Back to Journals » Clinical Ophthalmology » Volume 15
Predictors of Photic Phenomena with a Trifocal IOL
Authors Espaillat A ![]() , Coelho C
, Coelho C ![]() , Medrano Batista MJ, Perez O
, Medrano Batista MJ, Perez O ![]()
Received 17 September 2020
Accepted for publication 9 December 2020
Published 10 February 2021 Volume 2021:15 Pages 495—503
DOI https://doi.org/10.2147/OPTH.S282469
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Arnaldo Espaillat,1 Constanca Coelho,2 Michael J Medrano Batista,1 Obniel Perez1
1Anterior Segment Department, Instituto Espaillat Cabral, Santo Domingo, Dominican Republic; 2Lisbon Medical School, University of Lisbon, Lisbon, Portugal
Correspondence: Arnaldo Espaillat
Instituto Espaillat Cabral, Av. Independencia 853, Zona Universitaria, Santo Domingo, Dominican Republic
Tel +1-809-686-0268
Email [email protected]
Aim: To assess predictive factors associated with glares and halos in patients undergoing cataract surgery with PanOptix trifocal IOL implantation.
Methods: Single-center retrospective study. One hundred and forty eyes from 70 patients with cataract were bilaterally implanted with a trifocal PanOptix aspherical diffractive lens between 2017 and 2019 and followed-up for six months. All patients were evaluated for refraction, corneal topography, and aberrometry pre- and post-operatively. Patients were assessed at 1 day, 6 days, 1 and 6 months after surgery. One and six months post-operatively patients were asked to complete a satisfaction questionnaire that included photic phenomena assessment. Main outcome measures were photic phenomena at 1 and 6 months of follow-up. Predictors of photic phenomena at 1 and 6 months were also analyzed.
Results: A higher corneal coma was associated with more mild halos at 6 months with no association regarding other degrees of severity. The lower the age the higher the glare or halos, the higher the lens thickness and the lower the anterior chamber depth or chord μ the less halos at 1 month. A significant proportion of patients had more none/mild compared to moderate/severe glare and halos both at 1 and 6 months post-operatively. Baseline BCVA was the only predictor of halos at 1 month and glare and halos at 6 months post-surgery.
Conclusion: On multivariate regression analyses, the only predictor of photic phenomena was baseline visual acuity, suggesting that patients that have a better visual acuity before surgery are more demanding regarding visual outcomes after surgery.
Keywords: cataract surgery, PanOptix trifocal IOL, predictors of photic phenomena
Introduction
Multifocal lenses offer the possibility of spectacle-free vision and this could be a motivation for the use of multifocal IOLs instead of monofocal IOLs.1,2 Nevertheless, the association of multifocal IOLs with photic phenomena remains one of the major causes of complaint after surgery.1,2
Pseudophakic photic phenomena are characterized by nonuseful patterns projected onto the retina in positive forms. These photic phenomena refer to bright artifacts that are only present in certain light conditions and produce images as glares and/or halos.3
Trifocal IOLs were designed to provide near, intermediate, and distance visual performances and increase spectacle independence.4 AcrySof® IQ PanOptix™ (Alcon Laboratories, Inc., Fort Worth, TX, USA) is a nonapodized diffractive trifocal IOL that distributes light energy to three focal points in both small and large pupil conditions. Photic phenomena of multifocal IOLs, such as halos and glare, vary between patients1 with some continuing to experience pseudophakic photic phenomena5 many months after surgery. In this study, we assessed factors associated with glares and halos in patients with PanOptix IOL implantation.
Patients and Methods
Study Population
This was a single-center retrospective study, performed at Instituto Espaillat Cabral, Dominican Republic, between September 2017 and February 2019, which included a study population of 140 eyes from 70 patients undergoing cataract surgery with bilateral implantation of a trifocal PanOptix lens.
Inclusion criteria: age ≥ 45 years old; patients that wanted to have good vision most of the time without glasses at all distances; highest limit of mesopic pupil of 6 mm; corneal total higher-order aberration (HOA) ≤ 0.5 µm; corneal spherical aberration ≤ 0.3 µm; corneal coma ≤ 0.4 µm; corneal trefoil ≤ 0.3 µm; and angle kappa ≤ 0.58 mm. Exclusion criteria: patients with moderate or severe dry eye syndrome; any ocular pathology other than cataract or any systemic condition that, in the investigators’ opinion, could compromise the efficacy or safety of surgery; eyes with surgical complications or posterior capsular opacification that required an Nd:YAG laser capsulotomy; patients unwilling or unable to provide informed consent; patients with type A personality and/or unreal post-surgical visual expectations.
This study was conducted in agreement with the tenets of the declaration of Helsinki in its latest amendment (Brazil, 2013). All patients signed an informed consent form and the study was approved by the Ethics Committee of Instituto Espaillat Cabral. No patient-protected data were collected or reported.
The Trifocal PanOptix Lens
This is a single-piece hydrophobic IOL that is based on a quadrifocal optical principle. It is designed to have an intermediate focal point of 60 cm (arms-length) and an optimal close reading distance at 42 cm. The light efficiency of the IOL has been measured at 88% at a 3.0 mm pupil size.6,7 This IOL comes in a toric and non-toric version.
Surgical Procedure
All surgeries were performed by the same surgeon (AE) and were done either by standard phacoemulsification with the Centurion® Vision System (Alcon Laboratories, Inc.), or assisted with femtosecond laser (LenSx®; Alcon Laboratories, Inc.). The same patient had both their eyes operated within a week.
Assessments
Pre-operatively all patients underwent a comprehensive ophthalmic history and examination including tear osmolarity test (Tearlab Corporation, San Diego, CA, USA), corneal topography, and aberrometry (OPD-scan III, Nidek Co Ltd., Gamagori, Japan), biometry (IOLMaster 700, Carl Zeiss Meditec AG, Jena, Germany), specular microscopy (CEM 539, Nidek Co Ltd.), and macular and papillary Optical Coherence Tomography (Cirrus 4000 Hd OCT, Carl Zeiss Meditec AG). Patients who had a pre-operative keratometric astigmatism ≥0.7D against-the-rule or ≥1.0D with-the-rule were corrected with a toric IOL. The Barrett universal II formula was used to calculate the spherical power of the lens and the Barrett’s formula for toric lenses was used to calculate the cylindrical power.
Patients were assessed at 1 day, 6 days, 1 and 6 months after surgery. One and six months post-operatively, refraction, corneal topography, and aberrometry were performed and patients were asked to complete a satisfaction questionnaire including photic phenomena (Supplementary file 1). The presence of posterior capsular opacity was also assessed.
Manifest refraction, both corrected and uncorrected far and near visual acuity, pre-operative corneal aberration as well as post-operative total ocular and corneal aberration measurements, biometric values, and satisfaction questionnaire data were tabulated. Visual acuity data were recorded in Snellen notation but converted to logarithm of the minimum angle of resolution (logMAR) for analytical purposes. Data were analyzed pre-operatively and after surgery at 1 and 6 months of follow-up.
Outcomes
Main outcome measures were photic phenomena at 1 and 6 months of follow-up. We have also analyzed if any of the following pre-surgical parameters could be associated with photic phenomena in patients with PanOptix IOL implantation: mesopic pupil, angle kappa, total ocular and corneal higher-order aberrations, coma, trefoil, spherical aberration, corneal surface regularity index (SRI), and corneal irregular astigmatism index (IAI), all measured by OPD-scan III; average keratometry, corneal astigmatism, axial length, anterior chamber depth, lens thickness, and the apparent chord μ value, which is contemplated to be the distance between Purkinje image 1 and the apparent pupil center when viewed coaxially from the light source at the cornea,8,9 all measured by IOL M 700.
Statistical Analysis
All categorical variables are expressed as numbers and percentages. All continuous variables are expressed using mean and 95% Confidence Interval (95% CI) for the mean. Between-group analysis was performed using the Kruskal–Wallis test adjusted for multiple comparisons, the Mann–Whitney U-test or the Χ2 test, as appropriate. Three groups of glare and halos have been considered for association analyses: no vs mild vs moderate vs severe; absence vs presence; and no/mild vs moderate/severe. Four multivariate logistic regressions were performed, all with the backward conditional method, using glare and halos at 1 and 6 months as the dependent variables (groups no/mild vs moderate/severe) and age, baseline best-corrected visual acuity (BCVA) and sphere at 1 month as the independent variables. All multivariate analyses were adjusted for eye bilaterality. Tests were considered significant at α=0.05 significance level (two-sided). SPSS v20 was used for statistical analysis.
Results
Demographic Parameters
Of the 70 patients included in this study, 57.1% were females with a mean age of 62.2 years (95% CI 62.2–67.7). The 42.9% males showed a mean age of 66.9 years (95% CI 64.6–69.2). There were no differences in age between sexes (p=0.396). When analyzing age between the different groups of glares and halos, there were some significances, all in the same direction: the lower the age the higher the glare or halos (no vs mild vs moderate vs severe, p=0.013 for halos at 1 month; absence vs presence, p=0.038 for glare at 1 month, p=0.003 for halos at 1 month, p=0.012 for glare at 6 months, p=0.032 for halos at 6 months; and no/mild vs moderate/severe, p=0.043 for halos at 1 month).
Capsular Opacity and Vision Quality at 1 and 6 Months Post-Surgery and Refractive Parameters at 1 Month Post-Surgery
The incidence of capsular opacity was low both at 1 month and 6 months post-surgery (0.7% and 6.0%, respectively). At 6 months post-surgery, 3 eyes from 2 patients showed grade 1 posterior capsular opacification (PCO) with no need for YAG laser capsulotomy, whilst 4 eyes from another 2 patients showed grade 2 PCO and underwent YAG laser capsulotomy. Spectacle independence at all distances and at 1 and 6 months post-surgery varied between 97% and 100%. Between 96.6% and 98.5% of patients would recommend the surgery. Subjective vision quality perceived by patients at 1 month varied between 9.41 and 9.75 at all distances, and at 6 months varied between 9.25 and 9.61 at all distances. As for refractive results, and 1 month after surgery, the mean sphere was 0.09 diopters (D) with a 95% CI 0.04–0.14, the mean cylinder was −0.26D with a 95% CI −0.29–(−0.22), and a mean spherical equivalent of −0.04D with a 95% CI −0.09–0.02 – Table 1. Also, 81.2% of eyes were within ±0.25D and 97.1% within ±0.50D of spherical target, whilst 96.4% of eyes were within ≤0.50D and 98.6% within ≤0.75D of cylinder.
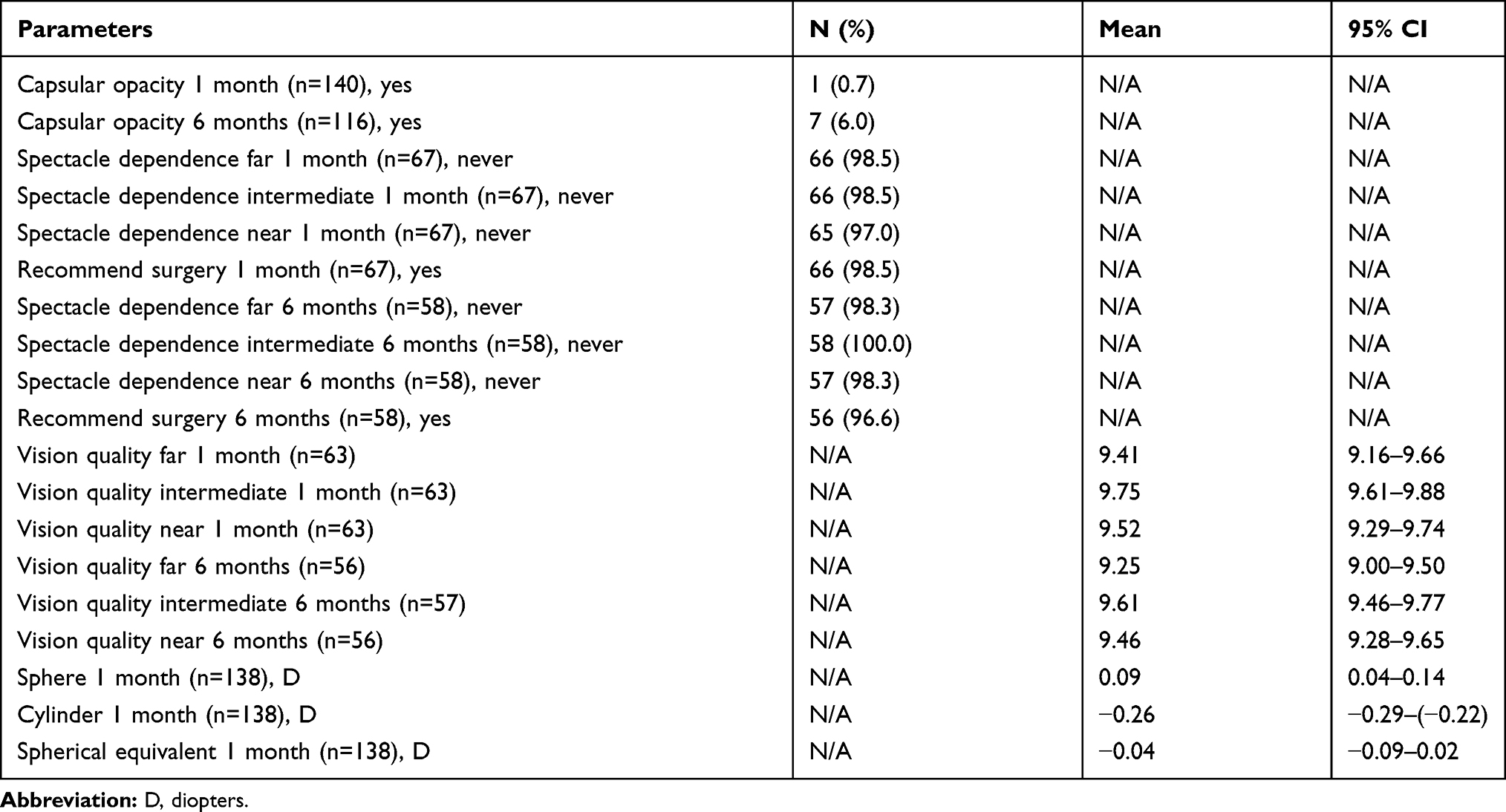 |
Table 1 Capsular Opacity and Vision Quality at 1 and 6 Months Post-Surgery and Refractive Parameters at 1 Month Post-Surgery |
Glare and Halos at 1 and 6 Months Post-Surgery: Topography and Aberration Parameters
When analyzing the 4 groups of glare and halos at 6 months, no vs mild vs moderate vs severe, patients with no halos at 6 months showed lower corneal coma when compared to patients with mild halos, with no differences on other topography or aberration parameters either for glare or halos at 6 months – Table 2. When analyzing only between the absence vs presence of glare or halos at 6 months, patients with higher corneal coma or higher total coma showed more halos at 6 months (p=0.007 and p=0.005, respectively). The 0.200 to 0.399 µm corneal HOA group reported less moderate halos at 1 month (28.6%) compared to mild (69.6%) or no (75.0%) halos (p=0.001). None of the topography or the remaining aberration parameters showed differences at 1 month.
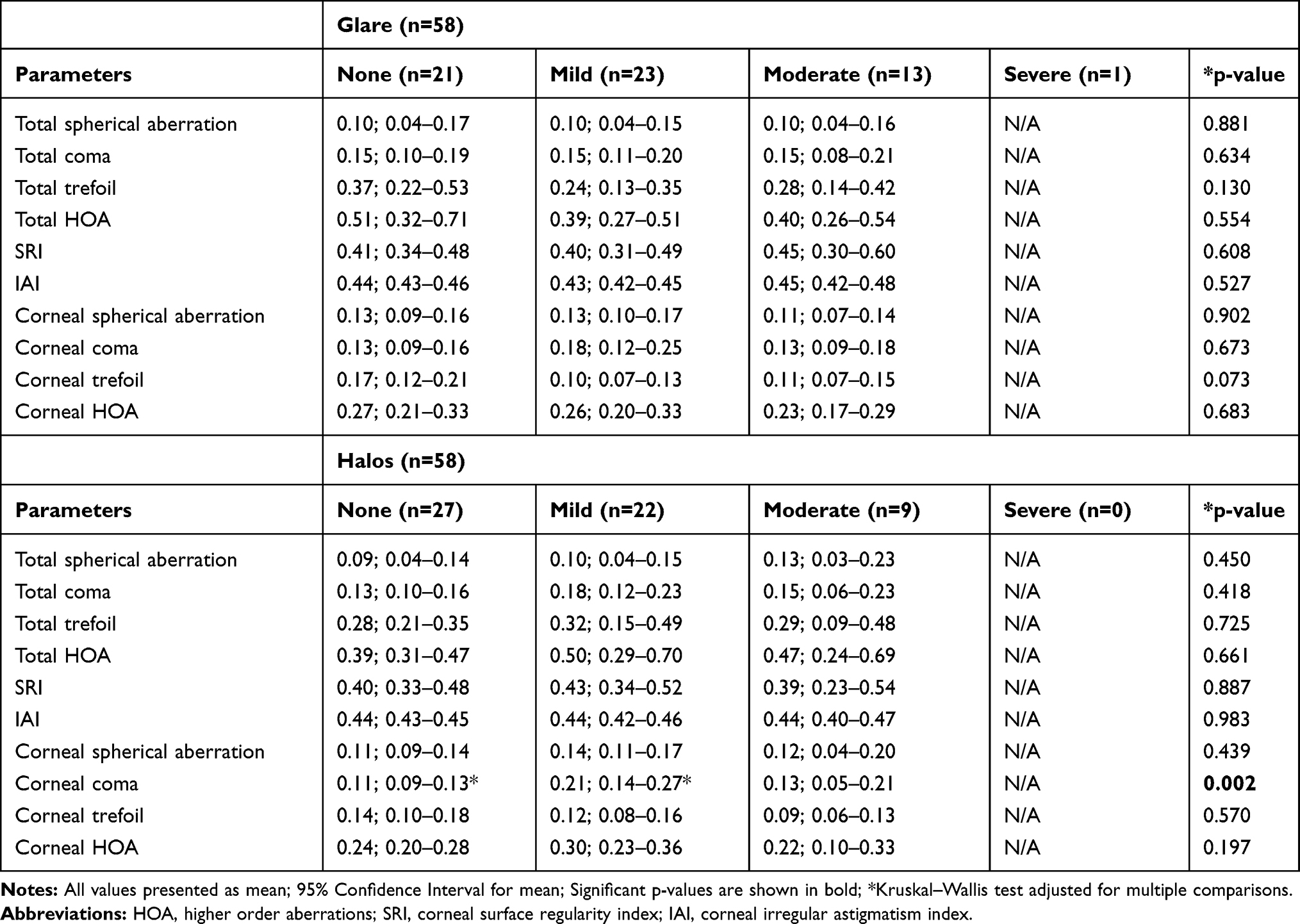 |
Table 2 Glare and Halos at 6 Months Post-Surgery: Topography and Aberration Parameters |
Glare and Halos at 1 and 6 Months Post-Surgery and Pre-Operative Biometry Parameters
None of the pre-operative biometry parameters showed an association with glare or halos at 6 months post-surgery, when considering the 4 groups of glare or halos (no vs mild vs moderate vs severe) – Table 3. However, when analyzing only between the absence vs presence of glare or halos at 1 month, patients with higher anterior chamber depth showed more halos at 1 month (p=0.044), whilst patients with higher lens thickness showed less halos at 1 month (p=0.035). Chord μ was higher in patients who reported halos at 1 month (p=0.007).
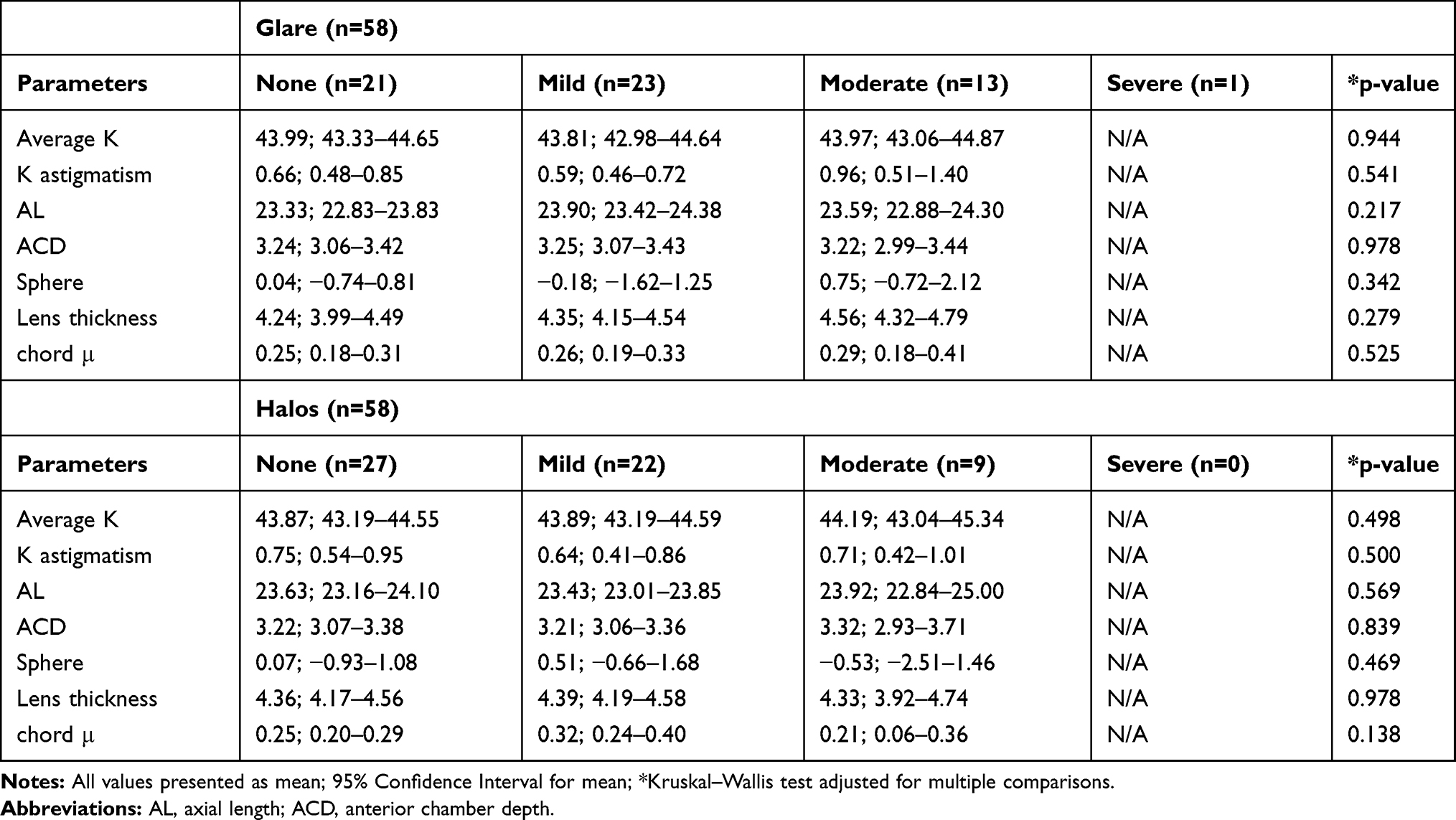 |
Table 3 Glare and Halos at 6 Months Post-Surgery: Pre-Operative Biometry Parameters |
Glare and Halos at 1 and 6 Months Post-Surgery: Refractive and Visual Acuity Parameters
Patients with worse pre-operative BCVA reported less glare and halos at 6 months, with different statistical significances depending on the compared groups of glare and halos (no vs mild vs moderate vs severe). Patients with mild glare at 6 months had lower 1 month spherical equivalent compared to patients with moderate glare – Table 4. Regarding glare and halos at 1 month, the same trend was observed, with patients with moderate glare or halos at 1 month having better pre-operative BCVAs compared to patients with no glare or halos (p=0.001 and p=0.002, respectively). When analyzing pre-operative BCVA considering only two groups of glare and halos, no/mild vs moderate/severe, there were also some significances, all in the same direction: the better the pre-operative BCVA the worse the glare or halos (p=0.042 for halos at 1 month; p=0.026 for glare at 6 months; p=0.003 for halos at 6 months).
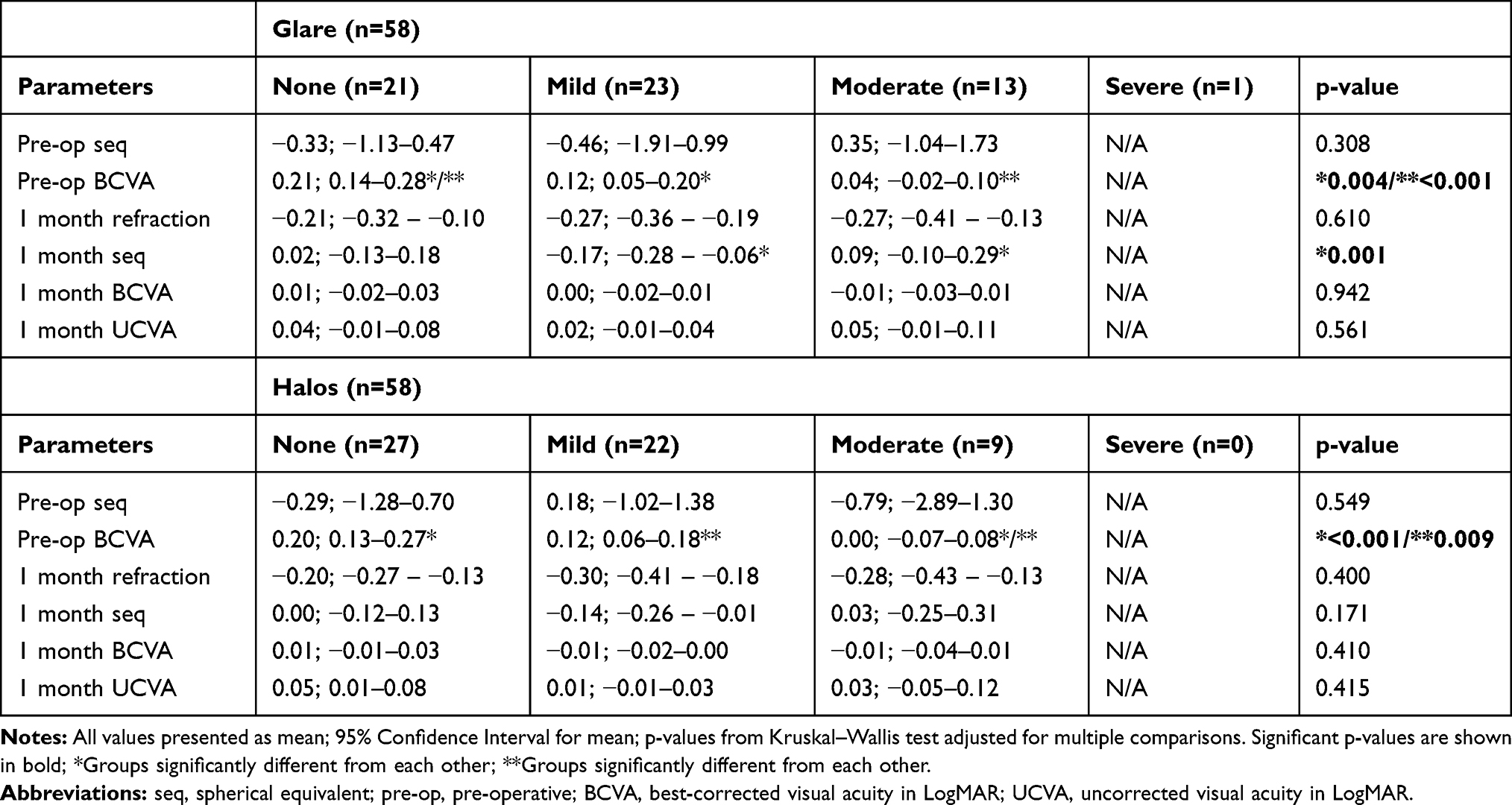 |
Table 4 Glare and Halos at 6 Months Post-Surgery: Refractive and Visual Acuity Parameters |
There was no correlation between pre-operative BCVA and sphere, cylinder or spherical equivalent at 1 month. There was also no association between pre-operative BCVA and spectacle dependence at all distances at 1 and 6 months.
Percentage of Patients with Glare and Halos Over Time
A significant proportion of patients had more none/mild compared to moderate/severe glare – Figure 1 – and halos – Figure 2 – both at 1 and 6 months post-operatively with no differences between time points.
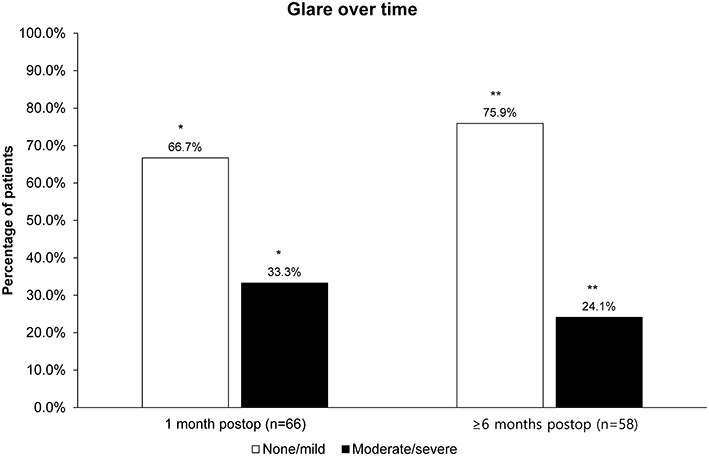 |
Figure 1 Percentage of patients with glare over time. */**p=0.001. p=ns between time points. |
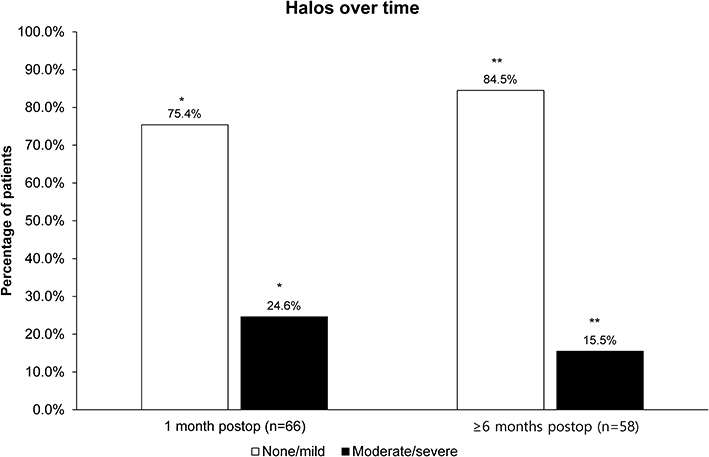 |
Figure 2 Percentage of patients with halos over time. */**p=0.002. p=ns between time points. |
Predictors of Glare and Halos at 1 and 6 Months Post-Surgery
After performing the multivariate logistic regressions with age, baseline BCVA and sphere at 1 month as the predictor variables, only BCVA at baseline was a negative predictor of halos at 1 month (B=−5.363, Exp(B)=0.005, 95% CI for Exp(B)=0.000–0.885, p=0.045), glare at 6 months (B=−5.522, Exp(B)=0.004, 95% CI for Exp(B)=0.000–0.832, p=0.043), and halos at 6 months (B=−12.203, Exp(B)=0.000, 95% CI for Exp(B)=0.000–0.084, p=0.014) post-surgery. The other two variables were not significant at the end of the iteration process.
Discussion
Post-surgery refractive results were good, with a mean spherical equivalent of −0.04D with a 95% CI −0.09–0.02, a sphere of 0.09D with a 95% CI 0.04–0.14, and a mean cylinder of −0.26D with a 95% CI −0.29–(−0.22), 1 month after surgery. These results are supported by the subjective vision quality perceived by patients, since the mean score at 1 month varied between 9.41 and 9.75 at all distances, and at 6 months varied between 9.25 and 9.61 at all distances (Table 1). Spectacle independence at all distances and at 1 and 6 months post-surgery varied between 97% and 100%, and probably for this reason between 96.6% and 98.5% of patients would recommend the surgery (Table 1). The incidence of capsular opacity was low both at 1 month and 6 months post-surgery (0.7% and 6.0%, respectively). At 6 months post-surgery, 3 eyes from 2 patients showed grade 1 PCO10 with no need for YAG laser capsulotomy, whilst 4 eyes from another 2 patients showed grade 2 PCO10 and underwent YAG laser capsulotomy. PCO had no influence on visual acuity or on the occurrence of glare or halos.
In our study, patients who presented a better baseline BCVA were more prone to perceive glares and halos after 1 month of surgery in comparison with the ones with a worse baseline BCVA. The same results were observed 6 months after surgery. Since the residual refractive error after surgery was very low and there was no correlation between pre-operative BCVA and sphere, cylinder or spherical equivalent at 1 month, and no association between pre-operative BCVA and spectacle dependence at all distances at 1 and 6 months, the relationship between pre-operative visual acuity and photic phenomena was not influenced by any of the mentioned results. Thus, the association between baseline BCVA and glares and halos seems to be dependent solely on the patient’s perception.
Overall, regression analysis corroborated the causality relation between a better baseline visual acuity and the occurrence of photic phenomena suggested by association analyses. These suggest that patients that have a better visual acuity before surgery are more demanding regarding visual outcomes after surgery, unlike those who have more visual impairment and therefore perceive any small improvement as important.
It has been proposed that perceived understanding of post-operative function and expectation-outcome discrepancy are important factors in the overall satisfaction of intervened cataract patients that generally present high expectations concerning the results of the procedures.11 Subjective visual symptoms, mostly blurred vision and photic phenomena, have been reported as the leading causes of patient dissatisfaction after multifocal IOL implantation, even though good visual acuity outcomes are obtained.12 Tchah et al suggested that visual acuity may not always be a good measure of subjective symptoms or patient satisfaction following implantation of multifocal IOL, since it was noticed that although all dissatisfied subjects had subjective visual complaints, their corrected distance visual acuity was 20/20 or better.5
Welch et al illustrated that the general level of patient satisfaction regarding cataract removal and IOL placement, while high, is still more affected by glare than by any other studied parameter, including UDVA, BCVA, posterior capsular opacification, and anterior capsular overlap of the IOL optic.13
Concerning the Acrysof IQ® PanOptix®, a study in 116 eyes of 58 patients evaluated visual outcomes with a visual satisfaction questionnaire (Catquest 9-SF with 5 added questions), which included photic phenomena, 9 and 12 months after surgery. A high percentage of patients did not present daily life challenges (84.5%), in spite of 32.8% reporting seeing halos often or always with illumination and 10.3% having occurrences of glare. Only 3.4% of patients declared to be quite unsatisfied with the surgery.14 Another study compared the visual performance and quality of vision of 60 binocularly implanted trifocal IOLs (FineVision vs PanOptix). Once again, halos were the most common phenomenon reported by patients, being mostly mild and therefore not considered to impact quality of life significantly.15
It has been suggested that glare and halos reported by pseudophakic patients can be attributed to spherical aberration. The contrast sensitivity anticipated for a multifocal IOL is lower than for healthy eyes, due to the increase in spherical aberration, and post-operative loss of contrast sensitivity after multifocal IOL implantation has been associated to HOA increase.16 The fact that the 0.200 to 0.399 µm corneal HOA group reported less moderate halos at 1 month compared to mild or no halos may indicate that patients within this range of HOA present a better visual quality and, therefore, less photic phenomena.
Our results also showed that both corneal coma and total coma are associated with mild halos at 6 months, which indicates that the lower the coma, the less the possibility of the occurrence of mild halos at 6 months. Univariate analysis, which considered corneal and total coma groups, showed the same results for the lower coma group, 0.000–0.199 µm.
Despite many patients with high angle kappa being asymptomatic, statistically significant association of angle kappa with the occurrence of halos and glares has been reported in some studies.17,18 Our results did not show any association between angle kappa and glare or halos. One possible explanation could be the cut-off value we have selected for the angle kappa in the inclusion criteria (≤0.58 mm). This is the value of the radius of the inner circle of the diffractive zone of the PanOptix trifocal IOL. It has been suggested that if the eye has an angle kappa greater than half of the diameter of the central ring of the multifocal IOL, light rays may pass through one or more of the multifocal rings and produce glare.19
Our results also suggest that the higher the lens thickness the less the occurrence of halos at 1 month. A higher value of chord μ was associated with a higher incidence of halos at 1 month, with no differences at 6 months or glare at any time point. The reported mean value and standard deviation for apparent chord µ is 0.30±0.15 mm. We may speculate that this absence of statistical significance may be due to the fact that in our study only one patient showed a chord µ value >0.6 mm and it has been suggested that values higher than 0.6 mm are more likely related to glare and halos with diffractive multifocal IOLs.20–22
Finally, age was associated with glare and halos at 1 and 6 months: lower aged patients showed more glare and halos at 1 month and 6 months. Similar results regarding halos in younger patients were published with the implantation of another trifocal IOL.23 Again these results suggest that lower aged patients are more demanding regarding visual outcomes after surgery. However, another study analyzed refractive and visual outcomes, patient satisfaction, and complications among different age groups. There were no statistically significant differences in visual phenomena or night driving difficulties reported by patients of different age groups.24
This study had some limitations. It was a single-center study, with no control group, and the time of follow-up might not have been sufficient to completely understand the level of bothersome related to unwanted photic phenomena, since its perception tends to decrease with time. It has been shown by the use of functional magnetic resonance imaging (MRI) that after the implantation of multifocal IOLs a form of long-term adaptation/functional plasticity occurs, since the study showed that fewer brain regions were required to perform the visual tasks as time passed.25 The main strengths of this study are the fact that all surgeries were performed by the same surgeon, thus reducing variability, and the fact that both objective and subjective parameters were collected.
Conclusion
This study shed some light on predictive factors of dissatisfaction for photic phenomena, allowing for a better management of patients’ expectations and increased satisfaction with the procedure. On multivariate regression analyses the only predictor of photic phenomena was baseline visual acuity, suggesting that patients that have a better visual acuity before surgery are more demanding regarding visual outcomes after surgery, unlike those who have more visual impairment and therefore perceive any small improvement as important.
Acknowledgments
There are no acknowledgements.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors have no conflicts of interest to declare.
References
1. de Silva SR, Evans JR, Kirthi V, Ziaei M, Leyland M. Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst Rev. 2016;12:Cd003169. doi:10.1002/14651858.CD003169.pub4
2. Khandelwal SS, Jun JJ, Mak S, Booth MS, Shekelle PG. Effectiveness of multifocal and monofocal intraocular lenses for cataract surgery and lens replacement: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2019;257(5):863–875. doi:10.1007/s00417-018-04218-6
3. Buckhurst PJ, Naroo SA, Davies LN, Shah S, Drew T, Wolffsohn JS. Assessment of dysphotopsia in pseudophakic subjects with multifocal intraocular lenses. BMJ Open Ophthalmol. 2017;1(1):e000064. doi:10.1136/bmjophth-2016-000064
4. Lee S, Choi M, Xu Z, Zhao Z, Alexander E, Liu Y. Optical bench performance of a novel trifocal intraocular lens compared with a multifocal intraocular lens. Clin Ophthalmol. 2016;10:1031–1038. doi:10.2147/OPTH.S106646
5. Tchah H, Nam K, Yoo A. Predictive factors for photic phenomena after refractive, rotationally asymmetric, multifocal intraocular lens implantation. Int J Ophthalmol. 2017;10(2):241–245. doi:10.18240/ijo.2017.02.10
6. Kohnen T. First implantation of a diffractive quadrafocal (trifocal) intraocular lens. J Cataract Refract Surg. 2015;41(10):2330–2332. doi:10.1016/j.jcrs.2015.11.012
7. Kohnen T, Herzog M, Hemkeppler E, et al. Visual performance of a quadrifocal (trifocal) intraocular lens following removal of the crystalline lens. Am J Ophthalmol. 2017;184:52–62. doi:10.1016/j.ajo.2017.09.016
8. Narang P, Agarwal A Chord mu: a new reference marker and its clinical relevance. Ocular Surgery News U.S. Edition; October 10, 2019. Available from: https://www.healio.com/ophthalmology/refractive-surgery/news/print/ocular-surgery-news/%7B61df24dc-e212-4f97-9b48-95ae4469aa2d%7D/chord-mu-a-new-reference-marker-and-its-clinical-relevance.
9. Holladay JT. Apparent chord mu and actual chord mu and their clinical value. J Cataract Refract Surg. 2019;45(8):1198–1199. doi:10.1016/j.jcrs.2019.03.029
10. Shakeel T, Dasgupta S. Comparative evaluation of posterior capsular opacification and Nd: YAG capsulotomy in children and adults. J Clin Exp Ophthalmol. 2019;5:105–107.
11. Chen Z, Lin X, Qu B, et al. Preoperative expectations and postoperative outcomes of visual functioning among cataract patients in Urban Southern China. PLoS One. 2017;12(1):e0169844. doi:10.1371/journal.pone.0169844
12. de Vries NE, Webers CAB, Touwslager WRH, et al. Dissatisfaction after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2011;37(5):859–865. doi:10.1016/j.jcrs.2010.11.032
13. Welch NR, Gregori N, Zabriskie N, Olson RJ. Satisfaction and dysphotopsia in the pseudophakic patient. Can J Ophthalmol. 2010;45(2):140–143. doi:10.3129/i09-266
14. Garcia-Perez JL, Gros-Otero J, Sanchez-Ramos C, Blazquez V, Contreras I. Short term visual outcomes of a new trifocal intraocular lens. BMC Ophthalmol. 2017;17(1):72. doi:10.1186/s12886-017-0462-y
15. Gundersen KG, Potvin R. Trifocal intraocular lenses: a comparison of the visual performance and quality of vision provided by two different lens designs. Clin Ophthalmol. 2017;11:1081–1087. doi:10.2147/OPTH.S136164
16. Bellucci R, Curatolo MC, New Extended A. Depth of focus intraocular lens based on spherical aberration. J Refract Surg. 2017;33(6):389–394. doi:10.3928/1081597X-20170329-01
17. Fu Y, Kou J, Chen D, et al. Influence of angle kappa and angle alpha on visual quality after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2019;45(9):1258–1264. doi:10.1016/j.jcrs.2019.04.003
18. Wang R, Long T, Gu X, Ma T. Changes in angle kappa and angle alpha before and after cataract surgery. J Cataract Refract Surg. 2020;46(3):365–371. doi:10.1097/j.jcrs.0000000000000063
19. Moshirfar M, Hoggan RN, Muthappan V. Angle Kappa and its importance in refractive surgery. Oman J Ophthalmol. 2013;6(3):151–158. doi:10.4103/0974-620X.122268
20. Prakash G, Prakash DR, Agarwal A, Kumar DA, Agarwal A, Jacob S. Predictive factor and kappa angle analysis for visual satisfactions in patients with multifocal IOL implantation. Eye (Lond). 2011;25(9):1187–1193. doi:10.1038/eye.2011.150
21. Karhanová M, Marešová K, Pluháček F, Mlčák P, Vláčil O, Sín M. The importance of angle kappa for centration of multifocal intraocular lenses. Cesk Slov Oftalmol. 2013;69(2):64–68.
22. Karhanová M, Pluháček F, Mlčák P, Vláčil O, Šín M, Marešová K. The importance of angle kappa evaluation for implantation of diffractive multifocal intra-ocular lenses using pseudophakic eye model. Acta Ophthalmol. 2015;93(2):e123–e128. doi:10.1111/aos.12521
23. Vryghem JC, Heireman S. Visual performance after the implantation of a new trifocal intraocular lens. Clin Ophthalmol. 2013;7:1957–1965. doi:10.2147/OPTH.S44415
24. Schallhorn SC, Schallhorn JM, Pelouskova M, et al. Refractive lens exchange in younger and older presbyopes: comparison of complication rates, 3 months clinical and patient-reported outcomes. Clin Ophthalmol. 2017;11:1569–1581. doi:10.2147/OPTH.S143201
25. Rosa AM, Miranda AC, Patricio MM, et al. Functional magnetic resonance imaging to assess neuroadaptation to multifocal intraocular lenses. J Cataract Refract Surg. 2017;43(10):1287–1296. doi:10.1016/j.jcrs.2017.07.031
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.