Back to Journals » Therapeutics and Clinical Risk Management » Volume 16
Pretreatment with Nalbuphine Prevents Sufentanil-Induced Cough During the Anesthesia Induction: A Randomized Controlled Trial
Authors Wang J ![]() , Duan J
, Duan J ![]() , Wang Q, Lu Y
, Wang Q, Lu Y
Received 28 January 2020
Accepted for publication 27 March 2020
Published 14 April 2020 Volume 2020:16 Pages 281—286
DOI https://doi.org/10.2147/TCRM.S247437
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor De Yun Wang
Jiang Wang,1,* Jinjuan Duan,1,2,* Qiuyue Wang,1 Yao Lu1
1Department of Anesthesiology, The First Affiliated Hospital of Anhui Medical University, Hefei 230022, People’s Republic of China; 2Department of Anesthesiology, Affiliated Anqing Hospital of Anhui Medical University, Anqing 246003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yao Lu
Department of Anesthesiology, The First Affiliated Hospital of Anhui Medical University Tel +86 55162922057
Email [email protected]
Background: Sufentanil-induced cough is frequent during the induction of anesthesia. The aim of this research was to assess the influence of pretreatment with nalbuphine on sufentanil-induced cough.
Patients and Methods: A total of 210 American Society of Anesthesiologists (ASA) I–II patients who are 18– 70 years old and scheduled for elective surgery were randomly divided into two groups. Group N was pretreated with 0.3 mg/kg nalbuphine at 150 s before induction with sufentanil, and Group C received the same volume of normal saline as the placebo. We assessed the incidence and severity of cough 2 minutes after sufentanil administration. We also recorded the hemodynamic changes and side effects of sufentanil after sufentanil administration.
Results: No patients had cough in group N, and 30 patients had cough in group C (degree of cough: mild 8; moderate 10; severe 12). The incidence and severity of cough in group N were significantly lower than those in group C.
Conclusion: Pretreatment with 0.3 mg/kg nalbuphine significantly suppressed the incidence and intensity of sufentanil-induced cough.
Keywords: nalbuphine, sufentanil, cough, anesthesia
Introduction
Sufentanil is widely used as an induction agent because of its beneficial properties, such as its analgesic effect with power potency, long duration, and hemodynamic stability. However, cough is the most common adverse effect of sufentanil. The occurrence of sufentanil-induced cough varies between 15% and 47.1% in unpretreated patients,1,2 which may lead to patient discomfort. Sufentanil-induced cough may increase the intracranial, intraocular, and intra-abdominal pressure.3 Therefore, cough should be avoided after sufentanil administration.
The primary action of sufentanil is on the opioid receptor and results in analgesia. However, the mechanism by which this drug produces cough is uncertain. In previous studies, many strategies, such as dezocine, magnesium, and dexmedetomidine, have been used to attenuate the incidence and intensity of cough. Nalbuphine, a synthetic opioid (μ-receptor antagonist and κ-receptor agonist), is a non-controlled opioid analgesic, and widely used to treat mild-to-severe pain. Moreover, nalbuphine has also been effectively used to treat opioid-induced the side effects, such as pruritus,4 bowel dysfunction,5 and so on. However, to our knowledge, there is no report to evaluate the influences of nalbuphine on the frequency of cough caused by sufentanil. Therefore, we performed this study to investigate the effects of nalbuphine on sufentanil-induced cough.
Methods
This study was approved by the Ethics Committee of the First Affiliated Hospital, Anhui Medical University (IRB #PJ2019-09-13) and written informed consent was obtained from all subjects participating in the trial. The trial was registered prior to patient enrollment at www.chictr.org.cn (ChiCTR1900023984, Principal investigator: Yao Lu, Date of registration: 2019-6-20).
The study was performed from July 2019 to August 2019 at First Affiliated Hospital of Anhui Medical University in accordance with the declaration of Helsinki, and a total of 240 patients were screened. A total of 210 participants scheduled for elective surgery were recruited in this study (Figure 1). The inclusion criteria included American Society of Anesthesiologists (ASA) I–II patients, both sex, aged 18–70 years, and body mass index (BMI) ≤30 kg/m2. Additionally, the participants were excluded if they met the following criteria: chronic cough, having an upper respiratory infection recently, smoking, asthma, bradycardia, use of angiotensin-converting enzyme inhibitors and steroids or bronchodilators. We randomly divided all participants into two groups using a computer-generated table of random numbers, with 105 patients in each group. The randomization results were kept in sealed opaque envelopes before the time of the study drug preparation. Group N was pretreated with 0.3 mg/kg nalbuphine for 150 s before induction with sufentanil (0.5 μg/kg), and Group C received the same volume of normal saline as the control group. The patients and anesthesiologists who recorded the intensity of cough were blinded to the assigned patient groups. The pretreatment drugs were prepared in a 20-mL syringe by the anesthesiologist who did not participate in the induction of anesthesia.
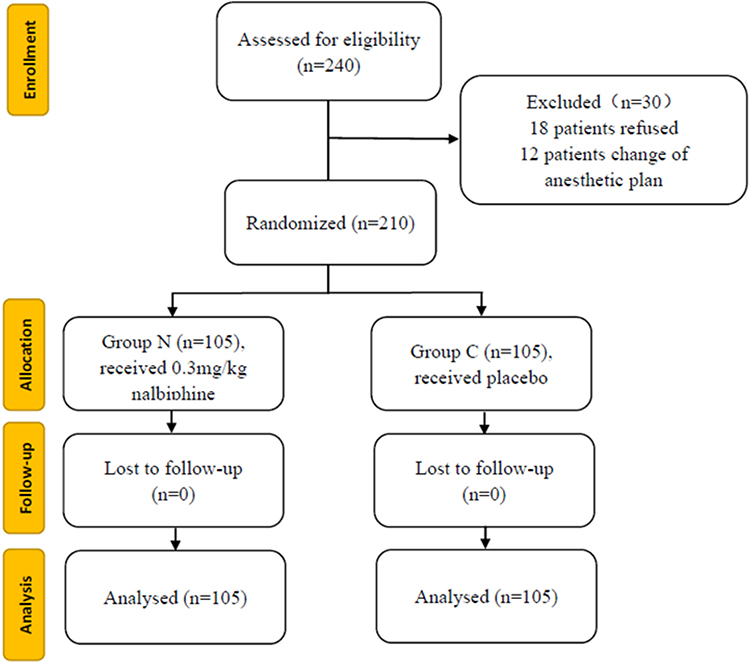 |
Figure 1 CONSORT flow of clinical procedures for the study. Group N pretreated with 0.3 mg/kg nalbuphine at 150 s before induction with sufentanil; Group C received the same volume of normal saline as the placebo. |
After patients arrived at the operating room, routine monitoring including noninvasive blood pressure, electrocardiogram, and oxygen saturation was applied, and venous access was established. The patients were oxygenated, and the study drug was administered before the induction of anesthesia. No drug was injected into the patient before the study drugs. One hundred and fifty seconds after pretreatment drug administration, anesthesia was induced with sufentanil over 3 s, while the patients were recorded for episodes of cough 2 minutes after the injection of sufentanil. The degree of coughing was graded depending on the number of episodes of cough: mild (1–2 times), moderate (3–5 times), severe (>5 times).6 The systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate (HR) were recorded before (T0) and 2 minutes after the nalbuphine injection (T1) and 2 minutes after the sufentanil injection (T2). Assisted mask ventilation was adopted if pulse oxygen saturation (SpO2) was less than 95%. If patients suffered from truncal rigidity, then the induction of anesthesia was performed with 0.02 mg/kg midazolam, 0.3 mg/kg etomidate, and 0.9 mg/kg rocuronium. Additionally, the side effects associated with sufentanil, such as apnea, truncal rigidity, bradycardia, or nausea, were recorded.
Sample size estimated using Power and Sample Size Program 3.0.43. According to the previous study, the frequency of cough induced by sufentanil was 27%,7 assuming a 60% lower frequency of cough after nalbuphine administration, the sample size was calculated as 91 patients per group at a power of 80% and a two-tailed α-error of 5%. Therefore, the sample size of this study was increased to 105 patients in each group.
All data are expressed as the mean ± standard deviation or percentages. The demographic data of patients and vital signs between two groups were compared using T-tests. The chi-squared test was used to analyze the frequency and severity of sufentanil-induced cough, ASA class, and gender. We used SPSS 13.0 to analyze all data. P<0.05 was considered statistically significant.
Results
No significant differences were found in demographic characteristics between the two groups (Table 1). The incidence of cough in group C was 28.5%, and no patients had cough in group N. Therefore, pretreatment with nalbuphine significantly reduced sufentanil-induced cough after the administration of nalbuphine. The severity of cough was significantly lower in group N (mild, moderate, severe: 0, 0, 0, respectively) than in the placebo (8, 10, 12) (Table 2). SBP, DBP, and HR were not significantly different at each time point between the two groups (Figure 2).
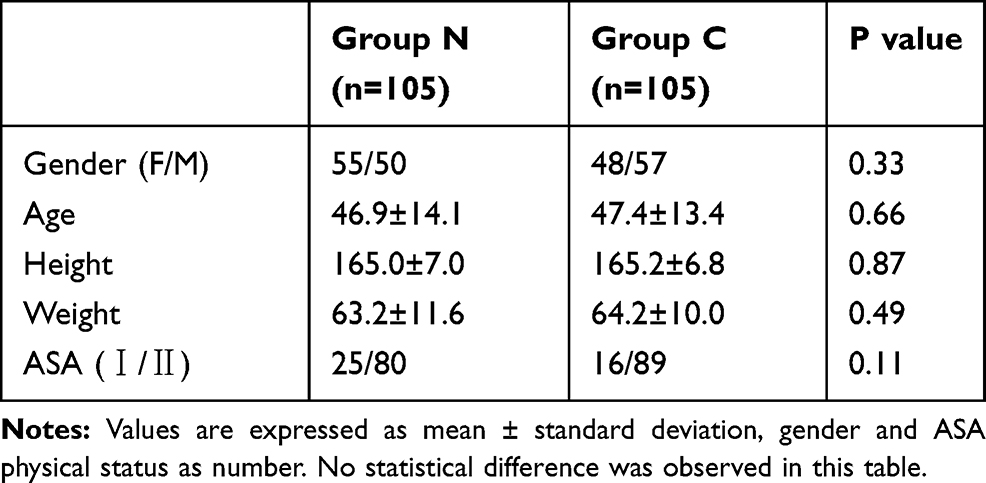 |
Table 1 Demographic Data of the Patients Receiving Nalbuphine or Placebo |
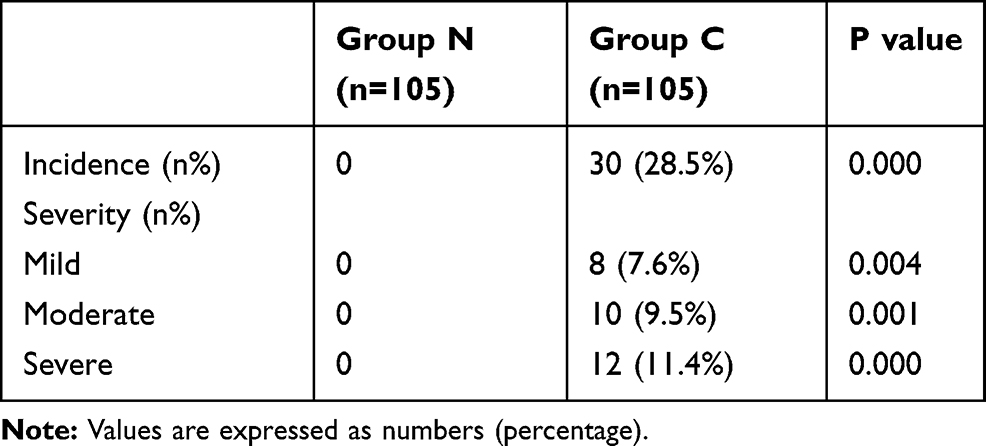 |
Table 2 Incidence and Severity of Cough in Patients Receiving Nalbuphine or Placebo |
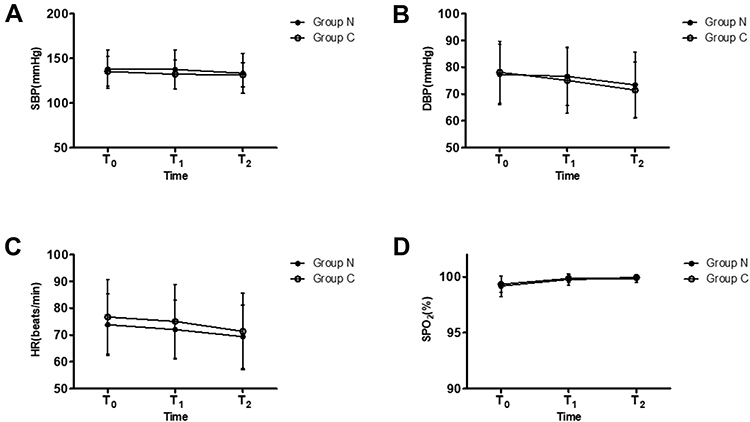 |
Figure 2 Changes in vital signs after treatment. (A) SBP (mmHg); (B) DBP (mmHg); (C) HR (beats/min); (D) SpO2 (%); Group N pretreated with 0.3 mg/kg nalbuphine at 150 s before induction with sufentanil; Group C received the same volume of normal saline as the placebo. SBP, DBP, HR and SpO2 were not significantly different at each time point between the two groups. Abbreviations: SBP, Systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; T0, time before administration of nalbuphine or normal saline injection; T1, 2 minutes after administration of nalbuphine or normal saline injection; T2, 2 minutes after the sufentanil injection. |
In the control group, one patient had nausea and two patients suffered from truncal rigidity.
Discussion
The results of this study revealed that pretreatment with 0.3 mg/kg nalbuphine significantly decreased the incidence and severity of cough compared to the control group.
Sufentanil-induced cough may lead to patient discomfort. Moreover, sufentanil-induced cough may increase intracranial, intraocular, and intra-abdominal pressures in patients with coexisting conditions, such as open eye injury, dissecting aortic aneurysm, and pneumothorax. Therefore, sufentanil-induced cough should be prevented in these patients. However, the mechanism of cough induced by sufentanil is unclear. Several mechanisms have been proposed to interpret fentanyl-induced cough. A pulmonary chemoreflex mediated by pulmonary C-fibers (J-receptors) or by irritant receptors (rapidly adapting receptors) is thought to be responsible for this phenomenon.8,9 Furthermore, the deformation of the mucosa caused by fentanyl inducing tracheal smooth muscle contraction can stimulate the irritant receptors in the tracheobronchial mucosa.10 Besides, a sudden adduction of the vocal cords or a supraglottic obstruction by soft tissue caused by opioid-inducing histamine release and muscle rigidity also makes a significant contribution to the cough.9,11
The main cause of cough may be related to sufentanil (1 μg/kg) reducing chest wall compliance.12 The sufentanil injection can lead to closure of the vocal cords which may be the major reason for difficult ventilation.13 Therefore, the expiratory work caused by glottal closure may be the possible mechanism of cough induced by sufentanil injection. In animals, we often use citric acid which stimulates C-fibers in the airway to activate the cough reflex.14 Sufentanil contains citrate salts, and the composition of citrate may be the cause of the cough reflex.
Various strategies, such as magnesium, dexmedetomidine, and dezocine, have been used to prevent sufentanil-induced cough. An et al1 found that magnesium could inhibit sufentanil-induced cough. Possible mechanisms, including magnesium, can induce bronchodilation by inhibiting cholinergic neuromuscular transmission and attenuating calcium-induced muscle contraction. In a previous research, Sun et al7 indicated that the administration of dexmedetomidine for 5 minutes significantly inhibited sufentanil-induced cough. The primary mechanism was that α2-adrenoreceptor agonists can reverse the muscular rigidity induced by sufentanil and block histamine-induced bronchoconstriction. The study by our team shows that pretreatment with 0.1 mg/kg dezocine was effective in suppressing sufentanil-induced cough. Our previous study proposed that the dezocine-mediated suppression of the cough induced by sufentanil may be mainly associated with κ-receptor antagonism, which in turn antagonizes sufentanil-activated μ receptors, thereby reducing cough.15
Nalbuphine is a synthetic opioid (μ-receptor antagonist and κ-receptor agonist), and the common use dose ranges from 0.2 mg/kg to 0.4 mg/kg.16 The onset time of nalbuphine was 2–3 minutes,17 so in our study, the pretreatment drug was administered at 150 s before sufentanil injection. The results of this study indicate that pretreatment with nalbuphine can effectively attenuate the incidence and severity of sufentanil-induced cough. A possible mechanism for this phenomenon is that nalbuphine prevents sufentanil-induced cough by partial μ-receptor antagonism, which antagonizes sufentanil-activated μ-receptor, thereby reducing cough. Moreover, nalbuphine may reverse the muscular rigidity induced by sufentanil, which results in reducing cough.
The limitation of this study is that we did not assess the effect of different doses of nalbuphine on the incidence and severity of sufentanil-induced cough. Additionally, the current study lacked pretreatment with nalbuphine to suppress cough induced by other opioid drugs. In the future, we will evaluate different doses of nalbuphine on the frequency and reflex degree of sufentanil-induced cough during the induction of anesthesia.
Conclusion
In conclusion, this research indicates that pretreatment with 0.3 mg/kg nalbuphine significantly suppressed the frequency and intensity of sufentanil-induced cough. Therefore, pretreatment with nalbuphine presents an effective way to prevent sufentanil-induced cough during the induction of anesthesia.
Abbreviations
ASA, American Society of Anesthesiologists; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; SpO2, pulse oxygen saturation.
Data Sharing Statement
The authors are pleased to share individual identified participant data. The data of this study including figures and tables will be available by contacting corresponding author. The data can be used permanently after the article is published.
Acknowledgments
The authors of this study would like to thank Meng G.G. for support in completing this study, Yu Y.Q., Chen C., and Tang W. for support in interpreting the data, and Liu X. for helping write the manuscript.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work is supported by the National Natural Science Foundation of China (No. 81770295).
Disclosure
All authors declare that they have no conflicts of interest.
References
1. An LJ, Gui B, Su Z, Zhang Y, Liu HL. Magnesium sulfate inhibits sufentanil-induced cough during anesthetic induction. Int J Clin Exp Med. 2015;8(8):13864–13868.
2. Agarwal A, Gautam S, Nath SS, Gupta D, Singh U. Comparison of the incidence and severity of cough induced by sufentanil and fentanyl: a prospective, randomised, double-blind study. Anaesthesia. 2007;62(12):1230–1232. doi:10.1111/j.1365-2044.2007.05249.x
3. Yu MS, Kim JY, Kim HY. Intravenous dexamethasone pretreatment reduces remifentanil induced cough. Korean J Anesthesiol. 2011;60(6):403–407. doi:10.4097/kjae.2011.60.6.403
4. Jannuzzi RG. Nalbuphine for treatment of opioid-induced pruritus: a systematic review of literature. Clin J Pain. 2016;32(1):87–93. doi:10.1097/AJP.0000000000000211
5. Candy B, Jones L, Vickerstaff V, et al. Mu-opioid antagonists for opioid-induced bowel dysfunction. Cochrane Database Syst Rev. 2008;6:CD006332.
6. Agarwal A, Azim A, Ambesh S, et al. Salbutamol, beclomethasone or sodium chromoglycate suppress coughing induced by iv fentanyl. Can J Anaesth. 2003;50(3):297–300. doi:10.1007/BF03017801
7. Sun S, Huang SQ. Effects of pretreatment with a small dose of dexmedetomidine on sufentanil-induced cough during anesthetic induction. J Anesth. 2013;27(1):25–28. doi:10.1007/s00540-012-1470-y
8. Karlsson JA. The role of capsaicin-sensitive C-fibre afferent nerves in the cough reflex. Pulm Pharmacol. 1996;9(5–6):315–321. doi:10.1006/pulp.1996.0041
9. Kamei J, Nakanishi Y, Asato M, Ikeda H. Fentanyl enhances the excitability of rapidly adapting receptors to cause cough via the enhancement of histamine release in the airways. Cough. 2013;9(1):3. doi:10.1186/1745-9974-9-3
10. Yasuda I, Hirano T, Yusa T, Satoh M. Tracheal constriction by morphine and by fentanyl in man. Anesthesiology. 1978;49(2):117–119. doi:10.1097/00000542-197808000-00012
11. Lin CS, Sun WZ, Chan WH, Lin CJ, Yeh HM, Mok MS. Intravenous lidocaine and ephedrine, but not propofol, suppress fentanyl-induced cough. Can J Anaesth. 2004;51(7):654–659. doi:10.1007/BF03018421
12. Yemen TA. Small doses of sufentanil will produce violent coughing in young children. Anesthesiology. 1998;89(1):271–272. doi:10.1097/00000542-199807000-00043
13. Bennett JA, Abrams JT, Van Riper DF, Horrow JC. Difficult or impossible ventilation after sufentanil-induced anesthesia is caused primarily by vocal cord closure. Anesthesiology. 1997;87(5):1070–1074. doi:10.1097/00000542-199711000-00010
14. Tanaka M, Maruyama K. Mechanisms of capsaicin- and citric-acid-induced cough reflexes in guinea pigs. J Pharmacol Sci. 2005;99(1):77–82. doi:10.1254/jphs.FPJ05014X
15. Liu XS, Xu GH, Shen QY, et al. Dezocine prevents sufentanil-induced cough during general anesthesia induction: a randomized controlled trial. Pharmacol Rep. 2015;67(1):52–55. doi:10.1016/j.pharep.2014.08.004
16. Lv Z, Fang J, Zhu J, et al. Intravenous dezocine pretreatment reduces the incidence and intensity of myoclonus induced by etomidate. J Anesth. 2014;28(6):944–947. doi:10.1007/s00540-014-1886-7
17. Gupta M, Gupta P. Nalbuphine pretreatment for prevention of etomidate induced myoclonus: a prospective, randomized and double-blind study. J Anaesthesiol Clin Pharmacol. 2018;34(2):200–204. doi:10.4103/joacp.JOACP_210_16
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.