV-negative TB patients.32 In support of this, baseline levels of some subsets of CD4+ T-lymphocytes have been shown to predict TB culture conversion.33 Weight loss in tuberculosis is mediated by appetite mediators, leptin and ghrelin, whose levels correlate with CD4+ T-lymphocyte-derived IFN-γ.34 Our observed association of weight loss and anaemia with CD4+ T-lymphocytopenia may be consequent to malnutrition observed among patients with longstanding infections.35,36 This is a plausible explanation in our study population whose symptoms had lasted over 90 days.
Skogmar et al also found a prevalence of CD4+ T-lymphocytopenia of 25% and 10% among HIV-negative TB patients when considering a cut off of CD4+ count of <500 cells/mm3 and 350 cells/mm3 respectively in Ethiopia.12 In contrast, Mhmoud et al found the proportion of HIV-negative TB patients with severe CD4+ T-lymphocytopenia (CD4+ count <300 cells/mm3) to be 83% in Sudan.14 Notably, these studies included participants without bacteriological confirmation of TB and different cut offs of the CD4+ count are employed. Dissimilar results can thus be expected.
Other studies have found CD4+ T-lymphocytopenia to be associated with extensive TB disease, low serum albumin level, low BMI, low haematocrit, smear positive TB, wasting and being bed ridden.11,12,37 These studies also invariably included patients without bacteriological confirmation of TB. Nonetheless, similar to Jones et al (1997), we found a low BMI to be significantly associated with CD4+ T-lymphocytopenia at bivariable logistic regression analysis.11 Also, since the haematocrit correlates with the haemoglobin levels,38 our association of CD4+ T-lymphocytopenia with anaemia is similar to the association of a low haematocrit with CD4+ T-lymphocytopenia reported by Jones et al. Moreover, the haematocrit demonstrated a high correlation with the haemoglobin levels in our study participants (Pearson’s correlation co-efficient of 0.803) hence its exclusion in the final logistic regression model in favour of the haemoglobin level.
One of the study limitations was missing data on the monocyte counts that necessitated imputation of missing data. We also did not evaluate the qualitative function of the CD4 T-lymphocytes to further characterise the immune responses among HIV-negative patients with CD4+ T-lymphocytopenia. Lastly, there might have been a referral bias of TB patients with severe disease as our study population was drawn from a national referral facility thus affecting generalizability of study findings. Nevertheless, the strength of our study lies in its utilisation of a homogenous population of bacteriologically confirmed TB cases.
Conclusion
The prevalence of CD4+ T-lymphocytopenia was high among HIV-negative TB patients. HIV-negative TB patients with weight loss, anaemia and a low CD8+ T-cell count were more likely to have CD4+ T-lymphocytopenia while those with monocytosis were less likely to have CD4+ T-lymphocytopenia. These findings suggest that HIV-negative TB patients with CD4+ T-lymphocytopenia have severe TB disease and immune dysfunction. We recommend further evaluation of the prognostic value CD4+ T-lymphocytopenia among HIV-negative TB patients.
Data Sharing Statement
Datasets generated and/or analysed during this study are available from the corresponding author upon reasonable request.
Funding
None.
Disclosure
The authors declare no conflicts of interest.
References
1. Global tuberculosis report 2019. Available from: https://www.who.int/tb/global-report-2019.
2. de Martino M, Lodi L, Galli L, Chiappini E. Immune response to Mycobacterium tuberculosis: a narrative review. Front Pediatr. 2019;7. doi:10.3389/fped.2019.00350.
3. Prezzemolo T, Guggino G, La Manna MP, Di Liberto D, Dieli F, Caccamo N. Functional signatures of human CD4 and CD8 T cell responses to Mycobacterium tuberculosis. Front Immunol. 2014;5. doi:10.3389/fimmu.2014.00180.
4. Kumar P. IFNγ-producing CD4+ T lymphocytes: the double-edged swords in tuberculosis. Clin Transl Med. 2017;6(1):21. doi:10.1186/s40169-017-0151-8
5. Sakai S, Kauffman KD, Sallin MA, et al. CD4 T cell-derived IFN-γ plays a minimal role in control of pulmonary Mycobacterium tuberculosis infection and must be actively repressed by PD-1 to prevent lethal disease. PLoS Pathog. 2016;12(5):e1005667. doi:10.1371/journal.ppat.1005667
6. Yao S, Huang D, Chen CY, Halliday L, Wang RC, Chen ZW. CD4+ T cells contain early extrapulmonary tuberculosis (TB) dissemination and rapid TB progression and sustain multieffector functions of CD8+ T and CD3- lymphocytes: mechanisms of CD4+ T cell immunity. J Immunol. 2014;192(5):2120–2132. doi:10.4049/jimmunol.1301373
7. Ellis PK, Martin WJ, Dodd PJ. CD4 count and tuberculosis risk in HIV-positive adults not on ART: a systematic review and meta-analysis. PeerJ. 2017;5:e4165. doi:10.7717/peerj.4165
8. Aung ZZ, Saw YM, Saw TN, et al. Survival rate and mortality risk factors among TB–HIV co-infected patients at an HIV-specialist hospital in Myanmar: a 12-year retrospective follow-up study. Int J Infect Dis. 2019;80:10–15. doi:10.1016/j.ijid.2018.12.008
9. Al-Aska A, Al-Anazi A, Al-Subaei S, et al. CD4+ T-lymphopenia in HIV negative tuberculous patients at King Khalid University Hospital in Riyadh, Saudi Arabia. Eur J Med Res. 2011;16(6):285–288. doi:10.1186/2047-783X-16-6-285
10. Uppal SS, Tewari SC, Verma S, Dhot PS. Comparison of CD4 and CD8 lymphocyte counts in HIV-negative pulmonary TB patients with those in normal blood donors and the effect of antitubercular treatment: hospital-based flow cytometric study. Cytometry B Clin Cytom. 2004;61B(1):20–26. doi:10.1002/cyto.b.20018
11. Jones BE, Oo MM, Taikwel EK, et al. CD4 cell counts in human immunodeficiency virus-negative patients with tuberculosis. Clin Infect Dis. 1997;24(5):988–991. doi:10.1093/clinids/24.5.988
12. Skogmar S, Schön T, Balcha TT, et al. CD4 cell levels during treatment for tuberculosis (TB) in Ethiopian adults and clinical markers associated with CD4 lymphocytopenia. PLoS One. 2013;8(12):e83270. doi:10.1371/journal.pone.0083270
13. Kony SJ, Hane AA, Larouzé B, et al. Tuberculosis-associated severe CD4+ T-lymphocytopenia in HIV-seronegative patients from Dakar. J Infect. 2000;41(2):167–171. doi:10.1053/jinf.2000.0721
14. Mhmoud NA, Fahal AH, van de Sande WWJ. CD4+ T-lymphocytopenia in HIV-negative tuberculosis patients in Sudan. J Infect. 2012;65(4):370–372. doi:10.1016/j.jinf.2012.06.003
15. Baluku JB, Nassozi S, Gyagenda B, et al. Prevalence of malaria and TB coinfection at a national tuberculosis treatment centre in Uganda. J Trop Med. 2019. doi:10.1155/2019/3741294
16. Nanzigu S, Waako P, Petzold M, et al. CD4-T-lymphocyte reference ranges in Uganda and its influencing factors. Lab Med. 2011;42(2):94–101. doi:10.1309/LMFT0VCE1UGO9YGD
17. Ministry of Health. National HIV Testing Services Policy and Implementation Guidelines. Published online 2016.
18. Jacques MK, Jayaraman P, Kuchroo VK, Behar SM. Defining the contribution of T cell exhaustion to failed immunity during TB. J Immunol. 2016;196(1 Supplement):
19. Zonios DI, Falloon J, Bennett JE, et al. Idiopathic CD4+ lymphocytopenia: natural history and prognostic factors. Blood. 2008;112(2):287–294. doi:10.1182/blood-2007-12-127878
20. Lin PL, Flynn JL. CD8 T cells and Mycobacterium tuberculosis infection. Semin Immunopathol. 2015;37(3):239–249. doi:10.1007/s00281-015-0490-8
21. Serbina NV, Flynn JL, Mansfield JM. CD8+ T cells participate in the memory immune response to Mycobacterium tuberculosis. Infect Immun. 2001;69(7):4320–4328. doi:10.1128/IAI.69.7.4320-4328.2001
22. Canaday DH, Wilkinson RJ, Li Q, Harding CV, Silver RF, Boom WH. CD4+ and CD8+ T cells kill intracellular Mycobacterium tuberculosis by a perforin and Fas/Fas ligand-independent mechanism. J Immunol. 2001;167(5):2734–2742. doi:10.4049/jimmunol.167.5.2734
23. Serbina NV, Lazarevic V, Flynn JL. CD4+ T cells are required for the development of cytotoxic CD8+ T cells during Mycobacterium tuberculosis infection. J Immunol. 2001;167(12):6991–7000. doi:10.4049/jimmunol.167.12.6991
24. Hertoghe T, Wajja A, Ntambi L, et al. T cell activation, apoptosis and cytokine dysregulation in the (co)pathogenesis of HIV and pulmonary tuberculosis (TB). Clin Exp Immunol. 2000;122(3):350–357. doi:10.1046/j.1365-2249.2000.01385.x
25. Sampath P, Moideen K, Ranganathan UD, Bethunaickan R. Monocyte subsets: phenotypes and function in tuberculosis infection. Front Immunol. 2018;9. doi:10.3389/fimmu.2018.01726.
26. Schrier SB, Hill AS, Plana D, Lauffenburger DA. Synergistic communication between CD4+ T cells and monocytes impacts the cytokine environment. Sci Rep. 2016;6(1):1–11. doi:10.1038/srep34942
27. YIN Y, QIN J, DAI Y, ZENG F, PEI H, WANG J. The CD4+/CD8+ ratio in pulmonary tuberculosis: systematic and meta-analysis article. Iran J Public Health. 2015;44(2):185–193.
28. Nagu TJ, Spiegelman D, Hertzmark E, et al. Anemia at the initiation of tuberculosis therapy is associated with delayed sputum conversion among pulmonary tuberculosis patients in Dar-es-Salaam, Tanzania. PLoS One. 2014;9(3):e91229. doi:10.1371/journal.pone.0091229
29. Kerkhoff AD, Wood R, Cobelens FG, Gupta-Wright A, Bekker L-G, Lawn SD. The predictive value of current haemoglobin levels for incident tuberculosis and/or mortality during long-term antiretroviral therapy in South Africa: a cohort study. BMC Med. 2015;13(1):1–13. doi:10.1186/s12916-015-0320-9
30. García-García M, de L, Ponce-de-León A, et al. Tuberculosis-related deaths within a well-functioning DOTS control program. Emerg Infect Dis. 2002;8(11). doi:10.3201/eid0811.020021
31. Filate M, Mehari Z, Alemu YM. Longitudinal body weight and sputum conversion in patients with tuberculosis, Southwest Ethiopia: a retrospective follow-up study. BMJ Open. 2018;8(9):e019076. doi:10.1136/bmjopen-2017-019076
32. Pilheu JA, De Salvo MC, Gonzalez J, Rey D, Elias MC, Ruppi MC. CD4+ T-lymphocytopenia in severe pulmonary tuberculosis without evidence of human immunodeficiency virus infection. Int J Tuberc Lung Dis. 1997;1(5):422–426.
33. Riou C, Gray CM, Lugongolo M, et al. A subset of circulating blood mycobacteria-specific CD4 T cells can predict the time to Mycobacterium tuberculosis sputum culture conversion. PLoS One. 2014;9(7):e102178. doi:10.1371/journal.pone.0102178
34. Zheng Y, Ma A, Wang Q, et al. Relation of leptin, ghrelin and inflammatory cytokines with body mass index in pulmonary tuberculosis patients with and without type 2 diabetes mellitus. PLoS One. 2013;8(11):e80122. doi:10.1371/journal.pone.0080122
35. Nájera O, González C, Toledo G, López L, Ortiz R. Flow cytometry study of lymphocyte subsets in malnourished and well-nourished children with bacterial infections. Clin Diagn Lab Immunol. 2004;11(3):577–580. doi:10.1128/CDLI.11.3.577-580.2004
36. Hughes S, Kelly P. Interactions of malnutrition and immune impairment, with specific reference to immunity against parasites. Parasite Immunol. 2006;28(11):577–588. doi:10.1111/j.1365-3024.2006.00897.x
37. Davoudi S, Rasoolinegad M, Younesian M, et al. CD4+ cell counts in patients with different clinical manifestations of tuberculosis. Braz J Infect Dis. 2008;12(6):483–486. doi:10.1590/S1413-86702008000600008
38. Quintó L, Aponte JJ, Menéndez C, et al. Relationship between haemoglobin and haematocrit in the definition of anaemia. Trop Med Int Health. 2006;11(8):1295–1302. doi:10.1111/j.1365-3156.2006.01679.x
39. Eller LA, Eller MA, Ouma B, et al. Reference intervals in healthy adult Ugandan blood donors and their impact on conducting international vaccine trials. PLoS One. 2008;3(12):e3919. doi:10.1371/journal.pone.0003919
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.